Embed Size (px)
Citation preview

An Approach to: Thyroid Function Tests
Rinkoo Dalan Consultant
Department of Endocrinology Tan Tock Seng Hospital

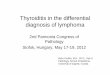
Hypothalamus
Median Eminence (base of brain)
Posterior Pituitary
Anterior Pituitary
Body
TRH
TSH
T3,T4
TRH
Regulation of Thyroid axis
----
T3, T4 ↑ TSH↓
T3, T4↓ TSH ↑

Na Io
TSH_R
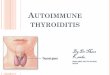
Within the thyroid gland
TSH
Tg
Io Tg + MIT,DIT
T3 T4
T4 T4 T4 T3
C-amp
Io
T4
Peripheral action of T3
T4 T4 T4

6 combinations possible TSH Low
Decreased Free T4
Decreased Free T4
Normal Free T4
High Free T4
TSH Low
TSH Low
TSH High
TSH High Normal Free T4
Increased Free T4 TSH High
TSH Normal with either increased or decreased free T4

TSH Low High Free T4 Common causes: Primary Hyperthyroidism : Graves’s Disease, toxic nodule or toxic MNG Relatively Common with low RAI uptake: Transient thyroiditis-postpartum, Silent (lymphocytic), post viral granulomatous subacute De Quervan’s Rare: Thyroxine ingestion, Ectopic thyroid tissue (struma ovari), Iodine Induced, Amiodarone. Rare with positive HCG: Pregnancy with hyperemesis gravidarum. HCG producing tumor; Familial gestational hyperthyroidism Rare –familial or resistant to treatment : Activating germline TSH-receptor mutation

Case 1: The lady with Pain in the Neck
46 yrs old lady presents with prolonged fever for 6/52 associated with anterior neck pain.
URTI 4/52 earlier On palpation Small diffuse,firm
goitre tender.
Tests Value RI
Free T4 44pM 8-21pM
TSH <0.001mIU/L 0.34-5.64
ESR 100 mm 3-5
TrAb 4 IU/L <2
Thyroid gland is not visible

Case 2: The depressed Lady A 46 yrs lady was started on Lithium for
depression. She presented with symptoms of heat
intolerance, weight loss and palpitations.
O/E : small diffuse non tender goitre
Tests Value RI
Free T4 25 pM 8-21pM
TSH <0.001mIU/L 0.34-5.64
Free T3 8 pM (4.5-6.8)
TrAb Not detectable
<2
Lithium was discontinued. Subsequently 3 months later: Free T4: 18pM; TSH: 1.0 mIU/L
Disturbed iodine kinetics with Expansion of intrathyroidal iodine pool ,
Escape phenomenon Overflow of thyroid hormones

Case -3: Lady who was persistently vomiting
A 28 years old lady presented with severe Nausea and vomiting Did not resolve with regular
medication
Free T4= 30 pM (8-21) TSH= 0.01mIU/L (0.34-5.6)
On further questioning: No past h/o thyroid problems No goitre Totally asymptomatic. Menstrual cycle: regular but has not had menses the last 2 cycles.
Pregnancy with hyperemesis Gravidarum

Case 4: The Giddy Lady 65 yrs old lady Giddiness and palpitations Apathetic No goitre palpable
Tests Value RI
Free T4 65 pM 8-21pM
TSH <0.001mIU/L 0.34-5.64
Free T3 24 pM (4.5-6.8)
TrAb >40 <2
Diagnosis : Thyrotoxicosis secondary to Graves’ Disease

6 combinations possible TSH Low
Decreased Free T4
Decreased Free T4
Normal Free T4
High Free T4
TSH Low
TSH Low
TSH High
TSH High Normal Free T4
Increased Free T4 TSH High
TSH Normal with either increased or decreased free T4

TSH Low Normal Free T4
Common Causes: Subclinical Hyperthyroidism T3 Toxicosis Thyroxine ingestion Normal Pregnancy Rare Causes: Steroids therapy Dopamine/Dobutamine infusions NTI

Case 5: 65 yrs old lady Giddiness and
palpitations Right thyroid nodule
palpable
Tests Value RI
Free T4 18 pM 8-21pM
TSH <0.001mIU/L 0.34-5.64
Free T3 12 pM (4.5-6.8)
TrAb Not detectable
<2
T3 Toxicosis secondary to Toxic Nodule

Case 6: A 28 years old lady Healthy-no medical problems at all. Newly enrolled in a school as a teacher Required to do health screening pre-
employment.
Tests Value RI
Free T4 15 pM 8-21pM
TSH 0.14 mIU/L 0.34-5.64
TrAb Not detectable
<2
On further questioning: No past h/o thyroid problems No goitre Totally asymptomatic. Menstrual cycle: regular but has not had menses the last cycle.
Normal Pregnancy : Physiological

Case 7 A 70 years old lady is admitted with complains of fever, giddiness , confusion increased urinary frequency. She is tachycardic at 120 /min and febrile with Temp:39 C. Because of acute confusion the HO ordered the ff : Ca, Mg, PO4, Thyroid panel
Free T4 : 16 pmol/L (8-21) TSH 0.24 mIU/L (0.34-5.64)
Free T3 : Low Diagnosis : Non-thyroidal illness. 2 months later repeat thyroid function : Free T4: 9 pmol/L, TSH:2.34 mIU/L

NTI

Case 8 A 70 yrs old Chinese lady seeks advice as a
routine screening: She had an episode of AF when she was
admitted for Pneumonia but reverted to normal after that.
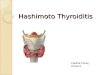
BMD : Osteopenia –T score-2.1 SD at hip No Goitre Free T4 : 15 pmol/L TSH: 0.01 mIU/L

An algorithm that outlines a proposed plan for the evaluation and therapy of subclinical hyperthyroidism. *, Based on data showing higher mortality ,atrial fibrillation, bone loss,
symptoms or reduced quality of life .
Cooper D S JCEM 2007;92:3-9 ©2007 by Endocrine Society

6 combinations possible TSH Low
Decreased Free T4
Decreased Free T4
Normal Free T4
High Free T4
TSH Low
TSH Low
TSH High
TSH High Normal Free T4
Increased Free T4 TSH High
TSH Normal with either increased or decreased free T4

TSH Low Decreased Free T4
Common: Non Thyroidal illness Recent Treatment for hyperthyroidism Rarer: Secondary Hypothyroidism Congenital TSH or TRH hormone
deficiency

Case 9: A 68 years old Taxi driver Presented with headache,nausea
and malaise. Minor accidents –usually knocks
down with pavements on the sides
Tests Value RI Free T4 8pM 8-21pM
TSH 0.21mIU/L 0.34-5.64
Free T3 2 pM 4-6 pM Prolactin 69,000
mIU/L 64-277

Case 10: A 30 years old Indonesian Presented with short height, constipation, low
intelligence Born normal but began to lag behind in growth
and intelligence at 5 years of age. No puberty and no secondary sexual
characteristics. Height 148 cm Bone age 11-12 years Epiphyses not fused Tests Value RI
Free T4 8 pM 8-21pM
TSH 0.21mIU/L 0.34-5.64
Free T3 2 pM 4-6 pM
LH <1 FSH <1 IGF-1 10

PROP-1 Mutation leading to combined multiple hormonal deficiencies Secondary hypothyroidism Hypogonadotrophic hypogonadism GH deficiency. Long history and the multiplicity of disorders suggests that he has a mutation in one of the genes encoding the transcription factors that are responsible for anterior pituitary development. MRI Pituitary :Looks hypoplastic to normal in appearance.

6 combinations possible TSH Low
Decreased Free T4
Decreased Free T4
Normal Free T4
High Free T4
TSH Low
TSH Low
TSH High
TSH High Normal Free T4
Increased Free T4 TSH High
TSH Normal with either increased or decreased free T4

Common • Chronic autoimmune
thyroiditis • Post radioiodine • Post thyroidectomy • Hypothyroid phase of
transient thyroiditis
TSH High Decreased Free T4
Rare (anti-TPO negative, no radioiodine or surgery) 1. Post external-beam irradiation to the neck 2. Drugs: amiodarone, lithium, interferons, interleukin-2 3. Iodine deficiency 4.Iodine excess-iodide goitre in Japan (water purification units) 5. Goitrogens 6. Amyloid goitre (large, firm goitre with systemic amyloidosis) 6. Riedel’s thyroiditis
Congenital hypothyroidism Thyroid agenesis/dysgenesis Iodide organification defects TSH receptor defects/resistance

Case 11 A 24 years old lady Presents with
dysmenorrhoea and increased flow.
Also has weight gain Cold intolerance Constipation O/E : small diffuse goitre
Thyroid Function Test: Free T4= 6 pmol/L (RI:8-21) TSH =50 mIU/L Anti TPO ab : positive
Diagnosis: Hashimoto’s Thyroiditis with Primary Hypothyroidism

6 combinations possible TSH Low
Decreased Free T4
Decreased Free T4
Normal Free T4
High Free T4
TSH Low
TSH Low
TSH High
TSH High Normal Free T4
Increased Free T4 TSH High
TSH Normal with either increased or decreased free T4

Common: Subclinical autoimmune hypothyroidism Rare: Heterophile (interfering) antibody Intermittent T4 therapy for hypothyroidism Drugs: amiodarone, sertraline, cholestyramine Recovery phase after non-thyroidal illness Congenital TSH-receptor defects Resistance to TSH associated with other (unspecified) defects Pendred’s syndrome—some cases (associated with sensorineural deafness and goitre)
TSH High Normal Free T4

Case 12
A 83 years old gentleman has baseline hyperlipidemia very well controlled on Simvastatin 20 mg daily.
He seeks advice regarding starting thyroxine
Free T4=13 pmol/L TSH = 7.1 mIU/L 6/12 later: Free T4 : 12 pmol/L TSH: 15 mIU/L
Diagnosis: Subclinical Hypothyroidism

Persistently raised TSH Concentration
TSH 5-9 mIU/L TSH >10 mIU/L
Consider treatment in young, Middle aged patients especially if child bearing age group females, goitre present or antibodies positive or symptomatic. Treat with Thyroxine Goal TSH conc 0.5-2.5 mIU/L
No treatment in patients >85yrs age. In patients older than 65 if treating target TSH<7 mIU/L
Treat with Levothyroxine Goal TSH <60 yrs 0.5-2.5 mIU/L Goal TSH>60 yrs 4-6 mIU/L

6 combinations possible TSH Low
Decreased Free T4
Decreased Free T4
Normal Free T4
High Free T4
TSH Low
TSH Low
TSH High
TSH High Normal Free T4
Increased Free T4 TSH High
TSH Normal with either increased or decreased free T4

Rare—with discordant free T4 versus free T3 • Interfering antibodies to thyroid hormones (anti-TPO
antibodies usually also present) • Familial dys-albuminaemic hyper-thyroxinaemia • Amiodarone Rare—other • Intermittent T4 therapy or T4 overdose • Resistance to thyroid hormone • TSH secreting pituitary tumour (hyperthyroid) • Acute psychiatric illness (first 1–3 week)
TSH High Increased Free T4

Case 13 A 65 years old lady presents after
fracture neck of femur. Weight loss 1/12 AF diagnosed 2 months ago Small goitre
Free T4= 22 pmol/L (8-21) TSH= 8.64 mIU/L (0.34-5.64) Free T3=12 pmol/L (4-6)
3/12 repeat at another centre Free T4= 64 pmol/L (8-21) TSH= 8.69 mIU/L (0.34-5.64) Free T3=12 pmol/L (4-6)
Differential diagnosis: Heterophilic antibodies Non thyroidal illness TSH resistance syndrome TSH producing pituitary adenoma

TRH Stimulation test-200 mcg
O min : 7.48 mIU/L 15 min: 7.13 mIU/L 30 min: 7.47 mIU/L 45 min: 7.16 mIU/L 60 min: 7.16 mIU/L
Diagnosis: TSH producing pituitary adenoma

6 combinations possible TSH Low
Decreased Free T4
Decreased Free T4
Normal Free T4
High Free T4
TSH Low
TSH Low
TSH High
TSH High Normal Free T4
Increased Free T4 TSH High
TSH Normal with either increased or decreased free T4
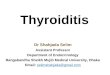
Primary hyperthyroidism
Central hypothyroidism
Subclinical hyperthyroidism
Primary hypothyroidism
Subclinical hypothyroidism
TSH resistance/
TSH producing pituitary adenoma

Reference
Colin M Dayan. Interpretation of thyroid function tests. Lancet 2001; 357: 619–24