Embed Size (px)
Citation preview

Short reports
Pl~~~~~~~~~~~~~~~~'
...... i;.. ~~-<. '. Y.',
0k
.. ...
............
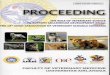
Figure 2 Endometrial curettage revealing the bone tissue and a fragment of a?endometrial gland (arrow head) with neutrophilic infiltration.
ing cause of endometrial ossificatidometritis, especially chronic endonossification may develop in the olhinflammatory tissue.7 Prolonged o0stimulation is thought to be relatipathogenesis of endometrial ossificatiever, this is unlikely in this patient.Bone formation in the endometriu
but may be observed in malignamiillerian tumour and teratoma,5 whibe considered as a differential diagnccially in older women.'"
In summary, endometrial ossification inpostmenopausal women is very rare; mostwomen presenting with this condition arebetween 20 and 40 years of age. Therefore, cli-nicians should consider the possibility ofendometrial ossification as a differential diag-
AA nosis of intrauterine foreign body on ultra-sound, even in older patients. In addition,pathologists should be aware of this rare entityto avoid a misdiagnosis of malignant mixedmuillerian tumour in the endometrial curettagespecimen, which may result in unnecessaryhysterectomy.
1 Qi L, Qunli S, Yanhua S, Xiaojuan Y. Pregnancy achievedafter treatment in a case of endometrial ossification. A casereport and literature review. Chin MedJ 1995;108:793-5.
2 Acharya U, Pinion SB, Parkin DE, Hamilton MPR. Osseousmetaplasia of the endometrium treated by hysteroscopicresection. BrJ7 Obstet Gynaecol 1993;100:391-2.
3 Rodriguez BD, Adamson GD. Hysteroscopic treatment ofn ectopic intrauterine bone. A case report. J Reprod Med
1993;38:515-20.4 Taylor PJ, Hamou J, Mencaglia L. Hysteroscopic detection
of heterotopic intrauterine bone formation. J Reprod Medon iS en- 1988;33:337-9.aetritis, as 5 Bhatia NN, Hoshiko MG. Uterine osseous metaplasia.d, 6ealing Obstet Gynecol 1982;60:256-9.d,healng 6 Ceccacci L, Clancy G. Endometrial ossification: report of anestrogenic additional case. Am J Obstet Gynecol 1981;141:103-4.ed to the 7 Waxman M, Moussouris HF. Endometrial ossificationedtothe following an abortion. Am J7 Obstet Gynecol 1978;130:587-
ion,6 how- 8.8 Wetzels LCG, Essed GGM, de Haan J, van de Kar AJF,
Willebrand D. Endometrial ossification: unilateral manifes-im is rare, tation in a septate uterus. Gynecol Obstet Invest 1 982;14:47-nt mixed 9 Ombelet W Endometrial ossification, an unusual finding inich should an infertility clinic. A case report. J Reprod Med)ss9 ep- 1989;34:303-6.
s5i5, espe- 10 Barwick KW, LiVolsi VA. Malignant mixed mulleriantumors of the uterus. Am J Surg Pathol 1979;3: 125-35.
J Clin Pathol 1997;50:172-174
Lithium associated autoimmune thyroiditis
M Shimizu, M Hirokawa, T Manabe, K Shimozuma, H Sonoo, T Harada
Department ofPathology, KawasakiMedical School,Kurashiki, Okayama,JapanM ShimizuM HirokawaT Manabe
Department of Breastand Thyroid SurgeryK ShimozumaH Sonoo
Kawasaki Coliege ofAllied HealthProfessionsT Harada
Correspondence to:Dr Michio Shimizu,Department of Pathology,Kawasaki Medical School,Kurashiki, Okayama 701-01,Japan.
Accepted for publication3 October 1996
AbstractA case of autoimmune thyroiditis afterlong term treatment with lithium isdescribed in a 29 year old Japanese womanwith manic depression. Positive serum
antithyroglobulin and antimicrosomal an-
tibodies, diffuse goitre, and microscopicchronic thyroiditis, as well as the clinicalhistory of long term lithium treatmentwere suggestive of lithium associatedautoimmune thyroiditis. Microscopically,there was a mild degree of interstitialfibrosis and a moderate degree of lym-phocytic infiltration. Some areas showed a
moderate degree of stromal fibrosis andatrophic thyroid follicles. Lymphoid folli-cles with germinal centres, disrupted thy-roid follicles with lymphocyticinfiltration, and Hurthle cells were alsoobserved. The differential diagnosis in
patients presenting with these histologicalfeatures includes painless (silent) thy-roiditis, autoimmune thyroiditis andlithium associated autoimmune thyroidi-tis. A detailed clinical history is essential ifthe correct diagnosis is to be reached.(7 Clin Pathol 1997;50:172-174)
Keywords: thyroid; lithium; autoimmune thyroiditis.
Lithium has been used in the treatment ofmanic and hypomanic depressive disorders formany years. Long term treatment with lithiumis associated with hypothyroidism, euthyroidgoitre, and hyperthyroidism. 1 The aetiology ofthe first two conditions can be explained by theeffect of lithium on the thyroid; however, thatof hyperthyroidism has been not been ex-plained adequately. Other cases of lithiumrelated thyroid disease have been reported but
172
on June 17, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.50.2.172 on 1 F
ebruary 1997. Dow
nloaded from

Short reports
-74~ ~ ~
j...
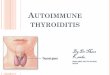
Figure 1 Thyroid follicles of varying sizes, lymphocytic infiltration and a lymphowith a germinal centre can be seen.
the histological findings have not. We da case highlighting the histological finclithium associated autoimmune thyroid
Case reportIn August 1993, a 29 year old Japanesewas admitted hospital for resection of agoitre because she wanted to have a balpatient's illness dated back to July 19fhad been treated for manic depressiclithium carbonate (600 mg/day) for 27 r
Goitre was not noted and serum
autoantibody was not measured at hepresentation. In October 1990, thecomplained of palpitations, irritaticweight loss, and was diagnosed withdisease. Immediately after this diagnowas treated with methimazole (15 r
until August 1993. The patient also coi
to be treated with lithium. In April 19results of her thyroid function tests weri
lows: thyroxine, 233 nmol/l (normal58-155 nmol/l); triiodo-thyronine, 3.6(1.2-3.1 nmol/l); thyroid stimulating h((TSH), <0.05 iIU/ml (0.03-5.00 pjand TSH binding inhibitor immunog(TBII), 22.9% (<15%), which were sui
*VJttt*-V.
V L~#-.e2AN M
-,
.:.;.4.
',0
of a diagnosis of Graves' disease. However,on admission in 1993, the patient hadbecome euthyroid, and diffuse goitre (rightlobe 6.5 x 2.3 x 1.7 cm; left lobe 6.5 x2.0 x 1.5 cm) was observed. Both serum an-tithyroglobulin and antimicrosomal antibodieswere positive at that time. The patientunderwent subtotal thyroidectomy for thediffuse goitre.
PathologyGrossly, the resected thyroid was covered withscattered white spots, but no mass was noted.Microscopically, lobulation of the gland wasobserved under low power. There was a milddegree of interstitial fibrosis and a moderatedegree of lymphocytic infiltration. The thyroidfollicles varied in size. Some areas showed amoderate degree of stromal fibrosis and
,idfollicle atrophic thyroid follicles. Lymphoid follicleswith germinal centres, disrupted thyroid folli-cles with lymphocytic infiltration, and Hiirthle
lescribe cells were also observed in some areas (figs 1lings of and 2). In other areas, papillary infoldings pro-1itis. jecting into the thyroid follicles and scalloping
of the colloid were present.
woman Discussiondiffuse The development of hypothyroidism or goitreby. The is a well known complication of long term88. She lithium treatment.' 4 5 There have, however,)n with only been sporadic cases of hyperthyroidismnonths. among patients treated with lithium.2 Otherthyroid lithium related or associated thyroid diseasesr initial have rarely been described in the literature, andpatient only three cases of lithium associated thyroidi-)n and tis and three cases of lithium associatedGraves' autoimmune thyroiditis have been reported.7isis, she In the cases of lithium associated thyroiditis,ng/day) thyroid antibody levels were not measured.ntinued Histologically, in the two cases reported by'92, the LiVolsi,7 lymphocytic infiltration, focal follicu-e as fol- lar atrophy and mild stromal fibrosis wereI range observed. It was also pointed out that theInmol/l histopathological appearance was consistentormone with that found in autoimmune thyroiditis. InIU/ml); the case reported by Kontozoglou andrlobulin Mambo,8 prominent fibroblastic activity andggestive numerous lymphoid follicles lacking typical
Hurthle cells were observed. Our patientshowed lymphocytic infiltration with lymphoidfollicles and interstitial fibrosis with focalfollicular atrophy, as well as disrupted thyroidfollicles and Hurthle cells. In addition, ourpatient presented with positive serum antithy-roid antibodies and diffuse goitre, and a clinicalhistory of long term lithium treatment, all ofwhich are suggestive of lithium associatedautoimmune thyroiditis. Lithium may alsonotably increase the titre of thyroid microsomalantibodies and convert latent subclinical au-toimmune disease into clinically overt illness.9
In practice, however, it is difficult to arrive at. the correct diagnosis without knowledge of the
patient's clinical history. In our patient, weconsidered that the lymphocytic infiltration
Ql.t'*W and lymphoid follicles with germinal centresWf ¢ ;. were too noticeable to be those typically found:- <*in Graves' disease, and chronic thyroiditis was
clearly observed histologically. Furthermore,
173
on June 17, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.50.2.172 on 1 F
ebruary 1997. Dow
nloaded from

Short reports
the findings of interstitial fibrosis, disruptedthyroid follicles, and Hurthle cells were notconsistent with euthyroid Graves' disease,medically treated Graves' disease, or Hashi-toxicosis, because of the lack of classicophthalmopathy, the replacement of normalthyroid follicular epithelium by hyperplasticepithelium in less than 50% of the specimen,and the euthyroid state in this patient.7 " Pain-less thyroiditis, also known as silent thyroiditis,is another possibility; this is characterised by apainless thyroid gland, raised serum concentra-tions of thyroid hormone, low radioactiveiodine uptake, and spontaneously resolvinghyperthyroidism.'0 Histologically, painless thy-roiditis resembles autoimmune thyroiditis, butaccording to Mizukami et al'0 stromal fibrosisand Hurthle cells are rare in the former. Aftercontacting the patient's clinician, we found thatshe had been receiving long term lithium treat-ment (over five years) for her psychiatriccondition, and we were then able to arrive atthe diagnosis of lithium associated autoim-mune thyroiditis. However, without knowledgeof the patient's clinical history, it probablywould have been difficult for us to differentiate
between painless thyroiditis and lithium associ-ated autoimmune thyroiditis. Treatment withmethimazole may have partly affected thechange from a hyperthyroid to a euthyroid statein this patient.
1 Jefferson JW. Lithium carbonate-induced hypothyroidism.Its many faces.JAMA 1979;242:271-2.
2 McDermott MT, Burman KD, Hofeldt FD, Kidd GS.Lithium-associated thyrotoxicosis. Am J Med 1986;80:1245-8.
3 Mizukami Y, Michigishi T, Nonomura A, Nakamura S,Noguchi M, Takazakura E. Histological features of the thy-roid gland in a patient with lithium induced thyrotoxicosis.J Clin Pathol 1995;48:582-4.
4 Bocchetta A, Bernardi F, Pedditzi M, Loviselli A, Velluzzi F,Martino E, et al. Thyroid abnormalities during lithiumtreatment. Acta Psychiatr Scand 1991;83:193-8.
5 Lee S, Chow CC, Wing YK, Shek CC. Thyroid abnormali-ties during chronic lithium treatment in Hong KongChinese: a controlled study. JAffect Disord 1992;26:173-8.
6 Gittoes NJL, Franklyn JA. Drug-induced thyroid disorders.Drug Saf 1995;13:46-55.
7 LiVolsi VA. Lymphocytes in the thyroid. In: Surgical pathol-ogy of the thyroid. Philadelphia: WB Saunders, 1990:68-97.
8 Kontozoglou T, Mambo N. The histopathologic features oflithium-associated thyroiditis. Hum Pathol 1983;14:737-9.
9 Calabrese JR, Gulledge AD, Hahn K, Skwerer R, Kotz M,Schumacher OP, et al. Autoimmune thyroiditis in manicdepressive patients treated with lithium. Am J Psychiatry1985;142:1318-21.
10 Mizukami Y, Michigishi T, Nonomura A, Nakamura S,Ishizaki T. Pathology of chronic thyroiditis: A new clinicallyrelevant classification. Pathol Annu 1994;29: 135-58.
I Clin Pathol 1997;50:174-176
Atypical manifestations in a patient with systemiclupus erythematosus
Department ofPathology, UniversityofHong Kong, QueenMary HospitalKY Lam
Department of ClinicalPathology, PamelaYoude NethersoleEastern HospitalF Cheung
Department ofMedicine, PamelaYoude NethersoleEastern HospitalL Y C YamC H Lee
Department ofDiagnostic Radiology,Pamela YoudeNethersole EasternHospitalK H Fung
Correspondence to:Dr King-Yin Lam,Department of Pathology,Queen Mary Hospital,Pokfulam Road, Hong Kong.
Accepted for publication5 November 1996
K Y Lam, F Cheung, L Y C Yam, C H Lee, K H Fung
AbstractSystemic lupus erythematosus (SLE) is achronic systemic inflammatory diseaseassociated with the production of variousautoantibodies and involvement of multi-ple organs. Necropsy findings in a 65 yearold woman with SLE who had multipleaortic aneurysms and dissections, as wellas other unusual manifestations, are de-scribed. The case illustrates the occur-rence of and the difficulties encounteredin the diagnosis of several diseases,namely aortic aneurysm, aortic dissec-tion, acute pancreatitis, and Penicilliummarneffei infection.(7 Clin Pathol 1997;50:174-176)
Keywords: systemic lupus erythematosus; aneurysm;dissection.
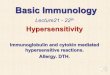
Figure 1
Systemic lupus erythematosus (SLE) is a thimracicaorchronic systemic inflammatory disease associ- section wouiated with the production of various autoanti- however,fozbodies and involvement of multiple organs. We aonretclume?report the necropsy findings in a patient with saccular ani
Axial contrast enhanced CT scan of distalrta at level of the left ventricle. Presence ofan5 (arrowhead) across the aortic lumen at thisId have suggested aortic dissection. This was,und to be the undermined edge of a saccularThe smaller compartment proved to be the true~n and the larger one to be the lumen of theteurysm at necropsy.
174
on June 17, 2022 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.50.2.172 on 1 F
ebruary 1997. Dow
nloaded from





![Hashimoto’s Thyroiditis and Encephalopathytiple sclerosis, and vitiligo [29]. It can be part of the autoimmune poly-endocrine syndrome type-2. Autoantibodies to TPO and Tg are inherited](https://img.pdfslide.us/doc/110x75/5eaf7a6990e3642c831b9a02/hashimotoas-thyroiditis-and-encephalopathy-tiple-sclerosis-and-vitiligo-29.jpg)