Embed Size (px)
Citation preview
AmyM.Wetherby,Ph.D.DistinguishedResearchProfessor
LaurelSchendelProfessorofCommunicationDisordersDirector,AutismInstitute
CollegeofMedicine,FloridaStateUniversity
MobilizingCommunitySystemstoImproveEarlyDetection&ChangeDevelopmentalTrajectoriesofToddlerswithAutismSpectrumDisorder:
StrategiesforBridgingResearchtoPractice
CullowheeConferenceonCommunicativeDisordersWesternCarolinaUniversity
March24,2017 Cullowhee,NC
Outline
1. Howdowebridgetheresearch-to-practicegap?• Whatdoestheresearchtellusaboutearly
detectionofASD?• RollingouttheAutismNavigatorweb-based
coursesandtoolsusingextensivevideofootage
2. CanwechangedevelopmentaltrajectoriesoftoddlerswithASD?• Whatdoestheresearchtellusaboutearly
interventionfortoddlerswithASD?• EarlySocialInteractionProjectCoachingmodel
Wetherby, 2017- Page 1

Financial&NonfinancialDisclosures
l AmyWetherbyisemployedbyFSUandhasreceivedgrantfundingtosupportresearchonearlydetectionandearlyinterventionfromNIH,USDOE,&theCDC.
l AmyWetherbyisauthoroftheCommunicationandSymbolicBehaviorScales(CSBS)andtheSCERTSModelpublishedbyBrookesPublishingandreceivesroyalties
l AmyWetherbyisanownerofAutismNavigator,LLC.Nosalaryisearnedand100%oftheprofitsaredonatedtoanonprofittosupportthecourses&tools.
RecommendationsoftheAmericanAcademyofPediatrics(2007)l Developmentalsurveillanceateverywell-childvisitfrom9to30months
l ScreenallchildrenforASDat18and24months
✔ Autismcanbediagnosedby18-24months,yetthemedianageofdiagnosisofASDis4-5yearsintheUS✔ Childrenofminority,lowincome,andruralfamiliesarediagnosedayearandahalflater.
Wetherby, 2017- Page 2

FundedbyNICHD,CDC,&NIDCD
www.FirstWordsProject.comPI:AmyM.Wetherby,Ph.D.FloridaStateUniversity
SORF –ObservationalScreeningTool
Systematic
Observationof
Red
FlagsofAutismSpectrumDisorder
Wetherby, 2017- Page 3

Push-Pull: BuildingtheCapacityofCommunitiestoImproveEarlyDetection&AccesstoCare
PrimaryCareFromPhysiciansto
EarlyCare&Learning
EarlyInterventionProviders
Copyright©2017.TheFloridaStateUniversity.Allrightsreserved.
SneakPeekatourGalleryLaunchinginApril2017www.FirstWordsProject.com
Copyright©2017.TheFloridaStateUniversity.Allrightsreserved.
Wetherby, 2017- Page 4

CourseIntroduction
Jump-StarttoPrimaryCare
1. CoreDiagnosticFeatures
2. PrevalenceandCause
3. EarlyDetection4. CollaboratingwithFamilies
5. Screening&Referral
6. EarlyInterventionBasics
for Primary Care
This8-hourcourselaunchedintheFall,2015.
Copyright©2017.TheFloridaStateUniversity.Allrightsreserved.
Copyright©2017.TheFloridaStateUniversity.Allrightsreserved.Copyright©2017.TheFloridaStateUniversity.Allrightsreserved.
Wetherby, 2017- Page 5
www.FirstWordsProject.comCopyright©2017.TheFloridaStateUniversity.Allrightsreserved.
Copyright©2017.TheFloridaStateUniversity.Allrightsreserved.
Wetherby, 2017- Page 6

Copyright©2017.TheFloridaStateUniversity.Allrightsreserved.
Wetherby, 2017- Page 7

Copyright © 2017 by Florida State University. All rights reserved.
Knowledge and Skills LevelØ Explore Function
• 5 Developmental Domains• Hundreds of Videos clips
illustrating 80 SC milestonesØ Study-Guide Function
• 15 Self-Guided Lessons• 5 Learning Assessments
Mastery LevelØ Home Visitors Guide to support families in
the SC Growth Charts
Wetherby, 2017- Page 8
www.AutismNavigator.com
Wetherby, 2017- Page 9
Wetherby, 2017- Page 10
Copyright © 2017. The Florida State University. All rights reserved.
Our New Gallery will Launch in April 2017www.FirstWordsProject.com
Wetherby, 2017- Page 11
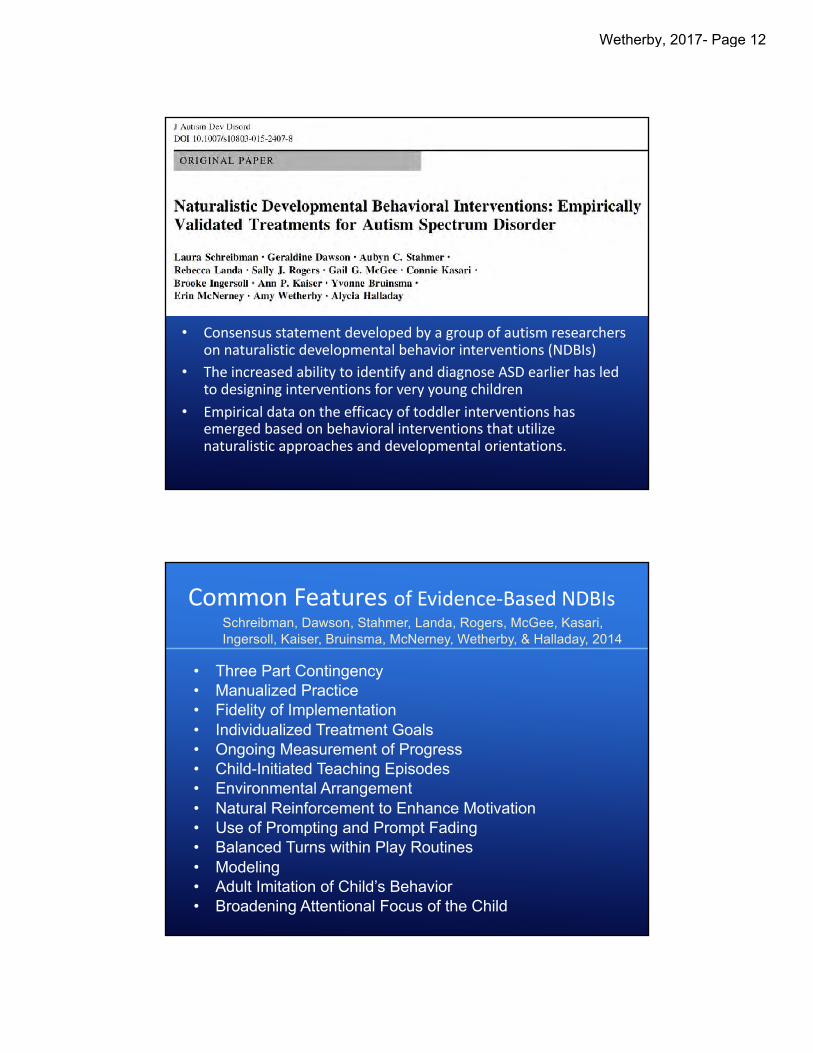
• Consensusstatementdevelopedbyagroupofautismresearchersonnaturalisticdevelopmentalbehaviorinterventions(NDBIs)
• TheincreasedabilitytoidentifyanddiagnoseASDearlierhasledtodesigninginterventionsforveryyoungchildren
• Empiricaldataontheefficacyoftoddlerinterventionshasemergedbasedonbehavioralinterventionsthatutilizenaturalisticapproachesanddevelopmentalorientations.
CommonFeaturesofEvidence-BasedNDBIs
• Three Part Contingency• Manualized Practice• Fidelity of Implementation• Individualized Treatment Goals• Ongoing Measurement of Progress• Child-Initiated Teaching Episodes• Environmental Arrangement• Natural Reinforcement to Enhance Motivation• Use of Prompting and Prompt Fading• Balanced Turns within Play Routines• Modeling• Adult Imitation of Child’s Behavior• Broadening Attentional Focus of the Child
Schreibman, Dawson, Stahmer, Landa, Rogers, McGee, Kasari, Ingersoll, Kaiser, Bruinsma, McNerney, Wetherby, & Halladay, 2014
Wetherby, 2017- Page 12

Whatdoweknowabouttoddlertreatments?
Clinician-ImplementedInterventions• RCTsofclinician-implementedinterventionshavehadpromisingeffectsonchild
outcomesofdevelopmentallevel&adaptivebehaviorbutmodesteffectsonautismsymptoms
• Requireconsiderableamountofprofessionaltime,rangingfrom20hours/weekfor2yearsto10hours/weekfor6months
Dawsonetal.,2010;Landa etal,2011
Parent-ImplementedInterventions• RCTsofparent-implementedinterventionshaveincreasedparentresponsivity,
synchronization,andinteractionskillsbuthavenotfoundsignificanteffectsonchildoutcomes.
• Verylowintensityrangingfrom11-24sessionsover3to12months
Carteretal.,2011;Greenetal.,2010;Rogersetal.,2012;Siller etal.,2012;Solomonetal.,2014
Background: Parent Implemented RCTsN Age
(months)Duration Intensity Proximal
EffectsDistalEffects
Carteretal.,2010
62 20 3.5months 8group/3ind sessions
X
Greenetal.,2010
152 24-59 12months 18sessions X
Kasari etal.,2010
42 30 2months 3Xweek X
Rogersetal.,2012
98 21 3months 1Xweek
Solomonetal.,2014
128 30-71 12months 1Xmonth X ADOS%Δin ASD/Autism
Wetherby, 2017- Page 13

Intensitymatters…
…so how do we achieve 25 hours per week in which the child is engaged actively and productively in meaningful activities?
(National Research Council, 2001)
esi.fsu.edu
Community-viable intervention model for toddlers with ASD & their families
Teach parents how to use supports and strategies in everyday activities at home and in the community
Funded byNIMH
Early Social Interaction Project
Wetherby, 2017- Page 14
ESITheoreticalPrinciples1. Afamily-centeredapproachtomeetthefamily’sneeds,
concerns,andprioritiesthroughouttheassessmentandinterventionprocess
2. Embeddedinterventioninnaturalenvironmentstoenhancegeneralizationforthechildandfamily
3. Parent-implemented,activity-basedintervention4. Intensityofprogrammingforatleast25hoursofactive
engagementperweek5. Systematicinstructionusingindividualizedandevidence-
basedstrategieswithmonitoring6. Developmentalapproachtargetingcoredeficitsofautism—
socialinteraction,communication,play,andemotionalregulationusingtheSCERTS curriculum
SCERTS Intervention Curriculum
S- SOCIALC- COMMUNICATIONE- EMOTIONALR- REGULATIONT- TRANSACTIONALS- SUPPORT
Barry Prizant, Amy Wetherby, Emily Rubin, & Amy Laurent
Brookes Publishing © 2006www.scerts.com
Wetherby, 2017- Page 15

CollaborativeExperimentalTreatmentStudyfundedbyNIMHandAutismSpeaks
Florida State University PI- Amy Wetherby
University of MichiganPI- Catherine Lord
esi.fsu.edu
EarlySocialInteractionProject
RCTofEarlySocialInteraction(ESI)ProjectWetherby,Guthrie,Woods,Schatschneider,Holland,Morgan,&Lord,2014
IndividualESIHighIntensity3individualsessionsperweek(2athomeand1inclinicplayroom);reducedto2sessionsperweekinlast3months
GroupESILowIntensity1groupsessionperweek(1educationmeetingand3playgroupsessionspermonth)
82childrenenteredstudyat18monthswithdiagnosisofASD
Comparedeffectsof2parent-implementedinterventionconditions(9months)
Employedacrossoverdesignsothatallfamiliesreceivedbothtreatments.
Wetherby, 2017- Page 16

MeasuringTreatmentOutcomesChildActiveEngagement
• Isthechildwellregulated?• Isthechildactively
participatinginaproductiverole?
• Isthechildengaginginreciprocalsocialinteraction?Ø sociallyconnectedØ shiftinggazetofaceØ respondingtoverbalbidsforinteractionØ initiatingcommunication
• Isthechild’sbehaviorflexible&generative?
The3LayerCake:Teachingstrategies&supportstoparentstopromote
childactiveengagementineverydayactivities
Supports for better skillswModel and build language, play & interactionwExtend activity, child’s roles, & transitions
wAdjust expectations & supportswBalance of interaction and independence
Supports for a common agendawMotivating activity wProductive roles wPredictability
wPositioning wFollow child’s attentional focus
Supports for social reciprocitywPromoting initiation wBalance of turns wNatural reinforcers
wClear message to ensure comprehension
Copyright©2014.TheFloridaStateUniversity.Allrightsreserved.
Wetherby, 2017- Page 17

“EverydayActivityCategories”topromotelearninginthenaturalenvironment
Play with PeopleSocial Games like Peek-a-boo, Rough
and Tumble, Songs & Rhymes
Play with ToysBlocks, Puzzles, Sand box, Playdough,
Cars and Trucks, Ball Games, Baby Dolls
Meals and SnacksPreparation, Eating, Cleanup
CaregivingDressing, Diaper Change, Bath,
Washing Hands, Brushing Teeth
Book Sharing Family Chores Mailbox, Laundry, Care for Pets, Plants
Copyright©2014.TheFloridaStateUniversity.Allrightsreserved.
Wetherby, 2017- Page 18
CourseIntroduction
1. ImprovingEarlyDetection
2. CollaboratingwithFamilies
3. DevelopmentalPerspectives
4. Evidence-basedInterventionStrategies
5. AddressingChallengingBehavior
for Early Intervention Providers
Copyright©2015byFloridaStateUniversity.Allrightsreserved.
1. LibraryofEverydayActivities
2. LibraryofActiveEngagement
3. LibraryofTransactionalSupports
4. LibraryofChildrenandFamilies
5. LibraryofCoachingPractices
TourGuideManualforH2GGuidedTour
LeadingfromtheMiddle
Copyright©2017byFloridaStateUniversity.Allrightsreserved.
for Early Intervention Providers
(Feb)
(Feb)
(Jun)
(Mar)
(Open)
(Open)
(Open)
Wetherby, 2017- Page 19
Tiered Structure for Professional Development of Autism Navigator Specialists
Tier1:CompleteK&SCourse&JoinLearnerCommunity
Tier2: LocalTeamLeadershipRolesinMasteryCourse
Tier3:CertificationtoDocumentImplementationFidelity
Tier4:CertificationasanAN Regional Specialist
Tier5:CertificationasaMasterCoach/GlobalTrainer
for Early Intervention Providers
Strategies for Statewide System Change
1. Regional Team Supports and Strategies to Engage Users§ Establish peer partners in your region§ Encourage intentional discussion groups§ Identify “Autism Navigator Specialists” to complete Mastery level§ Support feeling successful
2. Autism Navigator Learner Community§ Webinars on 1st & 3rd Tuesday of each month to focus on topics
identified by users and application of content§ Annual face-to-face meetings to engage users
3. E-Coaching to Support Fidelity of Implementation§ Autism Navigator LLC will offer e-coaching to provide feedback
and support to teams of Autism Navigator Specialists§ Video review and feedback on SORF, MAETS, fidelity of
implementation, and problem solving on specific cases
for Early Intervention ProvidersLessons from Implementation Science
Wetherby, 2017- Page 20

Autism spectrum disorder (ASD) is a neurodevelopmental disorder defined by persistent deficits in social communication and
social interaction, accompa-nied by restricted, repetitive patterns of behavior, inter-ests, or activities.
The signs of ASD are usually evident in early childhood. Though it is still considered a lifelong diag-nosis, with appropriate early intervention, individuals with ASD can lead produc-tive, inclusive, and fulfilling lives. Many children with ASD do well in school, par-ticipate in activities they en-joy, go on to college, and are employed in adulthood.
For most parents and professionals, ASD can be a very puzzling and complex disorder. Though a great deal of its mystery has yet to be uncovered, we know much more about it than we did 10 years ago. Just as our understand-ing has evolved over the years, so has the way we define, diagnose, and treat ASD.
Are there different types of ASD?ASD used to be called Pervasive Developmental Disorder
(PDD). These terms mean the same thing. PDD is the diagnostic classification in the DSM-IV (4th edition of the most widely used diagnostic manual of mental disorders published by the American Psychiatric Association in 1994). In the DSM-IV, PDD included five types or categories: autistic disorder, Asperger’s disorder, childhood disintegrative disorder, Rett’s syndrome, and pervasive developmental disorder-not otherwise specified (PDD-NOS).
The American Psychiatric Association released the new fifth edition of the DSM in May 2013. In the DSM-5 the term ASD has replaced PDD. Additionally, the DSM-5 does not have any catego-ries under ASD so that all individuals meeting the diagnostic criteria will fall under one autism spectrum. This change was made because research indicates the categories that were under PDD cannot be re-liably distinguished. This means the categories of autistic disorder, Asperger’s disorder, and PDD-NOS will no longer be used—instead the diagnosis of ASD will be used to cover the full spectrum.
How is ASD diagnosed?Diagnosing ASD can be difficult because there are no medical
or blood tests. The diagnosis is based on behavioral symptoms or features. These features include the absence of or delays in typical developmental milestones and the presence of unusual behaviors.
The diagnosis can involve a two-stage process. The first stage is screening, usually by doctors at well-child visits using validated screening checklists that parents fill out. The second stage is a com-prehensive diagnostic evaluation usually conducted by a multidisci-plinary team that gathers information from an interview and struc-tured observation.
Early detection means earlier access to intervention. An expe-rienced professional can make a diagnosis of ASD as early as 18 to 24 months of age, but often ASD is not diagnosed until 3 to 5 years of age or later, after the window of opportunity for very early inter-vention. The American Academy of Pediatrics recommends that all children be screened for ASD at 18 and 24 months of age.
What is Autism Spectrum Disorder?
Wetherby, 2017- Page 21

What are early red flags of ASD in toddlers?The diagnostic features of ASD can be easy to miss in young
children. Looking for possible red flags or early signs may help to find children at risk for ASD, and in need of a diagnostic evalu-ation. If your child shows some of the following red flags, talk to your child’s doctor. If you or your child’s doctor has concerns about possible ASD, ask for a referral to a developmental specialist or you can contact your local early intervention program.
Red Flags of ASD in Toddlers
Social Communication
Limited use of gestures such as giving, showing,waving, clapping, pointing, or nodding their head
Delayed speech or no social babbling/chatting
Makes odd sounds or has an unusual tone of voice
Difficulty using eye contact, gestures, and sounds orwords all at the same time
Little or no pretending or imitating of other people
Stopped using words that they used to say
Uses another person’s hand as a tool (e.g., puttingparent’s hand on a jar for them to open the lid)
Social Interaction
Does not look right at people or hard to get them tolook at you
Does not share warm, joyful expressions
Does not respond when someone calls their name
Does not draw your attention to things or show you things they’re interested in
Does not share enjoyment or interests with others
Repetitive Behaviors & Restricted Interests
Unusual ways of moving their hands, fingers,or whole body
Develops rituals such as lining objects up or repeating things over and over
Very focused on or attached to unusual kinds ofobjects such as strips of cloth, wooden spoons, rocks,vents, or doorstops
Excessive interest in particular objects, actions, oractivities that interferes with social interaction
Unusual sensory interests such as sniffing objects or looking out of the corner of their eye
Over- or under-reaction to certain sounds, textures, orother sensory input
Copyright © 2014 Florida State University. All rights reserved.
Wetherby, 2017- Page 22
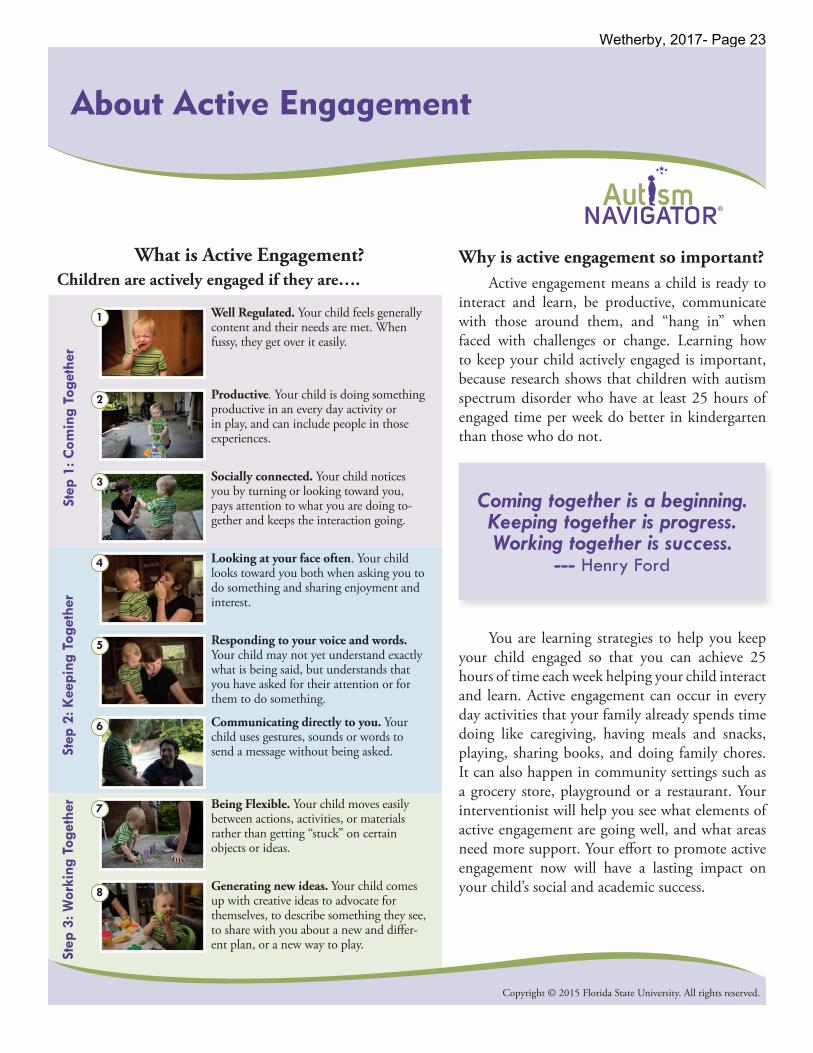
Why is active engagement so important? Active engagement means a child is ready to
interact and learn, be productive, communicate with those around them, and “hang in” when faced with challenges or change. Learning how to keep your child actively engaged is important, because research shows that children with autism spectrum disorder who have at least 25 hours of engaged time per week do better in kindergarten than those who do not.
About Active Engagement
Copyright © 2015 Florida State University. All rights reserved.
You are learning strategies to help you keep your child engaged so that you can achieve 25 hours of time each week helping your child interact and learn. Active engagement can occur in every day activities that your family already spends time doing like caregiving, having meals and snacks, playing, sharing books, and doing family chores. It can also happen in community settings such as a grocery store, playground or a restaurant. Your interventionist will help you see what elements of active engagement are going well, and what areas need more support. Your effort to promote active engagement now will have a lasting impact on your child’s social and academic success.
Well Regulated. Your child feels generally content and their needs are met. When fussy, they get over it easily.
What is Active Engagement?Children are actively engaged if they are….
Productive. Your child is doing something productive in an every day activity or in play, and can include people in those experiences.
Socially connected. Your child notices you by turning or looking toward you, pays attention to what you are doing to-gether and keeps the interaction going.
Looking at your face often. Your child looks toward you both when asking you to do something and sharing enjoyment and interest.
Responding to your voice and words. Your child may not yet understand exactly what is being said, but understands that you have asked for their attention or for them to do something.
Communicating directly to you. Your child uses gestures, sounds or words to send a message without being asked.
Being Flexible. Your child moves easily between actions, activities, or materials rather than getting “stuck” on certain objects or ideas.
Generating new ideas. Your child comes up with creative ideas to advocate for themselves, to describe something they see, to share with you about a new and differ-ent plan, or a new way to play.
Step
1: C
omin
g To
geth
er
Step
2: K
eepi
ng T
oget
her
Step
3: W
orki
ng T
oget
her
Coming together is a beginning. Keeping together is progress. Working together is success.
--- Henry Ford
1
2
3
4
5
6
7
8
Wetherby, 2017- Page 23

Page 1 of 2Copyright © 2015 Florida State University. All rights reserved.
What are Transactional Supports?
The term “Transactional Supports” refers to the supports or strategies used by parents to pro-mote their child’s learning and development. The following evidence-based intervention supports and strategies can be used in everyday activities with your child to promote active engagement and social communication development. These supports are organized into three layers; 1) Sup-ports for a Shared Agenda, 2) Supports for So-cial Reciprocity, and 3) Supports for Better Skills. Like making a layer cake, it’s important to develop the first layer before adding the second and third layers. Below is a suggested order for introduc-ing each support within a layer. Because they are cumulative, later supports rely on earlier supports being in place.
First Layer: Supports for a Shared agenda(so that you and your child are participating in the activity together)
1. A motivating activity is something your child wants to do that includes interesting materials. Activities such as hand washing are necessary but may not be motivating. Knowing that a fun activity is coming after a necessary activity is one way to make a necessary activity motivating. Adding interesting materials or other supports for a shared agenda can also help make necessary activities more interesting or sensible for your child and might even make them more fun.
2. A productive role lets your child know exactly what to do and that they are expected to use materials in an appropri-ate way and actively attend and participate. Roles can be as simple as turning a page, dropping clothes into a hamper from the dryer, or gathering materials for a painting activity.
3. Predictability of the activity lets your child know what is coming next by making the beginning, middle, and end of each activity clear to your child.
4. Positioning yourself so that you are close by, at your child’s level, and face-to-face to make it easier for your child to notice you, look at you, and interact with you.
5. Follow your child’s attentional focus means noticing and talking about what your child is paying attention to, doing, or experiencing. Asking your child to shift their attention to something else is placing more burden on your child’s social attention and can interfere with establishing a shared agenda.
About Transactional Supports
Wetherby, 2017- Page 24

Second Layer: Supports for Social Reciprocity(so that there is a give and take in interaction)
6. Promote child initiation by setting up a reason for your child to communicate, then waiting. When you ask your child to say a word they practice responding- not initiating communication. Natural pauses encourage your child to practice communicating their own ideas.
7. Balance turns so that you take no more than 1 ½ turns for each of your child’s turns. Keep in mind that your turn can be a comment, gesture or action that supports your child to take a turn next. Your child may also take turns using actions, gestures, or words.
8. Natural reinforcers such as offering help, comfort, a favorite snack or toy, shared enjoyment, or shared interest natu-rally reward your child’s communication. Saying “good talking!” has no connection with the intention your child is trying to communicate and therefore does not help your child learn that their words have power and meaning.
9. Clear messages to ensure comprehension make it clear to your child that you expect them to listen to and act on your words. Gestures or other contextual support are offered to ensure that your child understands your message. Language that is optional for your child to listen to may give the impression that the language of others can be “tuned out” or disregarded.
Third Layer: Supports for Better Skills(to promote social communication development)
10. Model language, play, and interaction to help your child know what they could say or do. Model language just above your child’s level, and use their perspective when possible, “as they would say it if they could”. Providing a model of language or behavior builds better skills by example and by giving the turn back to your child. Giving direc-tions or asking questions can provide a more limited response and may not build better skills.
11. Extend the activity, roles, and transitions to build on play, interaction, and connectedness. “Stretching” engaged time spent in activities and expanding roles your child can take on during transitions can add up quickly to more engaged time per week.
12. Adjust expectations and demands by offering more support when your child is struggling, and increasing expectations when things are going well to keep your child moving forward. Over time, you should be able to do less of the “work” and shift more responsibility to your child to keep interaction and communication going.
13. Balance interaction and independence by supporting interaction but also building independence with an eye toward what your child needs to learn in a group setting to prepare for the skills needed in preschool and kindergarten class-rooms.
You can promote your child’s learning and development by putting supports and strategies in place in everyday activities. Soon you will feel confident making every moment an opportu-nity to practice and learn! This allows you, with the support of your EI provider, the opportunity to achieve the intensity needed to support active engagement for your child with ASD. Support-ing your child’s ability to be flexible, to use a variety of materials, easily shift attention between materials or topics and people and not show rigidity or resistance to change, may indicate a good balance between the ability to work alone and to include others, setting the stage for self-directed learning and classroom success.
Copyright © 2015 Florida State University. All rights reserved. Page 2 of 2
Wetherby, 2017- Page 25
© 2016 The Florida State University. All rights reserved.
Child’s Name: ___________________________________________
Examiner: __________________________ Date: _______________
Setting: ____________________________ Age: _______________
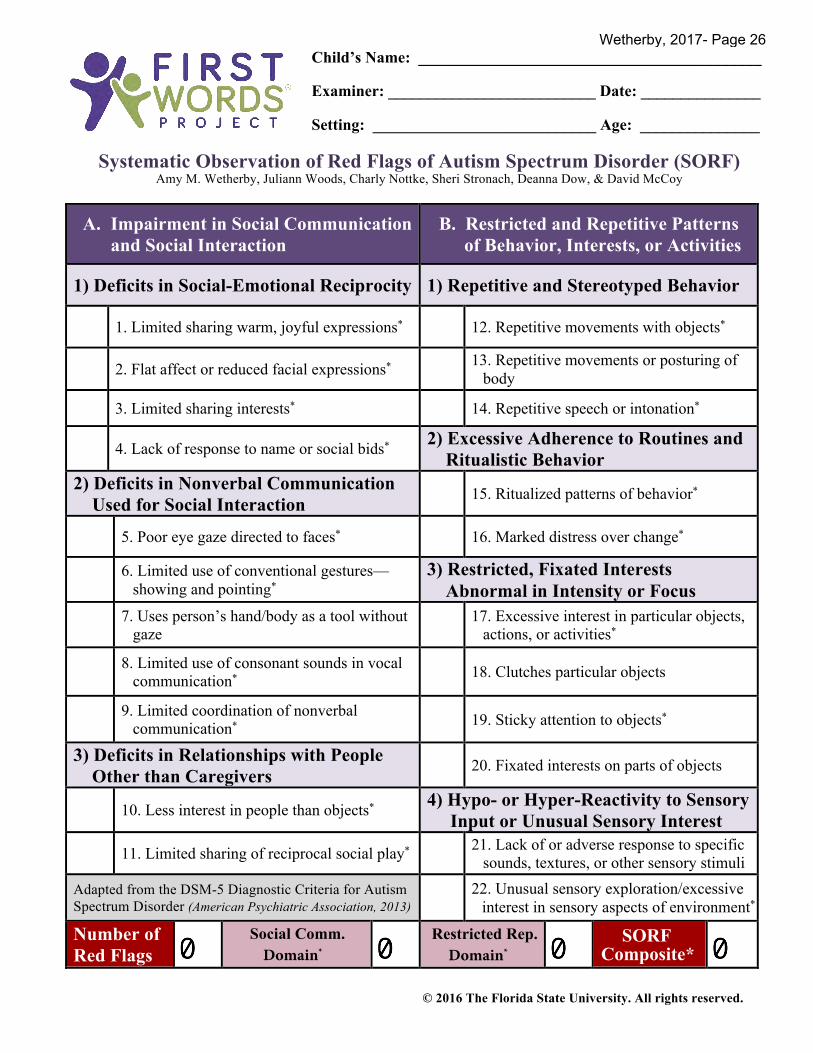
Systematic Observation of Red Flags of Autism Spectrum Disorder (SORF) Amy M. Wetherby, Juliann Woods, Charly Nottke, Sheri Stronach, Deanna Dow, & David McCoy
A. Impairment in Social Communication and Social Interaction
B. Restricted and Repetitive Patternsof Behavior, Interests, or Activities
1) Deficits in Social-Emotional Reciprocity 1) Repetitive and Stereotyped Behavior
1. Limited sharing warm, joyful expressions* 12. Repetitive movements with objects*
2. Flat affect or reduced facial expressions* 13. Repetitive movements or posturing ofbody
3. Limited sharing interests* 14. Repetitive speech or intonation*
4. Lack of response to name or social bids* 2) Excessive Adherence to Routines andRitualistic Behavior
2) Deficits in Nonverbal CommunicationUsed for Social Interaction 15. Ritualized patterns of behavior*
5. Poor eye gaze directed to faces* 16. Marked distress over change*
6. Limited use of conventional gestures—showing and pointing*
3) Restricted, Fixated InterestsAbnormal in Intensity or Focus
7. Uses person’s hand/body as a tool withoutgaze
17. Excessive interest in particular objects,actions, or activities*
8. Limited use of consonant sounds in vocalcommunication* 18. Clutches particular objects
9. Limited coordination of nonverbalcommunication* 19. Sticky attention to objects*
3) Deficits in Relationships with PeopleOther than Caregivers 20. Fixated interests on parts of objects
10. Less interest in people than objects* 4) Hypo- or Hyper-Reactivity to SensoryInput or Unusual Sensory Interest
11. Limited sharing of reciprocal social play* 21. Lack of or adverse response to specificsounds, textures, or other sensory stimuli
Adapted from the DSM-5 Diagnostic Criteria for Autism Spectrum Disorder (American Psychiatric Association, 2013)
22. Unusual sensory exploration/excessiveinterest in sensory aspects of environment*
Number of Red Flags
SORFComposite*
Social Comm. Domain*
Restricted Rep. Domain*
Wetherby, 2017- Page 26