Embed Size (px)
Citation preview

Leukopenia, leukocytosis

Follicular hyperplasia

NEOPLASTIC PROLIFERATIONS OF WHITE CELLS
• Lymphoid neoplasms– The phenotype of the tumor cells resembles
that of normal counterparts
• Myeloid neoplasms– Origin of hematopoietic stem cells that give
rise to cells of the myeloid lineage
• Histiocytoses – Proliferative lesions of macrophages and
dendritic cells

Etiology and pathogenetic factors in white cell neoplasia
• Chromosomal translocations and oncogenes
• Inherited genetic factors
• Virus
• Environmental agents
• Iatrogenic factors

Definition of lymphoid neoplasms
• Lymphoma
– Lymphoid neoplasms present predominantly as solid masses
• Leukemia (lymphoid leukemia)
– Lymphoid neoplasms involve mainly in bone marrow and usually in peripheral blood

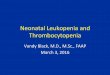
Histology of a lymph node

Secondary Lymphoid Follicle (B-cell)
Interfollicular
zone (T-cell)
Mantle zone
Germinal
center
Dark zone
Light zone
Centrocyte
Centroblast

Development of Lymphocytes

Normal Counterpart of B-cell Neoplasms


Lymphoma Classification
• “Revised European-American Classification of Lymphoid Neoplasms” (REAL) proposed by ILSG in 1994
• World Health Organization (WHO) classification
• Why classification?

Three major categories of lymphoid neoplasms
• B cell lymphomas– Precursor vs. peripheral
• T and NK cell lymphomas– Precursor vs. peripheral
• Hodgkin lymphoma (HL)
• Lymphoma vs. leukemia– Small lymphocyte, lymphoblast, Burkitt

The WHO Classification of the Lymphoid Neoplasms I. Precursor B-Cell Neoplasms
Precursor-B lymphoblastic leukemia/lymphoma
II. Peripheral B-Cell Neoplasms
Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL)
B-cell prolymphocytic leukemia
Lymphoplasmacytic lymphoma (LPL)
Splenic and nodal marginal zone lymphomas
Extranodal marginal zone lymphoma
Mantle cell lymphoma (MCL)
Follicular lymphoma (FL)
Marginal zone lymphoma (MZL)
Hairy cell leukemia
Plasmacytoma/plasma cell myeloma
Diffuse large B-cell lymphoma (DLBCL)
Burkitt lymphoma (BL)

III. Precursor T-Cell Neoplasms
Precursor-T lymphoblastic leukemia/lymphoma
IV. Peripheral T-Cell and NK-Cell Neoplasms
T-cell prolymphocytic leukemia
Large granular lymphocytic leukemia
Mycosis fungoides/Sézary syndrome
Peripheral T-cell lymphoma, unspecified (PTCL, NOS)
Anaplastic large cell lymphoma (ALCL)
Angioimmunoblastic T-cell lymphoma
Enteropathy-associated T-cell lymphoma
Panniculitis-like T-cell lymphoma
Hepatosplenic γ/δ T-cell lymphoma
Adult T-cell leukemia/lymphoma
NK/T-cell lymphoma, nasal type
NK-cell leukemia

V. Hodgkin Lymphoma
Classical subtypes
Nodular sclerosis (NS)
Mixed cellularity (MC)
Lymphocyte-rich (LRC)
Lymphocyte depletion (LD)
Lymphocyte predominance (LP)

Summary of Major Types of Lymphoid Neoplasms
Diagnosis Cell of Origin
Genotype Salient Clinical Features
BL Germinal center B-cell; CD10 expression usually seen
Translocations involving c-myc and Ig loci; usually t(8;14), but also t(2;8) or t(8;22). African (endemic) cases latently infected with EBV
Adolescents or young adults with jaw or extranodal abdominal masses; uncommonly presents as a "leukemia"; aggressive

SLL/CLL

Prolymphocyte

CLL

SLL/CLL

FL

Centrocyte & centroblast

FL (spleen)

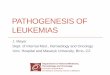
Bcl-2 expression in reactive and neoplastic follicles

DLBCL

DLBCL (spleen)


BL

BL


LPL

MCL

MCL


Mucosa-associated lymphoid tissue (MALT) type-lymphoma
Extranodal marginal zone lymphoma
Postgerminal center memory B-cell
Trisomy 18, t(11;18), t(1;14); latter create MALT1-IAP2 and BCL10-IgH fusion genes, respectively
Arises at extranodal sites in adults with chronic inflammatory diseases; may remain localized; indolent

Mature B cell lymphomas• Epidemiology
– Median age: 6th~7th decades• Mediastinal large B-cell lymphoma: 37• Burkitt lymphoma: 30
– In children• Burkitt lymphoma (BL)• Diffuse large B-cell lymphoma (DLBCL)
– M>F: mantle cell lymphoma– F>M: mediastinal large B-cell lymphoma

Risk factors
• Abnormality of the immune system– Immunodeficiency (HIV, recipient of
transplantation)• BL, DLBCL
– Autoimmune disease• MALT lymphoma

Etiology-- Infectious agents• EBV
– BL (100% in endemic, 40% in others)– lymphomas in immunosuppressed patients
• HHV8– primary effusion lymphoma
• Hepatitis C virus– lymphoplasmacytic lymphoma
• Bacteria– MALT lymphoma (stomach, skin, intestine)


Genetics• Mantle cell lymphoma (MCL)
– t(11;14): Cyclin D1/Bcl-1
• Follicular lymphoma (FL)– t(14;18): Bcl-2
• Burkitt lymphoma (BL)– t(8;14), t(2;8), t(8;22): c-myc
• MALT lymphoma– t(11;18): API-2

Clinical Presentations
• Predominantly disseminated (leukemia)– SLL/CLL, LPL, hairy cell leukemia (HCL),
splenic marginal zone lymphoma, myeloma
• Primary extranodal– MALT lymphoma
• Predominantly nodal– Follicular lymphoma, mantle cell
lymphoma, nodal marginal zone lymphoma

Clinical features and survival
• Indolent & incurable– SLL/CLL, FL: median survival > 5 yrs
• Indolent & curable– MALT lymphoma
• Incurable & aggressive– MCL: median survival 3 yrs
• Aggressive but curable– DLBCL (40% cure rate), BL

Mature T- and NK-cell neoplasms
• Incidence– 12% in the Western world
• Peripheral T-cell lymphoma, unspecified (PTCL-U)• Anaplastic large cell lymphoma (ALCL)
– 39% in Taiwan• Nasal and nasal-type NK/T-cell lymphoma
• Why?– Lower B lymphoma, virus, racial
predisposition

Etiology
• Virus– EBV
• NK/T-cell lymphoma• NK/T-cell leukemia
– HTLV-1• Adult T-cell leukemia/lymphoma
• unknown

PTCL, unspecified

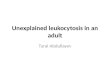
ALCL-hallmark (horseshoe) cells

ALK expression in ALCL


Nasal type NK/T-cell lymphoma
Natural killer cell (common) or cytotoxic T-cell (rare)
No specific chromosomal abnormality; uniformly EBV associated
Adults with destructive extranodal masses, most commonly sinonasal; often accompanied by hemophagocytic syndrome; aggressive

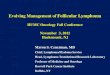
Reed-Sternberg (RS) cell

Characteristics
• About 30% of all lymphomas
• Usually arise in cervical lymph nodes
• The majority in young adults
• Typically localized at presentation• Scattered tumor cells in a background of
inflammatory cells
• The tumor cells are usually ringed by T-cells in a rosette-like manner

Mononuclear variant of RS cell

Lacunar variant

Lymphohistiocytic (L&H) variant

Subclassification• Nodular lymphocyte
predominant (NLPHL)– 5% of all HL– 30~50 y/o male– Most stage I/II– Develop slowly– Frequent relapses– Responsive to Tx– Rarely being fatal– 10 yr survival rate
>90%
• Classical (CHL)
– 95% of all HL– 15~35 & late adult– Neck, mediastinum– 55% stage I/II– 40% systemic
symptoms– EBV association– Curable in the majority– 5 yr survival >85%

NS type

MC type

NLP type

Signals mediate cross-talk between RS and surrounding normal cells

Clinical Differences Between Hodgkin and Non-Hodgkin Lymphomas
Hodgkin Lymphoma Non-Hodgkin Lymphoma
More often localized to a single axial group of nodes (cervical, mediastinal, para-aortic)
More frequent involvement of multiple peripheral nodes
Orderly spread by contiguity Noncontiguous spread
Mesenteric nodes and Waldeyer ring rarely involved
Waldeyer ring and mesenteric nodes commonly involved
Extranodal involvement uncommon
Extranodal involvement common

THANK YOU

HCL

HCL