Embed Size (px)
Citation preview

British Journal of Oral Surgery 17 (1979-80), 91-103
A MODIFIED PRE-AURICULAR APPROACH TO TH E TEMPOROMANDIBULAR JOINT AND MALAR ARCH
ADIL AL-KAYAT, B.D.S., M.MED.SCI., F.D.S.R.C.S., 1 and PAUL BRAMLEY, M.B., CH.B., B.D.S., F.D.S.R.C.S. 2
~ Departrnent of Oral Surgery, University of Baghdad; 2Department of Dental Surgery, University of Sheffield
Summary. In an attempt to improve visibility and safety in the surgical approach to the malar arch and jaw joint, anatomical dissections of 56 facial halves were undertaken. Observations are made on the relationship of the facial nerve bifurcation and its temporal branch to bony landmarks. Attention is drawn to the dangerous area of fusion of the superficial fascia, the superficial layer of temporal fascia and the periosteum of the malar arch. The safety of approaching the malar arch through the pocket formed by the splitting of the lower part of the temporal fascia is emphasised.
Minor modifications to the established pre-auricular approach were made and applied successfully to six sides in five patients.
Introduction
Surgical visibility of the jaw joint and malar arch is often compromised by efforts to protect the facial nerve and its branches. Sometimes it can be a bloody operation and the patient be left with a wide area of sensory loss over the distribution of the auriculo-temporal nerve. It is because of the anatomical difficulties and the search for good cosmetic results that there have been so many widely different surgical approaches to the area.
The various approaches are listed,
(1) Pre-auricular (Risdon, 1934; Blair & Ivy, 1936; quoted by Bellinger, 1940; Milch, 1938; McCann, 1965; Rowe & Killey, 1968; Giles, 1969; Thoma, 1969; Rowe, 1972).
(2) Submandibular (Risdon, 1934; Sleeper, 1952; Ward, 1961). (3) Post-auricular (Bockenheimer, 1920; Axhausen, 1931 ; Alexander, 1975). (4) Closed condylotomy (Ward, 1961). (5) Endaural (Rongetti, 1954; Davidson, 1956; Hosxe, 1972). (6) Intra-oral (Keen, 1909; Silverman, 1925; Wielage, 1928; Lewis, 1953; Dingman
& Natvig, 1964; Sear, 1972; Quinn, 1977). (7) Horizontal incision along the lower border of the malar arch (Balyeat, 1933;
Dingman & Harding, 1951 ; Riessner, 1952; Hueston, 1959). (8) Temporal (Gillies et al., 1927). (9) Through soft tissue laceration or scars (Gillies et al., 1927; Bingham, 1955;
Rowe & Killey, 1968).
Perhaps the most satisfactory and most commonly used method is the combination of a pre-auricular and endaural approach described by Rowe & Killey, (1968) and Rowe, (1972). In an attempt to find further improvements both in access and safety anatomical studies were undertaken.
(Received 26 September 1978; accepted 3 October 1978) 91

92 BRITISH JOURNAL OF ORAL SURGERY
Materials and methods
Observat ions were made on 56 facial halves of hard injected cadavers.
Table I
The age and sex dis t r ibut ion of the subjects
Age No. Sex
50-59 1 1M 60-69 8 4M 4F 70-79 10 4M 6F 80-89 7 7F 90+ 2 1M 1F
The parot id and temporal regions were exposed by using a cont inuous incision start ing in the temporal region as an inverted J pre-auricular incision and cont inu ing a round the auricular a t tachment and downward 2 cm behind the ramus and 2 cm below the body of the mandible. Once the parot id gland was exposed, one of the peripheral branches of the facial nerve was identified and dissected back towards the main t runk. The rest of the branches were then dissected f rom the main t runk towards their te rminal distr ibution.
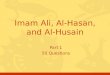
FIG. 1. Point C is the most anterior concavity of the bony external auditory canal. Point Z is the point on the lateral surface of the malar arch midway between its upper and lower border, where
the most posterior significant twig of the temporal ramus of the facial nerve crosses the arch.

A P P R O A C H TO THE T E M P O R O M A N D I B U L A R JOINT AND MALAR ARCH 93
In any surgery of this area it is important to know the location of the main trunk of the facial nerve at its bifurcation and that of the most posterior twig of the temporal ramus of the facial nerve as it crosses the malar arch. The bony landmarks chosen were those which could easily be palpated through the skin or during dissection. The following three sets of measurements were made, (1) The distance between point C, the most anterior concavity of the bony external
auditory canal, and point Z, the point on the lateral surface of the malar arch midway between its upper and lower border, where the most posterior twig of the temporal ramus of the facial nerve crosses the arch (Fig. 1).
(2) The distance between point B, the lowest concavity of the bony external auditory canal, and point F, the point at which the facial nerve bifurcates into the temporo- facial and cervicofacial divisions (Fig. 2).
(3) The distance between point PG (the lowest point of the post-glenoid tubercle) and point F. (Fig. 2.)
For technical reasons, the last two sets of measurements were only carried out in 20 facial halves. All measurements were taken by one observer and the accuracy of observations checked against a second observer. Data for each measurement were grouped according to sex and side of the head and compared using the Student's t test. There was no significant difference between sexes or sides for any measurements and therefore the data from all subjects were grouped. These three sets of measure- ments form part of a more extensive investigation which will be more fully reported elsewhere.
.... //ii/[:::12""-., , , ; . .
:" t" : : - ..-." .... . . i ; ! :.
- ; .
" . ) - " "" i "" "" i
: G ./... I .:" . ' :
, : ,."
~ . . . . - ' : :
FIG. 2. Point B is the lowest concavity of the bony external auditory canal. Point F is the bifurcation of the main trunk of the facial nerve. Point PG is the lowest point of the post-glenoid
tubercle.

94 BRITISH JOURNAL OF ORAL SURGERY
Dur ing the dissections, the great importance of the detailed ana tomy of the temporal fascia was recognised and this, together with a knowledge of the above measurements , formed the basis of a modified approach to the jo in t and malar arch which was then tried out on cadavers and finally used successfully on six sides in five patients.
Results
Measurements. The measurements CZ, BF and P F G are expressed in frequency histograms (Figs. 3 & 4). They show the number of observations, the mean and the range of each individual measurement.
The temporal fascia. Above, this is a single, thick layer at tached to the entire extent of the superior temporal line. Below, at about 2 cm above the malar arch, it divides into two layers, one of which is attached to the lateral and the other to the medial
6
~5 4-
3- E
cz []
I Ho f , , i , t
1.6 1.8 2.0 2.2 0
i i i , i i ~ i i
0.8 1.0 1.2 1.4 3.0 3.5
Distance Icm)
OnOO i i i i i t i
2.4 2.6 2.8
FIO. 3. Frequency histogram of relations of the temporal branch of the facial nerve to the anterior concavity of the external auditory canal - CZ.
Number of observations: 54 Mean: 2.0+0.5 cm Range: 0.8-3.5 cm.
5
4
3
-~ 2 E z 1
1.5
BFEI PGF
1.6 1.7 1.8 1.9 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 2.9 3.0 3.1 3.2 3.3 3.4 3.5
Distance (cm)
I I
Fla. 4. Frequency histogram of the relation: a) The bifurcation of the facial nerve to the lowest concavity of the external auditory canal - BF. b) The bifurcation of the facial nerve to the post-glenoid tubercle - PGF.
BF PGF Number of observations 20 20 Mean 2.3+0.28 cm 3.0+0.31 cm Range 1.5-2.8 cm 2.4-3.5 cm

A P P R O A C H TO THE T E M P O R O M A N D I B U L A R JOINT AND MALAR ARCH 95
Fro. 5. The relationship of the fascial layers to the malar arch.
1. Superficial fascia. 2. Temporal fascia. 3. Medial layer of temporal fascia. 4. Outer layer of temporal fascia. 5. Fatty tissue between the two layers of temporal fascia. 6. Malar arch.
Arrows point to the joint capsule and the condylar neck.
aspect of the periosteum investing the malar arch (Fig. 5). A small quantity of fat, the zygomatic branch of the superficial temporal artery, and the zygomatico-temporal branch of the maxillary nerve are contained between these two layers. At the level of the malar arch, the periosteum not only firmly blends with the outer layer of the temporal fascia, but also with the superficial fascia.
The temporal and zygomatic branches of the facial nerve cross the malar arch and lie within this tough connective tissue representing the fusion of the three layers (Fig. 6). In every case, it was difficult to dissect out the nerves without some minor damage to them.
The anatomical planes of the branches of the facial nerve. The facial nerve forms a large plexus inside the parotid gland. It is important to note that because of the antero- lateral course of the facial nerve, the peripheral branches are located more super- ficially. As the nerves ascend to cross the malar arch, they lie in the dense fibrous tissues described above. As the temporal branch ascends in a supero-anterior direc- tion, it lies, together with the superficial temporal vessels and the auriculo-temporal nerve in the well defined superficial fascia of the temporal region.

96 B R I T I S H J O U R N A L O F O R A L S U R G E R Y
~alp
iscia
Ten
Epi
Ma
'al ,scia
p fascia
of
:h
FIo. 6. Coronal section through the side of the head, anterior to the temporomandibular joint.
Discussion
The measurements. Although statistical analysis is useful in checking the accuracy of measurements, in terms of surgical safety, it is more important to appreciate the extremes of the range of measurements.
The main trunk and condylar neck. BF and P G F measurements were designed to investigate the relationship of the bifurcation of the facial nerve with readily identifi- able landmarks.
At a variable distance f rom the stylo-mastoid foramen, the facial nerve divides and the point of bifurcation lay within 1.5 cm and 2.8 cm below the lowest concavity of the bony external auditory canal and within 2.4 cm and 3.5 cm in an infero-posterior direction f rom the lowest point of the post-glenoid tubercle. These measurements can be used to identify the main trunk and also to avoid it.
The temporo-facial division and the temporal branches. The temporo-facial division of the facial nerve and the most posterior filament of the temporal branch always lie anterior to a line drawn between the point of the bifurcation to the post-glenoid tubercle (Fig. 2). The CZ measurement was designed to establish the safe extent of an incision along the malar arch. The nerve was on average 2.0 cm from the anterior concavity of the external auditory canal. However, in individual cases, the nerve approached as near as 0.8 cm and as far anteriorly as 3.5 cm. Protection of the tern-

APPROACH TO THE TEMPOROMANDIBULAR JOINT AND MALAR ARCH 97
poral branch could not be guaranteed if an incision directly down to the malar arch was extended more than 0.8 cm in front of the anterior border of the external auditory canal.
The temporal fascia. The difficulty we found in dissection of the temporal nerve filaments at the level of the malar arch is consistent with Riessner's (tO52) observa- tions. Paturet (1951), Rouvi6re (1959) and Loeb (1970) have also drawn attention to the relationship of the nerve filaments to the dense fusion of periosteum, temporal fascia and superficial fascia. It is therefore essential that the malar arch and temporo- mandibular joint should be approached deep to this fibrous fusion, either deep to both layers or by exploiting the surgical plane between the two layers of temporal fascia. Fig. 7 shows that the superficial fascia in the temporal region is a well defined structure and could be confused with the more deeply placed temporal fascia. The temporal fascia must be unequivocally identified and the easy plane of separation between the temporal fascia and the superficial fascia exploited (Gonzalez-Ulloa, 1962; Loeb, 1970).
A surgical approach
The anatomical features described above were applied to an approach to the malar arch and joint which gives excellent visibility with safety, but at the price
FI~. 7. The arrow points to the plane of separation of the temporal fascia and the superficial fascia.

98 BRITISH JOURNAL OF ORAL SURGERY
of a longer incision and wider exposure than is conventional. It differs from Rowe's (1972) description in the positioning of the skin incision and that through the temporal fascia.
The skirt incision is question mark-shaped (Figs. 8 & 9) and begins about a pinna's length away from the ear, antero-superiorly just within the hair line and curves backwards and downwards well posterior of the main branches of the temporal vessels till it meets the upper attachment of the ear. The incision then follows the attachment of the ear and just endaurally as described by Rowe (1972).
The temporal incision must be carried through the skin and superficial fascia to the level of the temporal fascia. The nerve filaments run in the superficial fascia and it is very important that the full depth of this fascia is reflected with the skin flap. Blunt dissection in this plane is carried downwards to a point about 2 cm above the malar arch where the temporal fascia splits. The pocket formed by the division con- tains fatty tissue which is easily visible through the thin lateral layer (Fig. 10). Beyond this point there should be no attempt at further dissection of the superficial fascia from the temporal fascia.
Starting at the root of the malar arch, an incision running at 45 ° upwards and for- wards is made through the superficial layer of the temporal fascia. Once inside this pocket, the periosteum of the malar arch can be safely incised and turned forward as one flap with the outer layer of temporal fascia, superficial fascia containing the nerves and skin (Fig. 11). The pocket can be developed anteriorly as far as the posterior
Post branch superf ic ial temporal a
• /
Branches of facial n
~kin incmion /
"" Tragus
Lower limit of skin incision
/
FIG. 8. Skin incision in relation to the underlying structures.

A P P R O A C H TO T H E T E M P O R O M A N D I B U L A R J O I N T A N D M A L A R A R C H 99
FIG. 9. Skin incision at operation.
border of the frontal process of the malar bone and posteriorly joined to the pre- auricular dissection which follows closely the cartilagenous external auditory canal beneath the glenoid lobe of the parotid gland and the superficial temporal vessels (Fig. 12). A small tortuous branch, the auricular artery, runs backwards from the superficial temporal artery to the ear. The middle temporal artery which comes off the superficial temporal artery perforates the temporal fascia to supply temporalis muscle. These should be divided and ligated.
Proceeding downwards from the lower border of the arch and articular fossa, the tissues lateral to the joint capsule are dissected and retracted. The base of the neck of the condyle can be exposed. The bifurcation of the facial nerve is not nearer than 2.4 cm in an infero-posterior direction from the post-glenoid tubercle. Care is needed not to extend deep dissection below the lower attachment of the ear.
Repair of the layers presents no problems. The incised outer layer of the temporal fascia can be repaired entirely without tension (Fig. 13). This is in marked contrast to the near impossibility of approximating the temporal fascia if it is incised at a higher level, where it is a single layer of tissue.
In all the cadavers and the adult patients the two layers of the temporal fascia and the pocket between them were easily identified. The one child in the group had a long

100 BRITISH JOURNAL OF ORAL SURGERY
Fro. 10. Arrow points to the fat lobules between the two layers of the temporal
fascia.
FIG. 11. Coronal section through the side of the head anterior to the temporo-mandibular joint after re-
flection of the pre-auricular flap.

A P P R O A C H TO THE T E M P O R O M A N D I B U L A R JOINT AND MALAR A R C H 10l
FIG. 12. Arrows mark the incision line of the superficial layer of temporal fascia. The malar arch is exposed after reflecting periosteum, lateral layer of temporal fascia and superficial fascia as one
layer (1).
standing bi-lateral ankylosis. In this case the two layers could not be distinguished. The need to cut through the combined layer in order to approach the malar arch did not create any problems of repair under tension when carried out at this low level.
The minor modifications of the pre-auricular approach described above have resulted in the following advantages,
(1) There is minimal bleeding and less sensory loss. The posterior placement of the skin incision and its wide backwards and upwards sweep spares the main branches of vessels and nerves.
(2) Fascial places are easily identified.
(3) There is excellent visibility. This is partly due to the large flap and partly because the unyielding temporal fascia is not reflected with the skin as in the approach described by Rowe and Killey (1968).
(4) The potential complications of muscle herniation and fibrosis are avoided. The muscle is never exposed and the superficial layer of temporal fascia can be closed without tension.

102 BRITISH JOURNAL OF ORAL SURGERY
FIG. 13. Tensionless closure of the lateral layer of temporal fascia (2). Arrows show the suture knots. Cartilage of the tragus marked 1.
(5) There is r emarkab ly litt le pos t -opera t ive d i scomfor t or swelling.
(6) A good cosmet ic resul t is achieved except in the very bald .
(7) The technique is easily teachable and speedi ly executed.
Acknowledgements
We should like to thank Mr R. Cousins, Department of Medical Illustration, Charles Clifford Dental Hospital, Sheffield, and Mr P. Elliott, Department of Medical Illustration, Hallamshire Hospital, Sheffield, for their assistance in producing the illustrations.
References
Alexander, R. W. (1975). Post-auricular approach for surgery of the temporo-mandibular articula- tion. Journal of Oral Surgery, 33, 346.
Axhausen, G. (1931). De operative freilegung des kiefergelenks. Chirnrg, 3, 713. Balyeat, F. S. (1933). Depressed fractures of the zygoma. American Dental Association Journal, 20,
168. Bellinger, D. H. (1940). Temporo-mandibular joint ankylosis and its surgical correction. Journal of
the American Dental Association, 27, 1563.

A P P R O A C H TO THE TEMPOROMANDIBULAR JOINT AND MALAR ARCH 103
Bingham, C. B. (1955). The fractured malar. Oral Surgery, Oral Medicine and OralPathology, 8, 13. Blair, V. P. & Ivy, R. H. (1936). Essentials of Oral Surgery, p. 374. St Louis: Mosby. Bockenheimer, R. (1920). Eine neue methode zur freilegung der keifergelenke ohne sichtbare narben
unde ohne verletzung des nervus facialis. Zentralblatt fiir Pathologie und Chirurgie, 47, 1560. /)avidson, A. S. (1956). Endaural condylectomy. British Journal of Plastic Surgery, 8, 64. Dingman, R. O. & Harding, R. L. (1951). Treatment of malunion fi'actures of facial bones. Plastic
and Reconstructive Surgery, 7, 505. Dingman, R. O. & Natvig, P. (1964). Surgery of facial fractures. Philadelphia: Saunders. Giles, H. V. (1969). A useful incision to the parotid gland and fractures of the mandible. International
Surgery, 51, 76. Gillies, H. D., Kilner, T. P. & Stone, D. (1927). Fractures of the malar-zygomatic compound with a
description of a new X-ray position. British Journal of Surgery, 14, 651. Gonzalez-Ulloa, M. (1962). Facial wrinkles, integral elimination. Plastic and Reconstructive Surgery,
29, 658. Hosxe, G. (1972). Une vole d'abord de l'articulation temporomandibulaire. Revue de Stomatologie
et de Chirurgie Maxillo-faciale, 73, 375. Hueston, J. T. (1959). The surgical exposure of the dislocated mandibular condyle. British Journal of
Plastic Surgery, 12, 275. Keen, W. W. (ed.) (1909). Surgery, its principles andpraetiee. Vol. 2, p. 146. Philadelphia: Saunders. Lewis, G. K. (1953). Treatment of old depressed fractures of the zygoma. Journal of Oral Surgery,
I I , 101. Loeb, R. (1970). Techniques for preservation of the temporal branches of the facial nerve during
face lift operations. British Journal of Plastic Surgery, 23, 390. McCann, C. F. (1965). Bilateral subcondylar osteotomy. Report of case. Journal of Oral Surgery,
23, 240, Milch, H. (1938). Bayonet incision for temporo-mandibular arthrotomy. American Journal of Ortho-
dontics and Oral Surgery, 24, 287. Paturet, G. (1951). Traite d'Anatomie Humaine. Tome I. Paris: Masson. Quinn, J. H. (1977). Lateral coronoid approach for intra-oral reduction of fractures of the zygomatic
arch. Journal of Oral Surgery, 35, 32•. Riessner, D. (1952). Surgical procedure in turnouts of the parotid gland, Archives of Surgery, 65,
831. Risdon, F. (1934). Ankylosis of the temporo-mandibular joint. Journal of the American Dental
Association, 21, 1933. Rongetti, J. R. (1954). Menisectomy: a new approach to the temporo-mandibular joint. Archives of
Otolaryngology, 60, 566. Rouvi6re, H. (1959). Anatomica Humana Descriptiva Topografica. Tome I. Madrid. Rowe, N. L. (1972). Surgery of the Temporo-mandibular Joint. Proceedings of the Royal Society of
Medicine, 65, 383. Rowe, N. L. & Killey, H. C. (1968). Fractures of the Facial Skeleton. 2nd ed. Baltimore: William &
Wilkins. Sear, A. J. (1972). Intra-oral condylectomy applied to unilateral condylar hyperplasia. British Journal
of Oral Surgery, 10, 143. Silverman, S. L. (1925). A new operation for displaced fractures of the neck of the mandibular
condyle. Dental Cosmos, 67, 876. Sleeper, E. L. (1952). Open reduction of condylar fracture. Oral Surgery, Mediehze and OralPathology,
5,4. Thoma, K. H. (1969). Oral Surgery. 5th ed., Vol. I, p. 88. St. Louis: Mosby. Ward, T. G. (1961). Surgery of the Mandibular Joint. Annals of the Royal College of Surgeons of
England, 28, 139. Wielage, M. F. (1928). New method in reducing fracture of the zygomatic arch. American Dental
Association Journal, 15, 1228.





![Technical report 1 Raffi Kayat|Structural · 2011-09-23 · [TECHNICAL REPORT 1 RAFFI KAYAT|STRUCTURAL] September 23, 2011 Semptember, 23rd 2011 J.. yrd Alzheimer’s enter & Research](https://img.pdfslide.us/doc/110x75/5e6f53bc3b16a5086937661a/technical-report-1-raffi-kayat-2011-09-23-technical-report-1-raffi-kayatstructural.jpg)
![Tampa, Florida January 12, 2012 Faculty Advisor: Dr. Ali ... · [THESIS PROPOSAL 1ST REVIEW RAFFI KAYAT|STRUCTURAL] January 12, 2012 January 12, 2012 J.. yrd Alzheimer’s enter &](https://img.pdfslide.us/doc/110x75/5b030a857f8b9a4e538bbc06/tampa-florida-january-12-2012-faculty-advisor-dr-ali-thesis-proposal-1st.jpg)

![Technical report 2 Raffi Kayat|Structural · 2011-10-19 · [TECHNICAL REPORT 2 RAFFI KAYAT|STRUCTURAL] October 19, 2011 October 19, 2011 J.. yrd Alzheimer’s enter & Research Institute](https://img.pdfslide.us/doc/110x75/5e7cc574cb60d06ed55b6a72/technical-report-2-raffi-kayat-2011-10-19-technical-report-2-raffi-kayatstructural.jpg)









![[Al-Qadaa And Al-Qadar] Fate And Destiny](https://img.pdfslide.us/doc/110x75/55587e4fd8b42a5d328b4940/al-qadaa-and-al-qadar-fate-and-destiny.jpg)