Embed Size (px)
Citation preview

/
Age-dependent effects in the transmission and control of COVID-19 epidemics
Authors: Nicholas G. Davies 1* , Petra Klepac 1^ , Yang Liu 1^ , Kiesha Prem 1 , Mark Jit 1 , CMMID
COVID-19 working group, Rosalind M Eggo 1*
The CMMID COVID-19 working group 1 is: Carl A B Pearson, Billy J Quilty, Adam J
Kucharski, Hamish Gibbs, Samuel Clifford, Amy Gimma, Kevin van Zandvoort, James D
Munday, Charlie Diamond, W John Edmunds, Rein MGJ Houben, Joel Hellewell, Timothy W
Russell, Sam Abbott, Sebastian Funk, Nikos I Bosse, Fiona Sun, Stefan Flasche, Alicia
Rosello & Christopher I Jarvis. Order of working group determined at random.
1 Department of Infectious Disease Epidemiology, London School of Hygiene & Tropical
Medicine, Keppel Street, WC1E 7HT
^ these authors contributed equally
* correspondence to Rosalind M Eggo [email protected] or Nicholas G Davies
The COVID-19 pandemic has shown a markedly low proportion of cases among
children. Age disparities in observed cases could be explained by assortative mixing
patterns and reactive school closures which decrease mixing between children, or by
children exhibiting lower susceptibility to infection, or by children having a lower
propensity to show clinical symptoms. We formally test these hypotheses by fitting an
age-structured mathematical model to epidemic data from six countries, finding
1
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
strong age dependence in the probability of developing clinical symptoms, rising
from around 20% in under 10s to over 70% in older adults. We find that interventions
aimed at halting transmission in children may have minimal effects on preventing
cases depending on the relative transmissibility of subclinical infections. Our
estimated age-specific clinical fraction has implications for the expected global
burden of clinical cases because of demographic differences across settings. In
younger populations, the expected clinical attack rate would be lower, although it is
likely that comorbidities in low-income countries will affect disease severity. Without
effective control measures, regions with older populations may see disproportionally
more clinical cases, particularly in the later stages of the pandemic.
The outbreak of COVID-19 caused by a novel coronavirus has shown a markedly low
proportion of children among reported cases from China 1,2 and other countries 3,4 , a feature
shared with the 2003 SARS epidemic 5 but not with the 2009 influenza A/H1N1p pandemic 6,7 .
There are not only relatively few COVID-19 cases reported in children, but more generally an
increased number of cases and risk of severe disease as age increases 8,9 . Understanding
the role of age in transmission and disease severity is critical for determining the likely
impact of social-distancing interventions for decreasing transmission, especially those aimed
at schools, and for estimating the expected global disease burden.
There are at least three hypotheses that could give rise to the age gradient in observed
COVID-19 cases in China. First, the contact patterns and demographics of China, and
Wuhan in particular, could have resulted in fewer children being infected. The outbreak was
linked to the Huanan Market in Wuhan City, China, and early cases were in older adults 10 .
Assortative mixing between adults could therefore have reduced transmission to children in
the very early stages of the outbreak. The subsequent closure of schools on 12th January
2
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
2020 for the Lunar New Year holiday could have reinforced this effect. Children tend to make
more social contacts than adults 11 and hence, all else equal, contribute more to transmission
in the community than adults 12,13 . This is why school closures are considered a key
intervention for epidemics of respiratory infections 8 , and without them, one would expect a
higher number of infected children. There is also a low proportion of children in China (21%
under 18 14 ), which would decrease the relative proportion of cases seen in children. Outside
of China, COVID-19 outbreaks may have been initially seeded by working-age travellers
entering the country 15,16 , producing a similar excess of older individuals in early phases of
local epidemics.
Second, there could be age-varying susceptibility to infection by SARS-CoV-2, where
children may be less susceptible to becoming infected on contact with an infectious person.
This would further reduce cases among children, and potentially lower transmission in the
population overall. Decreased susceptibility could result from immune cross-protection from
other coronaviruses, or non-specific protection resulting from recent infection by another
respiratory virus 17 of which children have higher rates 18,19 .
Third, children may be as susceptible to SARS-CoV-2 infection as other individuals, but may
more frequently experience milder or no symptoms. Such age-dependent variation in
severity has been observed for other respiratory virus infections 20 , including SARS 14,15 . For
COVID-19, there are indications of age dependence in severity 8 and mortality 21 of reported
cases 21 , which could extend to severity and likelihood of clinically reportable symptoms on
infection. These “subclinical” infections are more likely to remain undetected and would lead
to a reduction in reported cases among children, but children could still be capable of
transmitting the virus to others, potentially at lower rates than individuals exhibiting clinical
3
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
infections, as shown for influenza 22 . Subclinical cases are sometimes called “asymptomatic”
but very mild symptoms may not be noticed, even though they occur.
Distinguishing which of these hypotheses is most supported by available data has important
implications for policies that aim to control transmission 23 , especially through interrupting
child-driven transmission. For example, the impact of school closures depends on the role
and importance of children in the epidemic. Additionally, if the number of infections or cases
depends strongly on the role of children, countries with different age distributions could
exhibit substantially different epidemic profiles and overall impact of COVID-19 epidemics.
The role of children in transmission in Wuhan
We tested three hypotheses—(1) no age variation in susceptibility or severity, with the age
distribution of cases driven by age-dependent contact patterns alone; (2) varying
susceptibility to infection by age; and (3) varying clinical fraction by age—using an
age-structured dynamic transmission model (see Methods) with heterogeneous contact rates
between age groups drawn from social contact surveys in Shanghai 17 . We generated model
variants for each hypothesis ( Fig 1a ) and fitted to three data sources from the early epidemic
in Wuhan for each hypothesis ( Fig, 1b, 1c ). We included school closures, for which we
decreased the school contacts of children. We also estimated the effect of the holiday
period, and the travel and movement restrictions in Wuhan, on transmission ( Fig 1d ). We
found that under each hypothesis, the basic reproduction number R 0 was 3.2–3.6 initially,
was inflated 1.2–1.5-fold during the pre Lunar New Year holiday period, and then fell by
80–95% during restrictions in Wuhan, which brought R 0 below 1 ( Fig 1e ).
All model variants fitted the daily incident number of confirmed cases equally well ( Fig 1f ).
However, hypothesis 1 did not reproduce the observed age distribution of cases,
overestimating the number of cases in children and underestimating cases in older adults
4
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
( Fig 1g ). Hypotheses 2 and 3 fitted the age distribution of cases, but each implied a very
different fraction of subclinical infections by age, with much higher numbers of subclinical
infections under hypothesis 2 (Fig 1h) . Comparison using Deviance Information Criterion 6
(DIC) showed that hypothesis 2 (DIC: 691) and 3 (DIC: 558) were preferred over hypothesis
1 (DIC: 880), and hypothesis 3 was better supported than hypothesis 2.
Under hypothesis 2, where the severity was equal by age, 20% of both clinical and
subclinical infections occurred in the 70-100 year old age group ( Fig 1h ). Under hypothesis
3, 20% of clinical cases but less than 5% subclinical cases are in this group. Recent work
has demonstrated an age-dependent severity in hospitalised confirmed cases 24,25 , which
suggests that a high rate of subclinical infection in older adults may not be realistic. Close
follow-up of contacts of cases in Shenzhen, China, found that children were infected at the
same rate as adults 16 , lending more weight to hypothesis 3. Additionally, evidence of
increased severity by age 19 suggests that clinical signs are more likely in older adults, which
further decreases the plausibility of hypothesis 2.
5
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
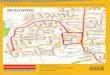
Fig. 1. Comparing the fit of hypotheses 1, 2, and 3 when fitted to data from Wuhan City, China. (a) Model diagram showing duration of disease states, where d parameters represent the duration of time in each disease state and y i is the fraction of infections that are clinical in age group i (see Methods). (b) Susceptibility by age for the three hypotheses. Age-specific values were estimated for hypothesis 2 and all ages had equal susceptibility for hypothesis 1 and 3. Susceptibility is measured as the probability of infection on contact with an infectious person. (c) Clinical fraction ( y i ) by age for the 3 hypotheses. Age-specific values were estimated for hypothesis 3 and all ages were equal for hypothesis 1 and 2. (d) Fitted contact multipliers for holiday and restricted periods for each hypothesis showed an increase in non-school contacts beginning on January 12th (start of Lunar New Year) and a decrease in contacts following restrictions on January 23rd. (e) Estimated R 0 values under each hypothesis. The red barplot shows the inferred window of spillover of infection. (f) Incident reported cases (black), and modelled incidence of clinical cases for the three hypotheses as fitted to the cases reported by China Centers for Disease Control 1 with onset on or before February 1st, 2020. Line marks mean and shaded window is the 95% highest density interval (HDI). (g) Age distribution of cases by onset date as fitted to the age distributions reported by Li et al. 26 Data are shown in the hollow bars, and model predictions in filled bars, where the dot marks the mean posterior estimate. (h) Inferred distribution of subclinical cases by age under each hypothesis. Credible intervals on modelled values show the 95% HDIs; credible intervals on data for panels d-f show 95% HDIs for the proportion of cases in each age group.
Estimating the age-specific clinical fraction
Since the initial outbreak in Wuhan, the virus has spread to other regions within China and
internationally. Local epidemics have exhibited a less extreme, but still marked lack of
reported cases among children. The expected proportion of children infected depends on
6
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
mitigation measures in place in each region, and is expected to be lower in regions which
have closed schools.
Using the best fitting and most biologically plausible hypothesis, hypothesis 3 — age-varying
clinical fraction — we estimated the age-specific clinical fraction for 32 settings across six
countries by using the stationary distribution of the next generation matrix to reproduce the
locally-reported age distribution of cases compiled from a variety of sources (Fig 2a) . We
used setting-specific demographics, measured contact matrices where possible, and
synthetic contact matrices otherwise 27 . The age-dependent clinical proportion was markedly
lower in younger age groups in all regions (Fig 2b), with 20% of infections in children under
10 resulting in clinical cases, rising to over 70% in adults over 70 in the consensus age
distribution estimated across all regions. To determine whether this distribution was capable
of reproducing epidemic dynamics, we fitted our dynamic model to the incidence of clinical
cases in Beijing, Shanghai, South Korea and Italy ( Fig 2c ). The consensus age-specific
clinical fraction was largely capable of reproducing the age distribution of cases, although
there are some outliers, for example the 20-30 age group in South Korea. This could be the
result of clustered transmission within a church group in this country 4 . The predicted age
distribution of cases for Italy is also less skewed towards older adults than reported cases
show, suggesting potential differences in age-specific testing in Italy 28 . Locally-estimated
age-varying clinical fraction captured these patterns more precisely (Fig. 2c) .
7
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
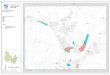
Fig 2. Estimating age-specific symptomatic rate from age-specific case counts for 6 countries. (a) Age-specific reported cases from 13 provinces of China, 12 regions of Italy, Japan, Singapore, South Korea, and Ontario, Canada. Hollow bars are data and colour is model fit with 95% HDI. (b) Fitted mean and 95% HDI for the age distribution in clinical fraction for all countries. (c) Fitted incidence of confirmed cases and resulting age distribution of cases using either the consensus (grey) or country-specific (colour) age-specific clinical fraction from b.
Impact of school closures under different demographics and subclinical
infectiousness
School closures during epidemics 29,30 and pandemics 31,32 aim to slow the spread of infections
by decreasing transmission amongst children 12 . School closures, which have been used
during influenza pandemics 31 , can decrease cases in children, but may also have
whole-population effects if children play a major role in transmission. The impact will depend
on the fraction of the population that are children and the contacts they have with other age
groups. Using schematic values 7 for pandemic influenza and our inferred values for
COVID-19 (Figure 3a) we compared epidemics in three cities with very different
demography: Milan (Italy, high median age), Birmingham (UK, intermediate median age),
8
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
and Bulawayo (Zimbabwe, low median age) (Fig 3b) , using measured contact matrices for
each country. There were many more clinical cases for COVID-19 than influenza in all cities,
with relatively more cases in children in the influenza-like scenario, and more cases in adults
in simulated COVID-19 epidemics ( Fig 3c) . More clinical cases were seen in older adults in
Milan compared with the other cities, and a markedly younger age distribution in clinical
cases in Bulawayo. Using the same age-dependent clinical fraction drawn from high and
upper-middle income countries in low and lower-middle income countries (LMIC) may
underestimate clinical cases due to the presence of comorbidities.
To fully explore the effect of school closure we simulated 3 months of school closures with
varying infectiousness of subclinical cases, at either 0, 0.25, 0.5 or 0.75 times the
infectiousness of clinical cases ( Fig 3d) . We found that school closures decreased peak
incidence slightly for influenza-like infections, and delayed the peak substantially. For
COVID-19 epidemics, the delay and decrease of the peak was smaller, and this was
especially the case in Bulawayo, which has the highest proportion of children (Fig 3e) .
Because children exhibit more subclinical cases for COVID-19, school closures were more
effective at reducing transmission of COVID-19 when the subclinical infectiousness was
assumed to be higher (Fig 3f) .
9
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
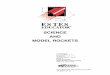
Fig. 3. Effect of school closure under different demographics and subclinical infectiousness. (a) Age dependence in clinical fraction (severity) and susceptibility to infection on contact for COVID, and for the schematic influenza-like scenarios (simplified, based on 7 ) considered here. (b) Age structure for the 3 exemplar cities. (c) Age-specific attack rate for COVID-19 and influenza-like infections, assuming 50% subclinical infectiousness. (d) Daily incidence of clinical cases in exemplar cities for COVID-19 versus influenza-like infections. R 0 is fixed at 2.4. The rows show the impact of varying the infectiousness of subclinical infections to be 0%, 25%, 50%, or 75% as infectious as clinical cases while keeping R 0 fixed. (e) Change in peak timing and peak cases for the three cities, for either COVID-19 or pandemic influenza. (f) Change in median COVID-19 peak timing and peak cases for the three cities,depending on the infectiousness of subclinical infections.
Implications for global preparedness
Strong age dependence in the fraction of COVID-19 infections that become clinical cases
has implications for the projected global burden. Simulating COVID-19 outbreaks in 146
capital cities, we found that the total expected number of clinical cases in an unmitigated
epidemic varied between countries depending on the median age of the population, which is
a proxy for the age structure of the population. The total clinical attack rate was higher, and
the peak height of the epidemic was greater, in older populations ( Fig 4a ). By contrast, the
number and peak of subclinical infections was lower in older populations ( Fig 4b ). The mean
estimated basic reproduction number, R 0 , was higher in cities with a lower median age ( Fig
4c ), because of the greater proportion of children and the higher number of contacts made
by children compared to adults. We applied the same age-dependent clinical fraction to all
10
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
countries, but the relationship between age and clinical symptoms may be different in
different countries, perhaps because of the age distribution of comorbidities, or the presence
of other possible comorbidities, such as HIV 33 . If the relationship between clinical fraction
and age skews younger in low and lower-middle income countries, there would be higher
clinical attack rates in these countries (Supplementary Section 4).
The expected age distribution of cases shifted substantially over time, where in the early
phase of the epidemic, the clinical case distribution tended to be skewed to younger ages,
and the late phase showed more cases in older individuals ( Fig 4d ). This impacts
projections for likely healthcare burdens at different phases of the epidemic, particularly
because older individuals tend to have higher healthcare utilisation on infection 1 ( Fig 4e ).
Fig. 4. Implications for global preparedness. (a) Expected clinical case attack rate (mean and 95% HDI), and peak in clinical case incidence for 146 countries in the Global Burden of Disease (GBD) country groupings 34 for an unmitigated epidemic. (b) Expected sub clinical case attack rate, and peak in subclinical cases. (c) Estimated basic reproduction number (R 0 ) in the capital city of each country assuming age-specific clinical fraction shown in Fig. 2b and 50% infectiousness of subclinically infected people. (d) Mean age of clinical cases on each day of an unmitigated epidemic in the 146 countries, and the epidemic curve for those epidemics. The epidemics are aligned at the peak, and colours mark the GBD groupings in a. (e) Age distribution of the first third and last third of clinical cases for 146 countries in GBD country groupings.
11
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
Conclusions We have shown a strong age dependence in the probability of displaying clinical symptoms
for COVID-19, from around 20% in under 10s, to over 70% in older adults. Given evidence of
a stark age gradient in severity 8 and mortality 21,28 , and recent studies of close follow up of
children at risk of infection 16 showing that infection was frequent in all age groups, the
plausibility of age-specific severity is higher than age-specific susceptibility to infection. For a
number of other pathogens, there is evidence that children (except for the very youngest)
have lower rates of symptomatic disease 12 and mortality 26 . For these reasons, we find that
age-specific clinical fraction is more supported than age-specific susceptibility to infection.
Serological surveys will provide critical information on the true distribution of subclinical
infections.
The age-specific distribution of subclinical infection we have found is similar in shape (but
larger in scale) to that generally assumed for pandemic influenza. However, for the 2009
influenza A/H1N1p pandemic, the age-specific susceptibility to infection was lower in older
individuals compared to COVID-19. These differences have a large effect on how effective
school closures may be in limiting transmission, delaying the peak of expected cases, and
decreasing the total and peak number of cases. For COVID-19, school closures are likely to
be much less effective than for influenza-like infections where children play a more
substantial role in transmission.
It is critical to determine how infectious subclinical infections are compared to clinical
infections in order to properly assess predicted burdens both with and without interventions.
It is biologically plausible that milder cases are less transmissible, for example, because of
an absence of cough 28,29 , but direct evidence is limited 35 . If those with subclinical infection
are similarly efficient transmitters of infection compared to those with clinical infections, the
12
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
overall burden in the groups at risk of severe disease, primarily older populations for
COVID-19 21 , remains high. If those with subclinical infections are (much) less efficient at
transmitting, then the overall contribution to the burden of clinical disease in the population
may be proportionally lower. At the same time, lower relative infectiousness would reduce
the impact of interventions targeting younger ages, such as school closure. By analysing
epidemic dynamics before and after school closures, it may be possible to estimate the
infectiousness of subclinical infections, however this will rely on granular data by age and
time.
A great deal of concern has been directed toward the expected burden of COVID-19 in low
and middle income countries (LMIC), which have lower population median age than many
high income countries. Our results show that these demographic differences, coupled with a
lower symptomatic fraction in younger ages, can result in proportionally fewer clinical cases
than would be expected in higher-income countries with flatter demographic pyramids. This
should not be interpreted as few cases in LMIC, because the projected epidemics are still
very large, resulting in high numbers infected. Moreover, the particular relationship found
with age here is drawn from high income countries, primarily in East Asia, and may reflect
not only age, but also the increasing frequency of comorbidities with age. This relationship,
therefore, may differ in LMIC for two key reasons: first, the distribution of non-communicable
comorbid conditions—which are already known to increase the risk of severe disease from
COVID-19 21 may be differently distributed by age, often occurring in younger age groups 34 ,
along with other possible risk factors such as undernutrition 36 ; and second, communicable
comorbidities such as HIV 33 , TB coinfection (which has been suggested to increase risk 37 ),
and others 38 may alter the distribution of severe outcomes by age. Observed severity and
burden in LMIC may also be higher due to a lack of health system capacity for intensive
treatment of severe cases.
13
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
There are some limitations to the study. The true explanation for the age distribution could
be a combination of age-specific susceptibility and clinical fraction, although some recent
studies indicate children are infected at similar 24 , or slightly lower rates 39 than adults, and
children are not commonly spared from other coronavirus infections 40,41 . It is not possible to
simultaneously estimate both effects from available data, so we were unable to validate a
mixture model. While information drawn from the early stages of the epidemic are subject to
uncertainty, age-specific information is drawn from several regions and countries, and
clinical studies support the hypothesis presented here. We assumed that clinical cases are
reported at a fixed fraction throughout the time period, although there may have been
changes in reporting. We assumed that subclinical infections were less infectious than
clinical infections but were not able to estimate how infectious subclinical infections were,
instead testing the sensitivity of our findings to this parameter. We have used mixing
matrices from the same country, but not the same location as the fitted data. We used
contact matrices that combined physical and conversational contacts. We therefore implicitly
assume that they are a good reflection of contact relevant for the transmission of
SARS-CoV-2. If fomite, or faecal-oral routes of transmission are important in transmission,
these contact matrices may not be representative of transmission risk.
The role of age in transmission is critical to designing interventions aiming to decrease
transmission in the population as a whole, and to projecting the expected global burden.
Early evidence 24 , including presented here, suggests that there is age dependence in the
risk of clinical symptoms following infection. Understanding if and by how much subclinical
infections contribute to transmission has implications for predicted global burden and the
impact of control interventions. This question must be resolved to effectively forecast and
control COVID-19 epidemics.
14
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
Methods Transmission model structure used in all analyses
We use an age-structured deterministic compartmental model (Fig. 1a, main text) stratified
into 5-year age bands, with time approximated in discrete steps of 0.25 days. We assume
that people are initially susceptible (S), and become exposed (E) after effective contact with
an infectious person. After an incubation period, exposed individuals either develop a clinical
or subclinical infection; an exposed age- i individual develops a clinical infection with
probability , otherwise developing a subclinical infection. Clinical cases are preceded by a yi
preclinical but infectious (I P ) state; from the preclinical state, individuals develop full
symptoms and become clinically infected (I C ). Based on evidence for other respiratory
infections 22 we assume that subclinical infections (I S ) are less infectious compared to
preclinical and clinical infections, and that subclinical individuals remain in the community
until they recover. We use 50% as a baseline for the relative infectiousness of individuals in
the subclinical state, and test the impact of other values (Supplementary section 3). Isolated
and recovered individuals eventually enter the removed state (R); we assume these
individuals are no longer infectious and are immune to reinfection.
The length of time an individual spends in states E, I P , I C , or I S is distributed according to
distributions , or , respectively (Table 1). The force of infection for an individual , d , ddE P C dS
in age group i at time t is
, (I I ) Nλi,t = ui∑
jcij,t P j + ICj + f S j / j
where is the susceptibility to infection of an age- i individual, is the number of age- j ui cij,t
individuals contacted by an age- i individual per day at time t , f is the relative infectiousness
of a subclinical case, and is the effective probability that a random age- j I I ) N ( P j + ICj + f S j / j
15
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
individual is infectious. Contacts vary over time t depending upon the modelled impact of
school closures and movement restrictions (see below).
To calculate the basic reproductive number, R 0 , we define the next generation matrix as
. GM c (y E(d ) 1 )fE(d ) N ij = ui ij,t j P + dC + ( yj S
R 0 is the absolute value of the dominant eigenvalue of the next generation matrix.
We use the local age distribution for each city or region being modelled, and synthetic or
measured contact matrices for mixing between age groups (Table 2). The mixing matrices
have four types of contacts: home, school, work and other contacts.
Parame ter
Description Applies in fits Value Reference
dE Incubation period (E to I P and E to I S ; days)
All amma(μ .0, ) ~ g = 4 k = 5 Derived from 42
dP Duration of preclinical infectiousness (days)
All amma(μ .4, ) ~ g = 2 k = 5 Derived from 42
dC Duration of clinical infectiousness (I C to R; days)
All amma(μ .2, .7) ~ g = 3 k = 3 43
dS Duration of subclinical infectiousness (days)
All amma(μ , ) ~ g = 7 k = 5 Assumed
ui Susceptibility for age group i Varies by age in Wuhan hypothesis 2, otherwise all ages equal
Estimated
yi Probability of clinical infection for age group i
Varies by age in Wuhan hypothesis 3, otherwise all ages equal
Either fixed (50%) or estimated
44
f Relative infectiousness of subclinical cases
All 50% (25% and 75% in sensitivity analysis)
Assumed
cij Number of age- j individuals contacted by an age- i individual per day
All Country-specific contact matrix (sensitivity analysis using synthetic matrices 19 )
China 32 ; UK 7 ; Zimbabwe 34
N i Number of age- i individuals All Demographic data 14
tΔ Time step for discrete-time simulation All 0.25 days
,Amin Amax Age range of seed cases Wuhan Estimated
16
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
tseed Day upon which seeding of infections starts
All Estimated
qH Relative change in non-school contacts during lunar new year holidays
Wuhan Estimated
qL Relative change in non-school contacts following large-scale restrictions
Wuhan, South Korea, Shanghai, Beijing, Italy
Estimated
tL Day upon which large-scale restrictions start
Wuhan, South Korea, Shanghai, Beijing, Italy
Fixed to January 23 for Wuhan; estimated for other settings
Table 1. Model parameters.
Location Mixing matrix details
Wuhan City, China We used mixing matrices measured in Shanghai in 2017/2018 45 , adapted to the demographics of Wuhan prefecture. This implicitly assumes that Shanghai mixing patterns are representative of large cities in China.
Regions of China: Anhui, Guangdong, Guangxi, Hubei, Hunan, Jiangsu, Jiangxi, Jilin Shaanxi, Shandong, Sichuan, Tianjin, Zheijiang provinces; Beijing, Shanghai.
We used mixing matrices measured in Shanghai in 2017/2018 45 , adapted to the demographics of each province / city.
Regions of Italy: Lombardia, Piemonte, Trento Veneto, Friulli Venezia Giulia, Liguria, Emilia-Romagna, Toscana, Marche, Lazio, Campania, Puglia regions; Milan.
We used mixing matrices measured in Italy in 2005/2006 11 , adapted to the demographics of each region / city. This assumes that these contact patterns will still be representative of contact patterns in 2020.
Ontario, Canada We used synthetic contact matrices, generated based on demographic information about the country 27 .
Japan We used synthetic contact matrices, generated based on demographic information about the country 27 .
Singapore We used synthetic contact matrices based on demographic information about the country 27 .
South Korea We used synthetic contact matrices based on demographic information about the country 27 .
Birmingham, UK We used mixing matrices measured in the UK in 2005/2006 11 , adapted to the demographics of Birmingham. This assumes that these contact patterns will still be representative of contact patterns in 2020.
Bulawayo, Zimbabwe We used mixing matrices measured in Manicaland, Zimbabwe in 2013 46 , adapted to the demographics of Bulawayo. This implicitly assumes that Manicaland mixing patterns are representative of Bulawayo.
150 capital cities We used synthetic contact matrices, generated based on demographic information about each country 27 .
Table 2. Details on mixing matrices used in the study.
17
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
Comparing age hypotheses by fitting to the Wuhan epidemic
We contrasted three possible hypotheses. In hypothesis 1, there were no age-related
differences in susceptibility ( ) or symptomatic fraction ( ). In hypothesis 2, ui = u yi = y
susceptibility varied by age ( ), but the proportion of exposed individuals who became (i)ui = u
clinical cases did not vary by age ( ). In hypothesis 3, the clinical case probability varied yi = y
by age ( ), but susceptibility did not ( ). Susceptibility and clinical fraction curves (i)yi = y ui = u
were fitted using three control points for young, middle, and old age, interpolating between
them with a half-cosine curve (see Methods for details).
We assumed that the initial outbreak in Wuhan was seeded by introducing one exposed
individual per day of a randomly drawn age between A min and A max for 14 days starting on a
day ( t seed ) in November 30,31 . We used the age distribution of Wuhan City prefecture in 2016 47
and contact matrices measured in Shanghai 32 as a proxy for large cities in China. This
contact matrix is stratified into school, home, work, and other contacts. We aggregated the
last three categories into non-school contacts and estimated how components of the contact
matrix changed early in the epidemic in response to major changes. Schools closed on
January 12th for the Lunar New Year holiday, so we decreased school contacts, but the
holiday period may have changed non-school contacts, so we estimate this effect by
inferring the change in non-school contact types, . Large-scale restrictions started on qH
January 23rd 2020 giving restrictions on travel and movement imposed by authorities, and
we inferred the change in contact patterns during this period, . Specifically: qL
, chool(t)·c ther(t)·c cij,t = s ij|school + o ij|other where
chool(t) s = { 1 t < 12 January 0 t ≥ 12 January
and 1 t < 12 January
ther(t) o = { q H 12 January ≤ t < 23 January q L t ≥ 23 January.
18
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
We fitted the model to incident confirmed cases from the early phase of the epidemic in
China (December 8, 2019-February 1, 2020) reported by China CDC 1 . During this period,
the majority of cases were from Wuhan City, and we truncated the data after February 1st
because there were more cases in other cities after this time. We jointly fitted the model to
the age distribution of cases at 3 time windows (December 8, 2019 to January 22, 2020)
reported by Li et al. 26 and a further time window (December 8, 2019 to February 11, 2020)
reported by China CDC 1 . Because there was a large spike of incident cases reported on
February 1 determined to have originated from the previous week, we amalgamated all
cases from January 25 to February 1, including those in the large spike, into a single data
point for the week. We assumed 10% of clinical cases were reported 19 . We used a Dirichlet
distribution with a flat prior to obtain 95% HDIs for reported case data stratified by age group
for display in figures.
We used Markov-chain Monte Carlo to jointly fit each hypothesis to the two sets of empirical
observations from the epidemic in Wuhan City, China. We used a negative binomial
likelihood for incident cases and a Dirichlet-multinomial likelihood for the age distribution of
cases, using the likelihood
L = egBinom(C |size 00, ean )(∏Kk=1
N k = 2 m = ck ) irMultinom(A | a )(∏Mm=1
D m200||a ||m
m )
Above, C k is the observed incidence on day k while c k is the model-predicted incidence for
day k, for each of K days. A m is the observed age distribution for time period m (case counts
for each age group) while a m is the model-predicted age distribution for the same period, and
is the total number of cases over all age groups in time period m , measured for M time |a || | m
periods. We set the precision of each distribution to 200 to capture additional uncertainty in
data points that would not be captured with a Poisson or multinomial likelihood model.
19
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
We distinguished fitted models using Deviance Information Criterion (DIC) 48 .
Parameter Description Prior
ui Susceptibility to infection upon contact with an infectious person
Non-age-varying: ormal(μ .1, .025, in )ui ~ n = 0 σ = 0 m = 0 Age-varying: young, middle, and old age fit as ormal(μ 5, 5, in , ax 0)ay ~ n = 1 σ = 1 m = 0 m = 3 ormal(μ 5, 5, in 0, ax 0) am ~ n = 4 σ = 1 m = 3 m = 6 ormal(μ 5, 5, in 0, ax 0) ao ~ n = 7 σ = 1 m = 6 m = 9 Susceptibility for young, middle, and old age fit as ormal(μ .1, .025, in )uy ~ n = 0 σ = 0 m = 0 ormal(μ .1, .025, in ) um ~ n = 0 σ = 0 m = 0 ormal(μ .1, .025, in ) uo ~ n = 0 σ = 0 m = 0 Then (see final row) oss(i|a , , , , , )ui = c y by am bm ao bo
yi Clinical fraction on infection Non-age-varying: .5yi = 0 Age-varying: young, middle, and old age fit as ormal(μ 5, 5, in , ax 0)ay ~ n = 1 σ = 1 m = 0 m = 3 ormal(μ 5, 5, in 0, ax 0) am ~ n = 4 σ = 1 m = 3 m = 6 ormal(μ 5, 5, in 0, ax 0) ao ~ n = 7 σ = 1 m = 6 m = 9 Susceptibility for young, middle, and old age fit as ormal(μ .5, .1, in , ax .5)yy ~ n = 0 σ = 0 m = 0 m = 0 .5 ym = 0 ormal(μ .5, .1, in .5, max ) yo ~ n = 0 σ = 0 m = 0 = 1 Then (see below) oss(i|a , , , , , )yi = c y yy am ym ao yo
tseed Timing of introduction of cases ormal(μ 5, 0, min , max 0) tseed ~ n = 1 σ = 3 = 0 = 3
qH Multiplicative factor for transmission during holiday period
eta(α , ) scaled to 0 qH ~ b = 2 β = 2 2
qL Multiplicative factor for transmission during large-scale restrictions
eta(α , )qL ~ b = 2 β = 2
,Amin Amax Age bounds for introduced cases
ormal(μ 0, 0, in 0, ax 0) A ~ n = 6 σ = 2 m = 4 m = 8 eta(α , ) scaled to 0 0 Arange ~ b = 2 β = 2 1
Amin = A Arange Amax = A + Arange
oss(a|x , , , , , ) c 1 y1 x2 y2 x3 y3 Cosine-smoothing function For a given age a (the midpoint age of age group i ) the function evaluates to for , to for , and to y1 ≤x a 1 y2 a = x2
for . Values of between and are y3 ≥x a 3 a x1 x2 interpolated between and , and values of y1 y2 a between and are interpolated between and , x2 x3 y2 y3 where the interpolation takes the shape of a cosine curve between and . π π
Table 2. Details of model fitting
20
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
Hypothesis 1 Hypothesis 2 Hypothesis 3
DIC 880 691 558
Age control points N/A Young 13 (3.7-24) Middle 43 (32-55) Old 70 (61-79)
Young 14 (11-18) Middle 55 (49-60) Old 64 (60-68)
ui 0.077 (0.073-0.08) Young 0.0076 (0.00081-0.014) Middle 0.062 (0.045-0.077) Old 0.11 (0.1-0.12)
0.078 (0.074-0.083)
yi Fixed at 0.5 Fixed at 0.5 Young 0.056 (0.0084-0.11) Middle 0.49 (0.48-0.51) Old 0.74 (0.64-0.89)
, days after Nov 1 tseed 19 (17-21) 18 (15-21) 16 (14-20)
Amid|seed 74 (63-80) 60 (34-75) 48 (31-70)
Arange|seed 4.5 (0.8-8.1) 0.78 (0.089-1.5) 2.9 (0.84-4.4)
qH 1.4 (1.3-1.6) 1.4 (1.3-1.5) 1.4 (1.3-1.5)
qL 0.14 (0.046-0.23) 0.21 (0.091-0.34) 0.2 (0.098-0.33)
Table 3. Posterior estimates and 95% highest density intervals for parameters fitted to data from Wuhan, China.
Analysis of the stationary age distribution of cases
To infer age-specific susceptibility from reported case distributions, we assumed that
reported cases follow the stationary distribution of cases reached in the early phase of an
epidemic. Using our dynamic model would allow modelling any transient emphasis in the
case distribution associated with the age of the individuals who seeded infection in a given
region, but since the age of the true first cases is not generally known, we used the
stationary distribution instead. Specifically, we used Bayesian inference to fit age-specific
susceptibility to the reported case distribution by first generating the expected case
distribution k i from (1) the age-specific susceptibility y i , (2) the measured or estimated
contact matrix for the country, and (3) the age structure of the country or region. We then
used the penalised likelihood
, ultinom(c |k ) ormal(y |μ , .25)L = M i i ∏n
i=2N i yi1 = 0 σ = 0
21
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
where c i is the observed case distribution, when fitting to data from a single country or
region. Above, the product of normal PDFs constrains the age-specific susceptibilities to
avoid overly sensitive responses to noisy data. When fitting to a combined set of regions
and/or countries, we used the penalised likelihood
irMultinom(c |sk ) ormal(y |μ , .25)L = ∏m
j=1D i,j i,j
wj∏n
i=2N i yi1 = 0 σ = 0
across countries with weights such that . We weighted 49 each of 1, , .., } j ∈ { 2 . m wj ∏
jwj = 1
the 13 provinces of China in our data set by 1/13, each of the 12 regions of Italy by 1/12, the
three reported case distributions from China CDC by 1/3, and data from South Korea,
Singapore and Japan each by 1, then scaled all weights to multiply to 1.
We fitted to the following data sources. For provinces of China, we used age-specific case
numbers reported by China CDC 1 as well as linelist data compiled by the Shanghai
Observer 50 . For regions of Italy, we used age-specific case numbers reported by the Istitute
Superiore di Sanità on March 13, 2020 51 . For South Korea, we used the linelist released by
Kim et al. based on data from the Korea Centers for Disease Control and Prevention 16 . For
Japan, we used the Open Covid Linelist 52,53 . For Singapore, we use data compiled from
Singapore Ministry of Health data by Alex Koh 15 .
To validate our line list analysis, we fitted the dynamic model to incidence data from Beijing,
Shanghai, South Korea and Lombary, Italy. We fixed the reporting rate for Beijing, Shanghai,
South Korea, and Lombardy to 20%. Beijing and Shanghai incidence data were given by
case onset, so we assumed no delay between reported and true case onsets. Incidence
data for South Korea were given by the date of confirmation only, so we assumed the
reporting delay followed a gamma distribution with a 7-day mean. Incidence data for Italy
were given separately for case onset and case confirmation, with only a subset of onset
22
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
dates available; accordingly, we fit the proportion of confirmed cases with onset dates and
the delay from onset to confirmation. We adjusted the size parameter of the negative
binomial distribution used to model case incidence to 10 to reflect greater variability among
fewer data points for these countries than for Wuhan. Beijing and Shanghai were fitted
jointly, with separate dates of introduction but the same fitted susceptibility, large-scale
restriction date and large-scale restriction magnitude. South Korea and Italy were each fitted
separately; we fitted a large-scale restriction date and magnitude for both South Korea and
Italy.
For both the linelist fitting and validation, we assumed that schools were closed in China, but
remained open in South Korea, Japan, Italy, Singapore, and Canada, as schools were open
for the majority of the period covered by the data in the latter five countries.
Quantifying the impact of school closure
To determine the impact in other cities with different demographic profiles we used the
inferred parameters from our linelist analysis to parameterise our transmission model for
projections to other cities. We chose these to compare projections for a city with a high
proportion of elderly individuals (Milan, Italy); a moderate-aged population (Birmingham,
United Kingdom); and a city in a low-income country with a high proportion of young
individuals (Bulawayo, Zimbabwe). For this analysis, we compared an outbreak of
COVID-19, for which the burden and transmission is concentrated in relatively-older
individuals, with an outbreak of pandemic influenza, for which the burden and transmission is
concentrated in relatively-younger individuals. We assumed that immunity to influenza builds
up over a person’s lifetime, such that an individual’s susceptibility to influenza infection
plateaus at roughly age 35, and assumed that the severity of influenza infection is highest in
the elderly and in children under 10 years old 7 .
23
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
To model Milan, we used the age distribution of Milan in 2019 54 and a contact matrix
measured in Italy in 2006 11 . To model Birmingham, we used the age distribution of
Birmingham in 2018 55 and a contact matrix measured in the UK in 2006 11 . To model
Bulawayo, we used the age distribution of Bulawayo Province in 2012 56 and a contact matrix
measured in Manicaland, Zimbabwe in 2013 46 . We assumed that the epidemic was seeded
by two infectious individuals in a random age group per week for 5 weeks to. We scaled the
age-specific susceptibility u i by setting the “target” basic reproductive number R 0 = 2.4 as an
illustrative example. We also performed a sensitivity analysis where we scaled u i to result in
R 0 = 2 in Birmingham, and using the same setting for u i in all three cities, so that the actual
R 0 changed depending upon contact matrices and demographics used to model each city.
This produced qualitatively similar results (Supplementary Information).
We projected the impact of school closure by setting the contact multiplier for school
contacts school(t) to 0. Complete removal of school contacts may overestimate the impact of
school closures because of alternative contacts children make when out of school 57 . This will
however give the maximum impact of school closures in the model to demonstrate the
differences.
Projecting the global impact
To project the impact of COVID-19 outbreaks in global cities, we used mixing matrices from
Prem et al. 27 and demographic structures for 2020 from World Population Prospects 2019 to
simulate a COVID-19 outbreak in 146 global capital cities for which synthetic matrices,
demographic structures and total populations were available. For simplicity, we assumed
that capital cities followed the demographic structure of their respective countries and took
24
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
the total population of each capital city from the R package maps . For each city, we scaled u i
to result in an average R 0 = 2 in Birmingham, UK, and used the same setting for u i for all
cities, so that the realised R 0 would change according to the contact matrices and
demographics for each city. We simulated 20 outbreaks in each city, drawing the
age-specific clinical fraction y i from the posterior of the estimated overall clinical fraction from
our line list analysis (Fig. 2), and analysed the time to the peak incidence of the epidemic,
the peak clinical and subclinical incidence of infection, and the total number of clinical and
subclinical infections. We took the first third and the last third of clinical cases in each city to
compare the early and late stages of the epidemic.
Acknowledgements We acknowledge the following for funding: NGD: National Institutes of Health Research (HPRU-2012-10096). PK, YL, KP, MJ: This research was partly funded by the Bill & Melinda Gates Foundation (INV-003174). YL, MJ: This research was partly funded by the National Institute for Health Research (NIHR) (16/137/109) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care. RME: HDR UK (grant: MR/S003975/1). The members of the CMMID COVID-19 working group and the funding they acknowledge are: Carl A B Pearson, Billy J Quilty (NIHR 16/137/109), Adam J Kucharski (Wellcome Trust grant: 206250/Z/17/Z), Hamish Gibbs (funded by the Department of Health and Social Care using UK Aid funding and is managed by the NIHR. The views expressed in this publication are those of the author(s) and not necessarily those of the Department of Health and SocialCare (ITCRZ 03010), Samuel Clifford (Wellcome Trust grant: 208812/Z/17/Z), Amy Gimma (Global Challenges Research Fund (GCRF) for the project "RECAP" managed through RCUK and ESRC (ES/P010873/1), Kevin van Zandvoort (supported by Elrha’s Research for Health in Humanitarian Crises (R2HC) Programme, which aims to improve health outcomes by strengthening the evidence base for public health interventions in humanitarian crises. The R2HC programme is funded by the UK Government (DFID), the Wellcome Trust, and the UK National Institute for Health Research (NIHR), James D Munday (Wellcome Trust grant: 210758/Z/18/Z), Charlie Diamond (NIHR 16/137/109), W John Edmunds, Joel Hellewell (Wellcome Trust grant: 210758/Z/18/Z), Timothy W Russel (Wellcome Trust grant: 206250/Z/17/Z), Sam Abbott (Wellcome Trust grant: 210758/Z/18/Z), Sebastian Funk (Wellcome Trust grant: 210758/Z/18/Z), Nikos I Bosse, Fiona Sun (NIHR EPIC grant 16/137/109), Stefan Flasche (Wellcome Trust grant: 208812/Z/17/Z), Alicia Rosello (NIHR grant: PR-OD-1017-20002), Christopher I Jarvis (Global Challenges Research Fund (GCRF) project ‘RECAP’ managed through RCUK and ESRC (ES/P010873/1)), RMGJH (European Research Commission Starting Grant: #757699).
25
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
Author contributions RME conceived the study. NGD and RME designed the model with PK, and YL, KP and MJ providing input. NGD designed the software and inference framework and implemented the model. YL processed the data. NGD and RME wrote the first draft of the manuscript. All authors interpreted the results, contributed to writing, and approved the final version for submission. Data Availability and Code Availability The data used for fitting are publicly available, but will also be made available with the code in the github repository for the project. Contact matrix data are available at zenodo 21,22 . Competing interests The authors have no competing interests. Additional information Supplementary Information is available for this paper. Correspondence and requests for materials should be addressed to Rosalind M Eggo or Nicholas G Davies at [email protected] or [email protected] References
1. Zhang. The epidemiological characteristics of an outbreak of 2019 novel coronavirus
diseases (COVID-19) in China. Chin. J. Epidemiol. 41 , 145–151 (20200217).
2. Sun, K., Chen, J. & Viboud, C. Early epidemiological analysis of the coronavirus disease
2019 outbreak based on crowdsourced data: a population-level observational study.
Lancet Digit. Health S2589750020300261 (2020) doi:10.1016/S2589-7500(20)30026-1.
3. D, C. et al. The early phase of the COVID-19 outbreak in Lombardy, Italy.
ArXiv200309320 Q-Bio (2020).
4. Shim, E., Tariq, A., Choi, W., Lee, Y. & Chowell, G. Transmission potential and severity
of COVID-19 in South Korea. Int. J. Infect. Dis. S1201971220301508 (2020)
doi:10.1016/j.ijid.2020.03.031.
5. Anderson, R. M. et al. Epidemiology, transmission dynamics and control of SARS: the
2002–2003 epidemic. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 359 , 1091–1105 (2004).
6. Jhung, M. A. et al. Epidemiology of 2009 Pandemic Influenza A (H1N1) in the United
26
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
States. Clin. Infect. Dis. 52 , S13–S26 (2011).
7. Greer, A. L., Tuite, A. & Fisman, D. N. Age, influenza pandemics and disease dynamics.
Epidemiol. Infect. 138 , 1542–1549 (2010).
8. Dong, Y. et al. Epidemiological Characteristics of 2143 Pediatric Patients With 2019
Coronavirus Disease in China. Pediatrics e20200702 (2020)
doi:10.1542/peds.2020-0702.
9. Zhao, X. et al. Incidence, clinical characteristics and prognostic factor of patients with
COVID-19: a systematic review and meta-analysis .
http://medrxiv.org/lookup/doi/10.1101/2020.03.17.20037572 (2020)
doi:10.1101/2020.03.17.20037572.
10. Huang, C. et al. Clinical features of patients infected with 2019 novel coronavirus in
Wuhan, China. The Lancet 395 , 497–506 (2020).
11. Mossong, J. et al. Social Contacts and Mixing Patterns Relevant to the Spread of
Infectious Diseases. PLOS Med. 5 , e74 (2008).
12. Cauchemez, S., Valleron, A.-J., Boëlle, P.-Y., Flahault, A. & Ferguson, N. M. Estimating
the impact of school closure on influenza transmission from Sentinel data. Nature 452 ,
750–754 (2008).
13. Eames, K. T. D., Tilston, N. L., Brooks-Pollock, E. & Edmunds, W. J. Measured Dynamic
Social Contact Patterns Explain the Spread of H1N1v Influenza. PLoS Comput. Biol. 8 ,
e1002425 (2012).
14. World Population Prospects - Population Division - United Nations.
https://population.un.org/wpp/.
15. Koh, A. Singapore COVID-19 Cases. http://alexkoh.net/covid19/.
16. Data Science for COVID-19 (DS4C). https://kaggle.com/kimjihoo/coronavirusdataset.
17. Cowling, B. J. et al. Increased Risk of Noninfluenza Respiratory Virus Infections
Associated With Receipt of Inactivated Influenza Vaccine. Clin. Infect. Dis. 54 ,
27
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
1778–1783 (2012).
18. Tsagarakis, N. J. et al. Age-related prevalence of common upper respiratory pathogens,
based on the application of the FilmArray Respiratory panel in a tertiary hospital in
Greece: Medicine (Baltimore) 97 , e10903 (2018).
19. Common cold. nhs.uk https://www.nhs.uk/conditions/common-cold/ (2017).
20. Galanti, M. et al. Rates of asymptomatic respiratory virus infection across age groups.
Epidemiol. Infect. 147 , e176 (2019).
21. Zhou, F. et al. Clinical course and risk factors for mortality of adult inpatients with
COVID-19 in Wuhan, China: a retrospective cohort study. The Lancet
S0140673620305663 (2020) doi:10.1016/S0140-6736(20)30566-3.
22. Van Kerckhove, K., Hens, N., Edmunds, W. J. & Eames, K. T. D. The Impact of Illness
on Social Networks: Implications for Transmission and Control of Influenza. Am. J.
Epidemiol. 178 , 1655–1662 (2013).
23. Lipsitch, M., Swerdlow, D. L. & Finelli, L. Defining the Epidemiology of Covid-19 —
Studies Needed. N. Engl. J. Med. 0 , null (2020).
24. Bi, Q. et al. Epidemiology and Transmission of COVID-19 in Shenzhen China: Analysis
of 391 cases and 1,286 of their close contacts .
http://medrxiv.org/lookup/doi/10.1101/2020.03.03.20028423 (2020)
doi:10.1101/2020.03.03.20028423.
25. Yang, Y. et al. Epidemiological and clinical features of the 2019 novel coronavirus
outbreak in China . http://medrxiv.org/lookup/doi/10.1101/2020.02.10.20021675 (2020)
doi:10.1101/2020.02.10.20021675.
26. Li, Q. et al. Early Transmission Dynamics in Wuhan, China, of Novel
Coronavirus–Infected Pneumonia. N. Engl. J. Med. NEJMoa2001316 (2020)
doi:10.1056/NEJMoa2001316.
27. Prem, K., Cook, A. R. & Jit, M. Projecting social contact matrices in 152 countries using
28
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
contact surveys and demographic data. PLOS Comput. Biol. 13 , e1005697 (2017).
28. Onder, G., Rezza, G. & Brusaferro, S. Case-Fatality Rate and Characteristics of Patients
Dying in Relation to COVID-19 in Italy. JAMA (2020) doi:10.1001/jama.2020.4683.
29. Chan, K. P. Control of Severe Acute Respiratory Syndrome in Singapore. Environ.
Health Prev. Med. 10 , 255–259 (2005).
30. Lau, J. T. F. Monitoring community responses to the SARS epidemic in Hong Kong: from
day 10 to day 62. J. Epidemiol. Community Health 57 , 864–870 (2003).
31. Cauchemez, S. et al. School closures during the 2009 influenza pandemic: national and
local experiences. BMC Infect. Dis. 14 , 207 (2014).
32. Cauchemez, S. et al. Closure of schools during an influenza pandemic. Lancet Infect.
Dis. 9 , 473–481 (2009).
33. Cohen, C. et al. Severe Influenza-associated Respiratory Infection in High HIV
Prevalence Setting, South Africa, 2009–2011. Emerg. Infect. Dis. 19 , (2013).
34. IHME. Global Burden of Disease. http://www.healthdata.org/gbd.
35. Williams, C. M. et al. Exhaled Mycobacterium tuberculosis output and detection of
subclinical disease by face-mask sampling: prospective observational studies. Lancet
Infect. Dis. S1473309919307078 (2020) doi:10.1016/S1473-3099(19)30707-8.
36. Murray, J. et al. Determining the Provincial and National Burden of Influenza-Associated
Severe Acute Respiratory Illness in South Africa Using a Rapid Assessment
Methodology. PLOS ONE 10 , e0132078 (2015).
37. Liu, Y. et al. Active or latent tuberculosis increases susceptibility to COVID-19 and
disease severity . http://medrxiv.org/lookup/doi/10.1101/2020.03.10.20033795 (2020)
doi:10.1101/2020.03.10.20033795.
38. Cohen, A. L. et al. Potential Impact of Co-Infections and Co-Morbidities Prevalent in
Africa on Influenza Severity and Frequency: A Systematic Review. PLOS ONE 10 ,
e0128580 (2015).
29
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
39. Zhang, J. et al. Age profile of susceptibility, mixing, and social distancing shape the
dynamics of the novel coronavirus disease 2019 outbreak in China .
http://medrxiv.org/lookup/doi/10.1101/2020.03.19.20039107 (2020)
doi:10.1101/2020.03.19.20039107.
40. Jevšnik, M. et al. Coronavirus infections in hospitalized pediatric patients with acute
respiratory tract disease. BMC Infect. Dis. 12 , 365 (2012).
41. Lee, J. & Storch, G. A. Characterization of Human Coronavirus OC43 and Human
Coronavirus NL63 Infections Among Hospitalized Children <5 Years of Age: Pediatr.
Infect. Dis. J. 33 , 814–820 (2014).
42. Backer, J. A., Klinkenberg, D. & Wallinga, J. Incubation period of 2019 novel coronavirus
(2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020.
Eurosurveillance 25 , (2020).
43. Kucharski, A. J. et al. Early dynamics of transmission and control of COVID-19: a
mathematical modelling study. Lancet Infect. Dis. S1473309920301444 (2020)
doi:10.1016/S1473-3099(20)30144-4.
44. Nishiura, H. et al. The Rate of Underascertainment of Novel Coronavirus (2019-nCoV)
Infection: Estimation Using Japanese Passengers Data on Evacuation Flights. J. Clin.
Med. 9 , 419 (2020).
45. Zhang, J. et al. Patterns of human social contact and contact with animals in Shanghai,
China. Sci. Rep. 9 , 1–11 (2019).
46. Melegaro, A. et al. Social Contact Structures and Time Use Patterns in the Manicaland
Province of Zimbabwe. PLOS ONE 12 , e0170459 (2017).
47. National Bureau of Statistics. China Statistical Year Book. (2005-2018).
http://www.stats.gov.cn/tjsj/ndsj/.
48. Spiegelhalter, D. J., Best, N. G., Carlin, B. P. & van der Linde, A. Bayesian measures of
model complexity and fit. J. R. Stat. Soc. Ser. B Stat. Methodol. 64 , 583–639 (2002).
30
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint

/
49. Varin, C., Reid, N. & Firth, D. An overview of composite likelihood methods. Stat. Sin.
21 , (2011).
50. Observer, S. Shanghai Observer. COVID-2019 Linelist.
http://data.shobserver.com/www/datadetail.html?contId=1000895.
51. Epicentro. Bolletino Sorveglianza Integrata COVID-19 12 Marzo 2020 Appendix .
https://www.epicentro.iss.it/coronavirus/bollettino/Bolletino-sorveglianza-integrata-COVI
D-19_12-marzo-2020_appendix.pdf.
52. COVID19_2020_open_line_list.
https://docs.google.com/spreadsheets/d/1itaohdPiAeniCXNlntNztZ_oRvjh0HsGuJXUJW
ET008/edit?usp=sharing.
53. Xu, B. et al. Open access epidemiological data from the COVID-19 outbreak. Lancet
Infect. Dis. S1473309920301195 (2020) doi:10.1016/S1473-3099(20)30119-5.
54. Milano (Metropolitan City, Italy) - Population Statistics, Charts, Map and Location.
http://citypopulation.info/en/italy/admin/lombardia/015__milano/.
55. Age breakdown of the population of Birmingham - Office for National Statistics.
https://www.ons.gov.uk/aboutus/transparencyandgovernance/freedomofinformationfoi/ag
ebreakdownofthepopulationofbirmingham.
56. Bulawayo (City, Zimbabwe) - Population Statistics, Charts, Map and Location.
http://citypopulation.info/php/zimbabwe-admin.php?adm1id=A.
57. Kucharski, A. J., Conlan, A. J. K. & Eames, K. T. D. School’s Out: Seasonal Variation in
the Movement Patterns of School Children. PLOS ONE 10 , e0128070 (2015).
31
. CC-BY 4.0 International licenseIt is made available under a perpetuity.
is the author/funder, who has granted medRxiv a license to display the preprint in(which was not certified by peer review)preprint The copyright holder for thisthis version posted March 27, 2020. .https://doi.org/10.1101/2020.03.24.20043018doi: medRxiv preprint