STEP 11. Erytrocyte disorder : abnormalities of size, shape, and
colour of red blood cell cause by increasing or decreasing amount
of Hbs rate in the erytrocyte.
2. Erytrocyte : red blood cell.
STEP 2
1. What is symptom of erytrocyte disorder ?
2. Identify and describe variety of erytrocyte disorder ?
3. What causes erytrocyte disorder ?
4. What are the test to diagnose blood disorder ?
5. What are physical examination of blood disorder ?
6. Whether if the number of erytrocyte is normal but there are
decreasing of haemoglobin level includes in the erytrocyte
abnormalities ?
7. What is the symptom of anemia ?
8. What are the various of anemia ?
9. What is the pathogenesis of anemia ?
STEP 3
1. Identify and describe variety of erytrocyte disorder ?
a. Red blood cell variation in shape :
Sperocyte : it has not central pallor.
Stomatocyte : shape of central pallor like mouth.
Eliptocis : its shape like elip.
Teardrop cell : the shape of cell is like a teardrop.
Pencil cell : the shape of cell is like a pencil.
Sickle cell : the shape of cell is like a moon or letter L.
b. RBC variation in size :
Microcytic cell : size of erytrocyte is less then lymfocyte
central.
Macrocytic cell : size of erytrocyte is bigger then lymfocte
central.
c. Based on colour of central pallor : Hypocromic : the diameter
of central pallor is less then 1/3 erytrocytes diameter.
Hypercromic : the diameter of central pallor is bigger then 1/3
erytrocytes diameter.
d. Based on haemoglobin :
Anemia : the condition when the number of erytrocyte is
decreasing.
Policitemia : the condition when the number of erytrocyte is
increasing.
Thalasemia : the condition when the number of erytrocyte
decreases based on abnormalities genetic.
2. What is symptom of erytrocyte disorder ?
Conjungtiva palpebra anemis.
Lack of concentration.
Tachycardy.
Headache.
Dispneu.
Dizzyness.
Hipoksia.
Sepalbia.
Exhausted.
Hypotensi.
Buzzing ear.
Cephalgia.
Anemia deficiency Fe : disfagia.
Anemia deficiency folat acid : red tounge.
Anemia hemolitic : icterus, hepatomegali.
3. What causes erytrocyte disorder ?
Hereditance.
Bleeding.
Unhealthy lifestyle.
Consuming heavy metal chemical.
Paracytes.
Menstruasi.
Pregnancy.
4. What are the test to diagnose blood disorder ?
Erytrocyte sedimentations rate.
Haemoglobin rate.
Hematokrit.
Counting amount of erytrocyte.
Counting amount of leucocyte.
Counting amount of thrombocyte.
Hematology routine.
Hematology specific.
5. What are physical examination of blood disorder ?
The palm is icteric or not.
The conjungtiva is pale or not.
The hair is easy to loss or not.
The colour of skin. Splenomegali.
The nail is spoon or not.
6. What are the various of anemia ?
Anemia caused by lossing blood : after experiencing bleeding
which is so fast, the body will replace the blood.
Anemia aplastic : the bone marrow can not produce erytrocyte
caused of radiation.
a. Primer congenital : it has hereditys pattern autocomal
resesive.
b. Primer ideopatic : the mechanism has been not known yet.
c. Secunder : because of radiation.
Anemia hemolitic : the cell is easy to licis. Anemia based on
etilogy :
a. Anemia pernisiosa : deficiency vit B12, bacause of instrinsic
factor of gaster (mucose), the gasters mucose can not absorb
properly.
7. Whether if the number of erytrocyte is normal but there are
decreasing of haemoglobin level includes in the erytrocyte
abnormalities ?
Anemia, because there is lack of haemoglobin in erytrocyte
(hypocrom)
8. What is the pathogenesis of anemia ?
Bleeding -> darah kental -> tachycardy.
9. Variety and etiology of polisitemia ?
10. What is thalasemia ?
STEP 4
1. Identify and describe variety of erytrocyte disorder ?
Classified by checking MCV (mean corpusculer volume). MCV allows
us to classify anemia as microcytic (MCV < 82 fL), normocytic
(MCV = 82-98 fL) and macrocytic (MCV > 98 fL).
a. Microcytic anemia
Faced with microcytic anemia, the three main diagnostic
possibilities include iron deficiency anemia (IDA), thalassemia,
and anemia of chronic disorders (ACD).
b. Normocytic anemia
The fundamental question in normocytic anemia is to recognize
the causes and susceptibility to treatment as soon as possible.
Among the causes are nutritional deficiency, renal failure and
hemolytic anemia
c. Macrocytic anemia
Macrocytosis is observed frequently using blood cell analyzers.
Its prevalence is 1.7%-3.9%, but 60% of the patients with
macrocytosis do not have anemia. On the other hand, macrocytosis
can be physiological in some circumstances (infants, pregnancy,
some families). Even keeping in mind the precedent data is
convenient to make a careful evaluation of macrocytosis in every
patient, to rule out any underlying pathology. In vitamin B12 and
folic acid deficiency, as well as in other diseases, macrocytosis
(blood) is accompanied by megaloblastosis (bone marrow). In such
cases, both terms can be used interchangeably. The starting point
in the diagnostic process for macrocytic anemia will be to rule out
therapy with drugs that interfere with nucleic acid metabolism,
such as hydroxyurea, methotrexate, trimethoprim, zidovudine or
5-fluorouracil, as well as habitual intake of alcohol
http://chealth.canoe.ca/channel_condition_info_details.asp?disease_id=280&channel_id=2022&relation_id=16451http://www.hem-aids.ru/system/files/attachments/646/anemii_anemii_pdf_008.pdf2.
What is symptom of erytrocyte disorder ?
Anemia symptoms
Patients with anemia may present with fatigue, dizziness and
dyspnea; however, mild anemia shows few clinical signs or symptoms.
The signs of anemia include pallor of the conjunctivae, face, nail
beds and palmar creases, although the absence of pallor does not
rule out anemia
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2754510/Symptoms
(Polycythemia)
Polycythemia may not cause any symptoms. It's often discovered
only if a hemoglobin test or a red blood cell count is done. Some
people do experience symptoms that appear gradually. These may
include itching following bathing, dizziness, and a flushing of the
face and hands. Weakness, headaches, visual disturbances, and a
sense of "fullness" in the head and in the left upper abdomen may
also be associated with the condition. Some people may have high
blood
pressure.http://chealth.canoe.ca/channel_condition_info_details.asp?disease_id=280&channel_id=2022&relation_id=16451Thalasemia
A lack of oxygen in the bloodstream causes the signs and
symptoms of thalassemias. The lack of oxygen occurs because the
body doesn't make enough healthy red blood cells and hemoglobin.
The severity of symptoms depends on the severity of the
disorder.
Symptoms
Alpha thalassemia silent carriers generally have no signs or
symptoms of the disorder. This is because the lack of alpha globin
protein is so minor that the body's hemoglobin works normally.
http://www.nhlbi.nih.gov/health//dci/Diseases/Thalassemia/Thalassemia_Signs.html3.
What causes erytrocyte disorder ?
TOXIC FORMS include plumbism. Here, lead salts attach to
erythrocyte membranes making it more vulnerable to lysis or removal
from circulation. Often we see a gingival "lead line" in
plumbism.
BLOOD INCOMPATIBILITIES These forms include immune hemolysis
such as from D or Rh antigens (maternal-fetal incompatibilities) or
the ABO antigens (transfusion-related incompatibilities).
AUTOIMMUNE HEMOLYTIC ANEMIAS may be associated with tumors,
infections and inflammatory conditions.
MECHANICAL HEMOLYSIS may be associated with artificial cardiac
valveshttp://jan.ucc.nau.edu/prh/bio320/lecture_10.html4. What are
the test to diagnose blood disorder ?
The reticulocyte countIncreased reticulocytes (greater than 2-3%
or 100,000/mm3 total) are seen in blood loss and hemolytic
processes, although up to 25% of hemolytic anemias will present
with a normal reticulocyte count due to immune destruction of red
cell precursors. faculty.washington.edu/rrichard 5. What are
physical examination of blood disorder ?
6. What are the various of anemia ?
1. Morphological classification
Classified by checking MCV (mean corpusculer volume). MCV allows
us to classify anemia as microcytic (MCV < 82 fL), normocytic
(MCV = 82-98 fL) and macrocytic (MCV > 98 fL).
Microcytic anemia
Faced with microcytic anemia, the three main diagnostic
possibilities include iron deficiency anemia (IDA), thalassemia,
and anemia of chronic disorders (ACD).
Normocytic anemia
The fundamental question in normocytic anemia is to recognize
the causes and susceptibility to treatment as soon as possible.
Among the causes are nutritional deficiency, renal failure and
hemolytic anemia
Macrocytic anemia
Macrocytosis is observed frequently using blood cell analyzers.
Its prevalence is 1.7%-3.9%, but 60% of the patients with
macrocytosis do not have anemia. On the other hand, macrocytosis
can be physiological in some circumstances (infants, pregnancy,
some families). Even keeping in mind the precedent data is
convenient to make a careful evaluation of macrocytosis in every
patient, to rule out any underlying pathology. In vitamin B12 and
folic acid deficiency, as well as in other diseases, macrocytosis
(blood) is accompanied by megaloblastosis (bone marrow). In such
cases, both terms can be used interchangeably. The starting point
in the diagnostic process for macrocytic anemia will be to rule out
therapy with drugs that interfere with nucleic acid metabolism,
such as hydroxyurea, methotrexate, trimethoprim, zidovudine or
5-fluorouracil, as well as habitual intake of alcohol
http://chealth.canoe.ca/channel_condition_info_details.asp?disease_id=280&channel_id=2022&relation_id=164517.
Whether if the number of erytrocyte is normal but there are
decreasing of haemoglobin level includes in the erytrocyte
abnormalities ?
8. What is the pathogenesis of anemia ?
Berdasarkan patogenesisnya, anemia digolongkan dalam 3
kelompok
(Wintrobe at all, 1999) yaitu:
1. Anemia karena kehilangan darah
Anemia karena kehilangan darah akibat perdarahan yaitu
terlalu
banyaknya sesl-sel darah merah yang hilang dari tubuh seseorang,
akibat
dari kecelakaan dimana perdarahan mendadak dan banyak
jumlahnya,
yang disebut perdarahan ekternal. Perdarahan dapat pula
disebabkan
karena racun, obat-obatan atau racun binatang yang
menyebabkan
penekanan terhadap pembuatan sel-sel darah merah. Selain itu ada
pula
perdarahan kronis yang terjadi sedikit demi sedikit tetapi terus
menerus.
Perdarahan ini disebabkan oleh kanker pada saluran pencernaan,
peptic
ulser, wasir yang dapat menyebabkan anemia.
2. Anemia karena pengrusakan sel-sel darah merah
Anemei karena pengrusakan sel-sel darah merah dapat terjadi
karena bibit penyakit atau parasit yang masuk kedalam tubuh,
seperti
malaria atau cacing tambang, hal ini dapat menyebabkan
anemia
hemolitik. Bila sel-sel darah merah rusak dalam tubuh, zat besi
yang ada di
dalam tidak hilang tetapi dapat digunakan kembali untuk
membentuk selsel
darah merah yang baru dan pemberian zat besi pada anemia jenis
ini
kurang bermaanfaat. Sedangkan asam folat dirusak dan tidak
dapat
digunakan lagi oleh karena itu pemberian asam folat sangat
diperlukan
untuk pengobatan anemia hemolitik ini.
3. Anemia karena gangguan pada produksi sel-sel darah merah
Sum-sum tulang mengganti sel darah yang tua dengan sel darah
merah yang baru sama cepatnya dengan banyaknya sel darah merah
yang
hilang, sehingga jumlah sel darah merah yang dipertahankan
selalu cukup
banyak di dalam darah, dan untuk mempertahakannya diperlukan
cukup
banyak zat gizi. Apabila tidak tersedia zar gizi dalam jumlah
yang cukup
akan terjadi gangguan pembentukan sel darah merah baru.
Anemia karena gangguan pada produksi sel-sel darah merah,
dapat
timbul karena, kurangnya zat gizi penting seperti zat besi, asam
folat, asam
pantotenat, vitamin B12, protein kobalt, dan tiamin, yang
kekurangannya
biasa disebut anemia gizi. Selain itu juga kekurangan eritrosit,
infiltrasi
sum-sum tulang, kelainan endokrin dan penyakit ginjal kronis dan
sirosis
hati. Menurut Husaini (1998) anemia gizi yang disebabkan
kekurangan
zat besi sangat umum dijumpai di
Indonesia.www.library.upnvj.ac.id/pdf/s1keperawatan09/207314005/bab2.pdf9.
Variety and etiology of polisitemia ?
Variety :
Polycythemia is an over-production of erythrocytes and blood
plethora (may be 2-3X; RBC 6-10 million/mm3). Often characterized
by liver enlargement and excessive thrombosis (elevated platelet
levels). Also presents general circulation problems.
Secondary polycythemia such as from excessive erythropoietin, or
subsequent to high-altitude training or to carbon monoxide
poisoning.
Primary polycythemia (polycythemia vera) may be due to a benign
tumor of the bone
marrow.http://jan.ucc.nau.edu/prh/bio320/lecture_10.htmlEtiology
:
Dehydration because of Shortage of water,prolonged vomiting,
diarrhea(BA Pathology Kumar Robins, issue 7)
10. What is thalasemia ?
Thalassemia
Thalassemia is a blood disorder passed down through families
(inherited) in which the body makes an abnormal form ofhemoglobin,
the protein in red blood cells that carries oxygen. The disorder
results in excessive destruction of red blood cells, which leads to
anemia.
Causes, incidence, and risk factors
Hemoglobin is made of two proteins: Alpha globin and beta
globin. Thalassemia occurs when there is a defect in a gene that
helps control production of one of these proteins.
There are two main types of thalassemia:
Alpha thalassemia occurs when a gene or genes related to the
alpha globin protein are missing or changed (mutated).
Beta thalassemia occurs when similar gene defects affect
production of the beta globin protein.
Alpha thalassemias occur most commonly in persons from southeast
Asia, the Middle East, China, and in those of African descent.
Beta thalassemias occur in persons of Mediterranean origin, and
to a lesser extent, Chinese, other Asians, and African
Americans.
There are many forms of thalassemia. Each type has many
different subtypes. Both alpha and beta thalassemia include the
following two forms:
Thalassemia major
Thalassemia minor
You must inherit the defective gene from both parents to develop
thalassemia major.
Thalassemia minor occurs if you receive the defective gene from
only one parent. Persons with this form of the disorder are
carriers of the disease and usually do not have symptoms.
Beta thalassemia major is also called Cooley's anemia.
Symptoms
The most severe form of alpha thalassemia major
causesstillbirth(death of the unborn baby during birth or the late
stages of pregnancy).
Children born with thalessemia major (Cooley's anemia) are
normal at birth, but develop severeanemiaduring the first year of
life.
Other symptoms can include:
Bone deformities in the face
Fatigue Growth failure
Shortness of breath Yellow skin (jaundice)
Persons with the minor form of alpha and beta thalassemia have
small red blood cells (which are identified by looking at their red
blood cells under a microscope), but no symptoms.
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001613/1. Giardina
PJ, Forget BG. Thalassemia syndromes. In: Hoffman R, Benz EJ,
Shattil SS, et al., eds.Hematology: Basic Principles and Practice.
5th ed. Philadelphia, Pa: Elsevier Churchill Livingstone; 2008:chap
41.
2. DeBaun MR, Frei-Jones M, Vichinsky E. Hemoglobinopathies. In:
Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds.Nelson Textbook
of Pediatrics. 19th ed. Philadelphia, Pa: Saunders Elsevier;
2011:chap 456.
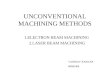
Anemia
Sintesa
Jumlah
Erytrocyte disorder
Polisitemia
Thalasemia
primer
sekunder
relatif
alpha
betha
mayor
minor
-anemia sideroblastik
Anemia hipoblastik
Anemia megaloblastik