Embed Size (px)
DESCRIPTION
adrenak cortex disorders
Citation preview

Adrenocortical Adrenocortical disordersdisorders
ByBy
AbdAlAziz AbdAllah, AbdAlAziz AbdAllah, MDMD

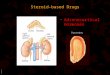
The adrenal gland is divided into two The adrenal gland is divided into two parts, adrenal cortex and medullaparts, adrenal cortex and medulla..
The adrenal cortex secretes androgen, The adrenal cortex secretes androgen, mineralocorticoids (eg, aldosteron) and mineralocorticoids (eg, aldosteron) and glucocorticoids (eg, crtisol)glucocorticoids (eg, crtisol)..
The adrenal medulla secretes The adrenal medulla secretes catecholamines (eg, epinephrine, catecholamines (eg, epinephrine, norepinephrine, dopamine)norepinephrine, dopamine)..

Aldosteron is primarily involved with Aldosteron is primarily involved with fluid and electrolyte balancefluid and electrolyte balance..
Aldosteron secretion causes sodium Aldosteron secretion causes sodium reabsorption in the distal renal reabsorption in the distal renal tubule in exchange for potassium tubule in exchange for potassium and hydrogen ionsand hydrogen ions..
The net effects are, fluid retention, The net effects are, fluid retention, decrease in plasma potassium and decrease in plasma potassium and metabolic alkalosismetabolic alkalosis..

Aldosteron secretion is stimulated byAldosteron secretion is stimulated by;;
--Renin-angiotensin systemRenin-angiotensin system..
--ACTHACTH..
--HyperkalemiaHyperkalemia..
--HypovolemiaHypovolemia . .
--HypotensionHypotension . .
--congestive heart failurecongestive heart failure..
--SurgerySurgery..

Glucocorticoids are essential for life and have Glucocorticoids are essential for life and have mutiple pysiological effectsmutiple pysiological effects..
Metabolic actions include enhanced Metabolic actions include enhanced gluconeogenesis and inhibition of peripheral gluconeogenesis and inhibition of peripheral glucose utilizationglucose utilization..
Glucocorticoids are required for vascular and Glucocorticoids are required for vascular and bronchial smooth muscle to be responsive to bronchial smooth muscle to be responsive to catecholaminescatecholamines..
Glucocorticoids are structurly related to Glucocorticoids are structurly related to aldosteron, so they have aldosteron like actionaldosteron, so they have aldosteron like action..

ACTH is the principal regulator of ACTH is the principal regulator of Glucocorticoids secretionGlucocorticoids secretion..
Secretion of ACTH and glucocorticoids Secretion of ACTH and glucocorticoids exhibit a diurnal rhythm, stimulated by exhibit a diurnal rhythm, stimulated by stress and inhibited by circulating stress and inhibited by circulating glucocorticoidsglucocorticoids..
Endogenous production of cortisol Endogenous production of cortisol averages 20 mg \ dayaverages 20 mg \ day..

Mineralocorticoid excessMineralocorticoid excess
I- 1ry hyper-aldosteronism (I- 1ry hyper-aldosteronism (Conn Conn syndrome)syndrome)::
Conn syndrome is characterized by increased Conn syndrome is characterized by increased aldosterone secretion from the adrenal glands, it aldosterone secretion from the adrenal glands, it was first described in 1955 by J. W. Conn in a was first described in 1955 by J. W. Conn in a patient who had an aldosterone-producing patient who had an aldosterone-producing
adenomaadenoma..

PathophysiologyPathophysiologyPrimary hyperaldosteronism is caused by Primary hyperaldosteronism is caused by
increased aldosterone excretion from the increased aldosterone excretion from the adrenals, which results primarily from 2 major adrenals, which results primarily from 2 major subtypessubtypes : :
((11 ) )unilateral aldosterone-producing adenoma , unilateral aldosterone-producing adenoma , Conn syndrome, (50-60% of cases)Conn syndrome, (50-60% of cases)
((22 ) )idiopathic hyperaldosteronism (IHA) or bilateral idiopathic hyperaldosteronism (IHA) or bilateral adrenal hyperplasia (40-50% of cases)adrenal hyperplasia (40-50% of cases) . .
((33 ) )Rarely, aldosterone can be secreted by Rarely, aldosterone can be secreted by adrenocortical carcinomas and ovarian tumorsadrenocortical carcinomas and ovarian tumors..

Aldosterone, by inducing renal Aldosterone, by inducing renal distal tubular reabsorption of distal tubular reabsorption of sodium, enhances secretion of sodium, enhances secretion of potassium and hydrogen ions, potassium and hydrogen ions, causing hypernatremia, causing hypernatremia, hypokalemia, and metabolic hypokalemia, and metabolic alkalosisalkalosis..

FrequencyFrequency::Prevalence for Conn syndrome; 0.05-2% of the Prevalence for Conn syndrome; 0.05-2% of the
populationpopulation..
Mortality/MorbidityMortality/Morbidity::The morbidity and mortality associated with The morbidity and mortality associated with
Conn syndrome, are primarily related toConn syndrome, are primarily related to ; ;11 - -Hypertension, especially if left untreated for Hypertension, especially if left untreated for
many years, can lead to many complications, many years, can lead to many complications, including heart disease )eg, coronary artery including heart disease )eg, coronary artery disease, congestive heart failure(, stroke, and disease, congestive heart failure(, stroke, and intracerebral hemorrhage )with very high blood intracerebral hemorrhage )with very high blood pressure(pressure(..

22--Hypokalemia, especially if severe, causes Hypokalemia, especially if severe, causes cardiac arrhythmias, which cancardiac arrhythmias, which can be fatal be fatal
AgeAgePeak incidence occurs in the third to sixth Peak incidence occurs in the third to sixth
decades of lifedecades of life..
SexSexPrimary hyperaldosteronism is twice as common Primary hyperaldosteronism is twice as common
in women as in menin women as in men..

II- 2ry hyperaldosteronismII- 2ry hyperaldosteronism::
There is increased renin-angiotensin with There is increased renin-angiotensin with increased aldosteron secretionincreased aldosteron secretion;;
--CHFCHF--Liver cirrhosis and ascitisLiver cirrhosis and ascitis
--Nephrotic syndromeNephrotic syndrome--Renal artery stenosisRenal artery stenosis

Clinical manifestationsClinical manifestations--HypertensionHypertension ; ;
--HypokalemiaHypokalemia;; patients with severe hypokalemia report fatigue, patients with severe hypokalemia report fatigue,
muscle weakness, cramping, headaches, and muscle weakness, cramping, headaches, and palpitations. They can also have polydipsia and palpitations. They can also have polydipsia and polyuria from hypokalemia-induced nephrogenic polyuria from hypokalemia-induced nephrogenic diabetes insipidusdiabetes insipidus..

--Metabolic alkalosisMetabolic alkalosis ; ;will lower ionized calcium levels and can will lower ionized calcium levels and can
cause tetanycause tetany..InvestigationsInvestigations::
Laboratory StudiesLaboratory Studies--hypernatremiahypernatremia
--Hypokalemia; normokalemia does not Hypokalemia; normokalemia does not exclude primary hyperaldosteronism. Several exclude primary hyperaldosteronism. Several studies have shown that 7-38% of patients studies have shown that 7-38% of patients with primary hyperaldosteronism have with primary hyperaldosteronism have normal baseline serum levels of potassiumnormal baseline serum levels of potassium

--metabolic alkalosismetabolic alkalosis--Renin levels are suppressed to less than 1 Renin levels are suppressed to less than 1
ng/mL/h in patients with primary ng/mL/h in patients with primary hyperaldosteronismhyperaldosteronism..
--A 24-hour aldosterone excretion rate of A 24-hour aldosterone excretion rate of greater than 14 ug is diagnostic of primary greater than 14 ug is diagnostic of primary hyperaldosteronismhyperaldosteronism

Imaging StudiesImaging Studies
--CT scanningCT scanning--MRIMRI

TreatmentTreatment
MedicalMedical medical therapy is used preoperatively to medical therapy is used preoperatively to
prevent the morbidity and mortality associated prevent the morbidity and mortality associated with hypertension and hypokalemia, thus with hypertension and hypokalemia, thus
decreasing surgical riskdecreasing surgical risk.. -- Sodium-restricted diet )<80 mEq or <2 g of Sodium-restricted diet )<80 mEq or <2 g of
sodium per daysodium per day..--Potassium-sparing agent )first-step agent( such Potassium-sparing agent )first-step agent( such
as spironolactoneas spironolactone100 mg initially, increase to 100 mg initially, increase to 400 mg/d for control of blood pressure400 mg/d for control of blood pressure..

--Potassium supplementation should not be Potassium supplementation should not be routinely administered with spironolactone routinely administered with spironolactone because of the potential for the development of because of the potential for the development of hyperkalemiahyperkalemia..
--Second-step agents include thiazides diuretics, Second-step agents include thiazides diuretics, ACE inhibitors, calcium channel antagonists, ACE inhibitors, calcium channel antagonists, and angiotensin II blockersand angiotensin II blockers..

Surgical CareSurgical Care
Surgery is the main therapy for Conn Surgery is the main therapy for Conn syndrome. A laparoscopic adrenalectomy syndrome. A laparoscopic adrenalectomy is favored, when possibleis favored, when possible

Anesthetic considerationsAnesthetic considerations
Preoperative correction of hypertension, CHF Preoperative correction of hypertension, CHF and volume and electrolytes imbalance specially and volume and electrolytes imbalance specially potassium is mandatorypotassium is mandatory..

Mineralocorticoid deficiencyMineralocorticoid deficiency
--Hypo-aldosteronismHypo-aldosteronism Atrophy or destruction of both adrenal Atrophy or destruction of both adrenal
glands results in a combined deficiency of glands results in a combined deficiency of Mineralocorticoid and glucocorticoid Mineralocorticoid and glucocorticoid
( addison disease)( addison disease). . --Isolated Mineralocorticoid deficiencyIsolated Mineralocorticoid deficiency;;
--Unilateral adrenalectomyUnilateral adrenalectomy--DM -Heparine therapyDM -Heparine therapy
--congenitalcongenital

C\PC\P
**Hypotension; due to hypovolemiaHypotension; due to hypovolemia**Metabolic acidosisMetabolic acidosis
**Hyperkalemia; any increase in s. Hyperkalemia; any increase in s. potassium without renal impairment, potassium without renal impairment, hypoaldosteronism should be consideredhypoaldosteronism should be considered..
**hyponatremiahyponatremia

Anesthetic managementAnesthetic management Preoperative preparation includesPreoperative preparation includes;;
**correction of fluid and electrolyte correction of fluid and electrolyte imbalanceimbalance
**exogenous mineralocorticoid, exogenous mineralocorticoid, fludrocortison 0.1-0.3 mg\ dayfludrocortison 0.1-0.3 mg\ day..

Glucocorticoid excessGlucocorticoid excess
Cushing syndromeCushing syndrome
Cushing syndrome is caused by prolonged Cushing syndrome is caused by prolonged exposure to elevated levels of either exposure to elevated levels of either endogenous glucocorticoids or exogenous endogenous glucocorticoids or exogenous glucocorticoidsglucocorticoids

CausesCauses::
--Exogenous steroid administrationExogenous steroid administrationSymptoms of glucocorticoid excess generally Symptoms of glucocorticoid excess generally
occur with the administration of oral steroids; occur with the administration of oral steroids; however, occasionally injections of steroids into however, occasionally injections of steroids into joints and the use of steroid inhalers can cause joints and the use of steroid inhalers can cause Cushing syndromeCushing syndrome..

Patients at risk to develop cushing syndrome Patients at risk to develop cushing syndrome includesincludes::
--rheumatological, pulmonary, neurological, and rheumatological, pulmonary, neurological, and nephrologic diseases that respond to steroid nephrologic diseases that respond to steroid therapytherapy..
--Patients who have undergone organ transplants Patients who have undergone organ transplants due to exogenous steroids required as part of due to exogenous steroids required as part of graft antirejection medication regimensgraft antirejection medication regimens..

Endogenous glucocorticoid administrationEndogenous glucocorticoid administration
--ACTH-producing pituitary adenoma ( Cushing ACTH-producing pituitary adenoma ( Cushing disease)disease)..
--Primary adrenal lesions; Overproduction of Primary adrenal lesions; Overproduction of glucocorticoids may be due to an adrenal glucocorticoids may be due to an adrenal adenoma, adrenal carcinoma, or macronodular adenoma, adrenal carcinoma, or macronodular or micronodular adrenal hyperplasiaor micronodular adrenal hyperplasia..

--Ectopic ACTH is sometimes secreted by oat Ectopic ACTH is sometimes secreted by oat cell or small-cell lung tumors or by carcinoid cell or small-cell lung tumors or by carcinoid tumorstumors

FrequencyFrequencyMost cases of Cushing syndrome are due to Most cases of Cushing syndrome are due to
exogenous glucocorticoids. Endogenous exogenous glucocorticoids. Endogenous Cushing syndrome has been estimated at 13 Cushing syndrome has been estimated at 13 cases per million individualscases per million individuals..
AgeAgeThe peak incidence of Cushing syndrome due to The peak incidence of Cushing syndrome due to
either an adrenal or pituitary adenoma is in either an adrenal or pituitary adenoma is in persons aged 25-40 yearspersons aged 25-40 years
Ectopic ACTH production due to lung cancer Ectopic ACTH production due to lung cancer occurs later in lifeoccurs later in life

SexSex
The female-to-male incidence ratio is The female-to-male incidence ratio is approximately 5:1 for Cushing syndrome due to approximately 5:1 for Cushing syndrome due to an adrenal or pituitary tumoran adrenal or pituitary tumor

Mortality/MorbidityMortality/Morbidity**Morbidity and mortality associated with Cushing Morbidity and mortality associated with Cushing
syndrome are related primarily to the effects of syndrome are related primarily to the effects of excess glucocorticoids. However, a large primary excess glucocorticoids. However, a large primary pituitary tumor may cause panhypopituitarism and pituitary tumor may cause panhypopituitarism and visual lossvisual loss..
**adrenocortical carcinomas are associated with a adrenocortical carcinomas are associated with a 5-year survival rate of 30% or less5-year survival rate of 30% or less..

* *multiple medical problems, including multiple medical problems, including hypertension, obesity, osteoporosis, fractures, hypertension, obesity, osteoporosis, fractures, impaired immune function, impaired wound impaired immune function, impaired wound
healing, glucose intolerance, and psychosishealing, glucose intolerance, and psychosis . .
* *adrenal crisisadrenal crisis

C\pC\p
ObesityObesity --moon faciesmoon facies--buffalo humpbuffalo hump
--Central obesity, increased waist-to-hip ratio Central obesity, increased waist-to-hip ratio greater than 1 in men and 0.8 in womengreater than 1 in men and 0.8 in women

SkinSkin Facial plethoraFacial plethora
abdominal striaeabdominal striae lanugo facial hairlanugo facial hair
Hirsutism and Steroid acneHirsutism and Steroid acne

Cardiovascular and renalCardiovascular and renal Hypertension and possibly edema may be Hypertension and possibly edema may be
present due to cortisol activation of the present due to cortisol activation of the mineralocorticoid receptor leading to sodium and mineralocorticoid receptor leading to sodium and water retentionwater retention
GastroenterologicGastroenterologic Peptic ulceration may occur with or without Peptic ulceration may occur with or without
symptomssymptoms . .

endocrineendocrine Galactorrhea and menstrual disturbancesGalactorrhea and menstrual disturbances
decreased libido and impotence in mendecreased libido and impotence in men..
Skeletal/muscularSkeletal/muscular Proximal muscle weaknessProximal muscle weakness
Osteoporosis and osteopeniaOsteoporosis and osteopeniaAvascular necrosis of the hipAvascular necrosis of the hip

NeuropsychologicalNeuropsychological
emotional liability, fatigue, and depressionemotional liability, fatigue, and depressionVisual-field defects, often bitemporal, and Visual-field defects, often bitemporal, and
blurred visionblurred vision
Adrenal crisisAdrenal crisis

InvestigationsInvestigations
Laboratory StudiesLaboratory StudiesHyperglycemiaHyperglycemia
Hypokalemic metabolic alkalosisHypokalemic metabolic alkalosis
Biochemical evaluation of Cushing syndromeBiochemical evaluation of Cushing syndrome::11--Urinary free cortisol excretion over 150 ug\ Urinary free cortisol excretion over 150 ug\
dayday..

22 - -dexamethasone suppression test; dexamethasone suppression test; glucocorticoids inhibit secretion of hypothalamic glucocorticoids inhibit secretion of hypothalamic CRH and pituitary ACTH but do not directly CRH and pituitary ACTH but do not directly affect adrenal cortisol production. The overnight affect adrenal cortisol production. The overnight 1-mg dexamethasone suppression test requires 1-mg dexamethasone suppression test requires administration of 1 mg of dexamethasone at administration of 1 mg of dexamethasone at 11 PM with subsequent measurement of cortisol 11 PM with subsequent measurement of cortisol level at 8 am.level at 8 am.44 In healthy individuals, the serum In healthy individuals, the serum cortisol level should be less than 2-3 ug/dLcortisol level should be less than 2-3 ug/dL..

33--loss of circadian rhythm of cortisol secretionloss of circadian rhythm of cortisol secretionNormal values, 10-25 ug\ml in the morning, 2-10 Normal values, 10-25 ug\ml in the morning, 2-10
ug\ml in the evening, elevated serum cortisol at ug\ml in the evening, elevated serum cortisol at 11 PM can be an early finding11 PM can be an early finding..
Recently, measuring salivary cortisol level has Recently, measuring salivary cortisol level has gained interest, as it is a simple and convenient gained interest, as it is a simple and convenient way of obtaining a nighttime sampl. levels less way of obtaining a nighttime sampl. levels less than 1.3-1.5 ng/mL exclude Cushing syndromethan 1.3-1.5 ng/mL exclude Cushing syndrome..

44 - -A plasma ACTH of less than 5 pg/mL is A plasma ACTH of less than 5 pg/mL is suggestive of a primary adrenal tumor. An ACTH suggestive of a primary adrenal tumor. An ACTH level greater than 10-20 pg/mL is consistent with level greater than 10-20 pg/mL is consistent with ACTH-dependent Cushing syndromeACTH-dependent Cushing syndrome..

Imaging studiesImaging studiesCT or MRI brain and abdomenCT or MRI brain and abdomen

TreatmentTreatment**Hypopysectomy for pituitary tumors, or Hypopysectomy for pituitary tumors, or
adrenalectomy for adrenal tumorsadrenalectomy for adrenal tumors..
**Pituitary irradiation is employed when Pituitary irradiation is employed when transsphenoidal surgery is not successful or not transsphenoidal surgery is not successful or not possiblepossible
**Patients with endogenous Cushing syndrome Patients with endogenous Cushing syndrome who undergo resection of pituitary, adrenal, or who undergo resection of pituitary, adrenal, or ectopic tumors should receive stress doses of ectopic tumors should receive stress doses of glucocorticoid in the intraoperative and glucocorticoid in the intraoperative and immediate postoperative periodimmediate postoperative period

**lifelong glucocorticoid and mineralocorticoid lifelong glucocorticoid and mineralocorticoid replacement is necessary in those patients who replacement is necessary in those patients who undergo bilateral adrenalectomyundergo bilateral adrenalectomy..

Anesthetic considerationsAnesthetic considerations
Preoperative managementPreoperative managementFrom the C\P those pt. Tend to be volume From the C\P those pt. Tend to be volume
overloaded, hypertensive and hypokalemic, so overloaded, hypertensive and hypokalemic, so Preoperative correction of these factors are Preoperative correction of these factors are essential by potassium and spironolactoneessential by potassium and spironolactone..

IntaoperativeIntaoperative Patients with osteoprosis are at risk for fracture Patients with osteoprosis are at risk for fracture
during positioningduring positioning..Preoperative weakness may indicate an Preoperative weakness may indicate an
increased sensitivity to muscle relaxantsincreased sensitivity to muscle relaxants..

Supplemental steroids are indicated forSupplemental steroids are indicated for;;--patients with Cushing syndrome due to patients with Cushing syndrome due to
exogenous glucocorticoidsexogenous glucocorticoids
--patients undergoing adrenalectomypatients undergoing adrenalectomyDose; I.V. hydrocortisone succinate 100 mg Dose; I.V. hydrocortisone succinate 100 mg
every 8 h beginning the evening before surgery every 8 h beginning the evening before surgery or on the morning of surgeryor on the morning of surgery..
Other complications of adrenalectomy include Other complications of adrenalectomy include significant blood loss and unintentional significant blood loss and unintentional
pneumothoraxpneumothorax..

Pseudo-Cushing SyndromePseudo-Cushing Syndrome
In 1976, Smalls and associates described 3 In 1976, Smalls and associates described 3 alcoholic patients who had the physical and alcoholic patients who had the physical and biochemical abnormalities of Cushing syndrome. biochemical abnormalities of Cushing syndrome. Most of the abnormalities disappeared with 1-3 Most of the abnormalities disappeared with 1-3 weeks of alcohol abstinence. About 30 cases weeks of alcohol abstinence. About 30 cases
have been reportedhave been reported..

PathophysiologyPathophysiologyThe mechanism remains unclear. Most evidence The mechanism remains unclear. Most evidence
suggests central stimulation of a corticotropin-suggests central stimulation of a corticotropin-releasing hormone, either at the hypothalamic or releasing hormone, either at the hypothalamic or
suprahypothalamic levelsuprahypothalamic level . .Persistence of abnormalities may lead to Persistence of abnormalities may lead to
complications such as hypertension, glucose complications such as hypertension, glucose intolerance, diabetes mellitus, and osteoporosisintolerance, diabetes mellitus, and osteoporosis..
The most important part of the history is the The most important part of the history is the extent and duration of alcohol abuseextent and duration of alcohol abuse..

Glucocorticoid deficiencyGlucocorticoid deficiency
Addison DiseaseAddison DiseaseThomas Addison first described the clinical Thomas Addison first described the clinical presentation of primary adrenocortical presentation of primary adrenocortical insufficiency )Addison disease( in 1855 in his insufficiency )Addison disease( in 1855 in his classic paper, On the Constitutional and Local classic paper, On the Constitutional and Local Effects of Disease of the Supra-Renal CapsulesEffects of Disease of the Supra-Renal Capsules..

PathophysiologyPathophysiology
Addison disease is adrenocortical insufficiency due Addison disease is adrenocortical insufficiency due to the destruction or dysfunction of the entire to the destruction or dysfunction of the entire adrenal cortex. It affects glucocorticoid and adrenal cortex. It affects glucocorticoid and mineralocorticoid function. The onset of disease mineralocorticoid function. The onset of disease usually occurs when 90% or more of both usually occurs when 90% or more of both adrenal cortices are dysfunctional or destroyedadrenal cortices are dysfunctional or destroyed..
FrequencyFrequency
The prevalence of Addison disease is 40-60 cases The prevalence of Addison disease is 40-60 cases per 1 million populationper 1 million population..

CausesCauses11 - -idiopathic autoimmune adrenocortical idiopathic autoimmune adrenocortical
insufficiencyinsufficiency..
22 - -Chronic granulomatous diseases; TB, Chronic granulomatous diseases; TB, sarcoidosis, histoplasmosissarcoidosis, histoplasmosis . .
33 - -Hematologic malignancies; as HodgkinHematologic malignancies; as Hodgkin
and non-Hodgkin lymphoma and leukemiaand non-Hodgkin lymphoma and leukemia . .

44 - -Metastatic malignant disease; as metastatic Metastatic malignant disease; as metastatic cancer of the lung, breast, colon or renal cell cancer of the lung, breast, colon or renal cell carcinomacarcinoma..
55--Infiltrative metabolic disorders; Amyloidosis Infiltrative metabolic disorders; Amyloidosis and hemochromatosisand hemochromatosis..
66 - -AIDSAIDS..

AgeAgeThe most common age at presentation in adults The most common age at presentation in adults
is 30-50 yearsis 30-50 years..
SexSexIdiopathic autoimmune Addison disease tends to Idiopathic autoimmune Addison disease tends to
be more common in females and childrenbe more common in females and children..

Secondary adrenal insufficiency is a result Secondary adrenal insufficiency is a result of inadequate ACTH secretion by the of inadequate ACTH secretion by the pituitary, the most common cause of pituitary, the most common cause of secondary adrenal insufficiency is secondary adrenal insufficiency is iatrogenic, the result of the administration iatrogenic, the result of the administration
of exogenous glucocorticoidsof exogenous glucocorticoids . .

C\PC\PPatients usually present with features of both Patients usually present with features of both
glucocorticoid and mineralocorticoid deficiency. glucocorticoid and mineralocorticoid deficiency. The predominant symptoms vary depending on The predominant symptoms vary depending on the duration of diseasethe duration of disease..
--Hyperpigmentation of the skin and mucous Hyperpigmentation of the skin and mucous membranes due to high ACTHmembranes due to high ACTH..
- -vitiligo, which most often is seen in idiopathic vitiligo, which most often is seen in idiopathic autoimmune Addison diseaseautoimmune Addison disease..

--clinical manifestations due to aldosteron clinical manifestations due to aldosteron deficiency; hyponatremia, hypovolemia, deficiency; hyponatremia, hypovolemia, hypotension, hyperkalemia and metabolic hypotension, hyperkalemia and metabolic acidosisacidosis

--clinical manifestations due to cortisol deficiency; clinical manifestations due to cortisol deficiency; weakness, fatigue, hypoglycemia, hypotension, weakness, fatigue, hypoglycemia, hypotension, and weight lossand weight loss..
--Prominent gastrointestinal symptoms may include Prominent gastrointestinal symptoms may include nausea, vomiting, and occasional diarrheanausea, vomiting, and occasional diarrhea..
- -Patients with Patients with secondary adrenal secondary adrenal insufficiencyinsufficiency have a history of tacking cortisol have a history of tacking cortisol..
- -acute adrenal crisisacute adrenal crisis

InvestigationsInvestigations
Laboratory StudiesLaboratory Studies--ACTH stimulation test; In patients with Addison ACTH stimulation test; In patients with Addison
disease, both cortisol and aldosterone show disease, both cortisol and aldosterone show minimal or no change in response to ACTHminimal or no change in response to ACTH..
--hyponatremiahyponatremia HyperkalemiaHyperkalemia
metabolic acidosismetabolic acidosis

--elevated )BUN( and creatinine due to the elevated )BUN( and creatinine due to the hypovolemia with decreased glomerular hypovolemia with decreased glomerular filtration ratefiltration rate..
--HypoglycemiaHypoglycemia
--adrenal autoantibodies may be presentadrenal autoantibodies may be present

Imaging studyImaging study
Chest x-ray TBChest x-ray TB
CT abdomenCT abdomen

TreatmentTreatment The goals of pharmacotherapy are to reduce morbidity The goals of pharmacotherapy are to reduce morbidity
and to prevent complications e.g adrenal crisisand to prevent complications e.g adrenal crisis;;11 - -ccorticosteroid: orticosteroid: Prednisone Prednisone 5-7.5 mg PO qd in am or 5 5-7.5 mg PO qd in am or 5
mg PO qd in am and 2.5 mg PO qd at 4-5 pmmg PO qd in am and 2.5 mg PO qd at 4-5 pm..
22 - -mineralocorticoid: mineralocorticoid: Fludrocortisone Fludrocortisone 0.05-0.1 mg PO qd; 0.05-0.1 mg PO qd; some patients may only require alternate-day dosingsome patients may only require alternate-day dosing..

Anesthetic considerationsAnesthetic considerations
Preoperative managementPreoperative management**ensure adequate replacement therapyensure adequate replacement therapy
**correct fluid and electrolytes disturbacescorrect fluid and electrolytes disturbaces

**for all patients who have received potentially for all patients who have received potentially suppressive doses of steroids, the daily suppressive doses of steroids, the daily equivalent of 5 mg of prednisone, by any route equivalent of 5 mg of prednisone, by any route of administration- topical, inhalational or oral-, of administration- topical, inhalational or oral-, for a period of more than 2 weeks any time in for a period of more than 2 weeks any time in the previous 12 months may be unable to the previous 12 months may be unable to
respond appropriately to surgical stressrespond appropriately to surgical stress . .

Adults normally secrete 20mg of cortisol daily, Adults normally secrete 20mg of cortisol daily, this may increase to over 300 mg under maximal this may increase to over 300 mg under maximal stressstress..
- -100100 mg of hydrocortisone phosphate every 8 h mg of hydrocortisone phosphate every 8 h beginning the evening before or on the morning beginning the evening before or on the morning of surgeryof surgery..

--an alternative low dose regimen, 25 mg of an alternative low dose regimen, 25 mg of hydrocortisone phosphate at the time of hydrocortisone phosphate at the time of induction followed by an infusion of 100 mg induction followed by an infusion of 100 mg during the subsequent 24 h, and this might be during the subsequent 24 h, and this might be appropriate for diabetic ptappropriate for diabetic pt..

IntaoperativeIntaoperative ensure adequate fluidensure adequate fluid..
PostoperativePostoperativeContinue the stress dose of steroids to gard Continue the stress dose of steroids to gard
against acute adrenal crisisagainst acute adrenal crisis..

1111 - -beta Hydroxylase Deficiencybeta Hydroxylase DeficiencyCongenital adrenal hyperplasia )CAH( is a Congenital adrenal hyperplasia )CAH( is a
general term used to describe a group of general term used to describe a group of inherited disorders in which a defect in cortisol inherited disorders in which a defect in cortisol biosynthesis is present with consequent biosynthesis is present with consequent overproduction of )ACTH( and secondary overproduction of )ACTH( and secondary adrenal hyperplasia as a consequenceadrenal hyperplasia as a consequence..
CausesCausesAn autosomal recessive diseaseAn autosomal recessive disease..

Patients with 11-beta-hydroxylase deficiency Patients with 11-beta-hydroxylase deficiency present with features of androgen excess, present with features of androgen excess, including masculinization of female newborns including masculinization of female newborns
and precocious puberty in male childrenand precocious puberty in male children . .
Approximately two thirds of patients also have Approximately two thirds of patients also have hypertension, which may or may not be hypertension, which may or may not be associated with mineralocorticoid excess, associated with mineralocorticoid excess, hypokalemia, hyperhypokalemia, hypernatremia natremia and metabolic and metabolic
alkalosisalkalosis . .

The hypertension is initially responsive to The hypertension is initially responsive to glucocorticoid replacement, but it may become a glucocorticoid replacement, but it may become a chronic condition subsequently requiring chronic condition subsequently requiring standard antihypertensive therapystandard antihypertensive therapy..

Addison Disease and PregnancyAddison Disease and Pregnancy
--Before glucocorticoid replacement therapy Before glucocorticoid replacement therapy became available, pregnancy in patients with became available, pregnancy in patients with adrenal insufficiency was associated with a adrenal insufficiency was associated with a
maternal mortality rate of 35-45%maternal mortality rate of 35-45% . .
--The usual glucocorticoid and mineralocorticoid The usual glucocorticoid and mineralocorticoid replacement dosages are continued throughout replacement dosages are continued throughout pregnancy. Some patients may require slightly pregnancy. Some patients may require slightly
more glucocorticoid in the third trimestermore glucocorticoid in the third trimester . .

During labor, adequate saline hydration and 25 During labor, adequate saline hydration and 25 mg of intravenous cortisol )ie, hydrocortisone mg of intravenous cortisol )ie, hydrocortisone sodium succinate( should be administered every sodium succinate( should be administered every
6 hours6 hours . .
At the time of delivery or if the labor is At the time of delivery or if the labor is prolonged, high-dose parenteral hydrocortisone prolonged, high-dose parenteral hydrocortisone should be administered )100 mg q6h or as a should be administered )100 mg q6h or as a
continuous infusion(continuous infusion( . .

After delivery, the dosage can be quickly After delivery, the dosage can be quickly tapered to a maintenance dose in 3 daystapered to a maintenance dose in 3 days..

Cushing Syndrome and PregnancyCushing Syndrome and PregnancyThe risk of maternal morbidity and a poor fetal The risk of maternal morbidity and a poor fetal
outcome is significant when Cushing syndrome outcome is significant when Cushing syndrome coexists with pregnancycoexists with pregnancy . .
Maternal hypertension may antedate the Maternal hypertension may antedate the pregnancy but becomes worse in two thirds of pregnancy but becomes worse in two thirds of patientspatients..

Preeclampsia or pregnancy-induced Preeclampsia or pregnancy-induced hypertension is noted in approximately 10% of hypertension is noted in approximately 10% of patientspatients..
Gestational DM occurs in approximately one thirdGestational DM occurs in approximately one third..
Congestive heart failure associated with severe Congestive heart failure associated with severe hypertension occurs in 10%hypertension occurs in 10%..

Wound breakdown after surgery is possibleWound breakdown after surgery is possible . .
Severe proximal myopathy and mental problems Severe proximal myopathy and mental problems ranging from emotional lability to profoundranging from emotional lability to profound
psychosis should be added to the list of medical psychosis should be added to the list of medical problems that may occurproblems that may occur..

Primary Hyperaldosteronism and PregnancyPrimary Hyperaldosteronism and PregnancyPatients present with hypertension, Patients present with hypertension,
hypokalemia, and elevated urine potassium hypokalemia, and elevated urine potassium levelslevels..
The goals of medical therapy should be The goals of medical therapy should be adequate control of blood pressure and adequate control of blood pressure and replacement of potassiumreplacement of potassium

spironolactone and angiotensin-converting spironolactone and angiotensin-converting enzyme inhibitors, are contraindicated in enzyme inhibitors, are contraindicated in
patients who are pregnantpatients who are pregnant . .
Methyldopa, beta-blockers, and calcium channel Methyldopa, beta-blockers, and calcium channel blockers have been used with variable outcomesblockers have been used with variable outcomes