Embed Size (px)
Citation preview
Acute inflammation 1
By Dr. S. Homathy

Clinical example of acute inflammation
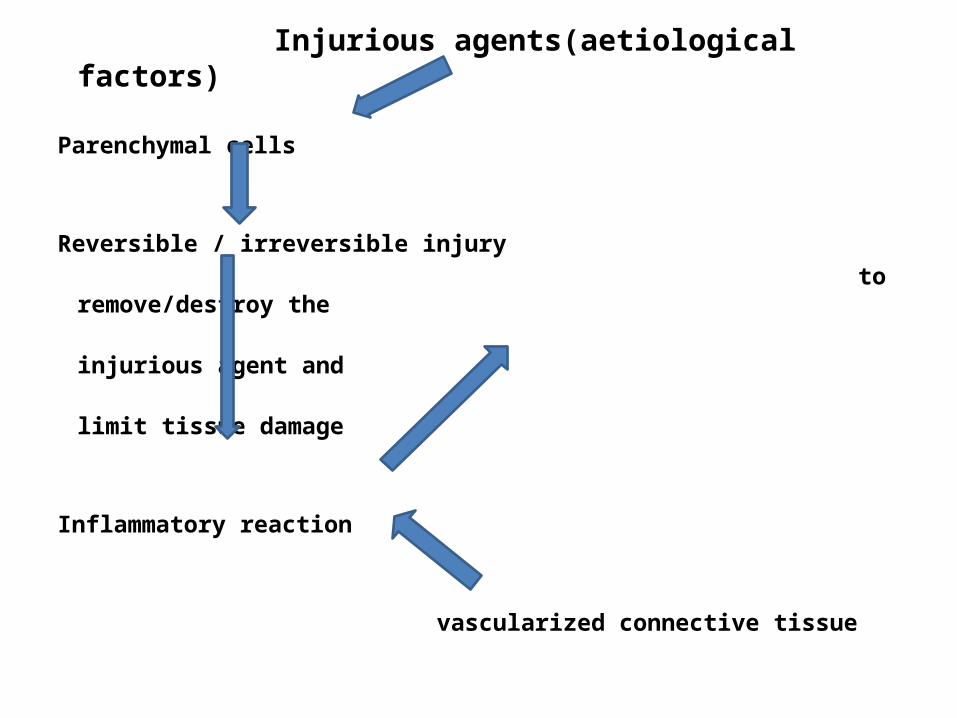
Injurious agents(aetiological factors)
Parenchymal cells
Reversible / irreversible injury
to remove/destroy the
injurious agent and
limit tissue damage
Inflammatory reaction
vascularized connective tissue
Pathological process
Alteration in the structure and function of tissues
Direct effects reactive changes in
of injurious agents vascularized CT
on tissues
Cell injury macroscopic and
microscopic changes
Definition of Inflammation
It is a protective response of the vascular and
supporting elements of a tissue to injury
Result in the formation of a protein – rich
exudate
To prevent further injury to tissues and to remove
or destroy the injurious agent and initiate repair.
• Although it is help full, it has considerable potential to cause harm
Eg :Anaphylactic reaction to insect bite / drugs.Chronic diseases- rheumatoid arthritis /
atherosclerosisIntestinal obstruction following inflammation
in the peritoneum.

Causative agents
InfectiousPhysicalChemicalTissue NecrosisForeign Bodies (FBs)Immune “responses”, or “complexes” /
hypersensitivity reactionsAround the neoplasm
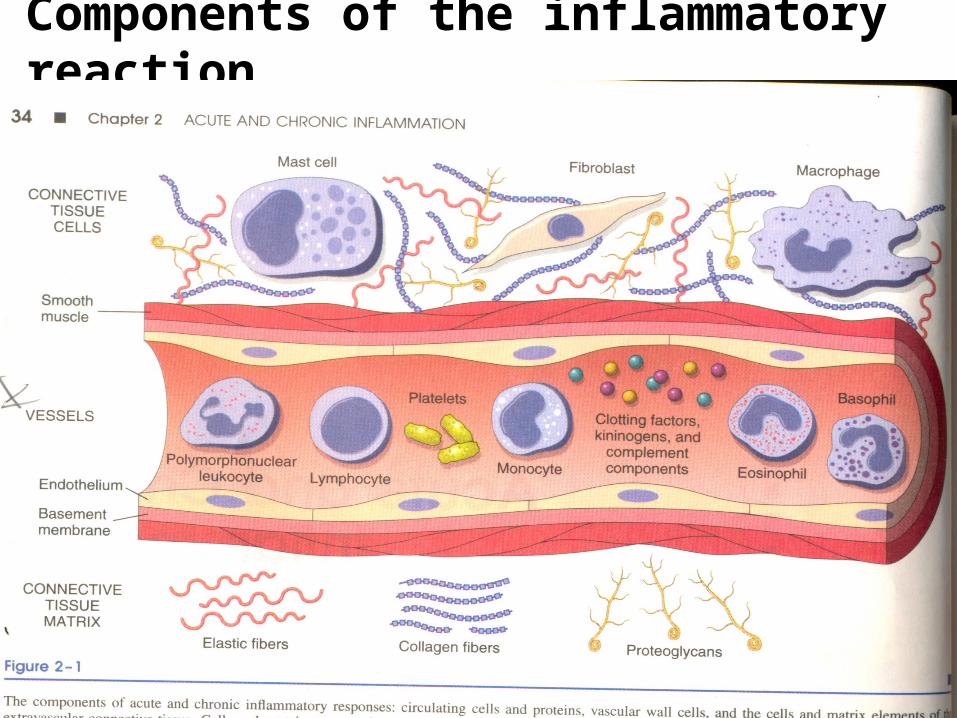
Components of the inflammatory reaction
Components of the inflammatory reaction
Circulating cells - N, E, B, L, Monocytes, platelets
Plasma proteins- clotting factors, Kininogens, complement components
Vascular wall cells – endothelial cells and smooth muscle cells.
Connective tissue cells – fibroblast and macrophages
Extracellular matrix – collagen, elastin, proteoglycan, fibronectin
Inflammatory response involve a highly complex set of events.
• Initial inflammatory stimulus
• Triggers the release of chemical mediaters from plasma and connective tissue cells

• Soluble mediators acting together or in sequence amplify the initial reaction
• Influence its evolution by vascular and cellular response.
• Inflammatory response is terminated when – Injurious stimulous is removed– Inflammatory mediators are dissipated, catabolized
/ inhibited
Inflammation
Acute inflammation Short durationLast for minutes to few
daysCharacterized by fluid
and plasma protein exudation
Neutropil leukocyte infiltration
Chronic inflammationLonger durationLast for days to yearsVascular proliferation
and scaringInflux of lymphocytes
and macrophages.
Acute inflammationIt is immediate and early response to injury
Designed to deliver leukocytes to the sites of injury
Leukocytes clear any invading microbes
Begin the process of breaking down necrotic tissues.
Cascade of events is integrated by local release of chemical mediators

It has two major componentsVascular changes
Changes in vascular caliber and flow- change in the caliber of
vesselsCauses increased blood flow
Increased vascular permeability
Structural changes permits
plasma proteins and
leucocytes to leave the
circulation
Cellular events
Cellular recruitment and activation
– Emigration of leukocytes
from the microcirculation
– Accumulate in the focus
of injury
Cardinal macroscopic changes
Vascular changes and cellular events produce
3 of the 5 classical local signs of acute
inflammation
Additional features are the consequences of mediators and leukocyte- mediated damage.
Local manifestations
• Heat (calor) described• Redness (rubor) by• Swelling (tumor) Cornelius Celsus• Pain (dolor) (1st century AD)
• Loss of function ( functio laesa)………………. ……………(described by Virchow-19th century)
Systemic manifestations
• Fever• Chills• Myalgia• Malaise
Process of acute inflammation
1. Transient vasoconstriction( within seconds)
2. Arteriolar vasodilation
3. Increased vascular permeability
4. Retardation of blood flow and stasis
5. Leukocyte extravasations and phagocytosis
6. Fibrin formation
7. Role of lymphatics
Vascular changes 1.Acute arteriolar vasodilation
Opens microvascular beds
Locally increased blood flow
Engorgement of the down-stream capillary beds
causes of increased heat and redness
Increased intravascular pressure causes an early
transudate (protein-poor filtrate of plasma) into
interstitium (vascular permeability still not increased yet)
2.Increasefd Vascular permeability (leakiness) commences– Transudate gives way to exudate (protein-rich)– Increases interstitial osmotic pressure contributing to
edema (water and ions)
• Accumulation of fluid in the extracellular space
Swelling pain due to increased pressure
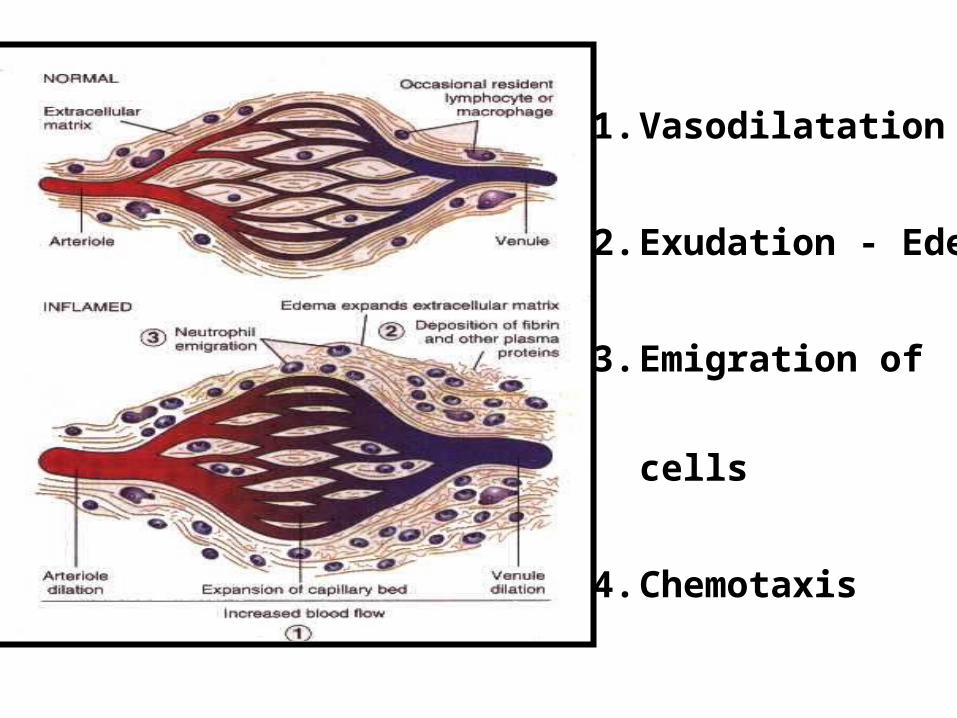
8021`1. Vasodilatation
2. Exudation - Edema
3. Emigration of cells
4. Chemotaxis

3.Retardation of blood flow and stasis
outpouring of albumin rich fluid into the extravascular
tissues results
in the concentration of RBCs in small vessels and
increased viscosity of blood.
Rouleux formation of red cells further increase the viscosity
Neutrophi become oriented at the periphery of vessels and
start to stick
Swelling of the endothelium
Increase of surrounding tissue pressure
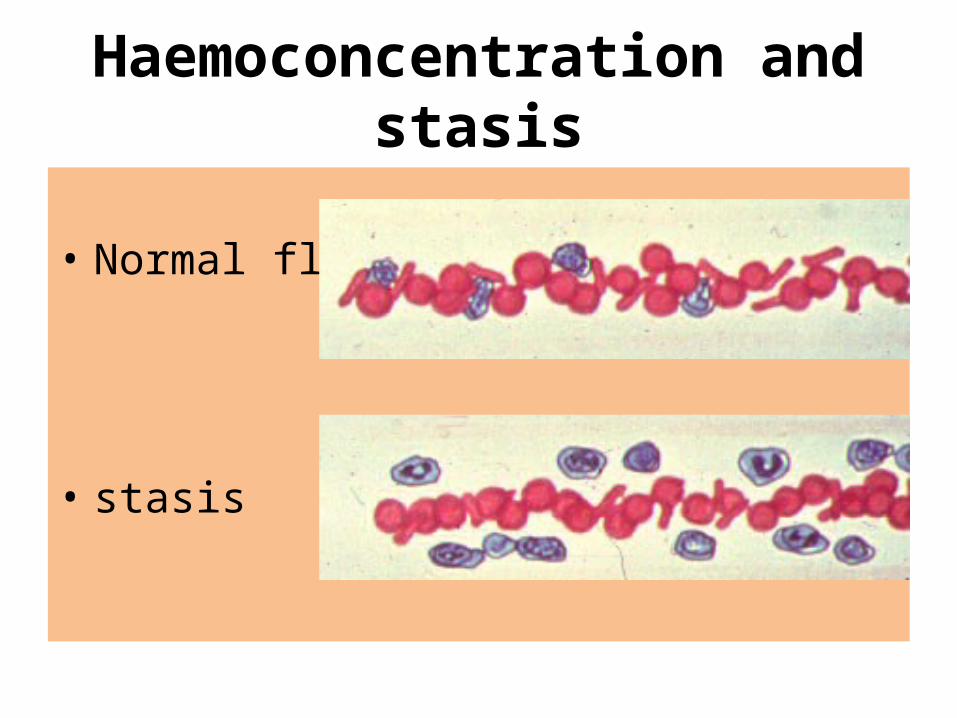
Haemoconcentration and stasis
• Normal flow
• stasis
Transudate:
An ultrafiltrate of blood plasma
permeability of endothelium is usually normal.
low protein content ( mostly albumin)
usually caused by alterations in hydrostatic or oncotic pressure.Implies a hydrostatic (pressure) problem
Exudate:
A filtrate of blood plasma mixed with inflammatory
cells and cellular debris.
permeability of endothelium is usually altered
high protein content.
caused by increased vascular permeability.
Implies an inflammatory process
• LEAKAGE OF PROTEINACEOUS
FLUID (EXUDATE, NOT TRANSUDATE)
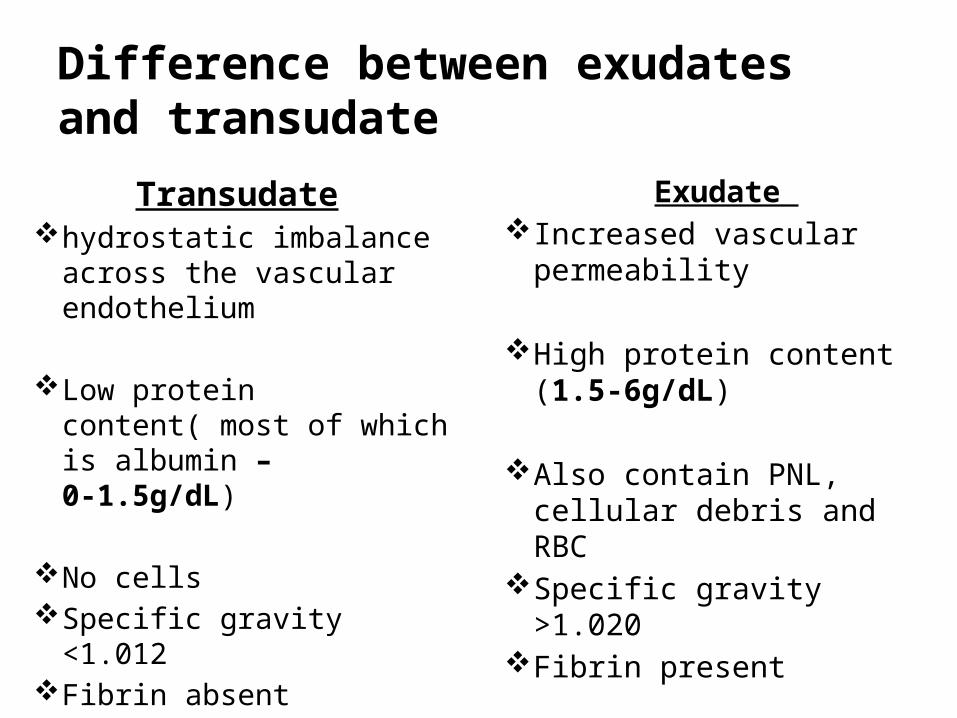
Difference between exudates and transudate
Transudate hydrostatic imbalance
across the vascular endothelium
Low protein content( most of which is albumin – 0-1.5g/dL)
No cellsSpecific gravity <1.012Fibrin absent
Exudate Increased vascular
permeability
High protein content (1.5-6g/dL)
Also contain PNL, cellular debris and RBC
Specific gravity >1.020Fibrin present
• Fluid appears grossly clear.
• Fluid appears grossly cloudy