Embed Size (px)
Citation preview

The Rules of Stopping Biologics: A European Perspec9ve
Alessandro Armuzzi, MD, PhD
IBD Unit
Complesso Integrato Columbus – Catholic University
Rome, Italy

How long for?
34.7%
27.4%
0 0 3 6 9 12 15 18 21 24
10
20
30
40
Time (months)
Hospitalisa9
on, surgery
or com
plica9
ons (%
)
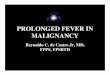
HR (95% CI) = 0.73 (0.62, 0.86), p<0.001
Khanna R, et al. Lancet 2015
CM ECI
REACT 1: Dme to first hospitalisaDon, surgery or complicaDon
Early combined immunosuppression bears a poten9al to slow down diges9ve damage in CD
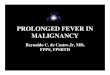
Adapted from Louis E et al. Gut. 2001
10 years: P<0.0001
Change at 1 Year: P=0.04
Inflammatory Stricturing
Fistulizing
Crohn’s disease long-‐term behaviour

Avoidance of long-‐term bowel
damage and subsequent disability
Treat-‐to-‐target concepts in IBD
Adapted from Bouguen G, et al. ClGH 2014 Peyrin-‐Biroulet L, et al. AJG 2015
Target Target Low
High
Baseline assessment Assessment Assessment
Iden'fica'on of a pre-‐defined
objec've target
Unreached target
How long for?

Prac9cal short-‐ and long-‐term common goals in the management of IBD
- Induce
clinical (+ endoscopic) remission
- Maintain
clinical (+ endoscopic) steroid-free remission
- Prevent complications (disease- and therapy-related)
- Optimise timing of surgery
- Improve patient-QoL

Benefits and risks of anti-TNFs in IBD
Benefits
● Efficacious for moderate to severe and/or IM-‐refractory IBD
● Important role in accelerated Step-‐up/Top-‐Down strategies
● High poten9al for MH
● Reduc9on in hospitaliza9on/surgeries (?)
● Improved quality of life
● Preven9on of disease progression/complica9ons (+/-‐)
Risks
● Allergic reac9ons
● Cutaneous reac9ons
● (Dys)Immune disorders
● Infec9ons (severe, opportunis9c)
● Tumours and lymphomas
● Costs

Why should we stop an9-‐TNFs (biologics) in IBD? (… if they keep working on a pa9ent)
• Medical reasons (Benefit/Risk) – Over-‐treatment of long-‐9me remieers – Safety concerns
• PaDents may ask for it – Convenience – Pa9ents do not like to take drugs – Pa9ents may be afraid of complica9ons – Specific situa9ons (e.g. pregnancy, elderly)
• Payor push back/cost – Medical costs

Waugh AW et al. APT 2010
Reason for discon9nuing an9-‐TNFs while in clinical remission
Reason N (%)
Physician choice 14 (32.6)
Loss of insurance 8 (18.6)
Pa9ent choice 8 (18.6)
Adverse events 7 (16.3)
Pregnancy 6 (13.9)

Lichtenstein G, et al. AJG 2012
Incidence of infec9ons in the TREAT registry
Treatment group Number
of paDents
Number of
events
Number of paDent-‐years
Unadjusted rate
per 100 paDent-‐years
Unadjusted RR (95% CI) raDo
P value
Serious infecDon
Other treatments only 4557 147 14710 1.00 1.00 (ref)
Infliximab treated 3420 333 16296 2.04 2.04 (1.45, 2.89) <0.001
Serious infecDon according to infliximab exposure within the previous 3 months
Other treatments only 5597 317 22344 1.42 1.00 (ref)
Infliximab treated 2942 163 7923 2.06 1.45 (1.10, 1.91) 0.008
● ProspecDve, mulDcentre, observaDonal registry (USA + Canada) ● 6273 paDents, 5.2 years mean follow-‐up (>30,000 pa9ent-‐years)

p=0.011
-‐CS 0
5
10
15
% PaD
ents with
seriou
s infecDon
+CS -‐CS +CS -‐IMM +IMM
-‐IMM +IMM
171/2329 93/913 120/1228 68/591 264/3242 188/1819
7.3
10.2 9.8 10.7
8.1
10.3
p=0.01
p=0.014
p=0.048
D’Haens G et al. UEGW 2013. Abstract OP214.
Incidence of infec9ons in the PYRAMID registry
PYRAMID: mul9centre, uncontrolled, 6-‐year non-‐interven9onal registry to evaluate the long-‐term safety of adalimumab • 5061 pa9ents enrolled and treated • Cumula9ve ADA exposure: 13,914.2 pa9ent-‐years • Median dura9on of cumula9ve exposure: 3.02 years (range 0.04–5.11)

D’Haens G et al. UEGW 2013. Abstract OP214.
Incidence of infec9ons in the PYRAMID registry (results at year 5)
Any ADA All paDents Events/100
PY
Any ADA Age (years)
Events/100 PY
N=5061 13351 PY
<40 yrs N=2999 7815 PY
40–65 yrs N=1907 5152 PY
≥65 yrs N=155 383 PY
Serious AE 3389 (25.4) 1978 (25.3) 1244 (24.1) 167 (43.5)
AE leading to disconDnuaDon
530 (4.0) 306 (3.9) 199 (3.9) 25 (6.5)
InfecDon 928 (7.0) 576 (7.4) 305 (5.9) 47 (12.3)
Serious infecDon 596 (4.5) 373 (4.8) 184 (3.6) 39 (10.2)
Malignancy 90 (0.7) 23 (0.3) 57 (1.1) 10 (2.6)
IntesDnal stricture 412 (3.1) 245 (3.1) 160 (3.1) 7 (1.8)

Incidence of non-‐Hodgkin’s T-‐cell Lymphomas in the REFURBISH study
Deepak P et al. Am J Gastroenterology 2013;108:99–105.
Thio
AnD-‐TNF
AnD-‐TNF with thio
Thio
AnD-‐TNF
AnD-‐TNF with thio
0.01
p<0.0001
p=1.00
p<0.0001
p<0.0001
p=1.00
p<0.0001
10 1 0.1 1000 10000 Odds raDo with 95% confidence intervals
100
Type of therapy
T-‐NHL
HSTCL
95% CI 5 - 354
95% CI 8 - 945
95% CI 3 - 993
95% CI 7 - 3045

Van der Walk ME, et al. Gut 2014
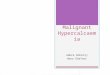
Healthcare costs of IBD have shiped from hospitalisa9on and surgery towards an9-‐TNFα therapy (COIN study)
Comparison of distribu9on of healthcare costs
1315 CD pa9ents and 937 UC pa9ents Cost items were derived from a 3 month follow-‐up web-‐based ques9onnaire Costs were expressed as mean 3-‐month costs per pa9ents

Long-‐term “real-‐life” experiences with an9-‐TNFs in IBD
Schnitzler F, et al. Gut 2009; Baert F, et al. J Crohns Coli9s 2013; Armuzzi A et al. Dig Liver Dis 2013; Armuzzi A , et al. Inflamm Bowel Dis 2014
CD -‐ IFX
CD -‐ ADA
UC -‐ IFX
UC -‐ ADA
≈ 2/3 of paDents are in “sustained“ clinical benefit at long-‐term follow up

An9-‐TNF Withdrawal in IBD: Relapse and Recapture Rates and Predic9ve Factors From 160 Pa9ents in a Pan-‐UK Study
Kennedy NA, et al. DDW 2015:S62
-‐ 160 IBD in CS-‐free remission -‐ median follow-‐up 9me: 25 months post withdrawal -‐ Younger age at diagnosis (p<.003) and elevated WCC(p<.04) predic9ve of relapse -‐ Re-‐introduc9on of an9-‐TNF successful in 92%

Casanova Gonzalez MJ, et al. UEGW 2015:OP92
Evolu9on aper an9-‐TNF drug discon9nua9on in IBD (mul9center retrospec9ve observa9onal study – Spain)
1) Relapse aper discon9nua9on: Incidence rate: 18% per pts-‐yr (95%CI 17-‐20)
1055 IBD (69% CD) in which an9-‐TNFs had been withdrawn aper clinical remission
2) Lower risk of relapse (mul9variate): IM treatment aper discon9nua9on (HR 0.7, 95%CI 0.6-‐0.9)
3) 69% of relapsers retreated with the same agent: 75% remission at FU, 11% mild adverse events

Louis E, et al. Gastroenterology 2012
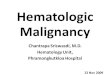
115 CD paDents in remission on IFX+AZA (CDAI<150 and steroid free ≥6 months)
Factor HR (95%CI) P
No previous surgery 4.0 (1.4-‐11.4) 0.01
Steroids (month -‐12 to -‐6) 3.5 (1.1-‐10.7) 0.03
Hemoglobin ≤ 14.5 (g/dl) 6.0 (2.2-‐16.5) <0.001
Male Gender 3.7 (1.9-‐7.4) <0.001
Fecal calpro ≥ 300 μg/g 2.5 (1.1-‐5.8) 0.04
Infliximab TL ≥ 2 mg/L 2.5 (1.1-‐5.4) 0.02
WBC > 6 (103/ml) 2.2 (1.2-‐4.2) 0.01
CRP hs > 5 (mg/l) 3.2 (1.6-‐6.4) <0.001
CDEIS > 0 2.3 (1.1-‐4.9) 0.04
Median follow up 28+/- 2 months
52.2% relapse 43.9% relapse
Maintenance of remission among pa9ents with CD on an9-‐metabolite therapy aper IFX therapy is stopped (STORI)

Bessissow T, et al. AJG 2012
75 UC pa9ents with Mayo endo score = 0 and 1-‐year FU
Factors OR (95% CI) P
Basal plasmacytosis 5.13 (1.32-‐19.99) 0.019
Biologics 0.24 (0.05-‐1.01) 0.052
Prognos9c Value of Histologic Markers on Clinical Relapse in Ulcera9ve Coli9s Pa9ents With MH

DE-‐ESCALATION OF BIOLOGICS IN IBD
Systema9c Review of Effects of Withdrawal of IM or Biologic Agents From Pa9ents with IBD
• 69 studies (4672 paDents): 18 on de-‐escala9on (drug cessa9on or dose reduc9on) of immunomodulator monotherapy
8 on immunomodulator de-‐escala9on from combina9on therapy
43 on de-‐escala9on of an9-‐TNF agents
• Stopping IM monotherapy aper a period of remission was associated with high rates of relapse in pa9ents with Crohn’s disease or ulcera9ve coli9s (around 75% relapse by 5 years aper therapy was stopped)
• Most studies of paDents with CD who disconDnued the immunomodulator aoer combo therapy found that rates of relapse did not differ from those of paDents who conDnued taking the drug (55%–60% had disease relapse 24 months aoer stop)
• Approximately 50% of paDents who disconDnued anD-‐TNF agents aoer combo therapy maintained remission 24 months later, but the proporDon decreased with Dme.
Torres J. et al, Gastroenterology 2015 Sept 14

Steroid-‐free deep remission in CD does not prevent disease relapse aper an9-‐TNF withdrawal
61 CD (77% AZA / 6MP): median FU 28 months (7-‐47)
Deep remission: Mucosal healing CalprotecDn <150 CRP <5 mg/L
Bortlik M. et al, Scand J Gastroenterol 2015

Relapse Rate Aper Discon9nuing an9-‐TNF in long-‐term deep remission is lower when nil drug levels
Ben-‐Horin S, APT 2015
48 paDents stopped IFX (n=35) or adalimumab (n=13) in deep endoscopic remission
Undetectable drug
Measurable drug levels
P<0.001 (Log rank test)
Months since anti -
TNF cessation

Long-‐Term Outcome of Pa9ents With CD Who Discon9nued Infliximab Therapy Upon Clinical Remission
Papamichael K, et al. CGH 2015

MAINTENANCE RETREATMENT
Infusion reac9ons (IR) 0-‐20%
Clinical benefit 55-‐98%
Domenech E, et al. 2010; Steenholdt C, et al. 2012; Laharie D, et al. 2009; Louis E, et al. 2012; Molnàr T, et al. 2013, Baert F, et al. 2014, Felice C, et al. 2014; Brandse JF, et al. 2014
Pre-‐medica9on Scheduled maintenance
Concomitant immunomodulators (IMM)
Episodic treatment Standard re-‐induc9on
Ab an9-‐IFX
RISK OF IR
Fidder H, et al. 2003; Fidder H, et al. 2009; Hanauer S, et al. 2004; Crandall C, et al. 2003; Laharie D, et al. 2009; Baert F, et al. 2014, Felice C, et al. 2014; Colombel JF, et al. 2004; Lees C, et al. 2009; Zabana E, et al. 2010
Retreatment with IFX in IBD

• CD patients retreated with VDZ after up to 1 year of drug holiday regained response • Similar trends observed with VDZ retreatment in subpopulations of completers or early terminators with
prior anti-TNF failure • No increase in AEs or SAEs observed with VDZ retreatment in completers/early terminators
Efficacy and Safety of Retreatment With Vedolizumab in Pa9ents With Crohn's Disease
Sands BE et al. DDW 2015:S-‐278
GEMINI II Completers GEMINI II Early Terminators
Visit PBO
(n=60) VDZ q8w
(n=69) VDZ q4w
(n=76) PBO
(n=59) VDZ q8w
(n=57) VDZ q4w
(n=40) Patients with clinical remission* (%)
GEMINI II
Week 6
Week 26
Week 52
48
50
52
46
71
74
51
62
68
44
22
NA
25
5
NA
28
8
NA
GEMINI Long term safety Week 0
Week 28
Week 52
Week 84
Week 108
53
70
63
52
37
77
73
70
51
32
71
75
68
55
34
9
48
44
42
34
4
23
32
26
25
10
28
25
23
23
*Defined as Harvey-Bradshaw Index score ≤4

Early Trough Levels and An9bodies to Infliximab Predict Safety and Success of Reini9a9on of Infliximab Therapy
128 IBD who restarted IFX aper a median 15-‐month discon9nua9on (range, 6–125 mo):
-‐ 84.5% short-‐term response -‐ 61% long-‐term response
Baert F, et al. CGH 2014

IFX + AZA IFX dose-‐escalaDon + AZA
IFX + AZA
AZA IFX reintroducDon
6 months steroid-‐free remission
IFX IFX dose escalaDon
AZA reintroducDon
Relapse
A proSpective randomized controlled trial comParing infliximAb-antimetabolites combination therapy to anti-metabolites monotheRapy and infliximab monothErapy in patients with Crohn’s disease in sustained steroid-free remission on combination therapy
RandomisaDon

Conclusion 1. The op9mal dura9on of biological therapy is s9ll unknown
2. Many factors are involved in the decision to stop biologics (“mul9ple rules”)
3. In clinical prac9ce, reflect on: a) pa9ent’s demographics, b) disease features, c) treatment
history, d) current disease status,
and discuss with the pa9ent about risk/benefit of the strategy on the long-‐term (case by case)
4. Stopping biologics may be jus9fied to op9mize benefit/risk (… and benefit/cost), but should not jeopardize 9ght disease control
5. Approximately 50% of pa9ents who stop biologics have a relapse within 2 years (…. but 50% will not!)
6. The majority of pa9ents who receive retreatment with biologics aper their discon9nua9on will achieve again clinical benefit (TL and concomitant IM!)