Embed Size (px)
Citation preview

MalignantHypercalcaemi
a
Ambre DohertyAmna Ghafoor

Introduction Normal range: 2.2-2.6 mmol/L Free Ca2+ ≥ 3.0 mmol/L = EMERGENCY [1] Ca2+ ≥ 4.0 mmol/L leads to death [2] Hypercalcaemia develops in 10% of cancers [3] Poor prognosis
o 80% die in first year even with treatment [2,4] Most common in breast cancer, multiple
myeloma and lung cancer (also prostate cancer, lymphoma, and renal cancer) [1-3]
50% of inpatient hypercalcaemia is caused by cancer [3]

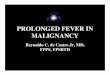
Calcium Physiology
Adapted from Wallis DE, Penckofer S and Sizemore GW, 2008. [5]
PTH
↑Ca2+
calcidiol calcitriol
Vitamin D3 from SKIN
calcitonin
-
+
+
+
+
+
-
-

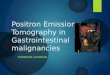
Aetiology
Adapted from Wallis DE, Penckofer S and Sizemore GW, 2008. [5]
OSTEOLYSISTumour cells activate osteoclasts locally – bone resorption
HUMOURAL MEDIATORSParathyroid-related protein (PTHrP) expressed in “normal” cells. Also secreted by tumour cells.Acts like PTH:• Bone
resorption• Distal tubule
calcium resorption DEHYDRATION
Calcium is a potent diuretic – salt and water loss

Polyuria Polydypsia Uraemia Hypercalciuria Nephrocalcinosis
Drowsiness Weakness Confusion Diminished reflexes
Clinical Manifestations Anorexia Constipation Nausea Vomiting
Pain (bone, abdo) Weakness Cardiac arrhythmia

Investigations FBC U&Es, corrected serum Ca2+, PO4-, Mg2+
LFTs Plasma PTH ?and PTHrP [6]
Calcidiol and calcitriol levels [6]
ECGo PR interval elongation, o shortening of QT interval or o a wide QRS complex

ManagementConsider the aims of treatment!1. Rehydration- IV 0.9% saline and monitor via catheter.
Ideally 3-6 L/24h.2. Encourage mobility 3. Ca2+ restriction4. Monitor U&Es- Ca2+ and albumin daily and monitor K+
and Mg2+ 5. Bisphosphonates- if 24 hours rehydration does not
lower corrected Ca2+ but risk metastatic calcium phosphate deposition.[7]
IV Pamidronate infusion. Takes 48 hours to work. Ca2+ stabilises in 3-7 days. Works in 70% of patients but need to repeat in 1-3 weeks as high recurrence rate. [4]

Management6. Salmon calcitonin – if severely symptomatic7. Loop Diuretics – furosemide, prevent fluid overload8. Corticosteroids – hematological malignancy, pain9. ? Treat underlying malignancy
Future directions[8]
Denosumab – - blocks RANKL- Secreted by osteoblasts, activates osteoclasts- For persistent/relapsed hypercalcaemia of malignancy

References1. Cassidy J, Bissett D, Spence R, Payne M, editors. Oxford handbook of
oncology. 3rd ed. Oxford: Oxford University Press; 2010.2. Watson M, Barrett A, Spence RAJ, Twelves C. Oncology (oxford core
texts). 2nd ed. Oxford: Oxford University Press; 2006. 3. Bower M, Waxman J. Oncology (lecture notes). 2nd ed. Chichester:
Wiley-Blackwell; 2010.4. Legrand SB. Modern management of malignant hypercalcaemia. Am
J Hosp Palliat Care. 2011 Nov;28(7):515-7. 5. Wallis DE, Penckofer S, Sizemore GW. The “sunshine deficit” and
cardiovascular disease. Circulation. 2009 Sep 30;118(14):1476-85.6. Clinical Key Elsevier: Hypercalcaemia associated with malignancy
[online]. 2012. [Accessed 2014 Feb 27]: [1 screen]. Available from: https://www.clinicalkey.com/#!/ContentPlayerCtrl/doPlayContent/21-s2.0-2001273/{"scope":"all"}
7. Donald A, Stein M, Scott Hill C. The hands-on guide for junior doctors. 4th ed. Chichester: Wiley-Blackwell; 2011
8. Hu MI, Glezerman I, Leboulleux S, et al; Denosumab for patients with persistent or relapsed hypercalcemia of malignancy despite recent bisphosphonate treatment. J Natl Cancer Inst. 2013 Sep 18;105(18):1417-20. doi: 10.1093/jnci/djt225. Epub 2013 Aug 29.