Embed Size (px)
Citation preview
8001-17Update on Published
CAP/ASCP/ASCO HER2 Testing and Clinical Decision Making
in Gastroesophageal Adenocarcinoma
Kay Washington, MD, PhD
Vanderbilt University Medical Center
DISCLOSURE
In the past 12 months, I have not had any significant financial interest or other relationship with the manufacturers of the products or providers of the services that will be discussed in my presentation.
Objectives
3
• Present the Guideline for HER2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma
• Review guidance to oncologists to:
• Help identify appropriate patients for HER2-targeted therapy
• Help identify which patients to test for HER2-targeted therapy
Objectives
4
• Provide guidance to pathologists on:
• Choosing the appropriate specimens to test for HER2
• How to test for HER2 expression/amplification
• How to interpret and report the test results to clinicians and patients
Objectives
5
• Introduction to ERBB2 (HER2), background and history in GEA and breast
• Methodology of Guideline process
• Clinical background on HER2 in GEA
• HER2 as a prognostic indicator
• Specimen selection for HER2 testing
• Immunohistochemistry (IHC) and in-situ hybridization (ISH) testing and interpretation
Objectives
6
• Brief discussion on HER2 genomic testing
• Reporting HER2 results and turnaround time (TAT)
• Summary of the Guideline and new directions with mention of ongoing clinical trials
Gastroesophageal Adenocarcinoma (GEA)
• Esophageal: 8th
• Stomach: 5th
• Most common cancers worldwide
• Often diagnosed at an advanced stage
• Therapies are limited
7
http://www.cancernetwork.com
8
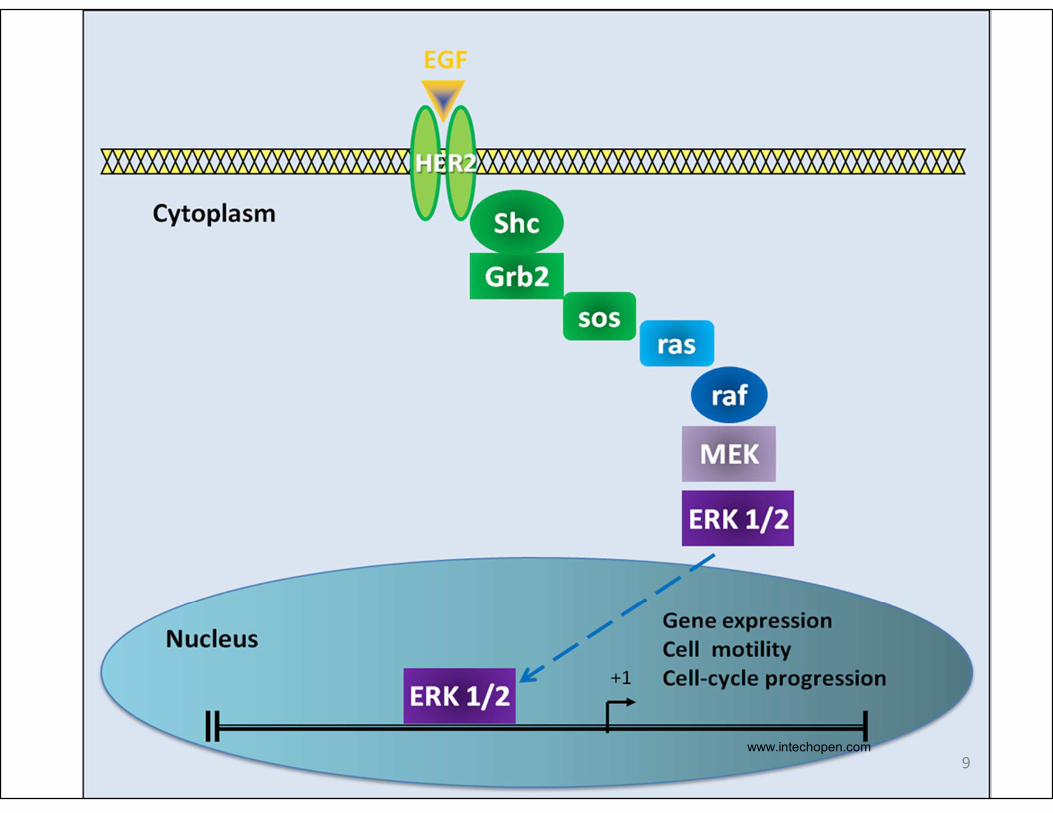
HER2 (ERBB2)
9www.intechopen.com
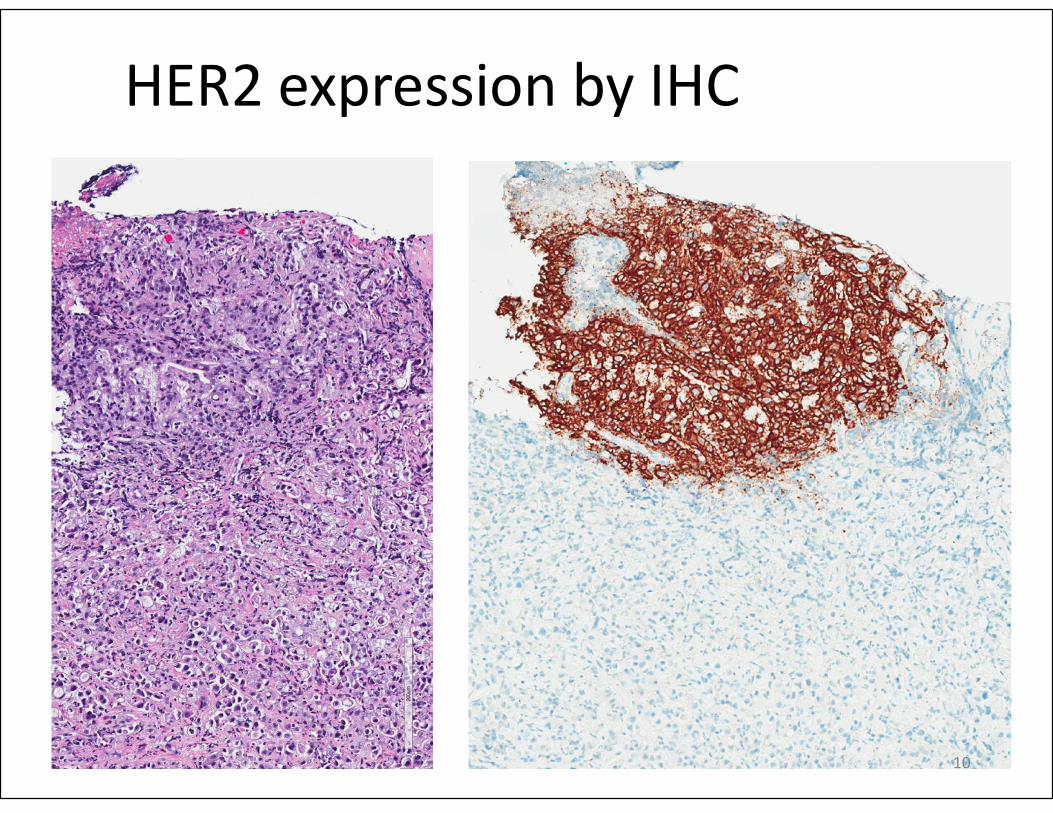
HER2 expression by IHC
10
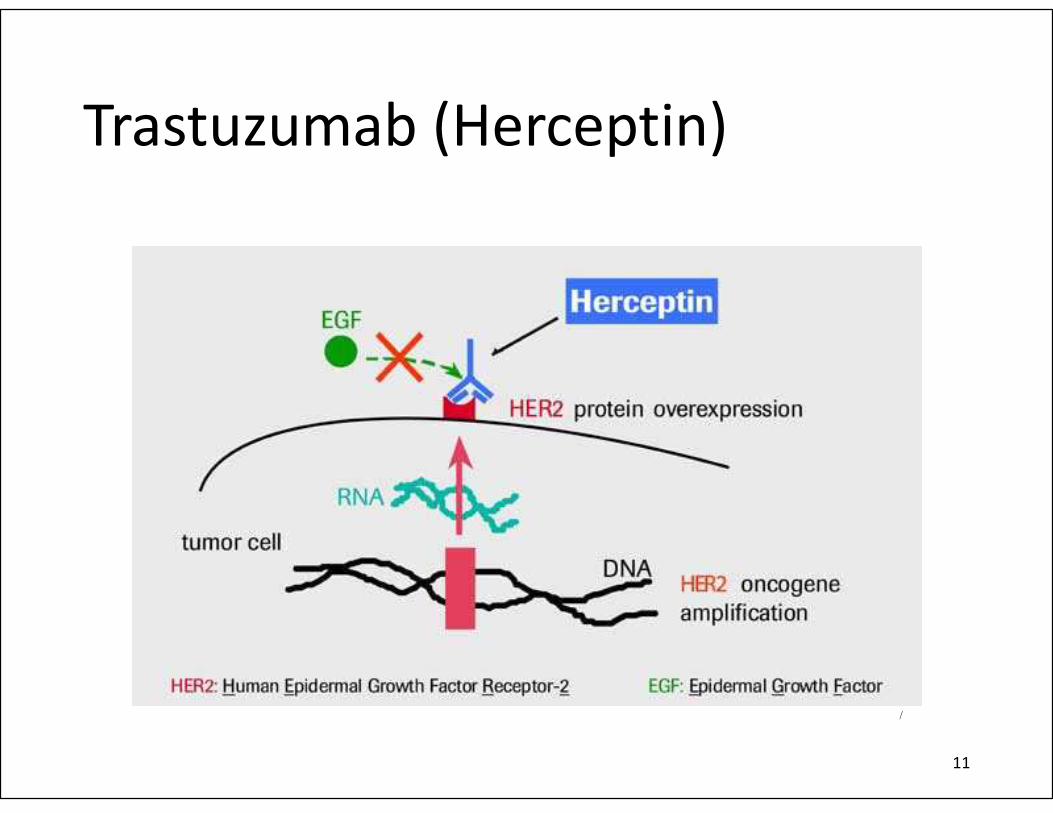
Trastuzumab (Herceptin)
11
http://trialx.com/
Bang et al, Lancet, 2010
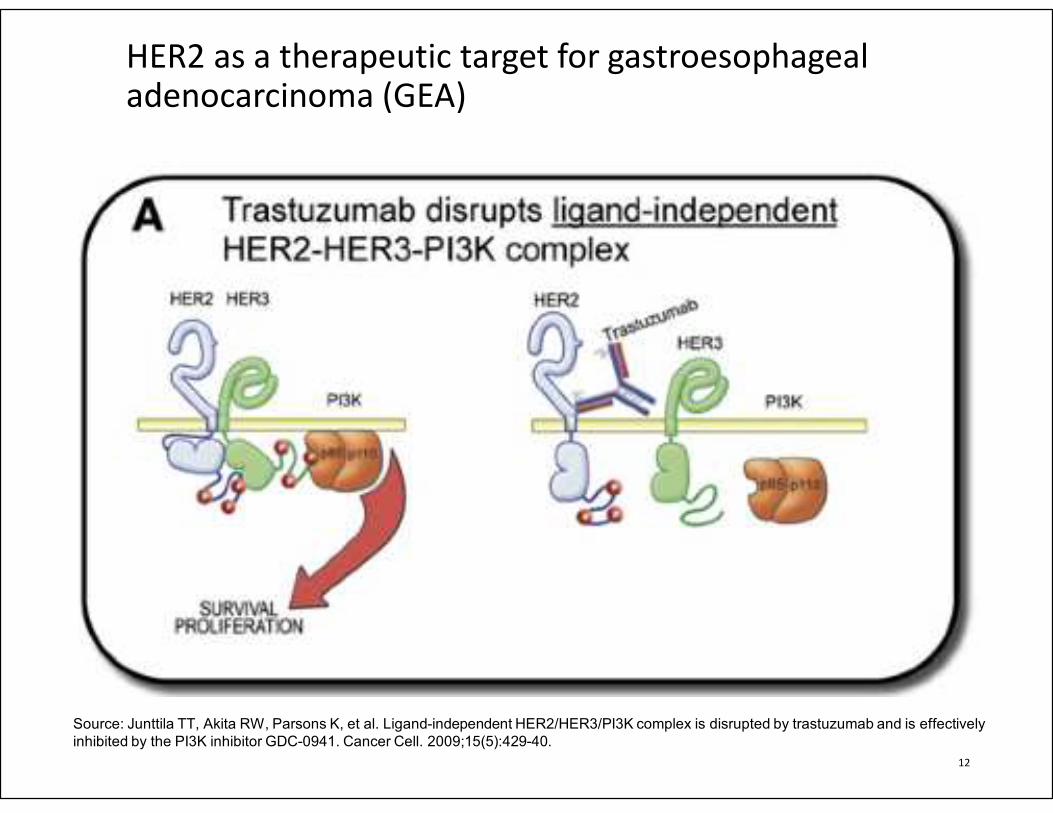
HER2 as a therapeutic target for gastroesophageal adenocarcinoma (GEA)
12
Source: Junttila TT, Akita RW, Parsons K, et al. Ligand-independent HER2/HER3/PI3K complex is disrupted by trastuzumab and is effectively
inhibited by the PI3K inhibitor GDC-0941. Cancer Cell. 2009;15(5):429-40.
Background
• 2007- expert panel with members from American Society of Clinical Oncology (ASCO) and the College of American Pathology (CAP)
oGuidelines for when and how to test for the HER2 gene in breast cancer
oRecommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: the American Society of Clinical Oncology/College of American Pathologists Clinical Practice Update
14
Source: Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American
Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31(31):3997-4013.
Methodology and Guideline Process
• Partner Organizations:
• CAP
• ASCP
• ASCO
• Pathologists, oncologists, gastroenterologist, patient advocate
• Physician methodologist experienced in systematic review and guideline development
• Medical librarian
15
HER2 Testing in GEA Project Team
16
Co-Chairs
Angela N. Bartley, MD – CAP
M. Kay Washington, MD – ASCP
Jaffer Ajani, MD - ASCO
Expert Panel
Al Benson, III, MD
Alfredo Carrato, MD, PhD
Margaret Gulley, MD
Dhanpat Jain, MD
Sanjay Kakar, MD
Srinadh Komanduri, MD
Helen Mackay, MD
Catherine Streutker, MD
Laura Tang, MD, PhD
Megan Troxell, MD, PhD
Advisory Panel
Andrew Bellizzi, MD
Katherine Geiersbach, MD
Syma Iqbal, MD
Rahul Jawale, MD
Alyssa Krasinskas, MD
Shiwen Song, MD
William Sukov, MD
Hanlin Wang, MD, PhD
Christopher Willett, MD
Christa Whitney-Miller, MD
Staff
Christina Ventura, MT(ASCP)
Carol Colasacco, MLIS, SCT(ASCP)
Jennifer Clark, BS, SCT(ASCP)
Nofisat Ismaila, MD (ASCO)
Conflict of Interest Review
• Potential panel members completed disclosure process reporting any actual or potential conflict
• Potential conflicts were reviewed by co-chairs
• Members were required to disclose conflicts continuously throughout the timeline
• No industry funding was involved in any aspect of the guideline development
• Panel members were volunteers
17
Key Questions – Overarching Questions
• Clinical question 1: What is the optimal testing algorithm for the assessment of HER2 status in patients with gastroesophageal adenocarcinoma?
oKey questions 1-6
• Clinical question 2: What strategies can help ensure optimal performance, interpretation and reporting of established assays in patients with gastroesophageal adenocarcinoma?
oKey questions 7-16
18
Systematic Review
• Title Abstract Review – 969 abstracts
• Full Text Review – dual review of 280 full text articles
• Data Extraction – 116 articles
o 1 Systematic review
o 2 Meta-analysis
o 2 Randomized control trials
o 27 Prospective studies
o 69 Prospective-retrospective studies
o 15 Retrospective studies
19
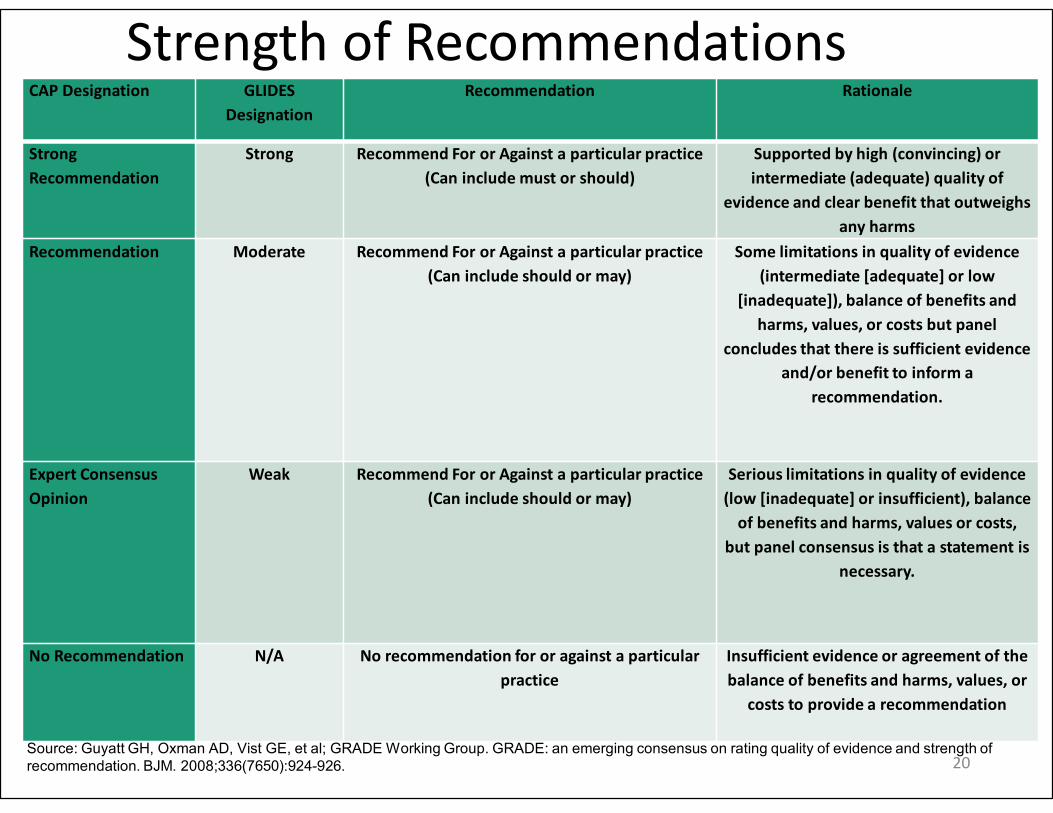
Strength of RecommendationsCAP Designation GLIDES
Designation
Recommendation Rationale
Strong
Recommendation
Strong Recommend For or Against a particular practice
(Can include must or should)
Supported by high (convincing) or
intermediate (adequate) quality of
evidence and clear benefit that outweighs
any harms
Recommendation Moderate Recommend For or Against a particular practice
(Can include should or may)
Some limitations in quality of evidence
(intermediate [adequate] or low
[inadequate]), balance of benefits and
harms, values, or costs but panel
concludes that there is sufficient evidence
and/or benefit to inform a
recommendation.
Expert Consensus
Opinion
Weak Recommend For or Against a particular practice
(Can include should or may)
Serious limitations in quality of evidence
(low [inadequate] or insufficient), balance
of benefits and harms, values or costs,
but panel consensus is that a statement is
necessary.
No Recommendation N/A No recommendation for or against a particular
practice
Insufficient evidence or agreement of the
balance of benefits and harms, values, or
costs to provide a recommendation
20Source: Guyatt GH, Oxman AD, Vist GE, et al; GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of
recommendation. BJM. 2008;336(7650):924-926.
Open Comment Period
• Open December 2015 and closed January 11th 2016.
• 294 responses were posted, with high agreement from open comment participants.
• Based on the open comment period,
• One draft recommendation was modified
• Four draft recommendations were combined
21
Recommendation 1
• Strong Recommendation: In patients with GEA who are potential candidates for HER2 targeted therapy, the treating clinician should request HER2 testing on tumor tissue.
• (Quality of evidence: High; Strength of recommendation: Strong)
22
Recommendation 3
• Recommendation: Treating clinicians or pathologist should request HER2 testing on tumor tissue in the biopsy or resection specimens (primary or metastasis) preferably prior to the initiation of trastuzumab therapy if such specimens are available and adequate. HER2 testing on FNA specimens (cell blocks) is an acceptable alternative.
• (Quality of evidence: Moderate/Intermediate; Strength of recommendation: Strong)
23
24
25
In patients with advanced GEA
Request in all patients who seem to qualify for trastuzumab (and chemotherapy)
26
Should you ever repeat HER2 testing?
No (no data but some BC docs do)
Should you continue trastuzumab beyond progression?
No (no data but many BC docs do)
Should you wait for HER2 results to start therapy?
NO (Most patients are symptomatic and can add trastuzumab later if HER2 is positive)
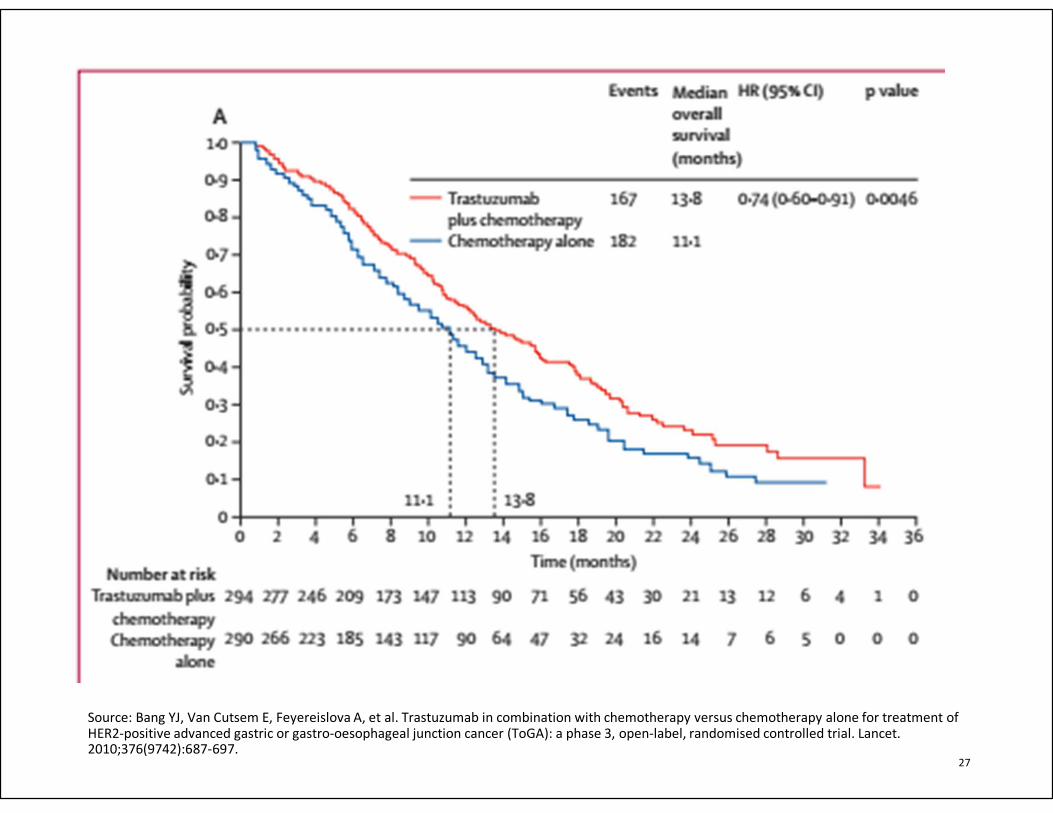
Source: Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687-697.
27
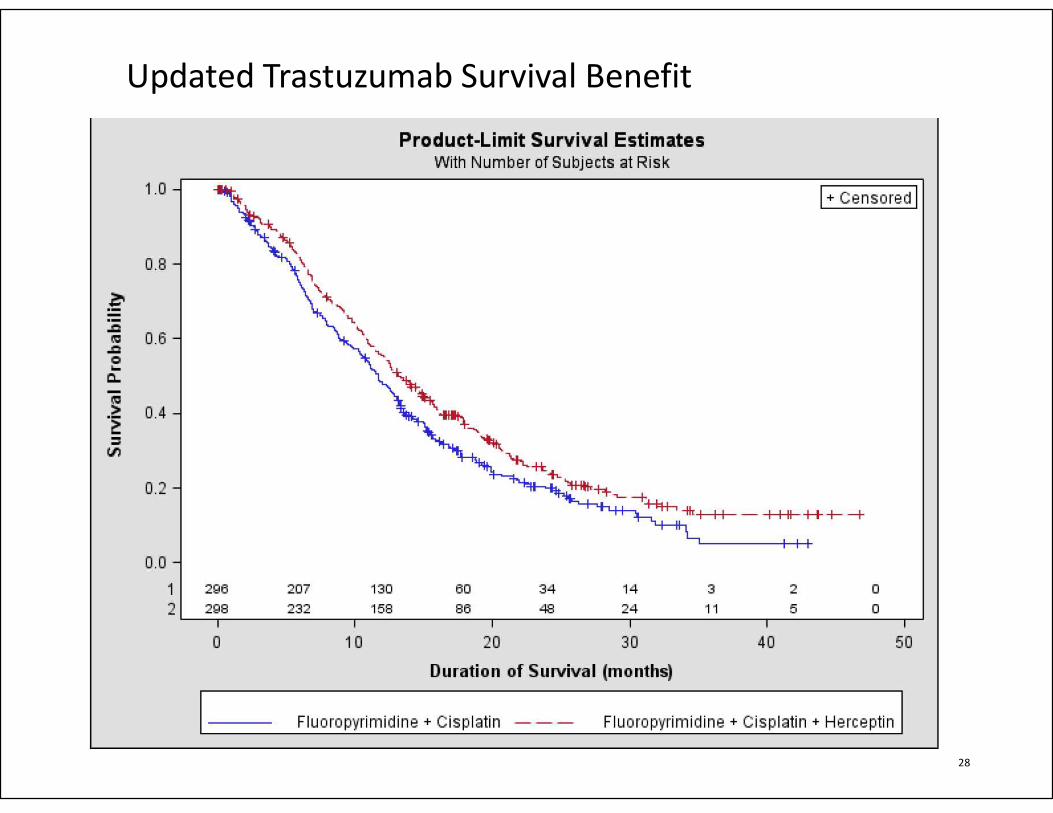
Updated Trastuzumab Survival Benefit
28
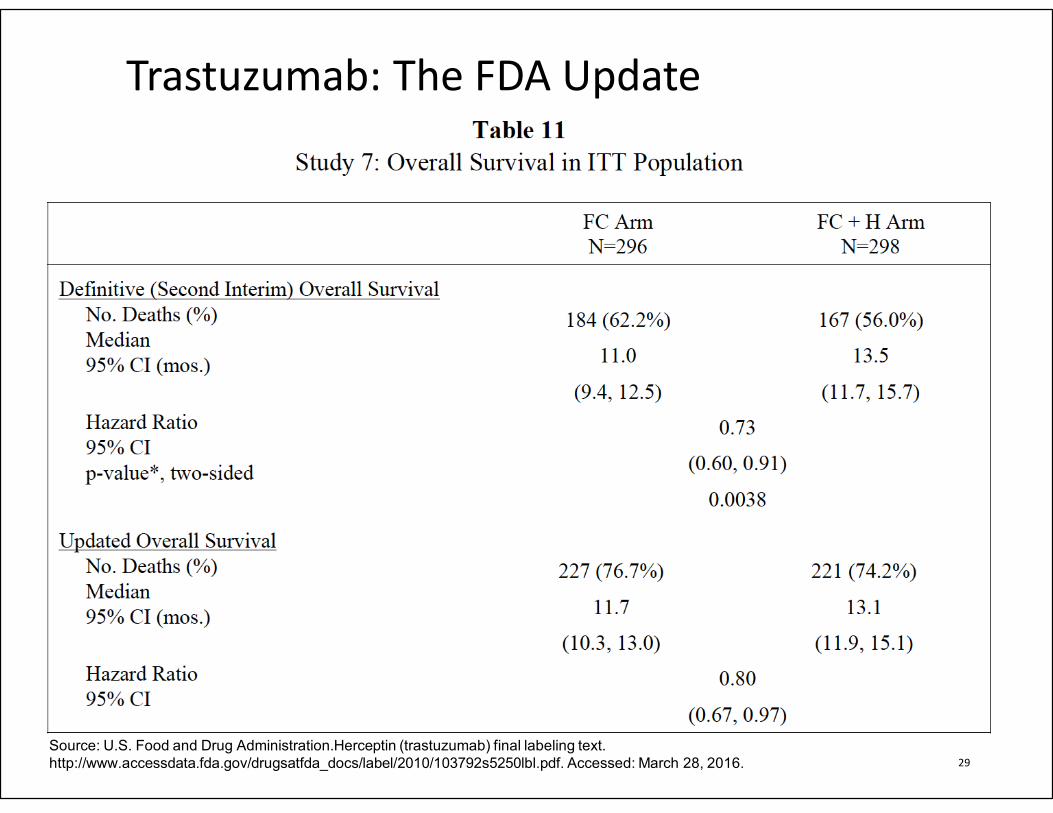
Trastuzumab: The FDA Update
29
Source: U.S. Food and Drug Administration.Herceptin (trastuzumab) final labeling text.
http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/103792s5250lbl.pdf. Accessed: March 28, 2016.
Other attempts to improve outcome of HER2 + tumor patients
30
• Both lapatinib trials (first line [Logic] and second line [Tytan]) were negative
• T-DM-1 trial was negative
• Pertuzumab trial (Jacob) results are pending. [dual blockade of HER2 and HER3 using trastuzumab and pertuzumab]
• Many interesting molecules are progressing in the clinic.
• e. g., margetuximab (Fc-modified chimeric monoclonal antibody in Phase 1)
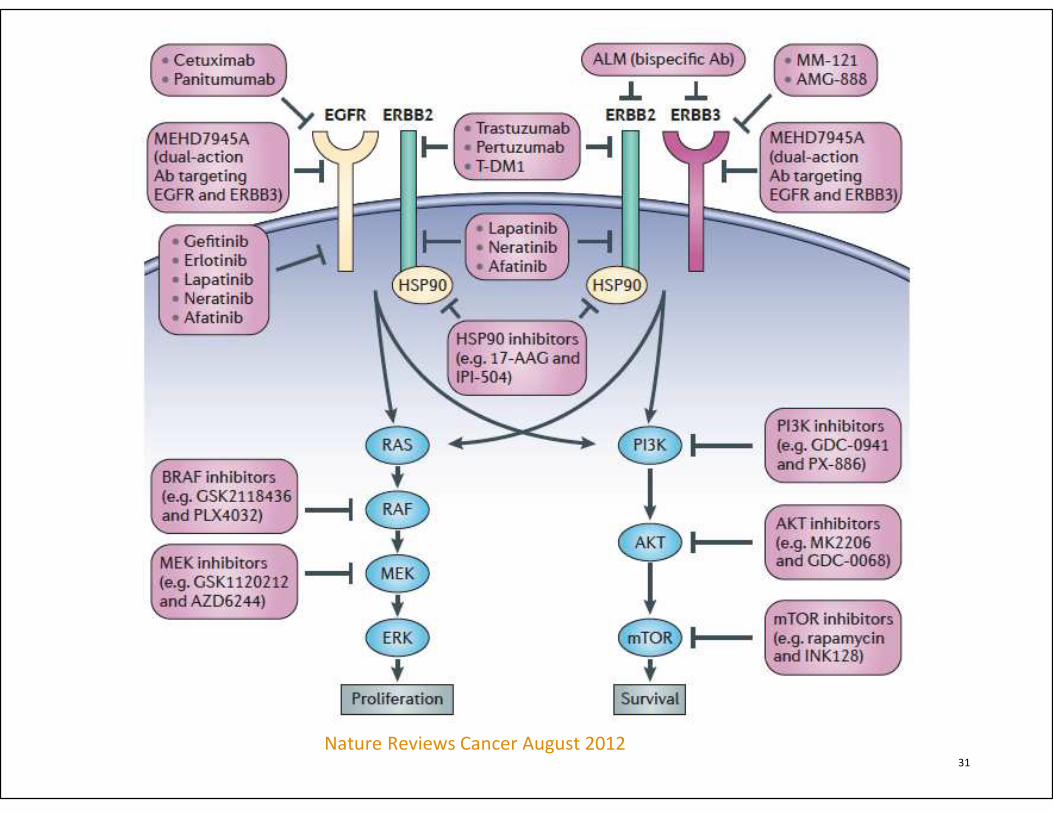
Nature Reviews Cancer August 2012 31
Nature Reviews Cancer August 2012
Conclusions
32
• No need to wait for HER2 status to start treatment with chemotherapy.
• Novel strategies (such adding a checkpoint inhibitor, bispecific antibodies, or adding immunogenic sequences to antibodies) may improve outcome even when HER2 is “negative”
Recommendation 2
• Recommendation: Treating clinicians or pathologist should request HER2 testing on tumor tissue in the biopsy or resection specimens (primary or metastasis) preferably prior to the initiation of trastuzumab therapy if such specimens are available and adequate. HER2 testing on FNA specimens (cell blocks) is an acceptable alternative.
• (Quality of evidence: Moderate/Intermediate; Strength of recommendation: Strong).
33
Tumor Specimens from the Primary GEA
• MAGIC trial: 93% concordance between biopsy and resection specimens
• ToGA trial: overall positive rate 23.2 % for biopsy and 19.7% for surgical specimens
34
Source: Okines AF, Thompson LC, Cunningham D, et al. Effect of
HER2 on prognosis and benefit from peri-operative chemotherapy
in early oesophago-gastric adenocarcinoma in the MAGIC trial.
Ann Oncol. 2013;24(5):1253-1261.
Tumor Specimens from the Primary GEA
• 381 advanced GEA patients:• No difference in HER2 positivity between
resections and biopsies (21% vs 19%) of primary of metastatic disease
• 207 advanced GEA patients:• 207 surgical resection specimens with paired
biopsies
• HER2 gene amplification in 31% of surgical resections and 32% of biopsy specimens
• Concordance between IHC and FISH: 90.9% and 90.2% in resections and biopsy specimens, respectively.
35
Source: Janjigian YY, Werner D, Pauligk C, et al. Prognosis of
metastatic gastric and gastroesophageal junction cancer by
HER2 status: a European and USA international collaborative
analysis. Ann Oncol. 2012;23(10):2656-2662.
Tumor Specimens from Resected GEA
• 61 consecutive pairs of biopsy and surgical specimens:
• Concordance of 92%
• Limited number of paired biopsy and resection specimens suggests a fair degree of concordance for HER2 expression/amplification.
36
Source: Pirrelli M, Caruso ML, Di Maggio M,
Armentano R, Valentini AM. Are biopsy specimens
predictive of HER2 status in gastric cancer
patients? Dig Dis Sci. 2013;58(2):397-404.
How many biopsy fragments are needed?
• A minimum of five, but optimally 6-8 biopsy fragments
• If there is concern of adequacy:
• Test additional specimen when available
• Communicate to clinician any question of adequacy
37
Source: Gullo I, Grillo F, Molinaro L, et al. Minimum biopsy set for HER2
evaluation in gastric and gastro-esophageal junction cancer. Endosc Int Open.
2015;3(2):E165-170.
38
Tumor Specimens from Metastatic GEA
• 100 primary gastric and metastatic lymph node specimens:
• Her2 overexpression in 33% of primary and 39% of metastatic lymph nodes
• 81 Primary versus metastatic lymph node specimens:
• 92.5% concordance of HER2 amplification by SISH
39
Source: Qiu Z, Sun W, Zhou C, Zhang J. HER2
expression variability between primary gastric
cancers and corresponding lymph node metastases.
Hepatogastroenterology. 2015;62(137):231-233.
Tumor Specimens from Metastatic GEA
• 68 paired GEA samples:
• 98.5% concordance of FISH and 95% concordance of IHC
• Only one case discordant; being negative in the primary and positive in the metastasis
• Given overall high degree of concordance, HER2 testing on neoplastic tissue from the primary or metastatic tumor is appropriate
40
Source: Bozzetti C, Negri FV, Lagrasta CA, et al.
Comparison of HER2 status in primary and
paired metastatic sites of gastric carcinoma. . Br
J Cancer. 2011;104(9):1372-1376.
Fine needle aspiration (FNA) or cytology specimen from primary or metastatic tumor
41
HER2 as a Prognostic Marker?
• Data are somewhat conflicting, but larger studies show no correlation with outcome
• Japanese cohort of 1006 patients • 836 HER2 negative, 112 HER2 positive
(defined as IHC 3+, FISH amplified) [948 undergoing curative resection]
• HER2 status correlated with older age, male gender, lower grade, and nodal status
• HR for recurrence was 1.109 (0.685-1.796), for cancer-related death 0.565 (0.262-1.219)
42
Source: Aizawa M, Nagatsuma AK, Kitada K, et al. Evaluation of
HER2-based biology in 1,006 cases of gastric cancer in a
Japanese population. Gastric Cancer. 2014;17(1):34-42.
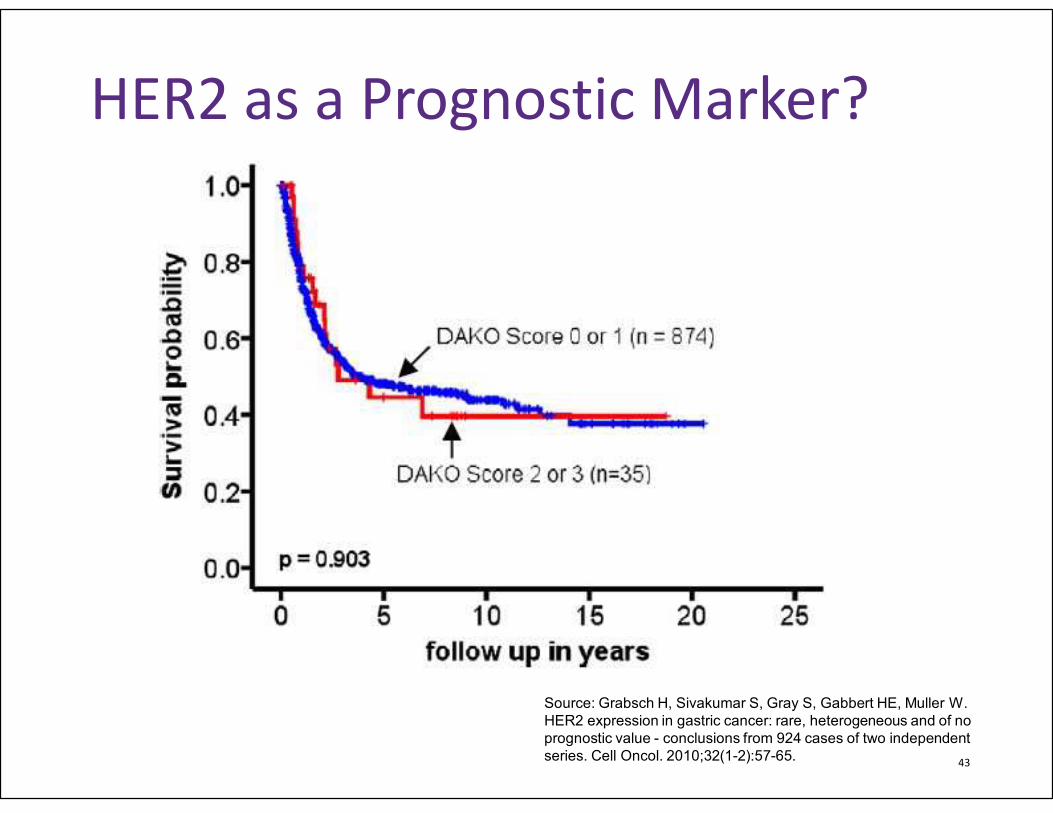
HER2 as a Prognostic Marker?
43
Source: Grabsch H, Sivakumar S, Gray S, Gabbert HE, Muller W.
HER2 expression in gastric cancer: rare, heterogeneous and of no
prognostic value - conclusions from 924 cases of two independent
series. Cell Oncol. 2010;32(1-2):57-65.
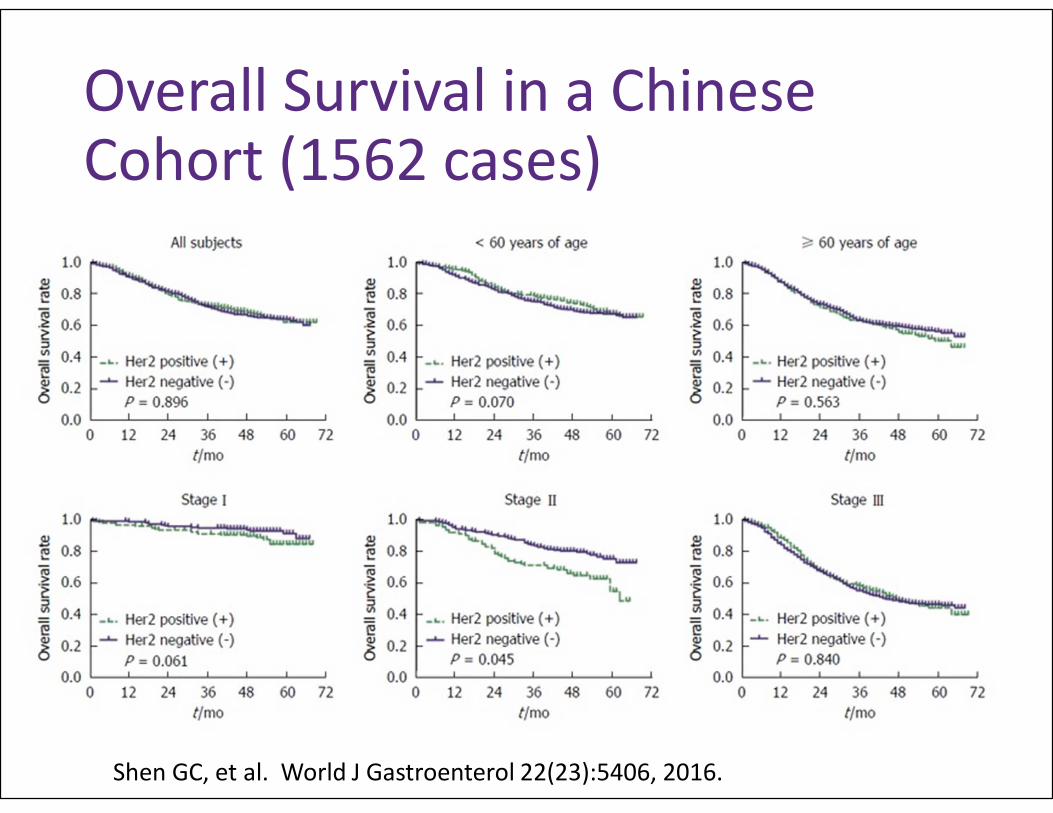
Overall Survival in a Chinese Cohort (1562 cases)
Shen GC, et al. World J Gastroenterol 22(23):5406, 2016.
Recommendation 5
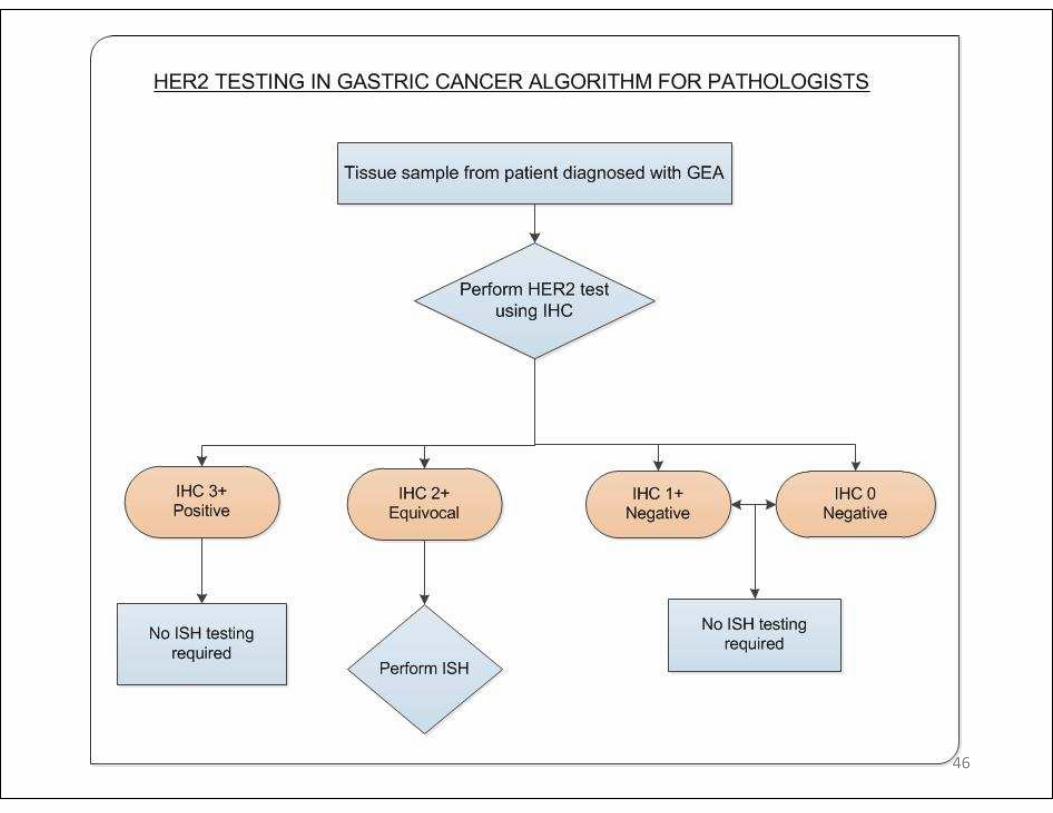
• Strong Recommendation: When GEA HER2 status is being evaluated, laboratories/pathologists should perform/order IHC testing first followed by ISH when IHC result is 2+ (equivocal). Positive (3+) or negative (0 or 1+) HER2 IHC results do not require further ISH testing.
• (Quality of evidence: High; Strength of recommendation: Strong)
45
46
Basis for Recommendation of IHC
• Patients with amplification by ISH without overexpression by IHC did not benefit from trastuzumab in ToGA
• Benefit of therapy appears to correlate with protein overexpression
• No need to test 0 and 1+ IHC with ISH (amplification rate is low (14-24%))
• IHC 3+ and ISH positivity concordance is high (>90%)
47
IHC 2+ cases should be tested with ISH
• 30-50% of IHC 2+ cases will show amplification (considered eligible for treatment)
• If there is uncertainty over whether score is 1+ or 2+, consider ISH
48
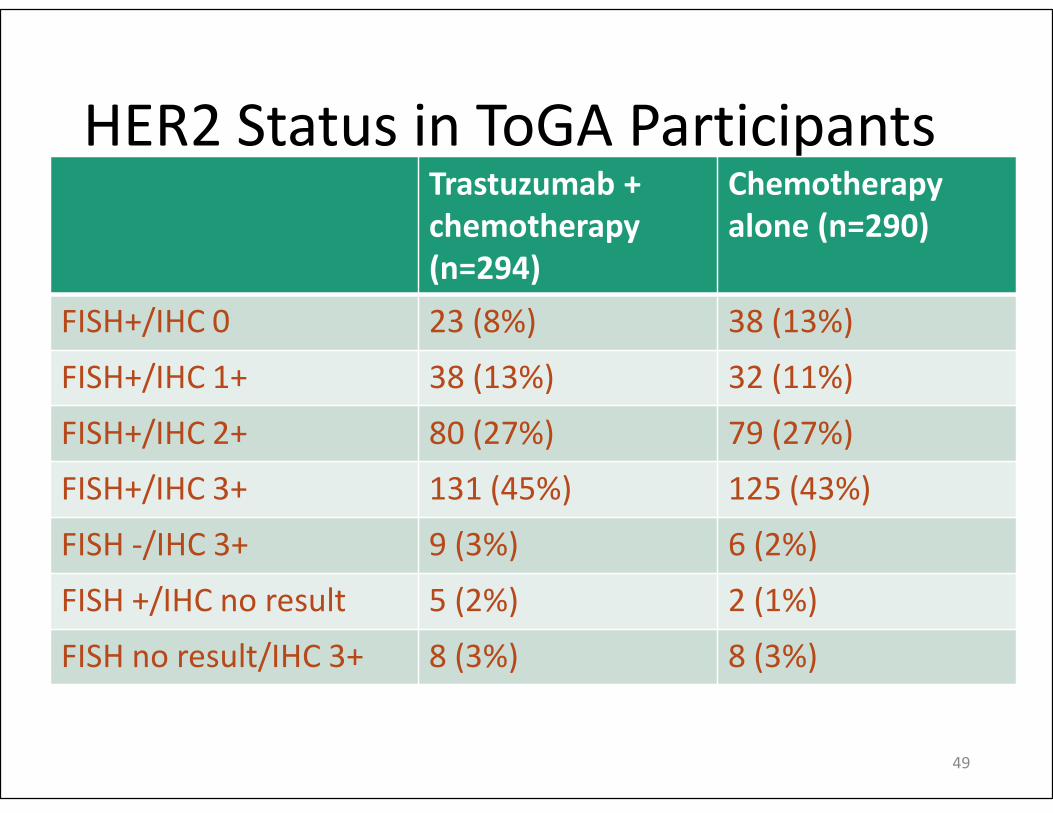
HER2 Status in ToGA ParticipantsTrastuzumab +
chemotherapy
(n=294)
Chemotherapy
alone (n=290)
FISH+/IHC 0 23 (8%) 38 (13%)
FISH+/IHC 1+ 38 (13%) 32 (11%)
FISH+/IHC 2+ 80 (27%) 79 (27%)
FISH+/IHC 3+ 131 (45%) 125 (43%)
FISH -/IHC 3+ 9 (3%) 6 (2%)
FISH +/IHC no result 5 (2%) 2 (1%)
FISH no result/IHC 3+ 8 (3%) 8 (3%)
49
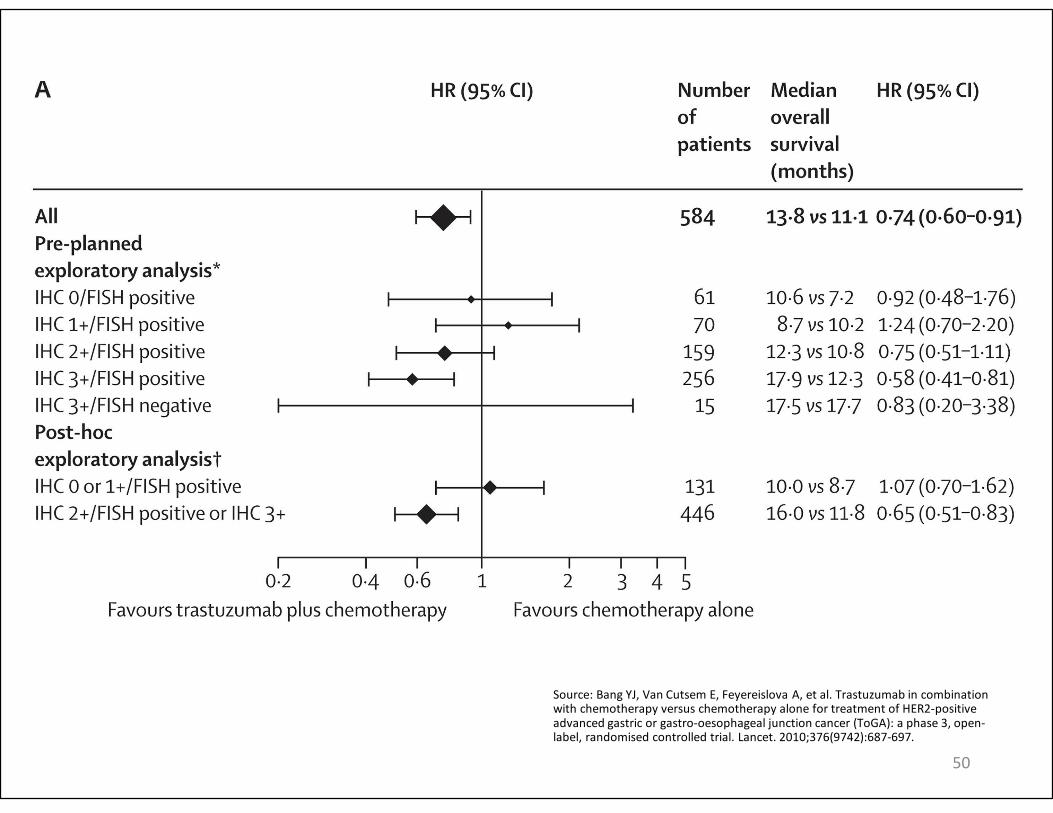
Source: Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687-697.
50
Recommendation 7
• Recommendation: Pathologists should select the tissue block with the areas of lowest grade tumor morphology in biopsy and resection specimens. More than one tissue block may be selected if different morphologic patterns are present.
• (Quality of evidence: Moderate/Intermediate; Strength of recommendation: Recommendation/Moderate)
51
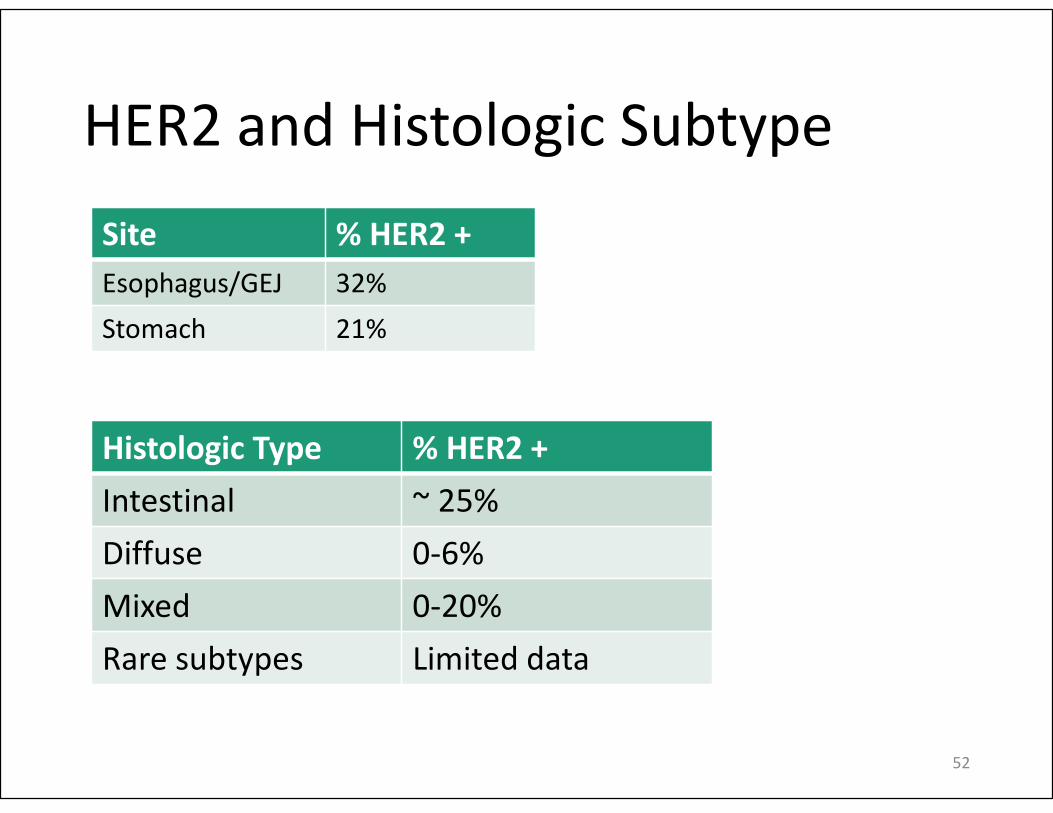
HER2 and Histologic Subtype
Site % HER2 +
Esophagus/GEJ 32%
Stomach 21%
52
Histologic Type % HER2 +
Intestinal ~ 25%
Diffuse 0-6%
Mixed 0-20%
Rare subtypes Limited data
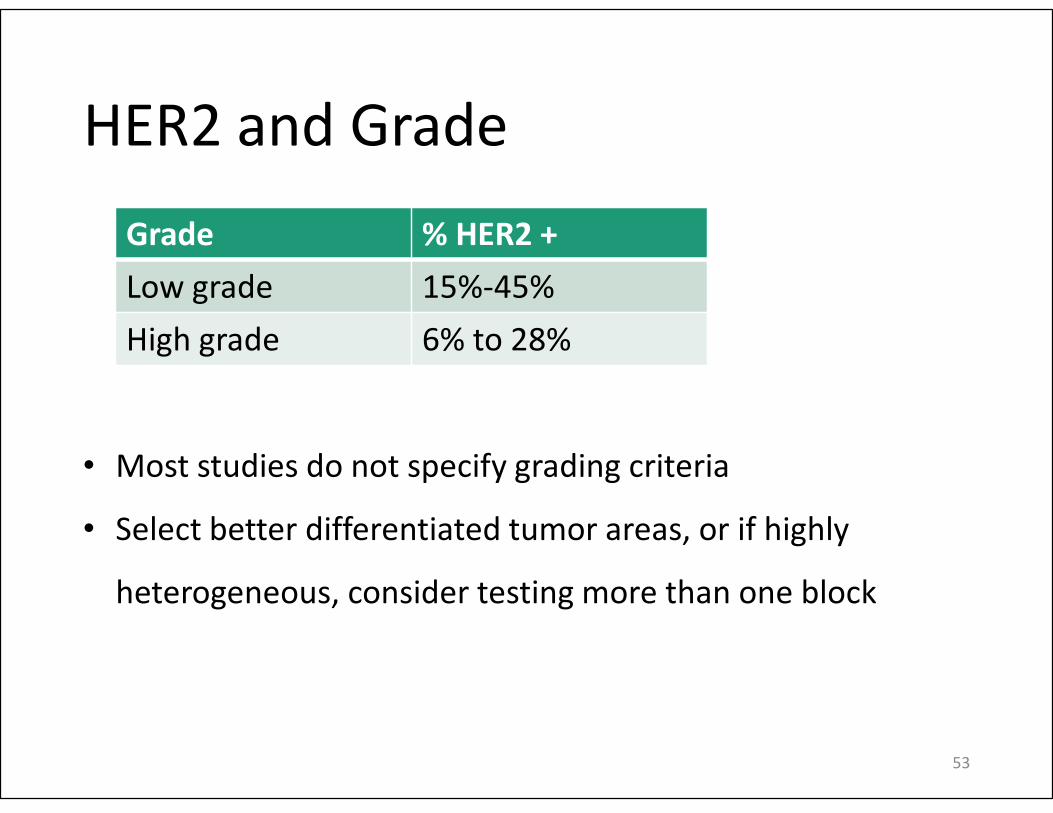
HER2 and Grade
Grade % HER2 +
Low grade 15%-45%
High grade 6% to 28%
53
• Most studies do not specify grading criteria
• Select better differentiated tumor areas, or if highly
heterogeneous, consider testing more than one block
Recommendation 4
• Strong recommendation: Laboratories/pathologists must specify the antibodies and probes used for the test and ensure that assays are appropriately validated for HER2 IHC and ISH on GEA specimens.
• (Quality of evidence: Moderate/Intermediate; Strength of recommendation: Strong)
54
Antibody Options
• Multiple antibodies available
• ToGA trial used HercepTest
• Many studies have used Ventana 4B5 or Thermo Fisher Scientific CB11
• Others are available
• Generally moderate to good concordance among antibodies
• No specific recommendation
55
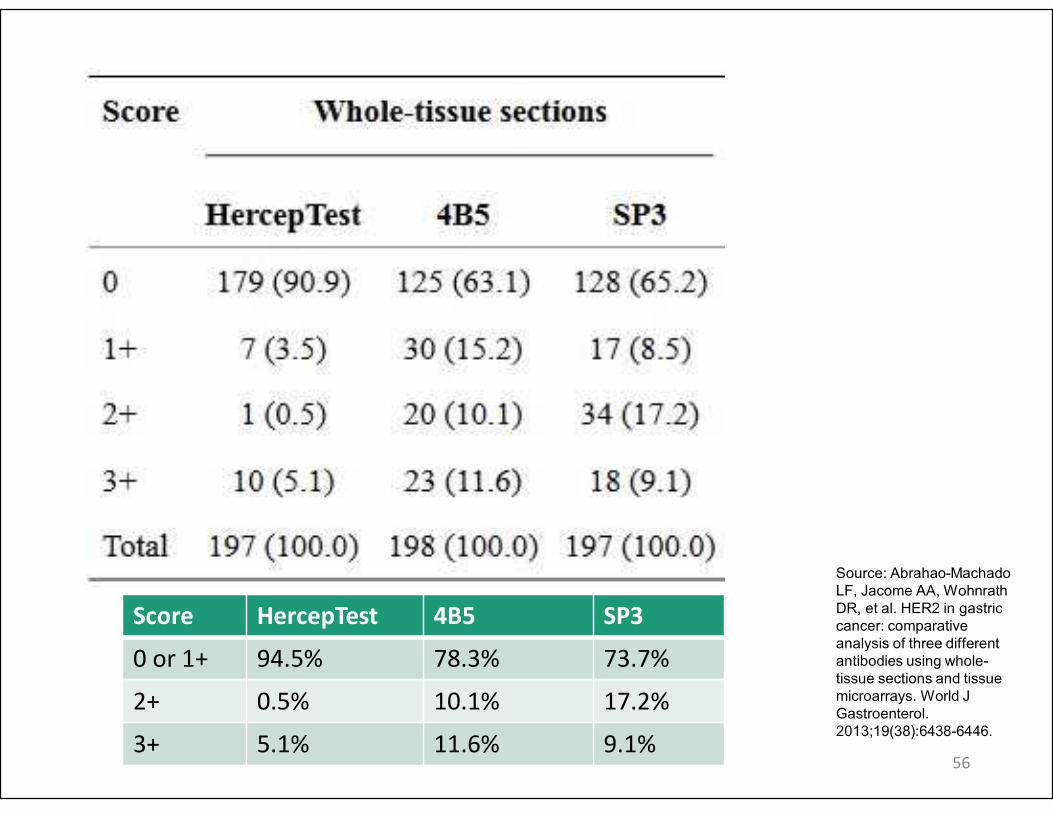
56
Source: Abrahao-Machado
LF, Jacome AA, Wohnrath
DR, et al. HER2 in gastric
cancer: comparative
analysis of three different
antibodies using whole-
tissue sections and tissue
microarrays. World J
Gastroenterol.
2013;19(38):6438-6446.
Score HercepTest 4B5 SP3
0 or 1+ 94.5% 78.3% 73.7%
2+ 0.5% 10.1% 17.2%
3+ 5.1% 11.6% 9.1%
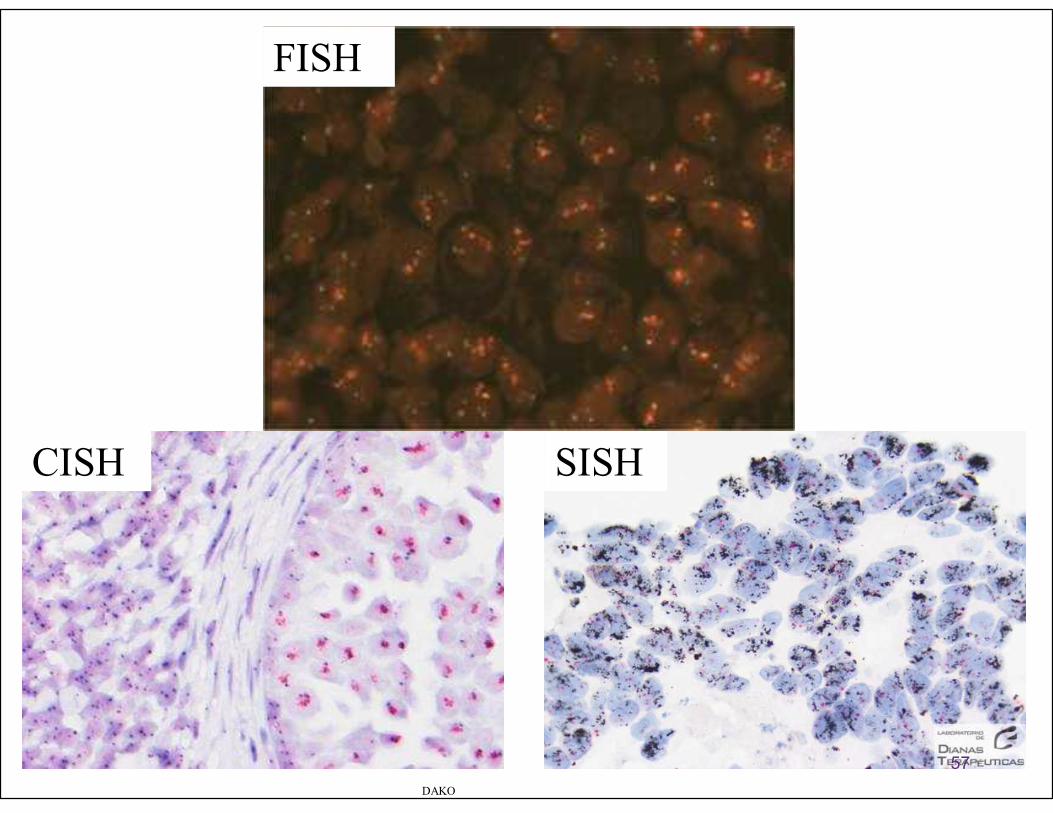
DAKO
CISH SISH
FISH
57
Validation of IHC and ISH
• Cases used for validation should predominantly be GEA cases
• CAP or CLSI guidelines for assay validation
• Method of sampling and fixative should be the same for validation and future use
• Use 20 positive and 20 negative specimens for FDA approved test and 40 of each for LDT
• Records of validation must be maintained per CAP
58
Recommendation 6
• Strong Recommendation: The pathologist should use the Ruschoff/Hofmann method in scoring HER2 IHC and ISH results for GEA.
• (Quality of evidence: Moderate/Intermediate; Strength of recommendation: Strong)
59
Source: Hofmann M, Stoss O, Shi D, et al.
Assessment of a HER2 scoring system for
gastric cancer: results from a validation
study. Histopathology. 2008;52(7):797-805.
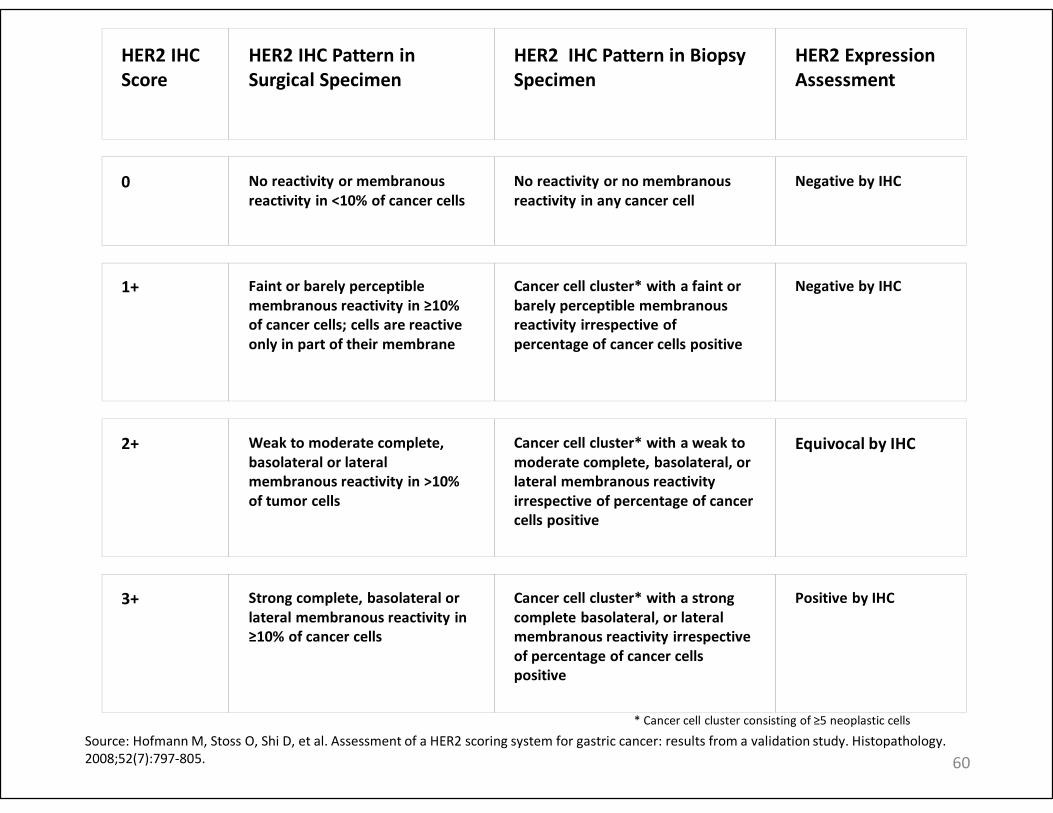
HER2 IHC
Score
HER2 IHC Pattern in
Surgical Specimen
HER2 IHC Pattern in Biopsy
Specimen
HER2 Expression
Assessment
0 No reactivity or membranous
reactivity in <10% of cancer cells
No reactivity or no membranous
reactivity in any cancer cell
Negative by IHC
1+ Faint or barely perceptible
membranous reactivity in ≥10%
of cancer cells; cells are reactive
only in part of their membrane
Cancer cell cluster* with a faint or
barely perceptible membranous
reactivity irrespective of
percentage of cancer cells positive
Negative by IHC
2+ Weak to moderate complete,
basolateral or lateral
membranous reactivity in >10%
of tumor cells
Cancer cell cluster* with a weak to
moderate complete, basolateral, or
lateral membranous reactivity
irrespective of percentage of cancer
cells positive
Equivocal by IHC
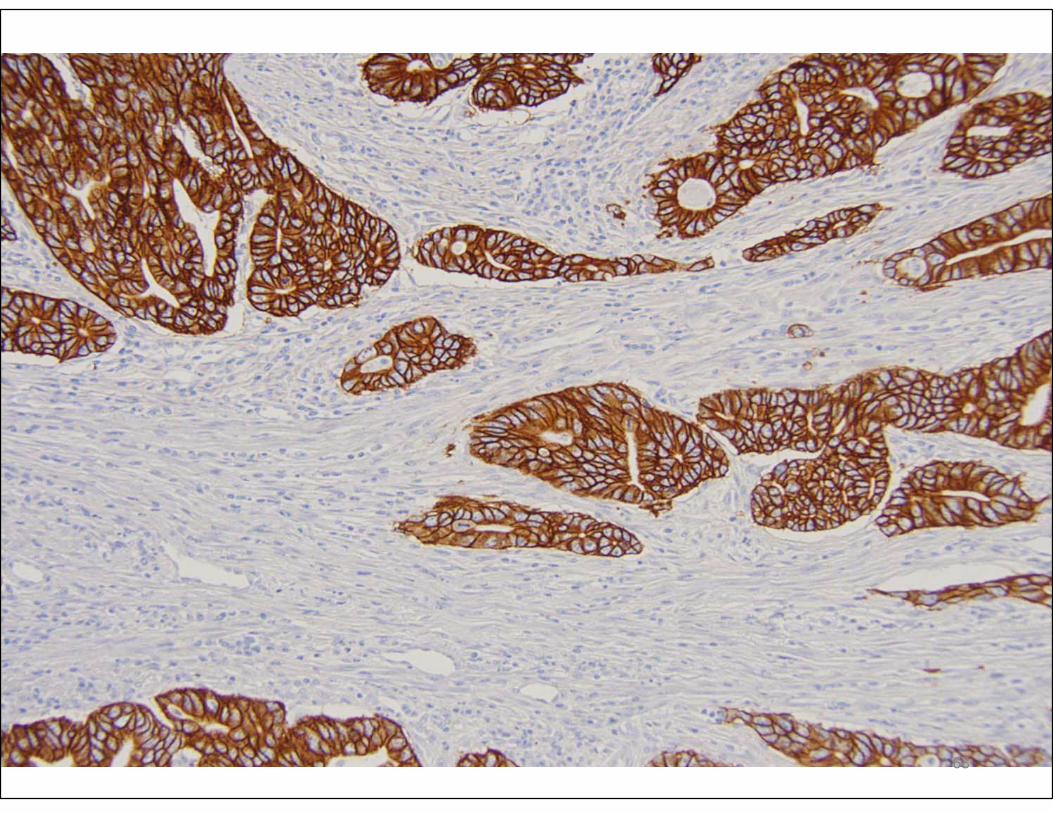
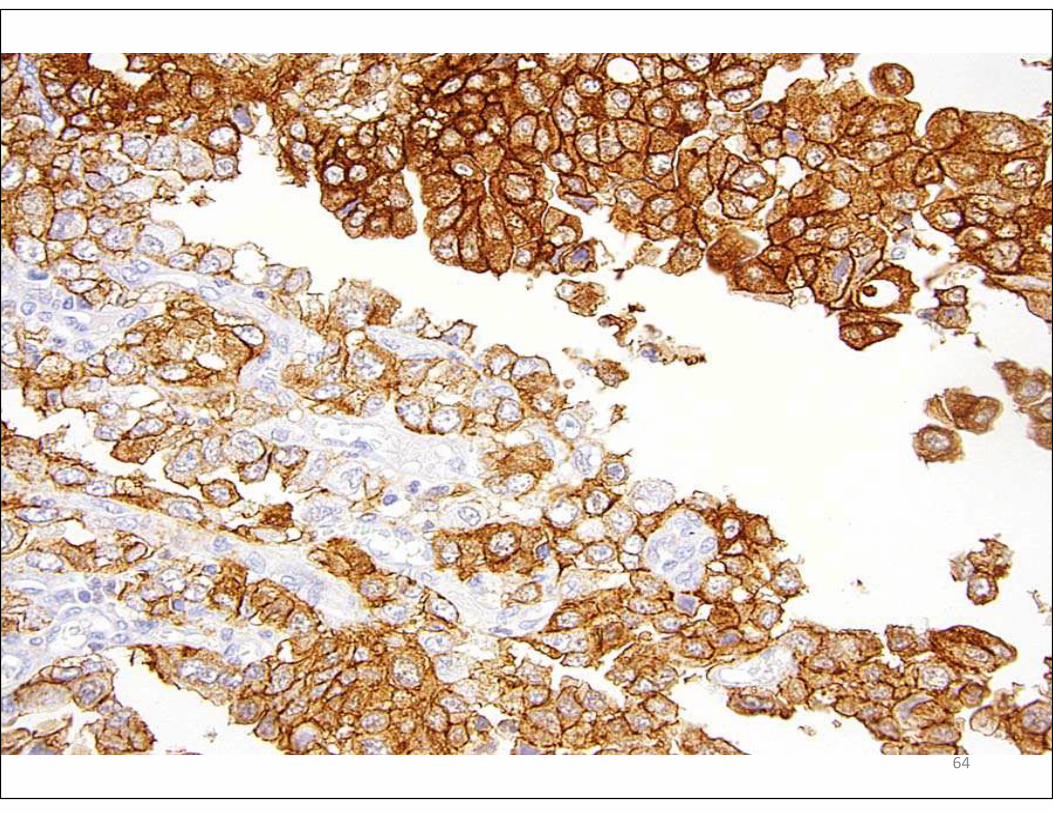
3+ Strong complete, basolateral or
lateral membranous reactivity in
≥10% of cancer cells
Cancer cell cluster* with a strong
complete basolateral, or lateral
membranous reactivity irrespective
of percentage of cancer cells
positive
Positive by IHC
* Cancer cell cluster consisting of ≥5 neoplastic cells
Source: Hofmann M, Stoss O, Shi D, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology.
2008;52(7):797-805. 60
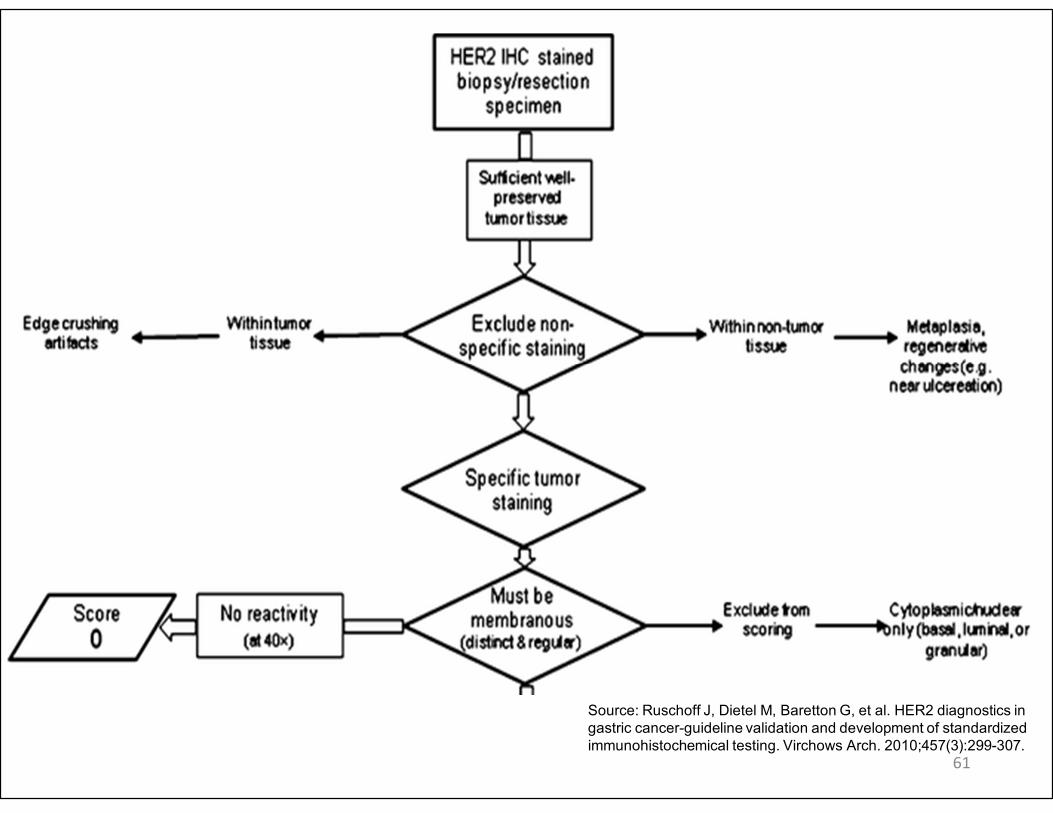
61
Source: Ruschoff J, Dietel M, Baretton G, et al. HER2 diagnostics in
gastric cancer-guideline validation and development of standardized
immunohistochemical testing. Virchows Arch. 2010;457(3):299-307.
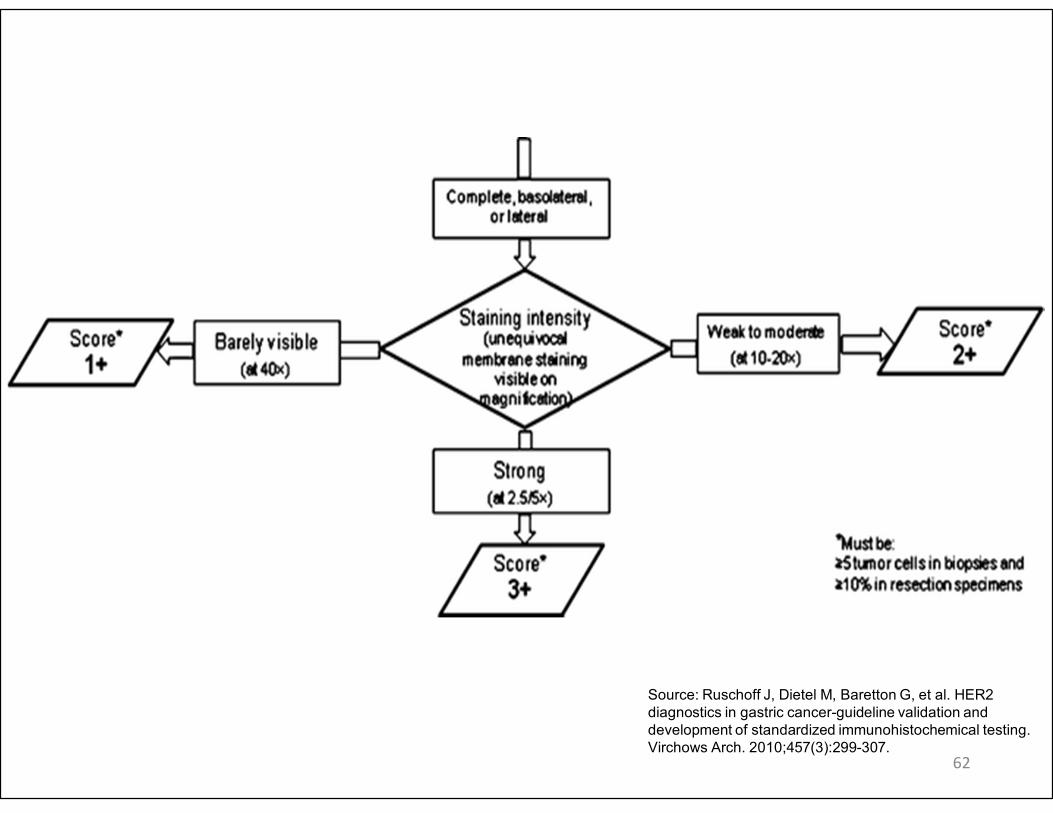
62
Source: Ruschoff J, Dietel M, Baretton G, et al. HER2
diagnostics in gastric cancer-guideline validation and
development of standardized immunohistochemical testing.
Virchows Arch. 2010;457(3):299-307.
63
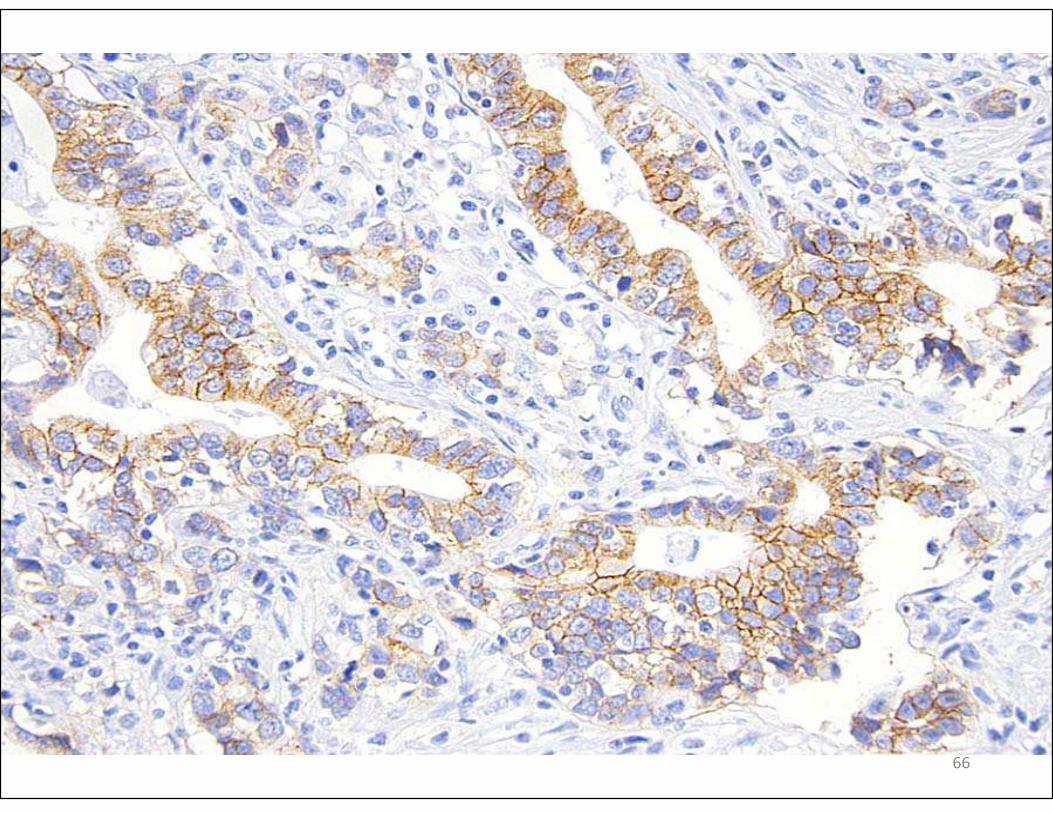
64
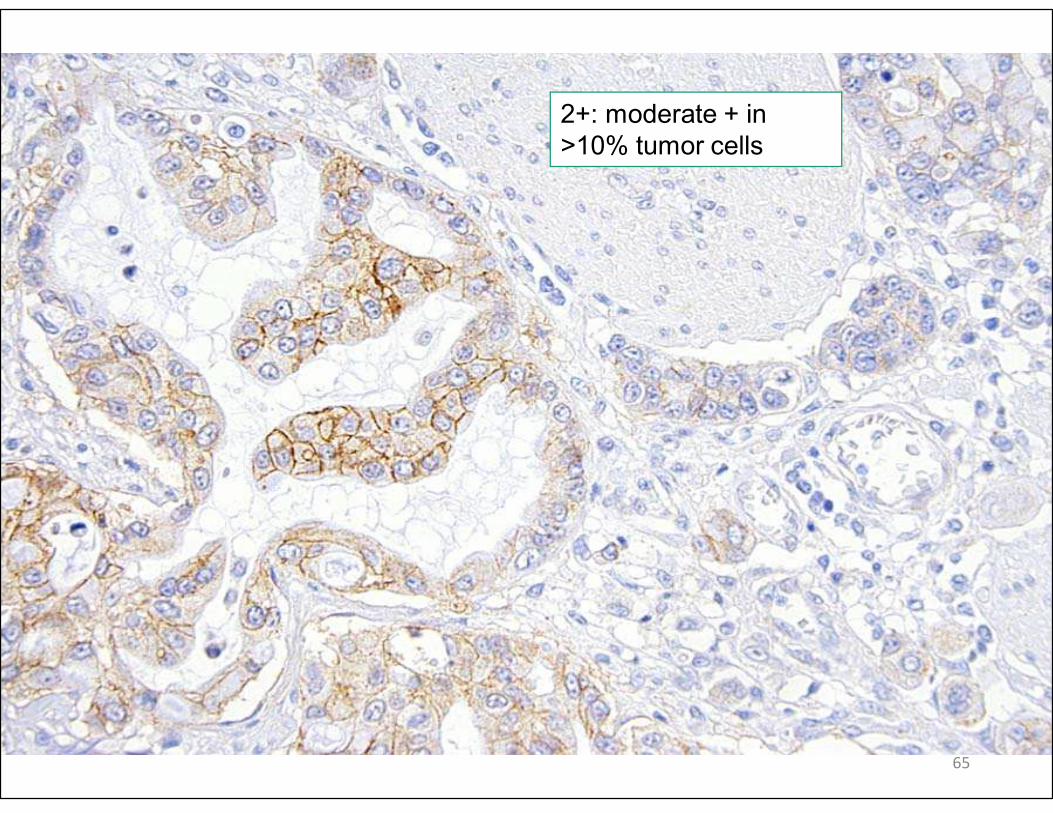
2+: moderate + in
>10% tumor cells
65
66
67
68
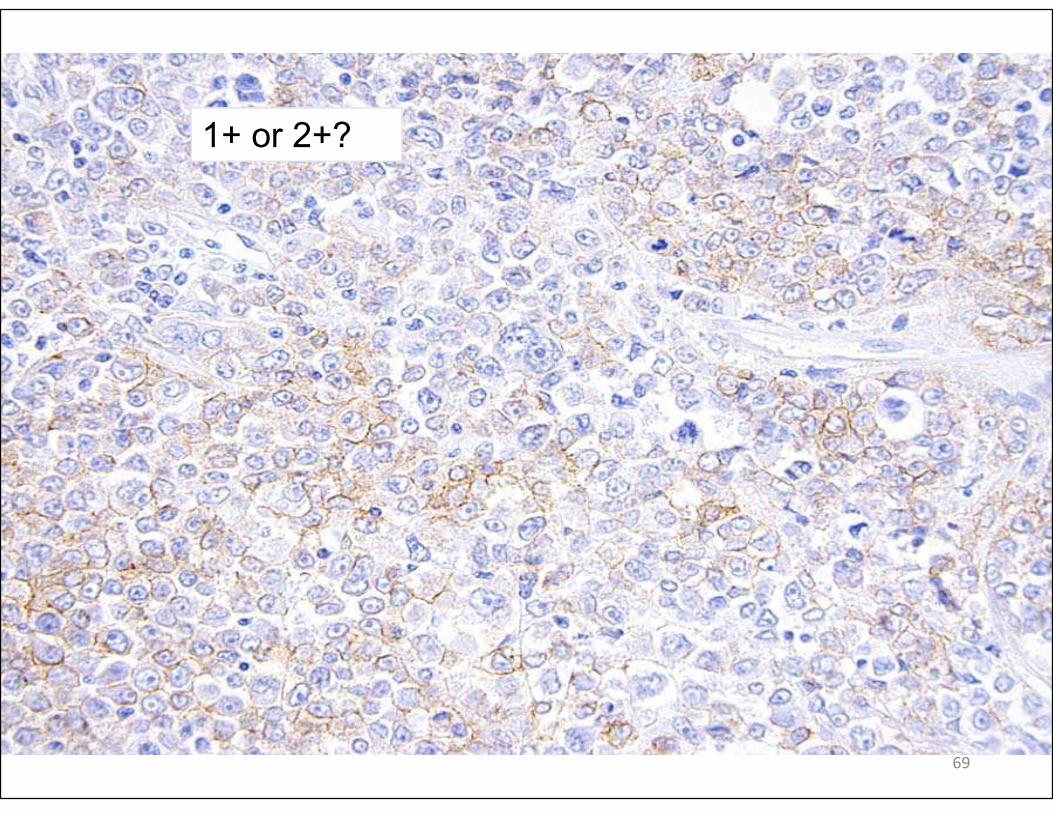
1+ or 2+?
69
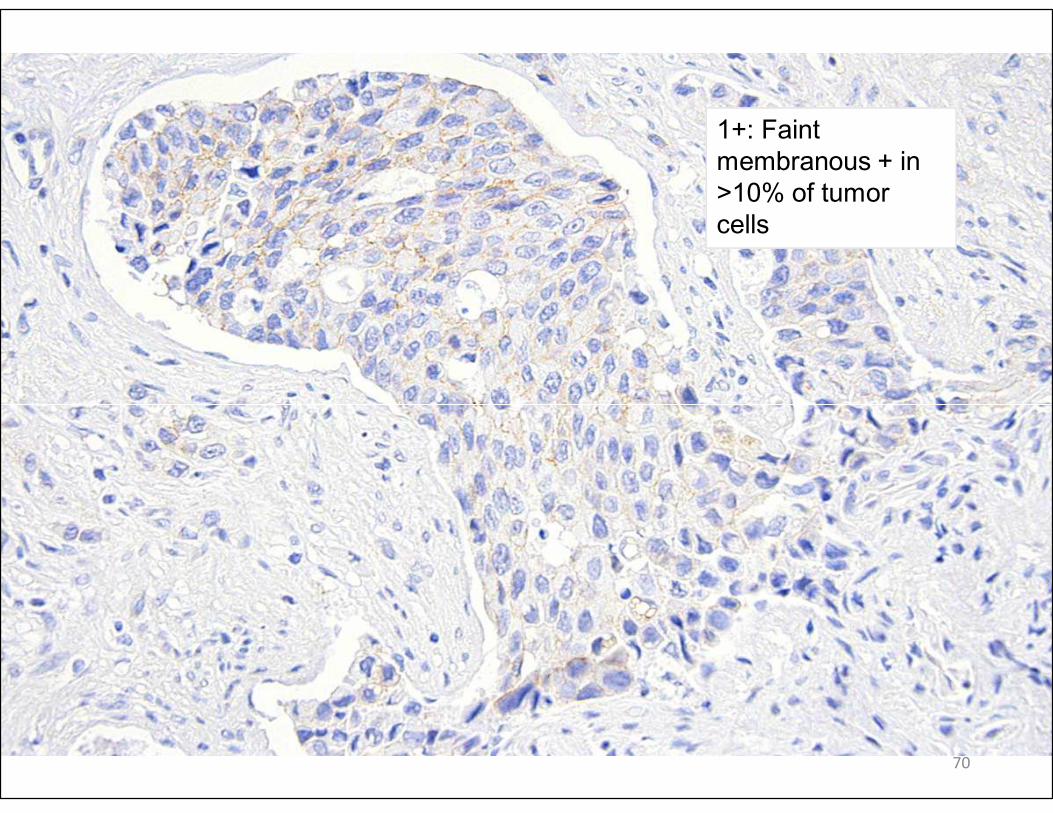
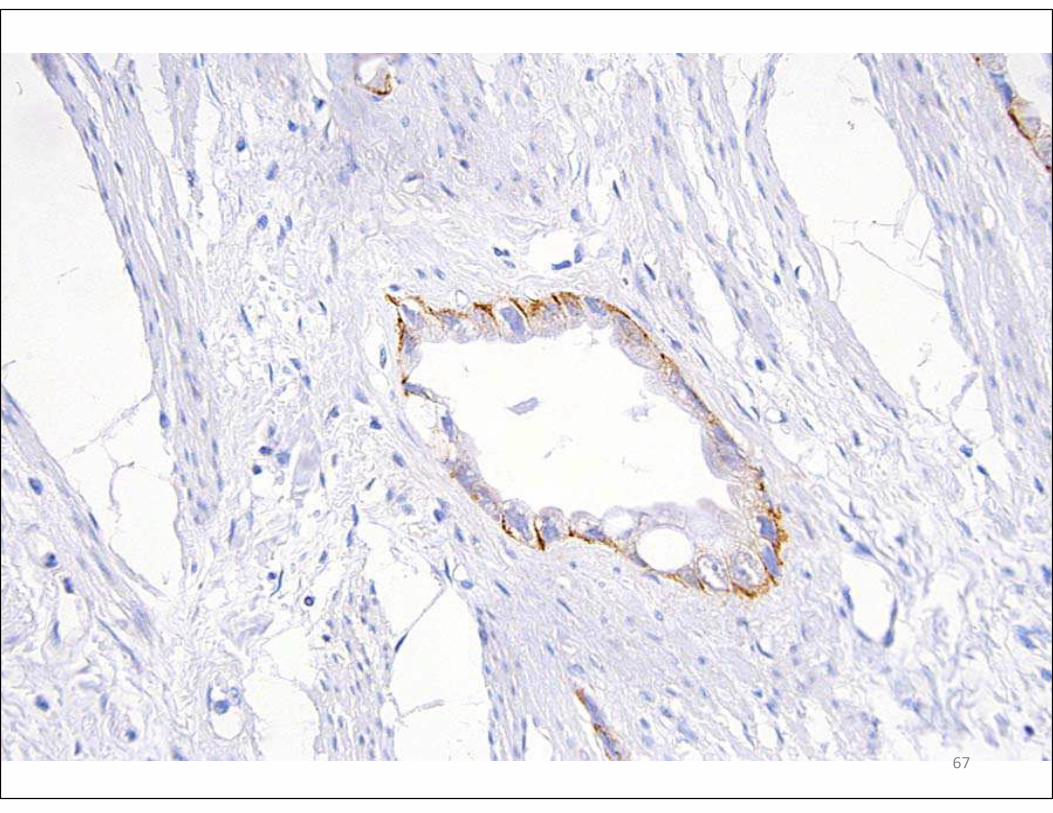
1+: Faint
membranous + in
>10% of tumor
cells
70
71
Pitfalls in IHC Assessment
• Gastric intestinal metaplasia and epithelium next to ulcers
• Edge effect
• Non-specific granular and pericellular staining
• Diffuse cytoplasmic and/or nuclear staining
• Non-specific staining in marginated cytoplasm in signet ring cells
72
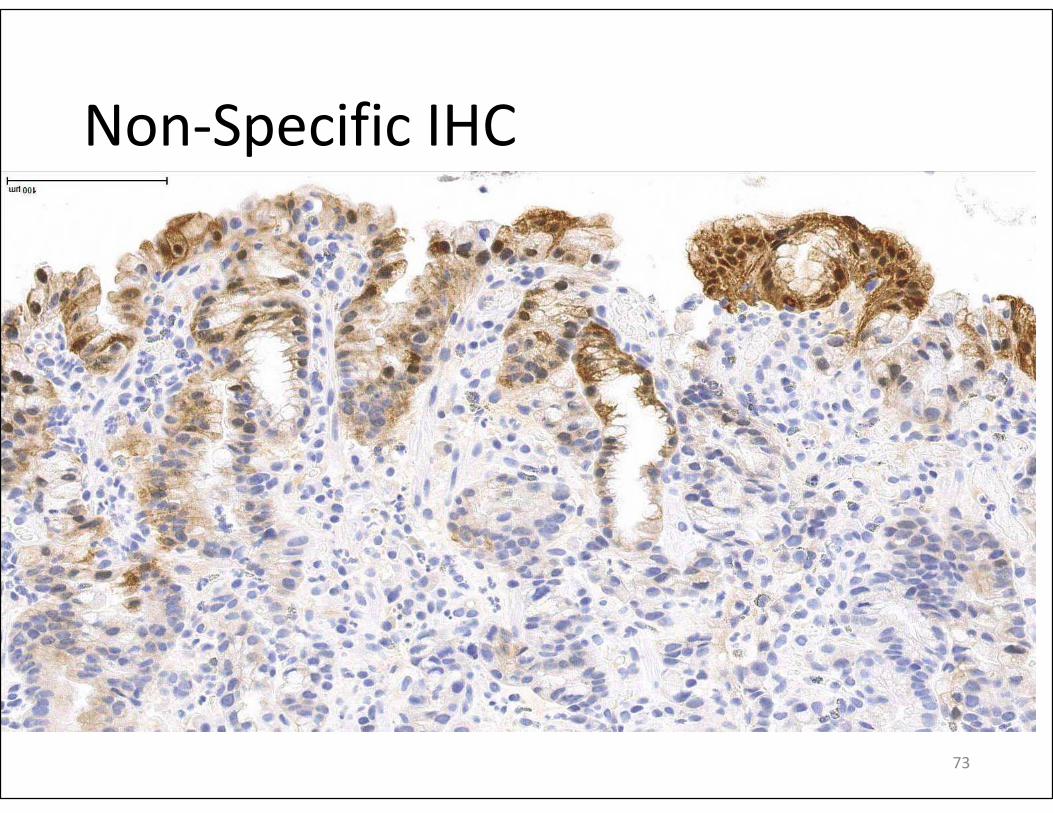
Non-Specific IHC
73
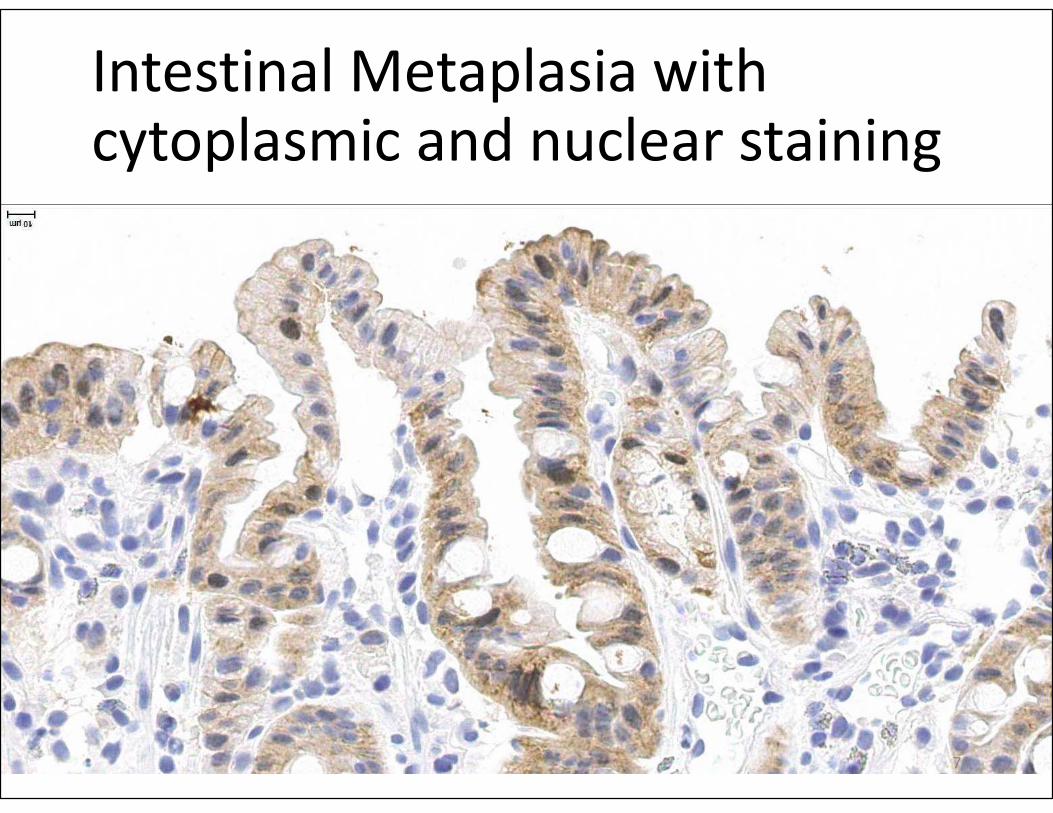
Intestinal Metaplasia with cytoplasmic and nuclear staining
74
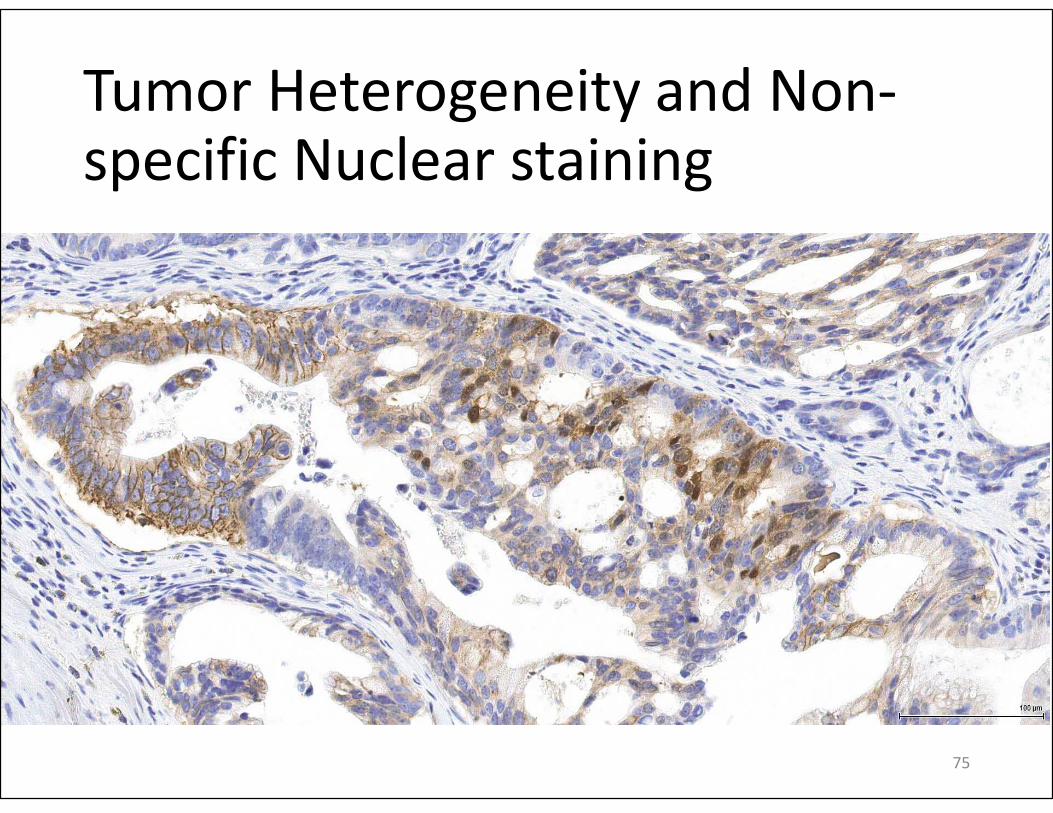
Tumor Heterogeneity and Non-specific Nuclear staining
75
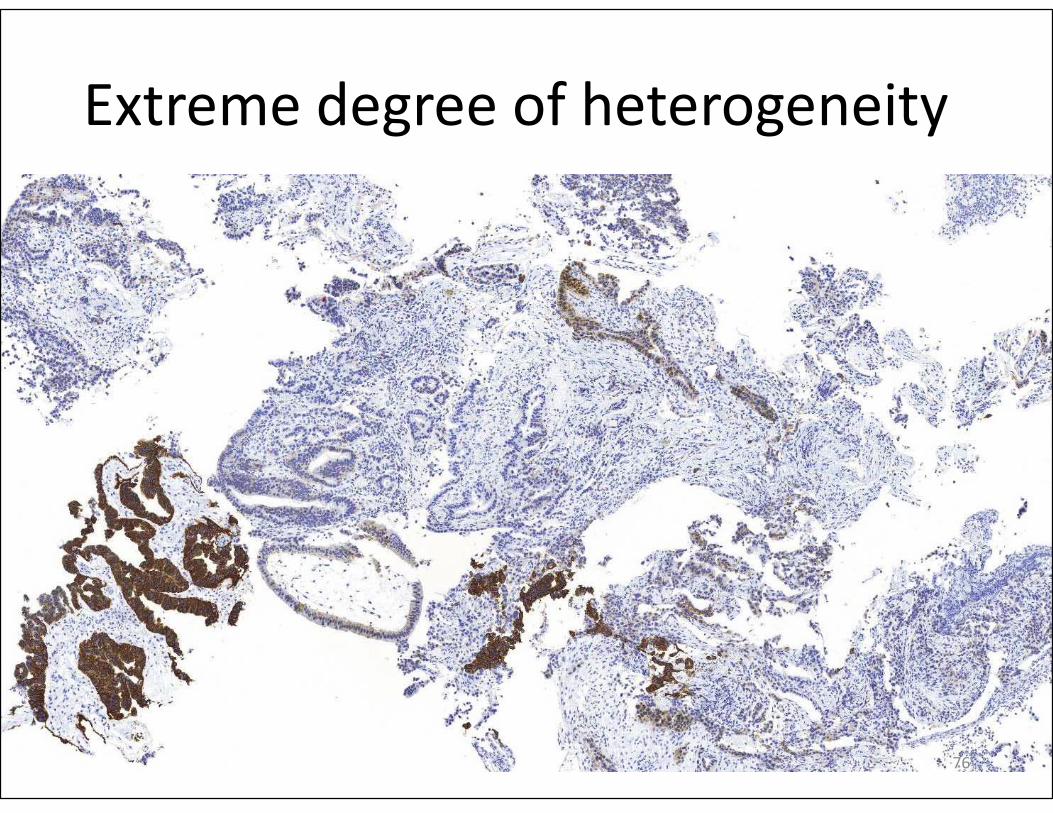
Extreme degree of heterogeneity
76
Tips to Increase Interobserver Agreement
• 3+: May be visible to naked eye; strong membrane + at low magnification using up to 5x objective
• 2+: Membrane expression first apparent using 10x objective
• 1+: Membrane expression at 40x objective
Membrane expression: distinct linear complete, basolateral, or lateral (not granular) expression at cell-cell contact sites
77
Source: Ruschoff J, Dietel M, Baretton G, et al. HER2 diagnostics in gastric
cancer-guideline validation and development of standardized
immunohistochemical testing. Virchows Arch. 2010;457(3):299-307.
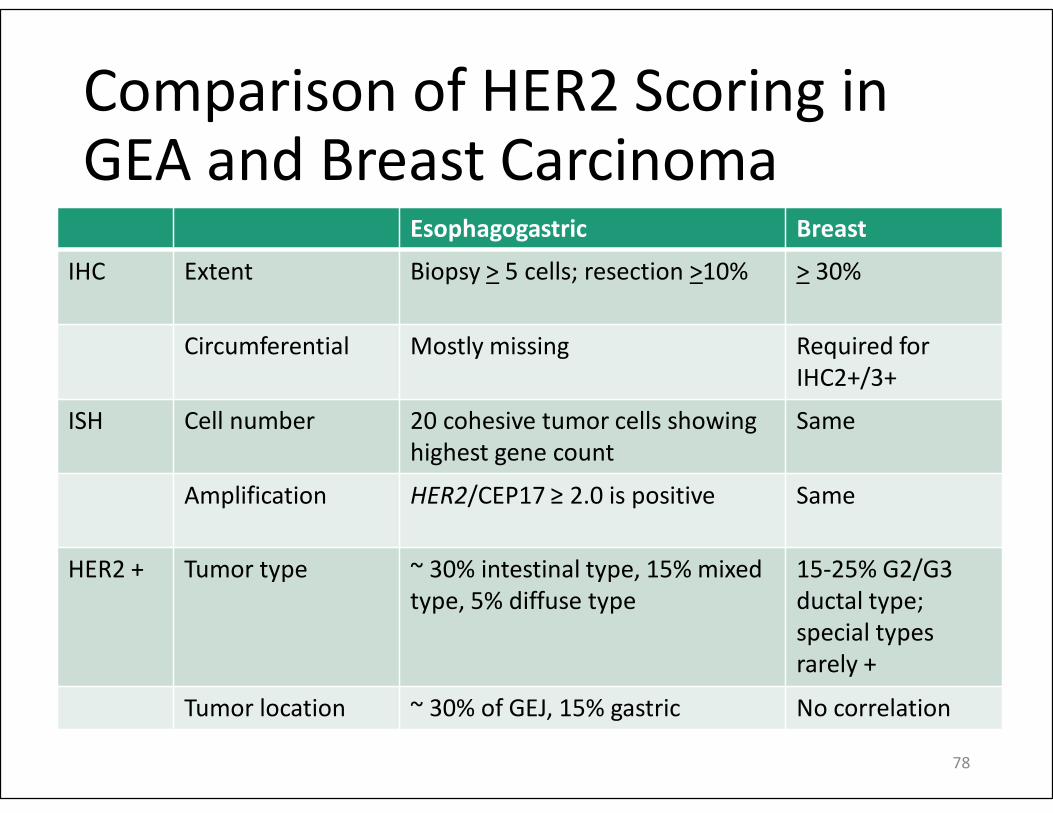
Comparison of HER2 Scoring in GEA and Breast Carcinoma
Esophagogastric Breast
IHC Extent Biopsy > 5 cells; resection >10% > 30%
Circumferential Mostly missing Required for
IHC2+/3+
ISH Cell number 20 cohesive tumor cells showing
highest gene count
Same
Amplification HER2/CEP17 ≥ 2.0 is positive Same
HER2 + Tumor type ~ 30% intestinal type, 15% mixed
type, 5% diffuse type
15-25% G2/G3
ductal type;
special types
rarely +
Tumor location ~ 30% of GEJ, 15% gastric No correlation
78
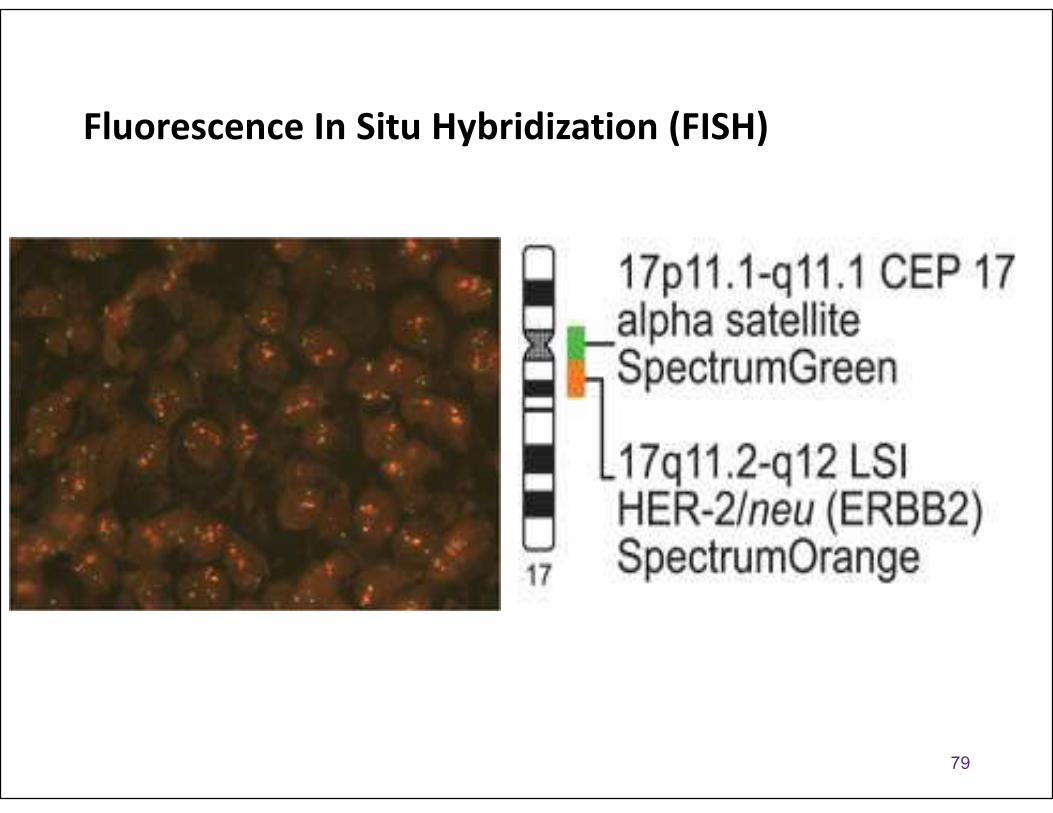
Fluorescence In Situ Hybridization (FISH)
79
www.abbot
tmolecular.
com
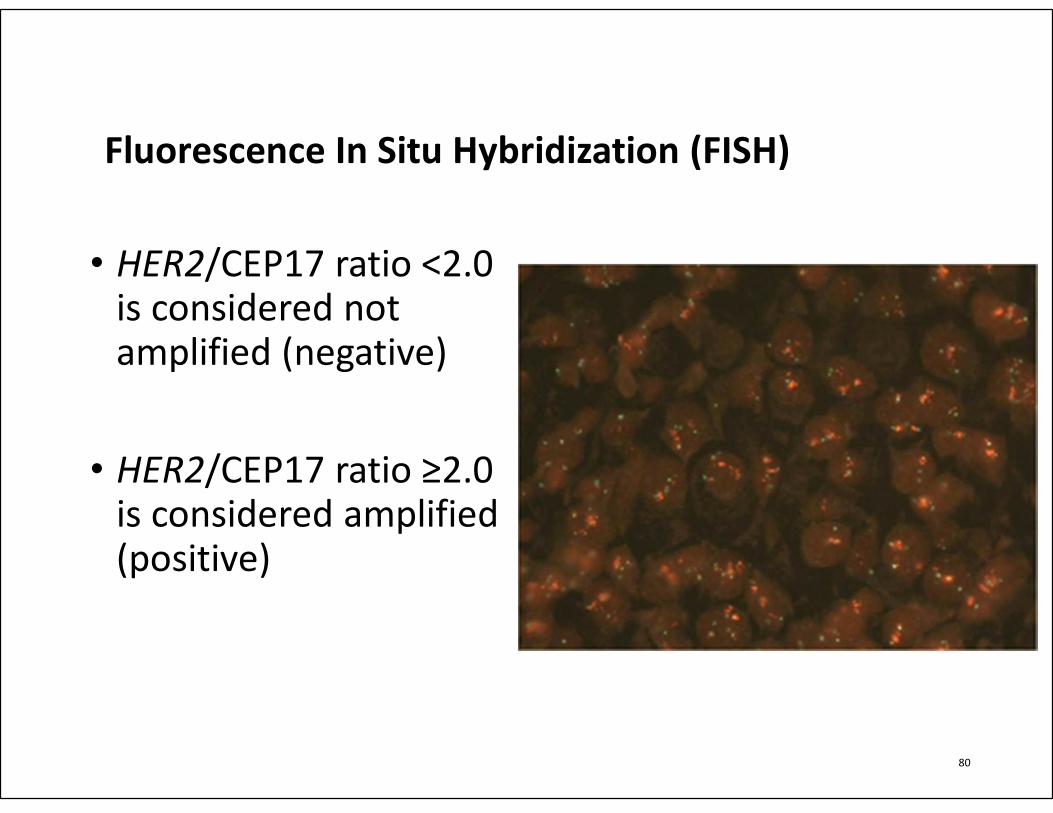
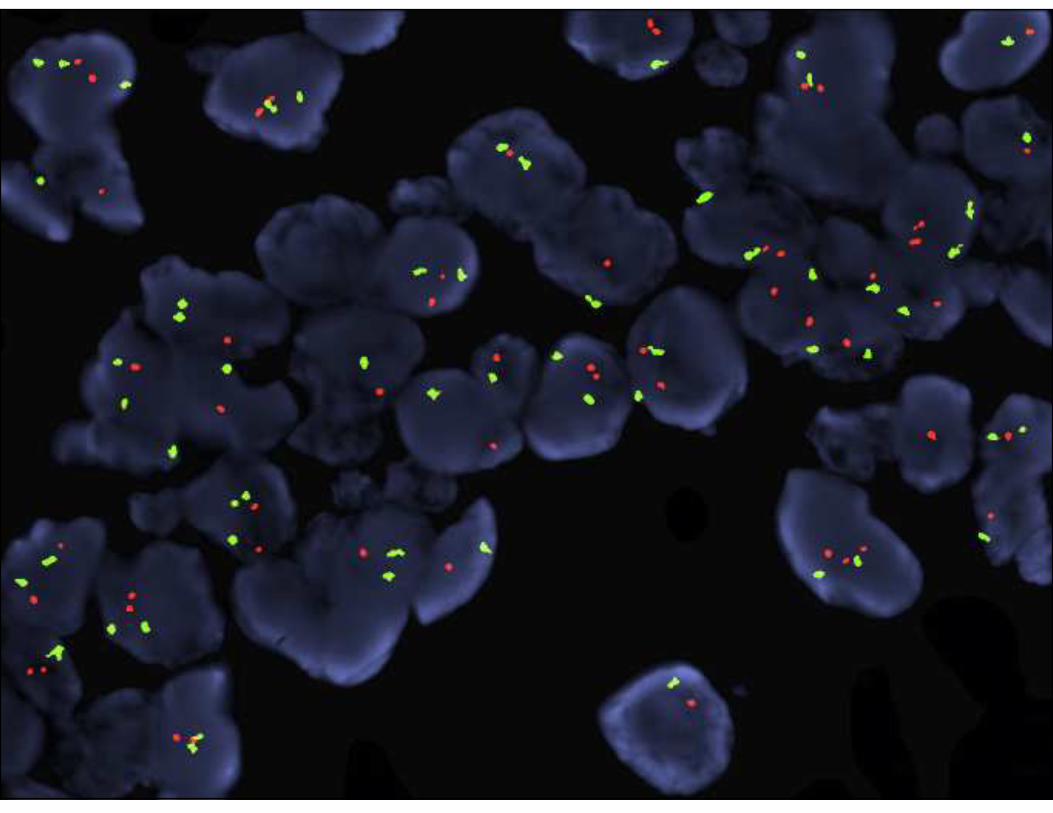
Fluorescence In Situ Hybridization (FISH)
• HER2/CEP17 ratio <2.0 is considered not amplified (negative)
• HER2/CEP17 ratio ≥2.0 is considered amplified (positive)
80
81
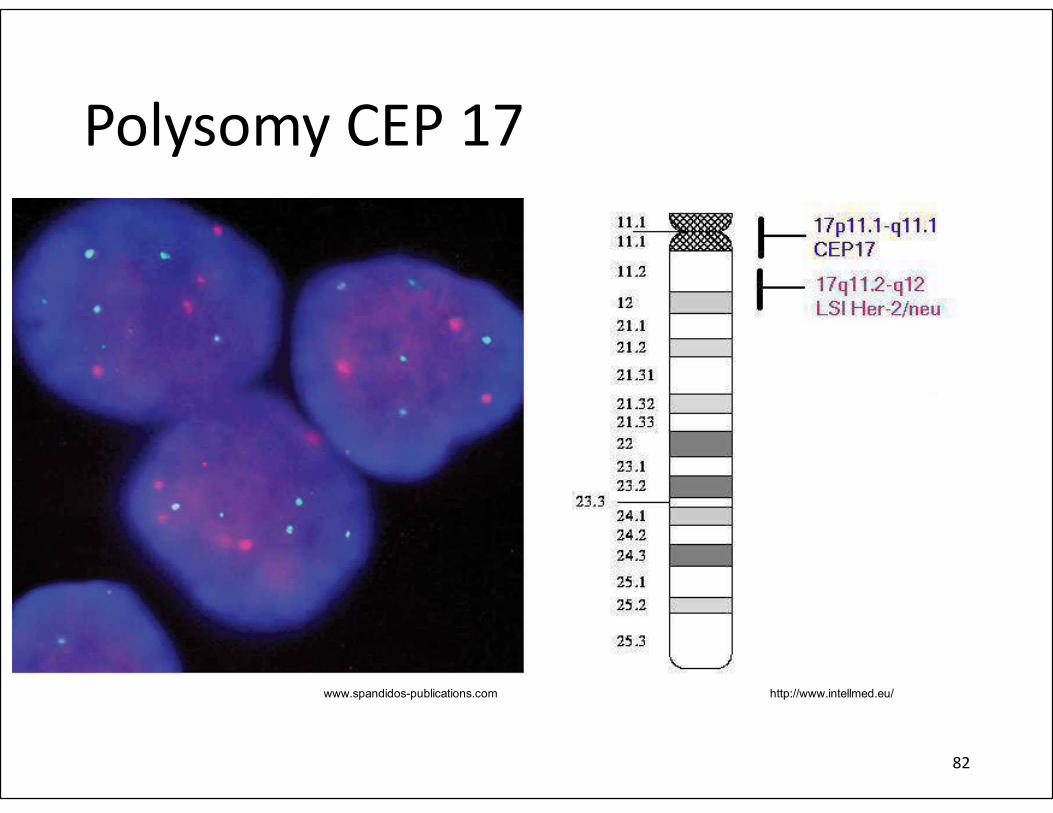
http://www.intellmed.eu/www.spandidos-publications.com
Polysomy CEP 17
82
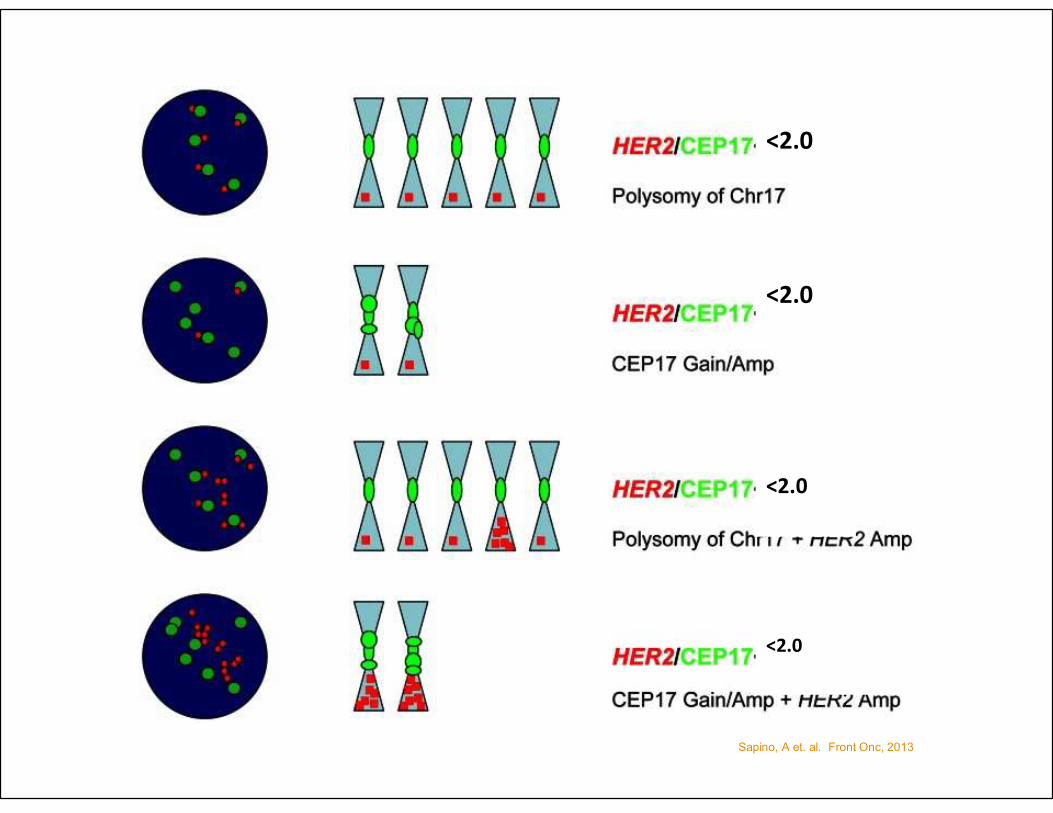
Sapino, A et. al. Front Onc, 2013
<2.0
<2.0
<2.0
<2.0
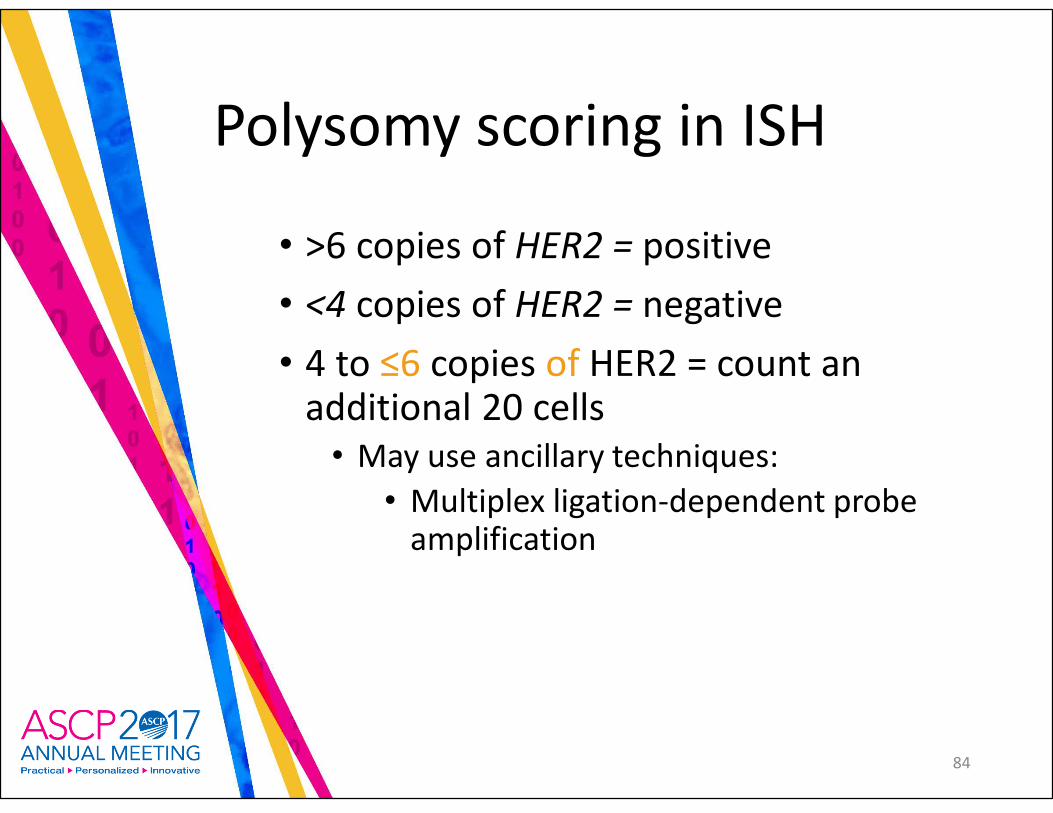
Polysomy scoring in ISH
• >6 copies of HER2 = positive
• <4 copies of HER2 = negative
• 4 to ≤6 copies of HER2 = count an additional 20 cells
• May use ancillary techniques:
• Multiplex ligation-dependent probe amplification
84
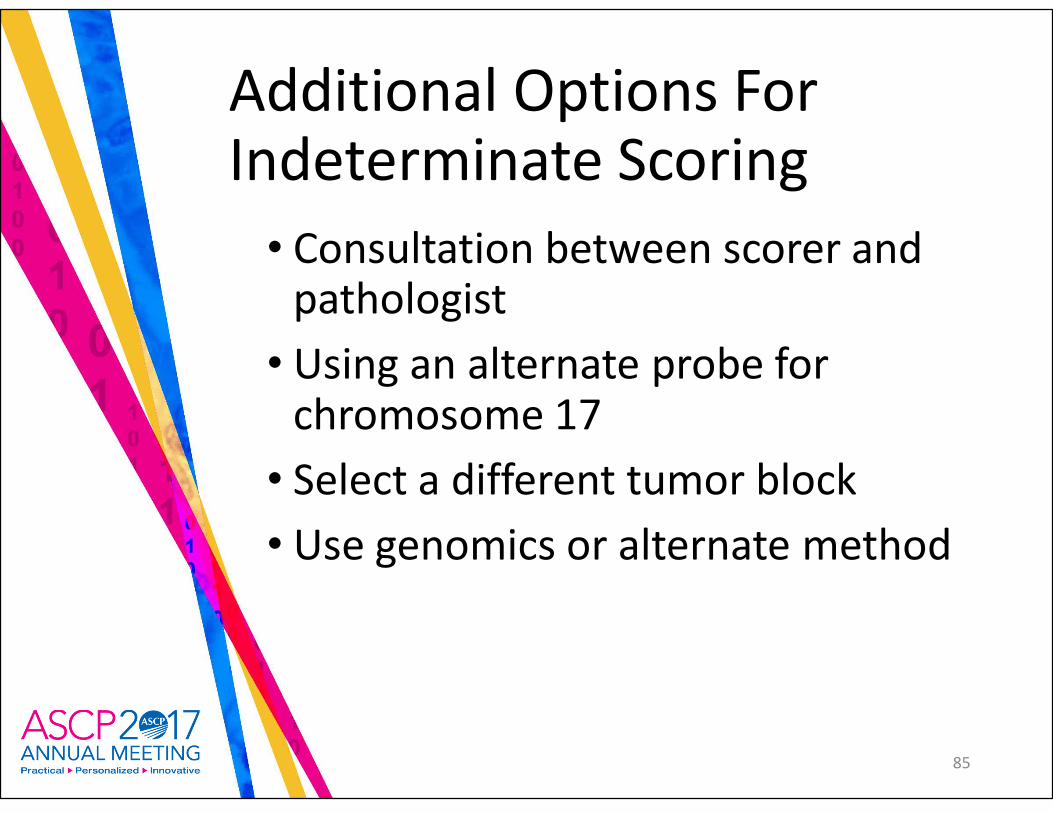
Additional Options For Indeterminate Scoring
• Consultation between scorer and pathologist
• Using an alternate probe for chromosome 17
• Select a different tumor block
• Use genomics or alternate method
85
Quality Assurance
• Assure adequate staining without:
• Background interference
• Overdigestion
• Other artifacts
Failure to detect probe signals in non-malignant cells can indicate poor quality hybridization
86
Technical issues = indeterminate
87
Recommendation 9
• Strong recommendation: Pathologists should identify areas of invasive adenocarcinoma and also mark areas with strongest intensity of HER2 expression by IHC in GEA specimen for subsequent scoring when ISH is required.
• (Quality of evidence: Moderate/Intermediate; Strength of recommendation: Strong)
88
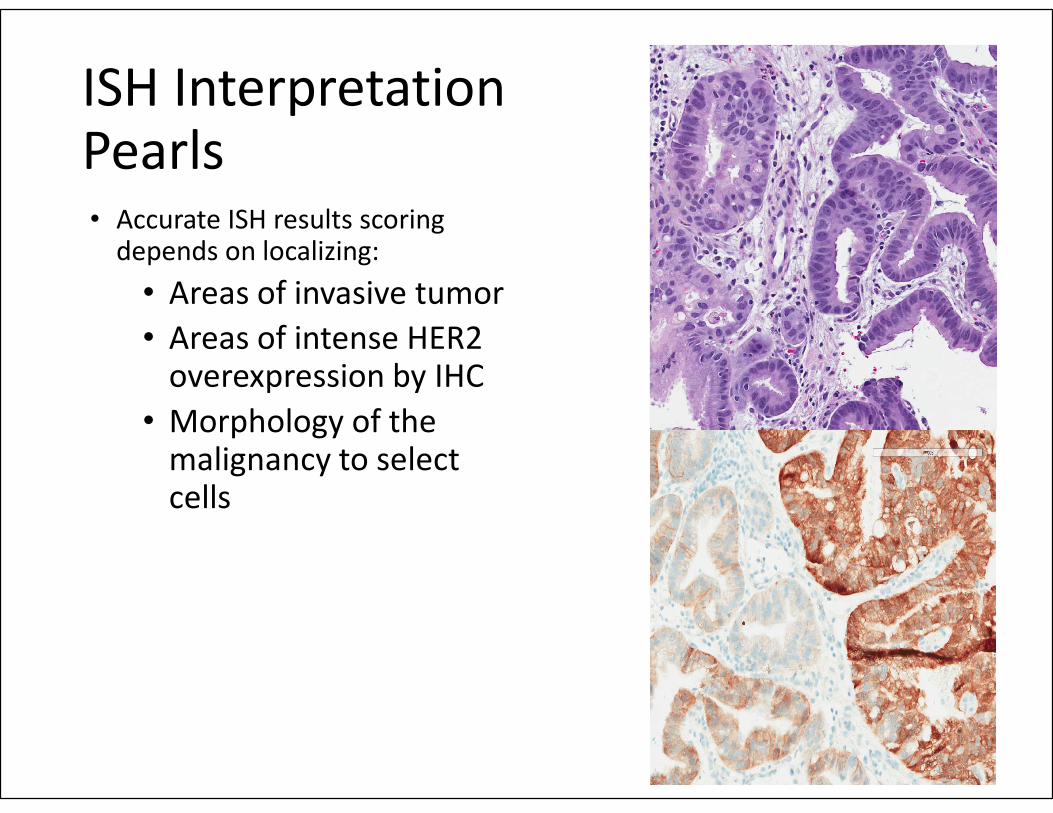
ISH Interpretation Pearls• Accurate ISH results scoring
depends on localizing:
• Areas of invasive tumor
• Areas of intense HER2 overexpression by IHC
• Morphology of the malignancy to select cells
89
ISH Interpretation Pearls
• Morphologic evaluation of ISH stains helps resolve problematic interpretations due to:
• Over or under fixation
• Delayed fixation
• Inadequate deparaffinization
• Protease digestion
90
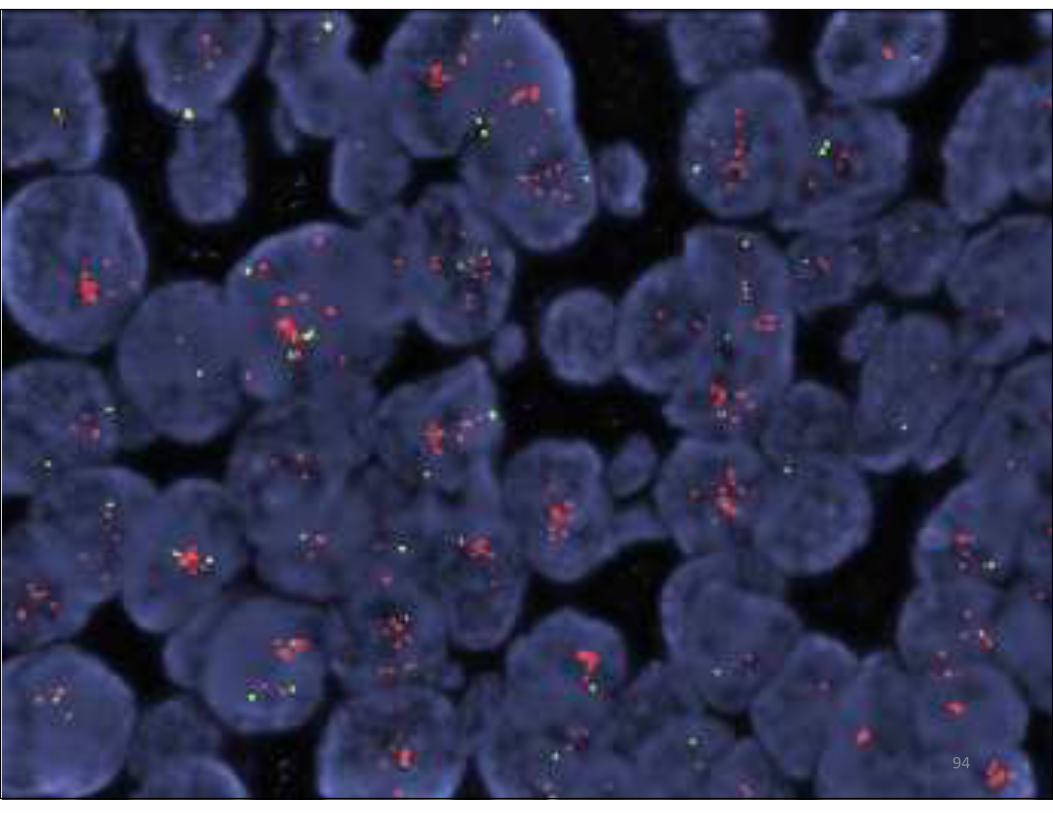
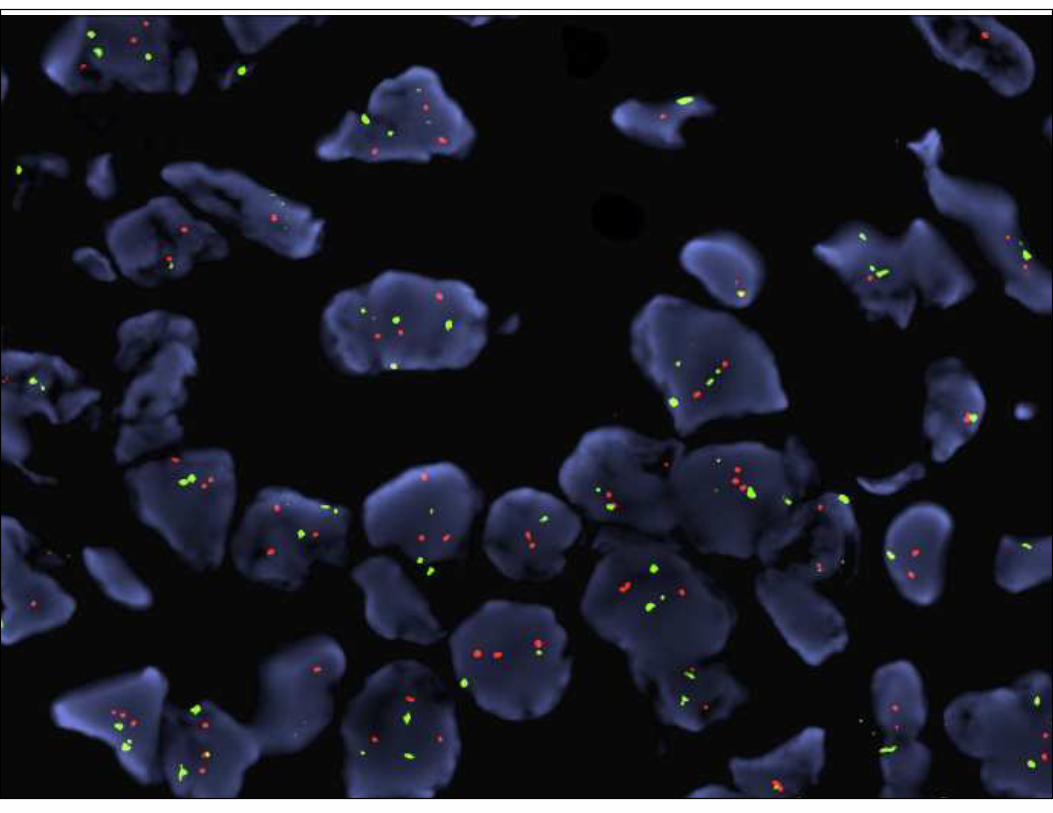
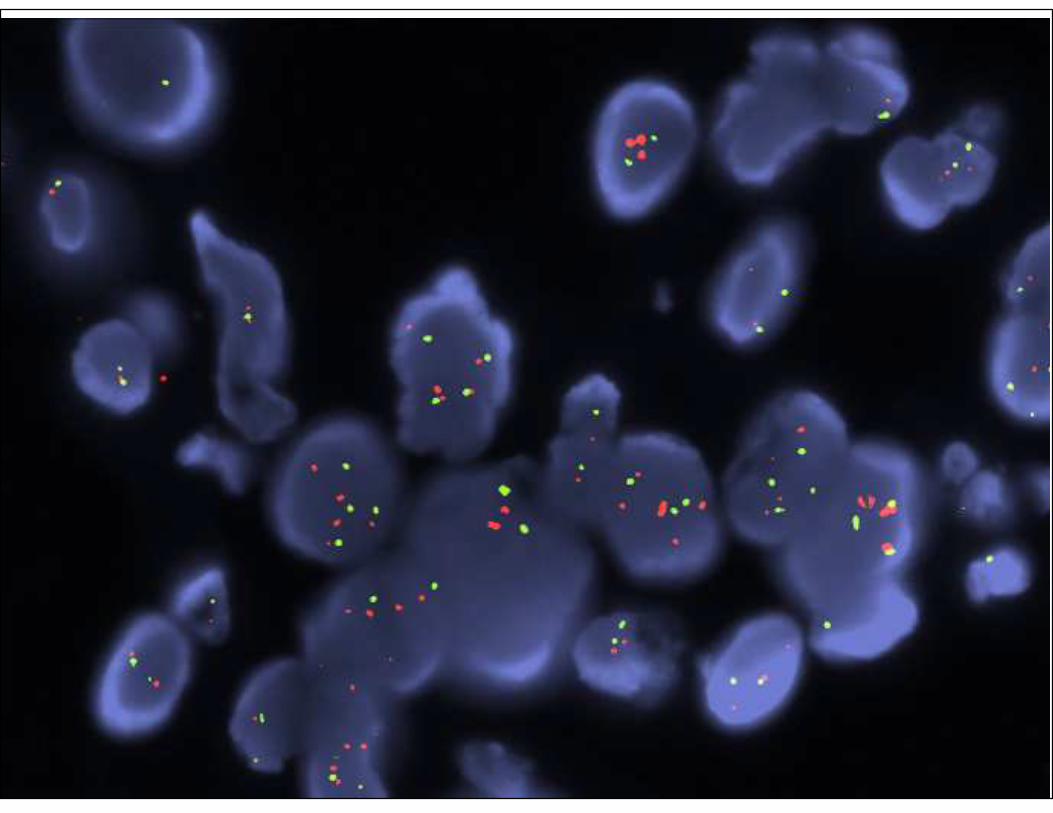
Examples of Real Cases:IHC and FISH Correlation
91
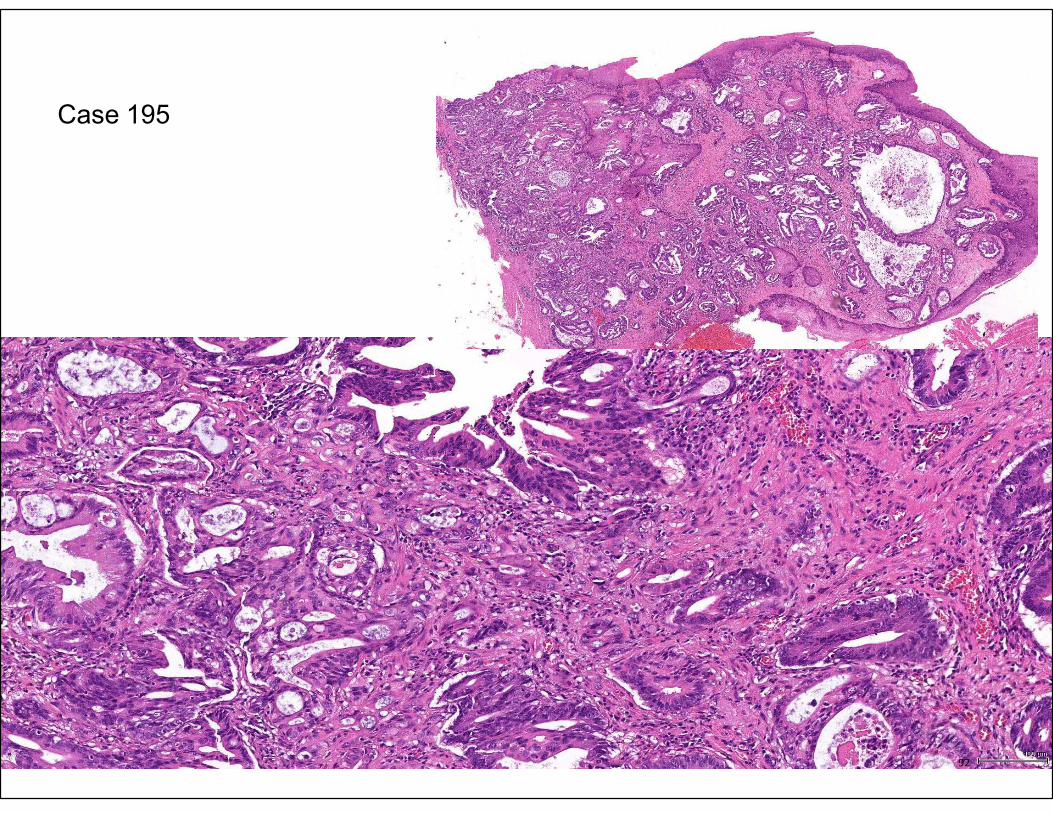
Case 195
92
93
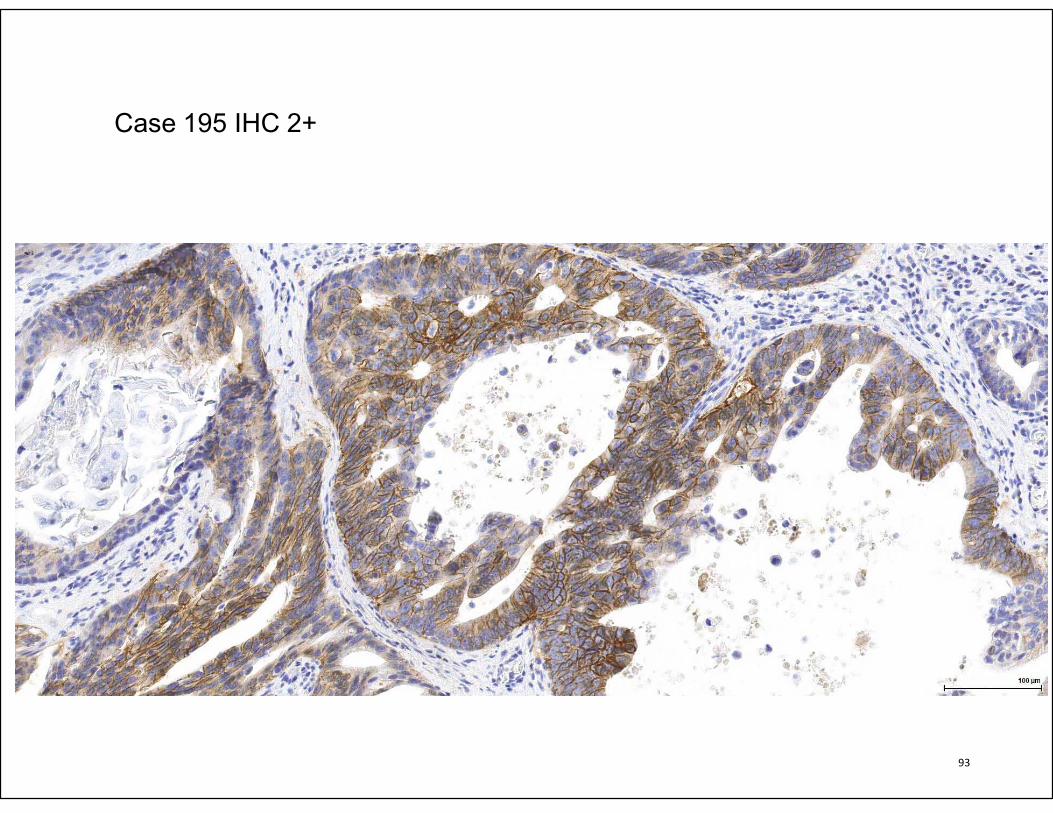
Case 195 IHC 2+
94
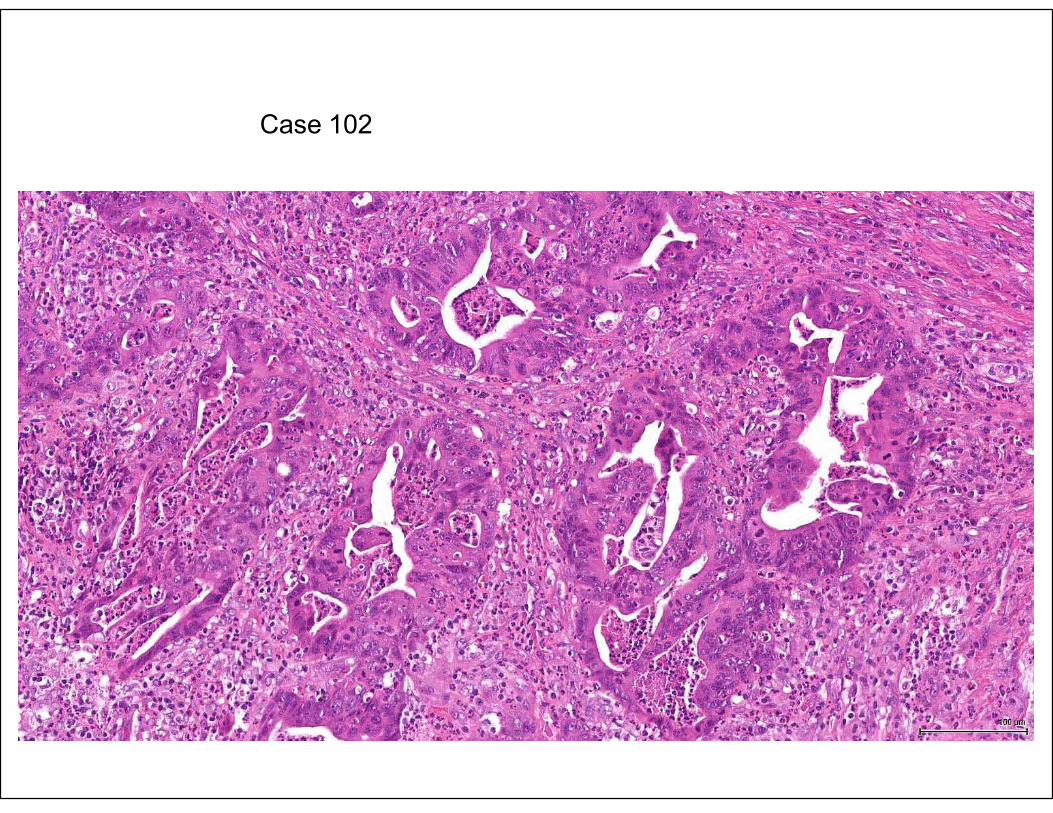
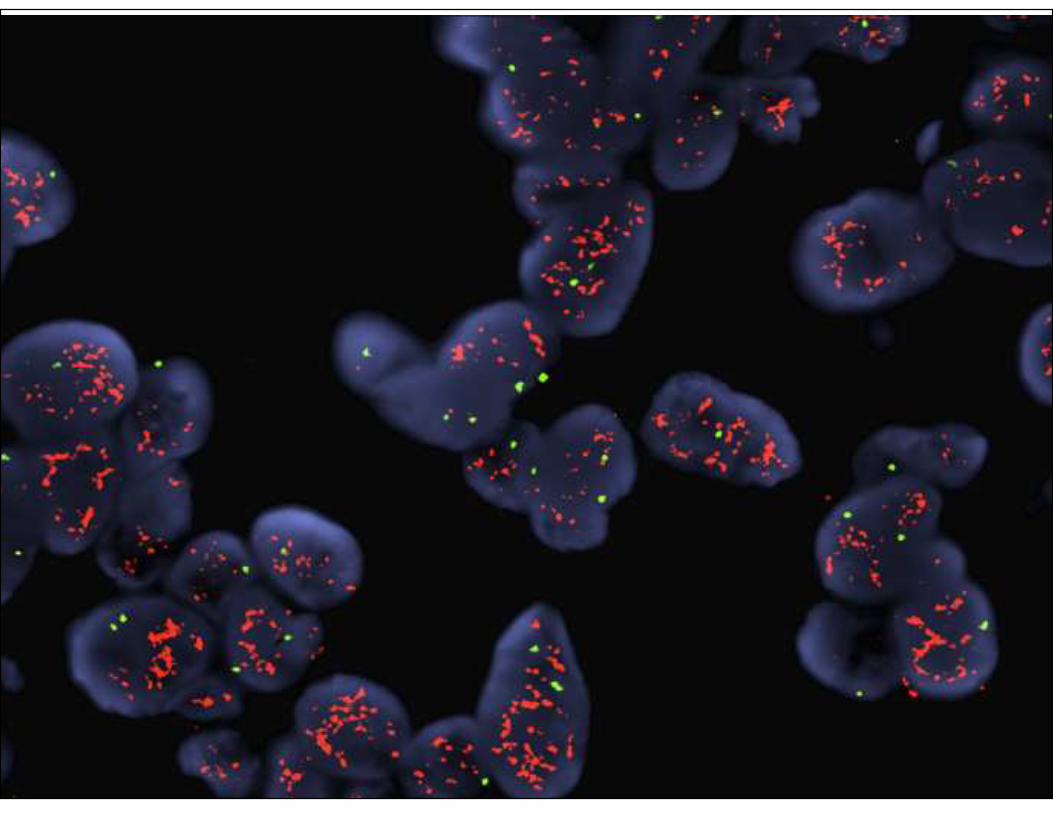
Case 102
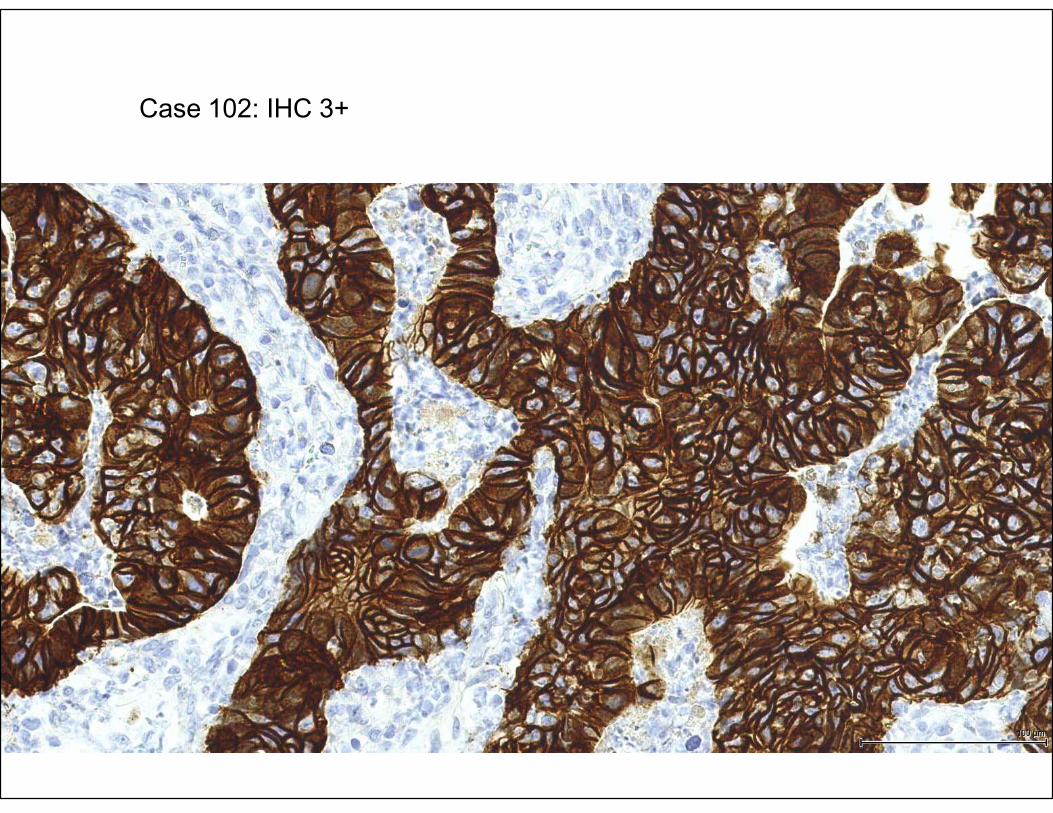
Case 102: IHC 3+
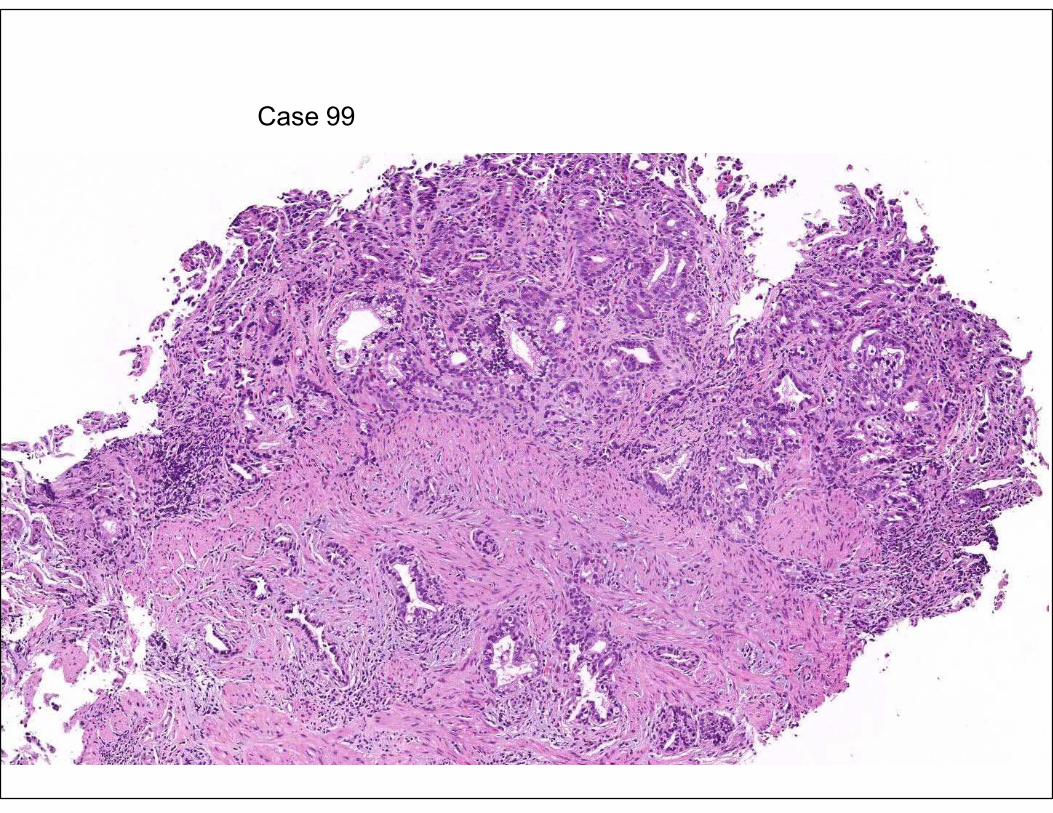
Case 99
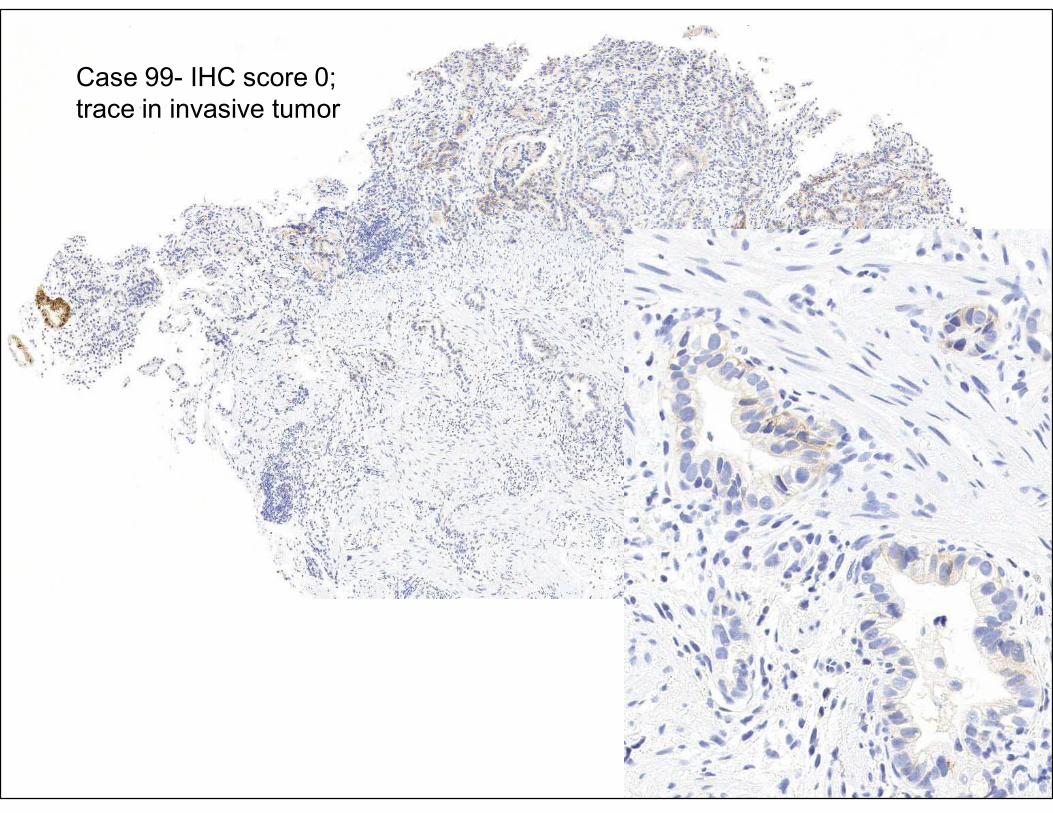
Case 99- IHC score 0;
trace in invasive tumor
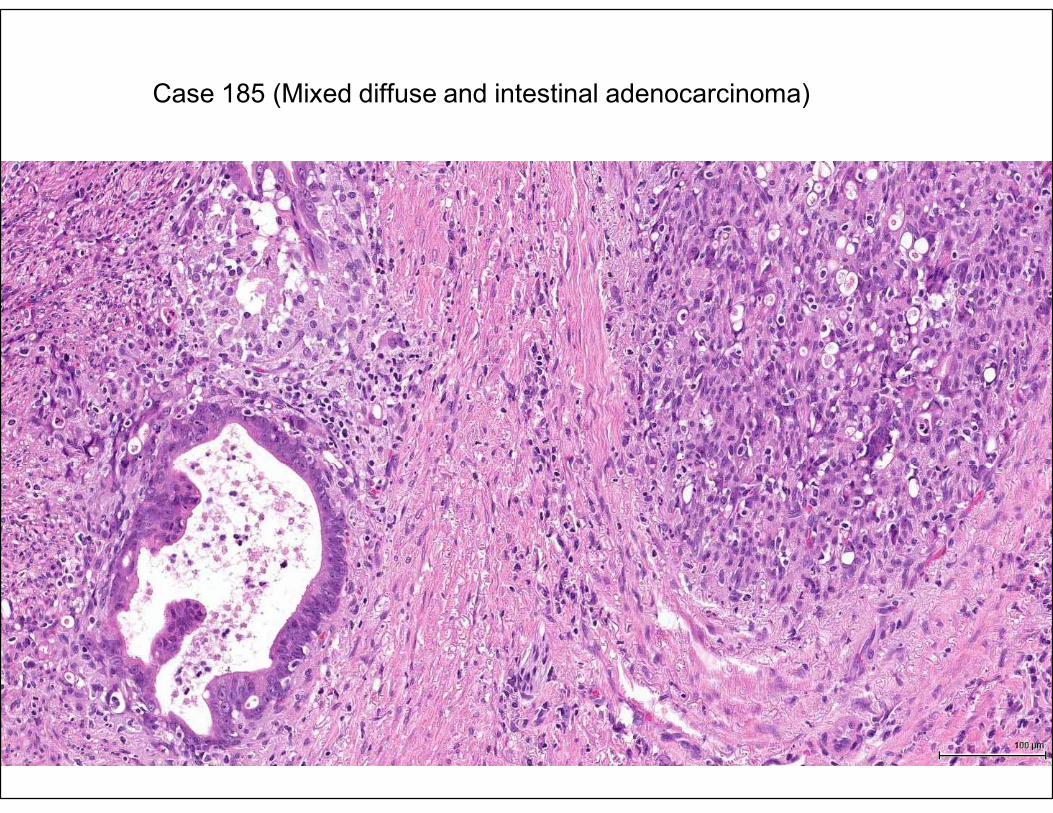
Case 185 (Mixed diffuse and intestinal adenocarcinoma)
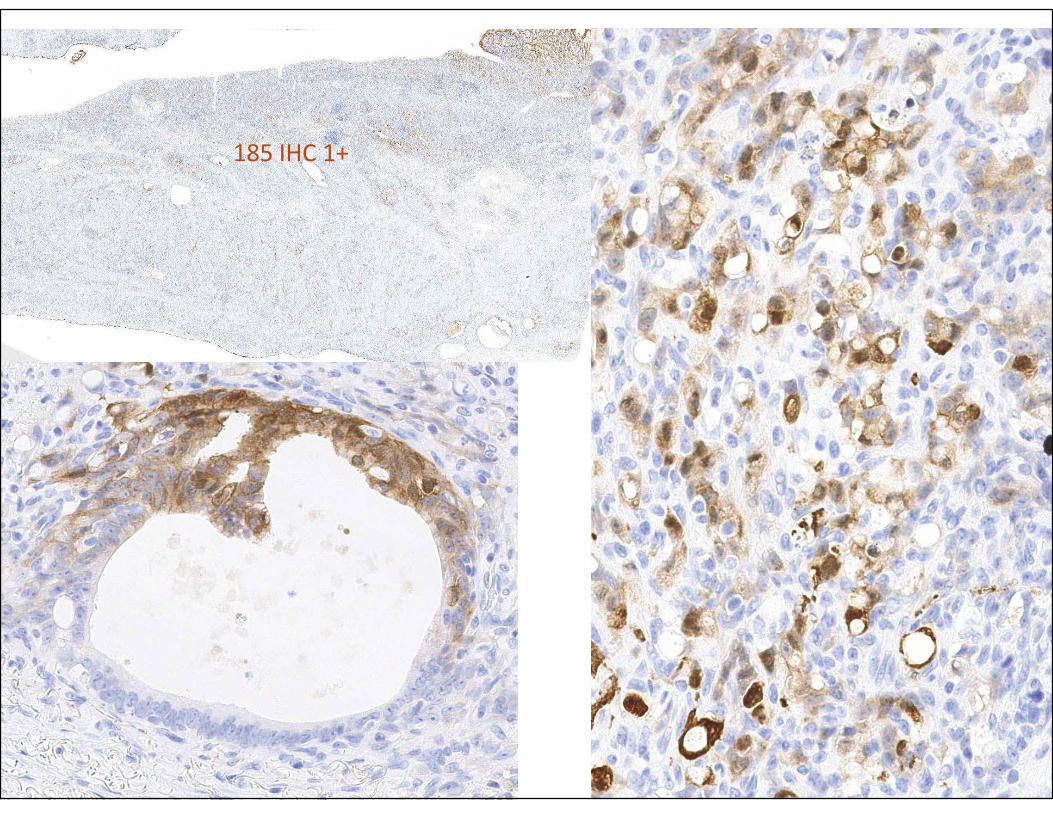
185 IHC 1+
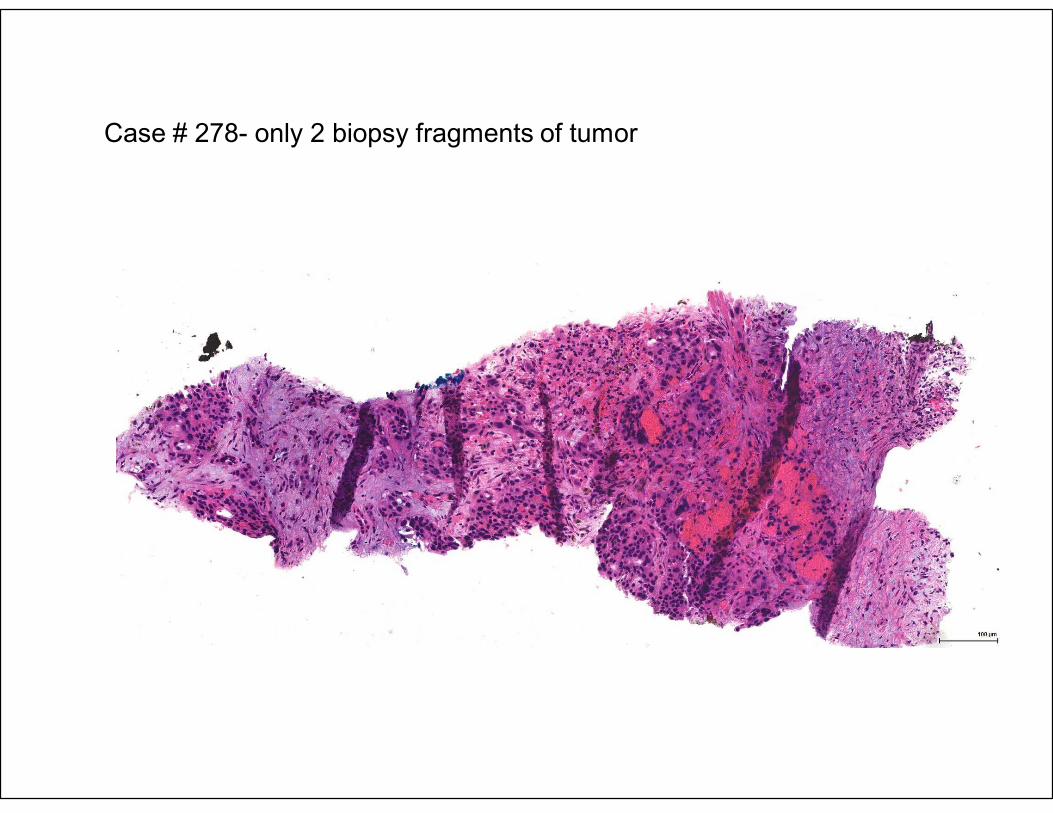
Case # 278- only 2 biopsy fragments of tumor
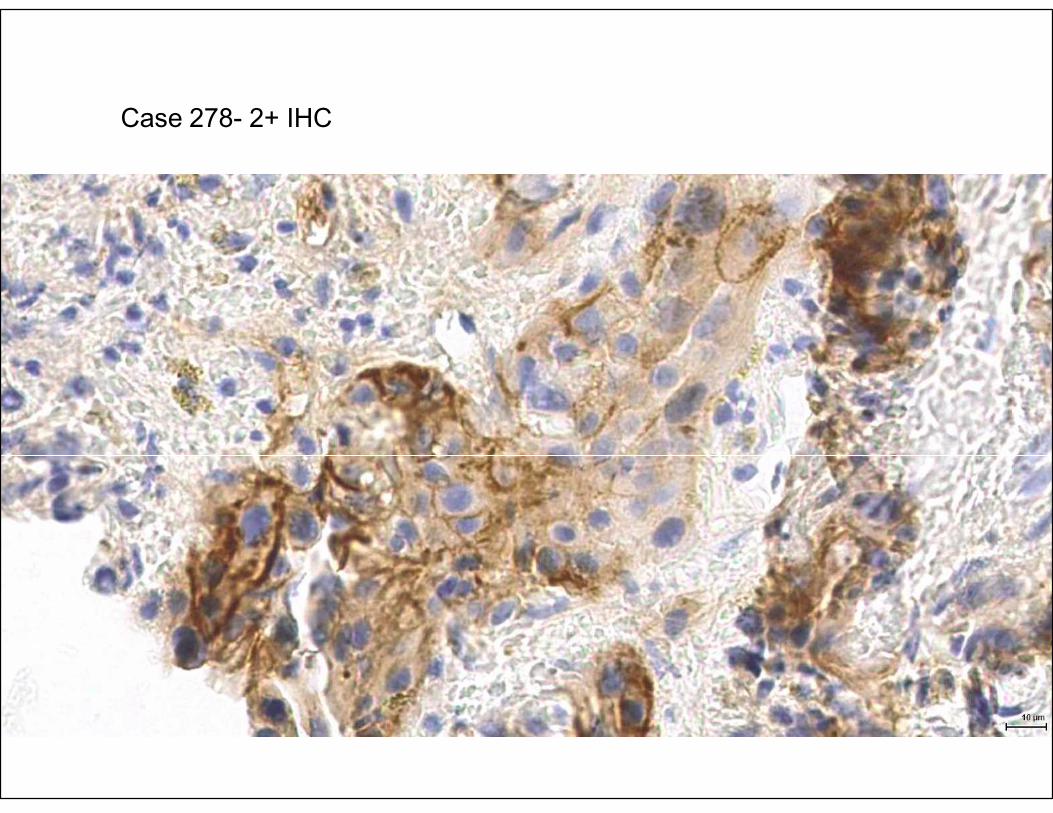
Case 278- 2+ IHC
Recommendation 10
• Strong Recommendation: Laboratories must incorporate GEA HER2 testing methods into their overall laboratory quality improvement program, establishing appropriate quality improvement monitors as needed to assure consistent performance in all steps of the testing and reporting process. In particular, laboratories performing GEA HER2 testing must participate in a formal proficiency testing program, if available, or an alternative proficiency assurance activity.
• (Quality of evidence: Moderate/Intermediate; Strength of recommendation: Strong)
107
Recommendation 11
• No Recommendation: There is insufficient evidence to recommend for or against genomic testing in GEA patients at this time.
108
• Polymerase chain reaction (PCR)
• Single nucleotide polymorphism (SNP) chip
• Comparative genomic hybridization (CGH) array
• Gene expression profiling by RNAseq or microarray
• Targeted/exome/whole genome sequencing
• Recent data showing 98% concordance of NGSwith HER2 IHC/FISH
(Ross DS, et al. J Mol Diagnostics 12(2):244-54, 2017)
• Quantitative proteomic analysis
109
Other techniques used to determine HER2 status
Recommendation 8
• Strong Recommendation: Laboratories should report HER2 testing results in GEA specimens in accordance with the CAP biomarker “Template for Reporting Results of HER2 (ERBB2) Biomarker Testing of Specimens From Patients With Adenocarcinoma of the Stomach or Esophagogastric Junction”.
• (Quality of evidence: Moderate/Intermediate; Strength of recommendation: Strong)
110
Source: Bartley AN, Christ J, Fitzgibbons PL, et al. Template for reporting results of HER2 (ERBB2) biomarker testing of specimens from patients with
adenocarcinoma of the stomach or esophagogastric junction. Arch Pathol Lab Med. 2015;139(5):618-620.111

Turnaround Time
112
Turnaround Time
• Report HER2 results as promptly as possible
• Benchmark: 90% of reports within 10 working days from the date of procedure or specimen acquisition
• Send out testing: 90% of specimens sent to the reference laboratory within 3 working days of tissue processing
113

114
© 2016 College of American Pathologists. Materials are used with the permission of the faculty.
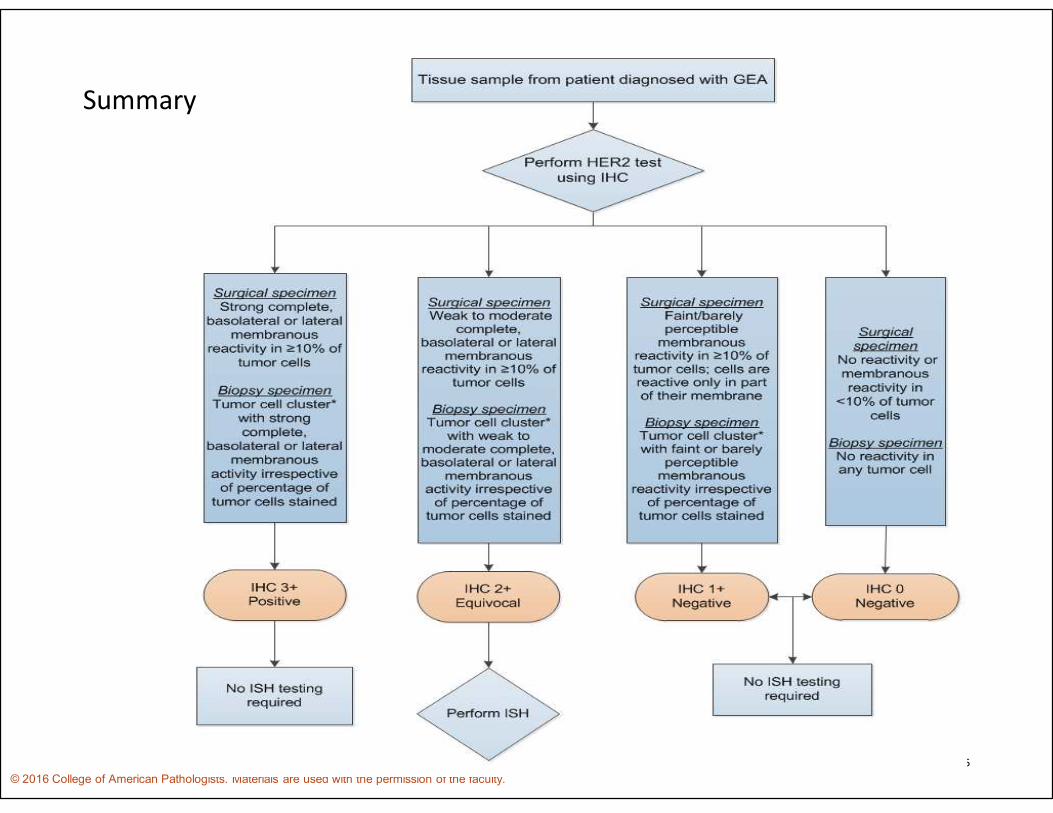
Summary
115
© 2016 College of American Pathologists. Materials are used with the permission of the faculty.
Summary
Future Directions
• Guideline will be reviewed every 4 years, or earlier as warranted as new data become available
116
Future Directions
117
• The JACOB (trastuzumab/pertuzumab) Study results are anticipated soon and it may change the paradigm
• Vaccine strategy using Her2 extracellular domain as the docking molecule for highly immunogenic sequences
• Bi-specific antibodies that may reduce secondary resistance and immune stimulation (including the innate immunity)
© 2016 College of American Pathologists. Materials are used with the permission of the faculty.
Future Directions
118
• More potent conjugates to include Her2 neu negative population (Her2 2+ but not amplified)
• Dual pathway inhibition by anticipating emerging resistance (other oncogenes like Her3, EGFR, IGF, c-MET to be targeted early on to prevent secondary resistance)
© 2016 College of American Pathologists. Materials are used with the permission of the faculty.
Pearls of Pathology
• HER2 testing is appropriate for advanced or metastatic GEA
• Guideline recommends use of IHC first, followed by ISH for 2+ cases
• Use the Ruschoff/Hoffman scoring system
• Scoring systems for HER2 in breast cancer are not appropriate for GEA
119© 2016 College of American Pathologists. Materials are used with the permission of the faculty.
References• Abrahao-Machado LF, Jacome AA, Wohnrath DR, et al. HER2 in gastric cancer: comparative analysis of three different
antibodies using whole-tissue sections and tissue microarrays. World J Gastroenterol. 2013;19(38):6438-6446.
• Aizawa M, Nagatsuma AK, Kitada K, et al. Evaluation of HER2-based biology in 1,006 cases of gastric cancer in a Japanese population. Gastric Cancer. 2014;17(1):34-42.
• Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687-697.
• Bartley AN, Christ J, Fitzgibbons PL, et al. Template for reporting results of HER2 (ERBB2) biomarker testing of specimens from patients with adenocarcinoma of the stomach or esophagogastric junction. Arch Pathol Lab Med. 2015;139(5):618-620.
• Bozzetti C, Negri FV, Lagrasta CA, et al. Comparison of HER2 status in primary and paired metastatic sites of gastric carcinoma. . Br J Cancer. 2011;104(9):1372-1376.
• Corso S, Giordano S. How can gastric cancer molecular profiling guide future therapies? Trends Mol Med. 2016;22(7):534-544.
• Grabsch H, Sivakumar S, Gray S, Gabbert HE, Muller W. HER2 expression in gastric cancer: rare, heterogeneous and of no prognostic value - conclusions from 924 cases of two independent series. Cell Oncol. 2010;32(1-2):57-65.
• Gullo I, Grillo F, Molinaro L, et al. Minimum biopsy set for HER2 evaluation in gastric and gastro-esophageal junction cancer. Endosc Int Open. 2015;3(2):E165-170.
• Guyatt GH, Oxman AD, Vist GE, et al; GRADE Working Group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendation. BJM. 2008;336(7650):924-926.
120
© 2016 College of American Pathologists. Materials are used with the permission of the faculty.
References• Hofmann M, Stoss O, Shi D, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation
study. Histopathology. 2008;52(7):797-805.
• Inoue K, Fry EA. Aberrant splicing of estrogen receptor, HER2, and CD44 genes in breast cancer. Genet Epigenet. 2015;7:19-32.
• Janjigian YY, Werner D, Pauligk C, et al. Prognosis of metastatic gastric and gastroesophageal junction cancer by HER2 status: a European and USA international collaborative analysis. Ann Oncol. 2012;23(10):2656-2662.
• Jiang H, Bai X, Zhao T, Zhang C, Zhang X. Fluorescence in situ hybridization of chromosome 17 polysomy in breast cancer using thin tissue sections causes the loss of CEP17 and HER2 signals. Oncol Rep. 2014;32(5):1889-1896.
• Junttila TT, Akita RW, Parsons K, et al. Ligand-independent HER2/HER3/PI3K complex is disrupted by trastuzumab and is effectively inhibited by the PI3K inhibitor GDC-0941. Cancer Cell. 2009;15(5):429-40.
• Okines AF, Thompson LC, Cunningham D, et al. Effect of HER2 on prognosis and benefit from peri-operative chemotherapy in early oesophago-gastric adenocarcinoma in the MAGIC trial. Ann Oncol. 2013;24(5):1253-1261.
• Pirrelli M, Caruso ML, Di Maggio M, Armentano R, Valentini AM. Are biopsy specimens predictive of HER2 status in gastric cancer patients? Dig Dis Sci. 2013;58(2):397-404.
• Qiu Z, Sun W, Zhou C, Zhang J. HER2 expression variability between primary gastric cancers and corresponding lymph node metastases. Hepatogastroenterology. 2015;62(137):231-233.
121
© 2016 College of American Pathologists. Materials are used with the permission of the faculty.
References• Ruschoff J, Hanna W, Bilous M, et al. HER2 testing in gastric cancer: a practical approach. Mod Pathol. 2012;25(5):637-
650.
• Sapino A, Goia M, Recupero D, Marchio C. Current challenges for HER2 testing in diagnostic pathology: state of the art and controverial issues. Front Oncol. 2013;3:129.
• Selcukbiricik F, Erdamar S, Buyukunal E, Serrdengecti S, Demirelli F. Is HER-2 status in the primary tumor correlated with matched lymph node metastases in patients with gastric cancer undergoing curative gastrectomy? Asian Pac J Cancer Prev. 2014;15(24):10607-10611.
• Smyth MJ, Stagg J. Her 2 in 1. Cancer Cell. 2010;18(2):101-102
• U.S. Food and Drug Administration.Herceptin (trastuzumab) final labeling text. http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/103792s5250lbl.pdf. Accessed: March 28, 2016.
• Van Cutsem E, Bang YJ, Feng-Yi F, et al. HER2 screening data from ToGA: targeting HER2 in gastric and gastroesophageal junction cancer. Gastric Cancer. 2015;18(3):476-484.
• Wolff AC, Hammond ME, Hicks DG, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practie guideline update. J Clin Oncol. 2013;31(31):3997-4013.
• Yarden Y, Pines G. The ERBB network: at last, cancer therapy meets systems biology. Nat Rev Cancer. 12:553-563.
• Yoshida H, Yamamoto N, Taniguchi H, et al. Comparison of HER2 status between surgically resected specimens and matched biopsy specimens of gastric intestinal-type adenocarcinoma. Virchows Arch. 2014;465(2):145-154.
• Zagozdzon R, Gallagher WM, Crown J. Truncated HER2: implications for HER2-tareted therapeutics. Drug Discov Today. 2011;16(17-18):810-816.
122
© 2016 College of American Pathologists. Materials are used with the permission of the faculty.

Thank you for participating!
123





![Interpretation Guide for VENTANA anti-HER2/neu (4B5) · 2 3 Introduction VENTANA anti-HER2/neu (4B5) Rabbit Monoclonal Primary Antibody [VENTANA HER2 (4b5)] is intended for the semi-quantitative](https://img.pdfslide.us/doc/110x75/5afd73a27f8b9aa34d8d810f/interpretation-guide-for-ventana-anti-her2neu-4b5-3-introduction-ventana-anti-her2neu.jpg)


![Primary cutaneous lymphomas: single center experience of … · in tumor stage and approximately 20% in histo-logical lymph node involvement [9-11]. Lymph node,inner organ involvement](https://img.pdfslide.us/doc/110x75/5e5e51adcf8b202fd16e13c3/primary-cutaneous-lymphomas-single-center-experience-of-in-tumor-stage-and-approximately.jpg)