Embed Size (px)
DESCRIPTION
--
Citation preview

FISIOLOGI KEHAMILAN

Physiology changes associated with pregnancy
Reproductive Tracts Breast Skin Water and Electrolit Hematology Cardiovascular
System
Respiratory System Gastrointestinal
System Urinary System Endocrine System Metabolism Skeleton


Reproductive Tracts
Uterus: from 50g-1100g
Isthmus uteri (lower segment of the uterus) Hegar sign
Braxton Hicks contraction: sporadic, irregular, asymmetrical, and painless, low pressure, lasting < 30 sec

Reproductive Tracts
Cervix and vulva —— Chadwick’s sign congestion of the pelvic vasculature, cause bluish or purplish discoloration of the cervix and vulva
Leukorrhea: increase in vaginal discharge, rich in glucose, lactic acid, low vaginal pH
Ovary: slightly enlarged, corpus luteum regresses after 10 weeks’ gestation

Breasts Early change
tenderness, tingling and heaviness vascular engorgement leads to enlargement
Ductal growth due to estrogen Alveolar hypertrophy due to progesteron
Enlargement and pigmentation of areolae Montgomery’s tubercles: enlargement of circumlacteal
sebaceous glands of the areola Colostrum may be expressed later in pregnancy Milk production
Estrogen, progesteron, prolactin, hPL, cortisol and insulin
Lactation likely due to drop in estrogen and progesterone after delivery

Skin
Spider angiomata (face, upper chest, and arm) and palmar erythemaelevated estrogen levels both regress after delivery
Striae gravidarum Increased eccrine sweating and sebum
excretion Hyperpigmentation Melasma: “mask of pregnancy”
elevated estrogen and progesteron Nevi may darken, enlarge or show increased
activity rapidly changing nevi should be excised

Body Water
TBW increases from 6.5L to 8.5L At term water content of fetus, placenta and
AF is 3.5L BV, PV, RBC, extravascular, intracellular
Pregnancy is a condition of chronic volume overload
Water retention exceeds Na retention-decreased plasma osmolality

Hematology – Blood volume
Increases progressively from 6 to 8 weeks gestation
maximum volume at 32 weeks - 45% increase
possibly due to estrogen stimulation of renin-angiotensin-aldosterone system
(Inc Prog, NO->Dec SVR->Dec MAP->Inc Na retention)


Hematology – RBC mass
Red blood cell mass increases by 250-450 cc by term
Increased production Possibly hormonally
mediated

Hematology - Iron Maternal requirement is
1000mg Increase maternal red cell mass : 500 mg Fetal development : 300 mg Compensate for normal iron loss : 200 mg
Normal pregnant woman needs to absorb about 3.5 mg/day of iron
the goal of iron supplementation is to prevent maternal iron deficiency
Iron is actively transported to the fetus

Hematologic changes
IMPLICATIONSThe increase in plasma volume and
rbc mass translates into a 45% increase in circulating blood volume
may protect from hemodynamic instability
may serve to dissipate fetal heat production and provide increase renal filtration
physiologic anemia of pregnancy may function to decrease blood viscosity may improve intervillous perfusion?

Hematology
LEUKOCYTES Peripheral wbc rises progressively during
pregnancy 1st ∆ – mean 9500/mm3 (3000-15,000) 2nd and 3rd ∆ – mean 10,500 (6000-16,000) Labor – may rise to 20-30,000
Rise is due to increase in pmns (demargination)
PLATELETS Platelets experience a progressive decline but
should remain within normal range Likely due to increased destruction

Hematology
COAGULATION FACTORSIncreased levels
Fibrinogen (Factor I) Factors VII through X
No change in prothrombin (Factor II), Factors V and XII
Decline in platelet count, Factors XI and XIII Bleeding time and clotting time are
unchanged in normal pregnancy

Cardiovascular – Cardiac output
Maternal cardiac output increases about 30-50% during pregnancy (mean 33%) pregnancy maximum of 6 L/min CO remains maximal until delivery Earliest rise in CO is due to increase in SV As pregnancy progresses
Gradual increase in mat HR (15-20 bpm rise) SV declines to near non-pregnant levels increase HR is what maintains the elevated CO


Cardiovascular – Cardiac output
CO is position dependent Lower when supine
IVC compression by the uterus reduces venous return to the heart
At 38-40 weeks, there is a 25-30% fall in CO when turning from the side to the back
Fall in CO is compensated by a rise in peripheral vascular resistance supine hypotensive syndrome (1-10% patients)

Cardiovascular – Cardiac output
Distribution of CO First trimester and non-pregnant state
Uterus receives 2-3% By term
Uterus receives 17% Breasts 2%
Reduction of the fraction of CO going to the splanchnic bed and skeletal muscle
CO to the kidneys, skin, brain and coronary arteries does not change

Cardiovascular – Arterial BP
BP varies with position
Peripheral vascular resistance falls during pregnancy
Progesterone’s smooth muscle relaxing effect ?heat production by the fetus vasodilatation
The reduction in PVR may lead to a progressive fall in systemic arterial bp during the first 24 weeks of pregnancy
Gradual rise after 24 weeks non-pregnant levels by term

Cardiovascular – Venous system
Venous compliance increases during pregnancy decrease in flow velocity and stasis progesterone effects on smooth muscle Forearm venous pressure increases by 40-50% Calf venous pressures are always higher
due to the enlarging uterus

Cardiovascular - LV function
Left ventricular dimensions and volume increase during pregnancy most parameters of LVF are the same as in the
non-pregnant state Ejection fraction, rate of internal diameter
shortening, percentage of fractional shortening, and ventricular wall thickness
Bottom line: preservation of myocardial function

Cardiovascular changes
Stroke volume +30% Heart rate +15% Cardiac output +40% Oxygen consumption +20% SVR (systemic vascular resistance) -5% Systolic BP -10mmHg Diastolic BP -15mmHg Mean BP -15mmHg

Respiratory system
UPPER RESPIRATORY TRACT Hyperemic mucosa of nasopharynx
Estrogen-mediated nasal stuffiness and epistaxis
Polyposis of nose and sinuses may occur and regress after delivery
“chronic cold”
MECHANICAL CHANGES Configuration of thoracic cage changes early in
pregnancy Increase in subcostal angle, transverse diameter and
circumference of chest With advancing gestation, the level of diaphragm is
pushed up


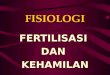
Changes in pulmonary function tests during pregnancy
Serial measurements of lung volume compartments during pregnancy. Functional residual capacity decreases approximately 20 percent during the latter half of pregnancy, due to a decrease in both expiratory reserve volume and residual volume. Redrawn from Prowse, CM, Gaensler, EA, Anesthesiology 1965; 26:381.
Serial measurements of lung volume compartments during pregnancy. Functional residual capacity decreases approximately 20 percent during the latter half of pregnancy, due to a decrease in both expiratory reserve volume and residual volume. Redrawn from Prowse, CM, Gaensler, EA, Anesthesiology 1965; 26:381.

Respiratory system
LUNG VOLUME AND PULMONARY FUNCTION 30-40% increase in tidal volume (Amount of
air I and E with each breath) 30-40% increase in minute ventilation (likely P4
mediated) ERV falls by 20% Vital capacity and inspiratory reserve volume
remain unchanged

Respiratory system
LUNG VOLUME AND PULMONARY FUNCTION Respiratory rate is unchanged Due to elevation of the diaphragm
Total lung volume decreases (diaphragm) by 5% Residual volume decreases (RV) by 20% FRC is reduced 20%
No change in FEV1 or the ratio of FEV1 to forced vital capacity

Respiratory system
GAS EXCHANGE Minute ventilation rises 30-40% by late
pregnancy O2 consumption increases only 15-29%
Results in higher PAO2 (alveolar) and PaO2 (arterial) Normal PaO2: 104-108 mmHg
Fall in PACO2 and PaCO2 levels Normal PaCO2 level: 27-32 mmHg
Increases gradient of CO2 facilitating transfer from fetus to mother
Arterial pH remains unchanged Increased bicarbonate excretion via kidneys

Respiratory system
DYSPNEA OF PREGNANCY Common complaint
60-70% of patients late first or early second trimester
Likely due to various factors reduced PaCO2 levels awareness of increased tidal volume of
pregnancy


Renal system
ANATOMY Kidney enlargement
increased renal vascular and interstitial volume, R>L Ureteral and renal pelvis dilatation by 8 weeks
Right > left mechanical compression by uterus and ovarian venous
plexus smooth muscle relaxation by progesterone
Implications Increased incidence of pyelonephritis difficulty in interpreting radiographs interference with studies

Renal system
RENAL HEMODYNAMICS Effective renal plasma flow (ERPF) and GFR
increase Filtration fraction falls
Returns to normal by late third Δ Endogenous creatinine clearance increases
Begins by 5 weeks

Renal system
METABOLITES increased GFR decline in serum urea and
creatinine BUN – 8-9 mg/dl by end 1st Δ Decline in serum creatinine
0.7 mg/dl by end 1st Δ 0.5-0.6 mg/dl by term
Early decline in serum uric acid levels nadir at 24 weeks same as nonpregnant level at end of pregnancy due
to increased reabsorption of urate

Renal system
SALT AND WATER METABOLISM Plasma osmolality begins to decline by 2
weeks after conception reduction in serum sodium and other anions
Sodium loss during pregnancy 50% rise in GFR Progesterone: natriuresis
Renal tubular reabsorption of Na+ increases (aldosterone, estrogen and deoxycorticosterone)
Sodium homeostasis

Renal system
NUTRIENT EXCRETION Increase in glucose excretion
1-10 g glucose excretion per day Due to 50% increase in GFR
implications inability to use urine glucose susceptibility of pregnant women to UTI
Increase in amino acid excretion during gestation no increased protein loss (100-300 mg/24 hr)
Increased urinary loss of folate and vitamin B12

Gastrointestinal - Appetite
Increase early 1st Δ
Increase intake 200 kcal by end 1st Δ RDA: 300 kcal/day during pregnancy
Sense of taste may be blunted
Pica check for poor weight gain and refractory
anemia South - clay or starch (laundry or cornstarch) UK – coal Also soap, toothpaste and ice pica

Gastrointestinal - Mouth Unchanged pH or production of saliva
Saliva production is unaltered Ptyalism – usually in women with HEG
due to inability to swallow Can lose up to 1-2 L of saliva per day Decreasing starchy foods might help
Gums – edematous and soft May bleed after brushing
Epulis gravidarum regress 1-2 mos after delivery excise if persistent or excessive bleeding

Gastrointestinal - Stomach
Decreased tone and motility progesterone possibly due to decreased levels of motility
Conflicting info about delayed gastric emptying
Reduced tone of the gastroesophageal junction sphincter Increased intraabdominal pressure leads to acid
reflux Lower incidence of PUD
may be due to decreased gastric acid secretion delayed emptying, increase in gastric mucus, and protection of mucosa by prostaglandins

Gastrointestinal - Small bowel
Reduced motility of small bowelincreased transit time in the third trimester and postpartum
Enhanced iron absorption as a response to increased iron needs

Gastrointestinal - Colon
Constipation Mechanical obstruction by the uterus Reduced motility (p4) Increased water absorption
Portal venous pressure is increased Dilation of gastroesophageal vessels
issue in those with preexisting esophageal varices Dilation of hemorrhoidal veins
hemorrhoids

Gastrointestinal - Gallbladder
Fasting and residual volumes double in 2nd and 3rd Δ Slower rate of emptying
Biliary cholesterol saturation increases and chenodeoxycholic acid decreases increased risk gallstone formation

Gastrointestinal - Liver Liver does not enlarge Hepatic blood flow remains unchanged
CO to the liver decreases by ~35% Spider angiomata and palmar erythema
elevated estrogen levels Lab data
Drop in serum albumin Rise in serum alkaline phosphatase
placental production and some hepatic production Rise in serum cholesterol, fibrinogen, ceruloplasmin,
binding proteins for corticosteroids, sex steroids, thyroid hormones, and vitamin D
No change in serum bilirubin, AST, ALT, protime and 5’ nucleotidase
Rise in GGT is controversial

Gastrointestinal system
NAUSEA AND VOMITING Morning sickness complicates 70% of
pregnancies Onset 4-8 weeks up to 14-16 weeks Cause?
Relaxation of smooth muscle of stomach, elevated levels of steroids and hCG
Rx – supportive: reassurance, support, and avoiding triggers…
HEG weight loss, ketonemia, electrolyte imbalance and
dehydration possible renal or hepatic damage IVF, antiemetics
NPO continue IV

Gastrointestinal change
Morning sickness
hyperremesis gravidarum (weight loss, ketonemia and electrolyte imbalance)
Dietary craving: pica
Decreased gastrointestinal motility: reflux and heartburn
Gallbladder function, cholestasis
Hyperemia and softening of the gums (epulis)
Hemorrhoid
Appendix displaced


Endocrine System
Estrogen Progesteron hCG

Function of hCG
Prevent involution of the corpus luteum at the end of the monthly female sexual
Instead, it causes the corpus luteum to secrete even larger quantities of its sex hormones—progesterone and estrogens—for the next few months.
These sex hormones prevent menstruation and cause the endometrium to continue to grow and store large amounts of nutrients.
Human chorionic gonadotropin also exerts an interstitial cell–stimulating effect on the testes of the male fetus, resulting in the production of testosterone

Function of Estrogen
Enlargement of the mother’s uterus Enlargement of the mother’s breasts and growth of
the breast ductal structure Enlargement of the mother’s female external
genitalia. Relax the pelvic ligaments of the mother, so that
the sacroiliac joints become relatively limber and the symphysis pubis becomes Elastic allow easier passage of the fetus through the birth canal.
Affect many general aspects of fetal development during pregnancy, for example, by affecting the rate of cell reproduction in the early embryo.

Functions of Progesteron
Causes decidual cells to develop in the uterine endometrium.
Decreases the contractility of the pregnant uterus preventing uterine Contractions.
Increases the secretions of the mother’s fallopian tubes and uterus to provide appropriate nutritive matter for the developing morula and blastocyst.
Helps the estrogen prepare the mother’s breasts for lactation.

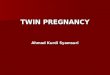
Rates of secretion of estrogens and progesterone, and concentration of human chorionic gonadotropin at
different stages of pregnancy.

Endocrine - Thyroid The normal pregnant woman is euthyroid Changes in thyroid morphology and lab indices
Estrogen-induced increase in TBG Decreased circulating extrathyroidal iodide Thyroid enlargement usually not detected by exam Normal thyroidal uptake of iodide
Serum TSH decreases early in gestation rises to pre-pregnancy levels by end of first Δ
T4 increases early in gestation role of hCG stimulating the thyroid
Rise in TBG leads to rise in total T4 and total T3 active hormones free T4 and free T3 are unchanged
Free T4 is the most reliable method of evaluating thyroid function in pregnancy

Endocrine - Adrenal glands
Expansion of the zona fasciculata site of glucocorticoid production
Plasma corticosteroid-binding globulin (CBG) rises due to enhanced liver synthesis
Free plasma cortisol rises increased production and delayed clearance
Plasma DOC (deoxycorticosterone) rises fetoplacental unit
DHEAS (dehydroepiandrosterone) decreases
Testosterone is slightly elevated Increased SHBG and androstenedione

Endocrine - Pancreas Hypertrophy and hyperplasia of the B cells Fasting associated with accelerated starvation
maternal hypoglycemia, hypoinsulinemia and hyperketonemia
due to diffusion of glucose by the fetoplacental unit Feeding response
hyperglycemia, hyperinsulinemia, hypertriglyceridemia and reduced tissue sensitivity to insulin
glucose response greater during pregnancy peripheral resistance to insulin: diabetogenic effect
of pregnancy. hPL and cortisol mediated greater insulin resistance as the pregnancy advances

Endocrine - Pancreas
Fetus primarily depends on glucoseFacilitated diffusion
carrier-mediated but not energy dependent process
Active transport of amino acids to the fetus
Ketones diffuse freely across the placenta

Endocrine - Pituitary
The pituitary gland enlarges in pregnancy
proliferation of chromophobe cells on the anterior pituitary
stalk remains midline

Skeleton
Lordosis keep center of gravity over the legs back pain…
Relaxin relaxation of the pubic symphysis and
sacroiliac joints facilitates vaginal delivery but may lead to
discomfort Implications
unsteadiness of gait and trauma from falls

Skeleton
Total serum calcium declines throughout pregnancy until 34-36 weeks due to the fall in serum albumin
Serum ionized calcium is constant and unchanged “Physiologic hyperparathyroidism”
increased gut absorption decreased renal losses no bone loss seen in bone density studies
preservation due to calcitonin? Rate of bone turnover and remodeling
increases throughout pregnancy twice as great at term

Metabolism
Basal metabolism rate, BMR : +15-20% Weight gain : 12.5 kg (± 24 pons)
o Fetus : 3400 go Placenta : 650 go Amniotic : 800 go Uterus : 960 go Plasma, red cells : 1450 go Mammary glands : 405 go Extracellular, extravascular water : 1480 go Deposition of fat and protein : 3345 g
Insulin resistance


Conclusion
Understanding maternal physiology is crucial in understanding the changes and clinical scenarios associated in pregnancy
This knowledge will help us distinguish the physiologic and pathologic processes during pregnancy
This knowledge will also improve patient’s education about their pregnancy

Selamat Belajar