-
8/13/2019 0.Trauma Kepala
1/25
HEAD TRAUMA
Oleh :Litany alamudi
Pembimbing :Dr. Jovizal,Sp.S
-
8/13/2019 0.Trauma Kepala
2/25
-
8/13/2019 0.Trauma Kepala
3/25
Layers of the Cranial Vault
Anatomy of the
Brainwww.neurosurgery.org/pubpgages/patres/anatofbrain.html#micro
-
8/13/2019 0.Trauma Kepala
4/25
Definition Traumatic Brain Injury
Traumatic brain injury (TBI) is a seriousneurodisorder commonly
caused by car accidents,
sports related events or violence
Review molecular mechanisms in the pathogenesis of traumatic
brain injuryhttp://www.hh.um.es
-
8/13/2019 0.Trauma Kepala
5/25
Mechanisms of Injury for TBI
-
8/13/2019 0.Trauma Kepala
6/25
Traumatic Brain Injury
Primary Brain Injury
Results from what hasoccurred to the brain at
the time of the injury
Secondary Brain Injury
Physiologic andbiochemical events which
follow the primary injury
World journal of emergency surgerymolecular mechanisms of
traumatic brain injury:the missing link in management
-
8/13/2019 0.Trauma Kepala
7/25
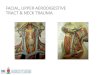
Traumatic Head Injury
www.med.ub.es/All-Net/english/neuropage/trauma/head-8htm
-
8/13/2019 0.Trauma Kepala
8/25
HEAD INJURIES / BRAIN INJURIES
Skull fractureDiffuse Axonal InjuryEpidural HematomaSubdural
Hematoma
Coup contussionContracoup contussion
World journal of emergency surgerymolecular mechanisms of
traumatic brain injury:the missing link in management
-
8/13/2019 0.Trauma Kepala
9/25
EPIDURALANDSUBDURALHEMATOMA
www.med.ub.es/All-Net/english/neuropage/trauma/head-8htm
-
8/13/2019 0.Trauma Kepala
10/25
SUBDURALHEMATOMA
C d C
-
8/13/2019 0.Trauma Kepala
11/25
Coup and ContracoupContusions
A combination of vascular and tissue damage leadsto cerebral
contusion
Coup contusions occur at the area of direct impact
to the skull and occur because of the creation ofnegative
pressure.
Contracoup contusions are similar to coupcontusions but are
located opposite the site of
direct impact
World journal of emergency surgerymolecular mechanisms of
traumatic brain injury:the missing link in management
-
8/13/2019 0.Trauma Kepala
12/25
-
8/13/2019 0.Trauma Kepala
13/25
ASSESSMENT
Note: Monitorsecure airway and protect c-spine
Assess breathing
Assess circulation Control major bleeding
Prevent hypotension
Transport decision and interventions
GCS
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
14/25
ASSESSMENT DETAILEDEXAM
Vital signs SAMPLE history Head-to-toe exam, including
neurological
and GCS, fluid Continuous observation
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
15/25
Management ofTraumatic Head Injury
Maximize oxygenation and ventilation
Support circulation / maximize cerebral
perfusion pressure
Decrease intracranial pressure
Decrease cerebral metabolic rate
Guidelines for the management of severe traumatic brain injury
3rd edition
P i S d
-
8/13/2019 0.Trauma Kepala
16/25
Primary vs. SecondaryBrain Injury
Primary injury is immediate from bruising orpenetrating
objects
Secondary injury is from hypoxia orperfusion of the brain Caused
by swelling, hypoxia, or hypotension Hyperventilation decreases
perfusion of the brain
tissueProtect airway, give oxygen, maintain BP
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
17/25
Intracranial Pressure (ICP)
ICP is usually low (15mmhg was one of five
independent risk factors associated with death.
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
18/25
Lowering ICP
Evacuate hematoma Drain CSF Intraventricular catheters use is
limited by degree of
edema
Craniotomy Permanence, risk of infection, questionable
benefit
Reduce edema Promote venous return Reduce cerebral metabolic
rate Reduce activity associated with elevated ICP
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
19/25
Diuretic Therapy
Osmotic Diuretic Mannitol (0.25-1 gm / kg) Increases osmolarity
Vasoconstriction
(adenosine)
Loop Diuretic Furosemide Decreased CSF formation Decreased
systemic and
cerebral blood volume(impairs sodium and water
movement across blood brainbarrier)
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
20/25
Hypertonic Fluid Administration
Hypertonic saline Comparing mannitol with barbiturates for
controlICP after TBI
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
21/25
Anesthetics, Analgetic and sedatives
High dose barbiturate therapy can result in control ofICP when
all others medical and surgical treatmentshave failed.
Anticonvulsants - Prevent seizure activity
PentobarbitalAdverse effects include hypotension and bone
marrow dysfunction
Used only after unsuccessful attempts to control
ICP and maximize CPP with other therapies
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
22/25
Dose regimens
-
8/13/2019 0.Trauma Kepala
23/25
Factors that Effect Secondary BrainInjuries
Blood PressureOxygenationTemperature
Control of Blood GlucoseFluid Volume Status Increased
Intracranial Pressure
Guidelines for the management of severe traumatic brain injury
3rd edition
-
8/13/2019 0.Trauma Kepala
24/25
References
Dr. Baxter Larmon, Director of the UCLA CPCand Professor of
Medicine, UCLA School ofMedicine
UCLA EMT Lectures, Barry Jensen and EMTTeam, 2003
Brady / DOT paramedic lectures and curriculum
www.emedicine.com
-
8/13/2019 0.Trauma Kepala
25/25
Evidence SupportingNormoventilation
Forbes et al. (1998) Journal of Neurosurgery, 88(3)
Marion et al. (1995) New Horizons, 3(3)
McLaughlin & Marion (1996) Journal of Neurosurgery, 85(5
Muizelaar et al. (1991) Journal of Neurosurgery, 75(5)
Newell et al. (1996) Neurosurgery, 39(1)
Skippen et al. (1997) Critical Care Medicine, 25(8)
Yundt & Diringer (1997) Critical Care Clinics, 13(1)