Embed Size (px)
Citation preview

Schizophrenia & Related Psychotic
DisordersAssessment; Differential Diagnosis;
Comorbidity
Heather I. Milliken, MDCM; FRCPC; CSPQ
Associate Professor, Department of Psychiatry, Dalhousie University
Psychiatrist, Nova Scotia Early Psychosis Program
Chair, Canadian Psychiatric Association
Continuing Professional Development Committee

Disclosure: Funding Support
(Past 2 Years)
• Clinical trials
• Janssen; Lundbeck; Otsuka
• Advisory boards:
• Janssen; Lundbeck; Otsuka;
• CME honoraria:
• Janssen

Learning Objectives
At the end of this presentation participants will be able to:
1. Describe the Canadian Schizophrenia Guidelines (2017)
2. Discuss the differential diagnosis for psychotic disorders
3. Describe the signs and symptoms of schizophrenia
4. Discuss the issues related to comorbid substance use disorders and schizophrenia with a focus on the upcoming legalization of cannabis
5. Describe the management of comorbid substance use disorders and schizophrenia with a focus on smoking cessation

Schizophrenia & Related
Psychotic Disorders
Canadian Guidelines for the Assessment and Diagnosis of Patients with Schizophrenia
Spectrum and Other Psychotic Disorders
Canadian Journal of Psychiatry, Volume 62, Number 9, September 2017, 594 - 603

Canadian Guidelines: Development
• Goal: To provide evidence-based recommendations for the
assessment and treatment of schizophrenia and schizophrenia
spectrum disorders for use by mental health care professionals
• 9 working groups (child & adolescent and adult psychiatrists
specializing in schizophrenia & related psychotic disorders; general
psychiatrists; family physician; pharmacist; evidence based
medicine methodologist; 4 individuals with lived experience with
schizophrenia; Schizophrenia Society of Canada representative)
• Used the ADAPTE process
– Systematic approach using existing guidelines
– 6 relevant guidelines identified; modified to suit Canadian context
– Recommendations based on level of evidence :1++; High quality meta-
analyses; systematic reviews of RCTS; 2++; High quality systematic
reviews of case control or cohort studies; 3; Nonanalytic studies (case
reports; case series); 4; Expert opinion
– Graded based on level of evidence (A, B, C, D, De Novo)

Canadian Guidelines: Development
• Recommendations finalized at in-person
consensus meeting attended by members of
all working groups
• Recommendations launched at CPA 67th
Annual Conference, Ottawa, September
14th-16th 2017
• Recommendations published Canadian
Journal of Psychiatry, Volume 62, Number 9,
September 2017, 594 - 603

Schizophrenia & Related Psychotic
DisordersTerminology & Phases of Illness

Terminology
• Psychosis– Term which is used to refer to disorders in which there is a
loss of contact with reality
– Psychosis affects the ability to think, feel, perceive and act
• “Prodromal Psychosis”
– Onset of non-specific signs and symptoms (sub-threshold
symptoms) but before the onset of clearly identifiable
psychotic signs and symptoms.
– Historically has been a retrospective diagnosis made at
time of presentation with first episode psychosis
– 80-90% of individuals with schizophrenia retrospectively
report a prodromal period

Terminology
• First episode psychosis
– Refers to the initial diagnosis of a psychotic disorder in an individual’s lifetime
• Early psychosis
– Refers to early course of illness after initial diagnosis
• “Critical period”
– 1st 5 years after onset of illness

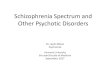
Pre-morbid
Phase
At risk/
Prodromal
Phase
Duration
of Untreated
PsychosisStable Phase
Diagnosis
Treatment
of First/Acute
Episode
Onset
Psychotic
Symptoms
Functional
Decline/
Subthreshold
Symptoms
Stabilization
Phase
Optimize
Recovery
Relapse
Prevention

Schizophrenia & Related Psychotic
DisordersAssessment:
Is it “Prodromal Psychosis”?

Common Prodromal Symptoms
In descending order of frequency
• Reduced concentration, attention
• Reduced drive and motivation, anergia
• Depressed mood
• Sleep disturbance
• Anxiety
• Social withdrawal
• Deterioration of role functioning
• Irritability

Prodromal Symptoms
• Epidemiological evidence of continuum of psychotic symptoms in general population1
• Commonly seen in a number of different psychiatric disorders
• Do not have sufficient specificity or sensitivity to be used as signs of risk of initial onset of psychosis in general population (low predictive validity)2
1 van OJ, Linscott RJ, Myin-Germeys I et al Psychol Med 2009; 39(2): 179-195
2Malla AK, Norman RM. Br J Psychiatry 1994; 164: 487-93

Detection of “At Clinical High
Risk” Individuals• Recent focus on prospectively defining “at clinical high
risk” individuals
• Strategies combine prodromal symptoms with other risk
factors
– Family history
– Transient psychotic symptoms or schizotypal personality
traits
– Decline in functioning
• Measures and criteria have been developed that can
reliably detect “at clinical high risk” individuals
– 25-35% risk of developing diagnosable psychotic illness**Fusi-Poli P, Bonoldi I, Yung AR et al. Arcg Gen Psychiatry 2012;693):
220-229

Assessment: PRIME Screen
• For use with help-seeking individuals
• Easy to administer self-report questionnaire that
can be completed in waiting room prior to
interview
• 12 items rating experiences within the past year
from 0 (definitely disagree) to 6 (definitely agree)
• Purpose is identification of individuals for whom
a more through assessment is indicated
– Score of at least 5 on 3 items or 6 on 1 item

Within the past year Definitely
disagree
Somewhat
disagree
Slightly
disagree
Not sure Slightly
agree
Somewhat
agree
Definitely
agree
I think that I have felt that there are odd or
unusual things going on that I can’t explain. 0 1 2 3 4 5 6
I think that I might be able to predict the
future 0 1 2 3 4 5 6
I may have felt that there could possibly be
something interrupting or controlling my
thoughts, feelings, or actions.
0 1 2 3 4 5 6
I have had the experience of doing
something differently because of my
superstitions.
0 1 2 3 4 5 6
I think that I may get confused at times
whether something I experience or perceive
may be real or may be just part of my
imagination or dreams.
0 1 2 3 4 5 6
I have thought that it might be possible that
other people can read my mind, or that I
can read other’s minds
0 1 2 3 4 5 6
I wonder if people may be planning to hurt
me or even may be about to hurt me 0 1 2 3 4 5 6
I believe that I have special natural or
supernatural gifts beyond my talents and
natural strengths
0 1 2 3 4 5 6
I think I might feel like my mind is “playing
tricks” on me 0 1 2 3 4 5 6
I have had the experience of hearing faint or
clear sounds of people or a person
mumbling or speaking when there is no one
near me
0 1 2 3 4 5 6
I think that I may hear my own thoughts being
said out loud 0 1 2 3 4 5 6
I have been concerned that I might be “going
crazy” 0 1 2 3 4 5 6

Assessment
• Answers to PRIME screen useful to guide
questions to elicit nature, frequency and
severity of symptoms; course of illness;
impact on functioning; substance use;
psychiatric and physical comorbidity
• If suspect prodromal psychosis refer to
NSEPP (ages 19-35) or IWK Youth
Psychosis Program (ages 12- 18)

Canadian Guidelines:
“At Clinical High Risk”
• Recommendation 1: Modified from NICE
Strong)
– If a person is distressed; decline in functioning
and has
• Transient or attenuated psychotic symptoms or other
signs/symptoms suggestive of possible psychosis or
schizophrenia or
• First degree relative with psychosis or schizophrenia
or schizotypy
– Refer ASAP for comprehensive assessment to
specialized EPP program or mental health
service

Canadian Guidelines:
“At Clinical High Risk”
• Recommendation 2: (NICE Strong)
– A consultant psychiatrist or trained mental health
clinician with experience in “at clinical high risk
states” should carry out assessment
– Use of SIPS/SOPS or CAARMS
– Identify comorbid AXIS 1 conditions
• 73%
• Depression most common

Schizophrenia & Related Psychotic
DisordersAssessment:
First Episode Psychosis
Schizophrenia Spectrum Disorders

Canadian Guidelines: Assessment
• Recommendation 1: Assessment and Care
Planning (Level of evidence: C)
– Initial comprehensive multidisciplinary
assessment (including evaluation by a
psychiatrist)

Recommendation 1: Assessment and Care Planning
• Full mental status examination with particular
attention to symptoms of psychosis, negative
symptoms, general psychopathology, insight and
competence
• Risk of suicide and aggression
• Psychiatric history including prior diagnoses and
treatment; prior hospitalizations and emergency
room treatments

Recommendation 1: Assessment and Care Planning
• For patients with previous episodes review
and document
– All treatments provided:
• Types; doses
• Duration of treatment
• Response to treatment
• Adherence
• Outcomes (including quantitative measures if
possible)

Recommendation 1: Assessment and Care Planning
• History of substance use (tobacco; alcohol;
cannabis; hallucinogens; stimulants; opioids;
other)
• History of any neurodevelopmental or
psychosocial problems
• Current social and occupational (educational)
functioning
• Past and current physical health
– Accessibility to primary care

Recommendation 2: Assessment of First Episode Psychosis (De Novo Recommendation)
• See new patients within 2 weeks of referral
• Assessment as per recommendation 1 with
particular attention to:
– Onset of changes in behaviour and timing and
course of symptoms
– Relationship of substance use to onset of
symptoms
– Onset of decline in function (prognostic value)
– Duration of untreated psychosis (prognostic value)

Recommendation 3: Neuropsychological Assessment (De Novo Recommendation)
• Suggested in:
– First episode psychosis
– Poor response to treatment (treatment
resistance)
– Evidence of cognitive impairment
• MATRICS cognitive battery
• Interpretation of results optimally done by
neuropsychologist
• Predictor of functioning
• Focus of specific interventions

Recommendation 4: Brain Imaging (De Novo Recommendation)
• Not routinely recommended in first episode
psychosis
• Consider on case-by-case basis for first episode
and recurrent acute episodes
– History of signs and symptoms suggestive of
intracranial pathology
– History of head injury with loss of consciousness

Recommendation 5: Genetic Testing (De Novo Recommendation)
• Testing for 22q11.2 deletion syndrome if
characteristic features present

First Episode Psychosis
Differential Diagnosis

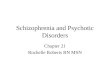
Types of psychotic disorders
PSYCHOSIS
DELUSIONS HALLUCINATIONS
ODD BEHAVIOUR
THOUGHT DISORDER
BRIEF PSYCHOSIS
SCHIZOPHRENIFORM
PSYCHOSIS
SCHIZOPHRENIAA
SCHIZO-
AFFECTIVE
DISORDER
BIPOLAR
DISORDER
PSYCHOTIC
DEPRESSION
SUBSTANCE
INDUCED
DUE TO A
MEDICAL
CONDITION
DELUSIONAL
DISORDER
PSYCHOSIS *NEC
*Psychosis NEC = Psychosis Not Elsewhere Classified

Differential Diagnosis: DSM 5Disorder Characteristics
Schizophrenia Meets Criteria A for symptoms; Signs of illness for ≥ 6 mo; Criteria A symptoms for ≥ 1 month; social/occupational dysfunction
Schizophreniform psychosis
Similar to schizophrenia except duration of illness of < 6 mo.
Schizoaffective disorder
Uninterrupted period of illness meeting Criteria A for Schizophrenia and criteria for Major Depression or Mania; Lifetime prevalence of > 2 wks. of Criteria A symptoms in absence of mood episode; Mood episode is present for > 50% of total duration of illness
Delusional disorder Delusions for > 1 mo and does not meet the criteria for schizophrenia2013-2014 31

Differential Diagnosis: DSM 5Disorder Characteristics
Brief psychotic disorder
Psychotic symptoms for > 1 day but < 1 mo; May or may not be related to stressor; full return to premorbid level of functioning
Substance-induced psychotic disorder
Delusions or hallucinations develop within 1 mo of substance intoxication or withdrawal; are etiologically related to substance use & are not better accounted for by another psychotic disorder
Psychotic disorder due to another medical condition
Delusions or hallucinations are direct physiologic consequence of another medical condition & develop in absence of delirium

Differential Diagnosis: DSM 5
Disorder Characteristics
Psychotic disorder not elsewhere classified
Psychotic symptoms present but criteria for specific disorder not met or there is insufficient or contradictory information
Major depression with psychotic features
Major depressive episode with mood congruent (most common) or mood incongruent psychotic symptoms
Bipolar disorder Manic episode with mood congruent (most common) or mood incongruent psychotic symptoms

Criteria A: Schizophrenia &
Schizophreniform Psychosis
• At least 2 of the following and at least 1 must
include 1-3:
1. Delusions
2. Hallucinations
3. Disorganized speech
4. Grossly abnormal psychomotor behaviour such
as catatonia
5. Negative symptoms

Signs and Symptoms of
Schizophrenia

1. Crow TJ. Br Med J 1980;280:66–8 2. Andreasen NC. Lancet 1995;346:477–8
It is now accepted
that psychosis
encompasses three
key domains of
disturbance1,2
Classification of Schizophrenia Symptoms
Negative
Positive
Cognitive

Positive Symptoms Include:
1. Hallucinations
2. Delusions
3. Thought Disorder
4. Disorganized or Bizarre behaviour

Positive Symptoms: Hallucinations
• Are sensory perceptions that occur in the absence of any real external stimulus
• Can affect any of the senses. The person may hear, see, smell, feel or taste sensations that are not there.
• The hallucinations are very real to the person and may be very distressing.

Positive Symptoms: Delusions
• Strongly held (fixed) false beliefs not shared by
other people
• Are believed to be very real even when the
person is told they are not.

Persecutory
Grandiose
Religious
Somatic
Delusions of
Reference
Delusions of
Control
Delusions

Positive Symptoms:
Thought Form Disorder
A person with psychosis:
• May think and communicate less logically.
• Have problems organizing their thoughts.
• May have thought that may be confused, sped up or slowed down.
• May have speech that reflects their thought process.
• May jump from one topic to the next.
• Stop in the middle of a sentence.
• Make up words.
• May simply be difficult to understand.

Positive Symptoms: Disorganized
or Bizarre Behaviour
People with psychosis may behave differently
than they usually do.
• May become extremely active or agitated, restless.
• May laugh inappropriately or display inappropriate
appearance, hygiene or conduct.
• May become guarded or untrusting (may stop eating
because of fear their food is poisoned).
• Hold body in strange postures or make odd gestures.

• Behaviours or experiences that have been
reduced or lost because of the illness. Problems getting motivated (avolition)
Problems taking pleasure in things (anhedonia)
Withdrawal from social relationships & activities
(asociality)
Problems getting words out (alogia)
Seeming flat and blunted
Negative Symptoms

• May be misinterpreted by caregivers as “laziness”
• May have greater effect on functioning than positive
symptoms
• More difficult to treat than positive symptoms & may
take longer to respond to treatment
• Have significant effect on caregivers Negative symptoms are one of the main predictors
of the level of burden and distress in a sample of 52 caregivers of
patients with schizophrenia1
More specifically, anhedonia/asociality and blunted affect were
strong predictors of burden in a sample
of 101 caregivers2
1.Dyck et al. Psychosomatic Medicine (1999).
2. Ukpong. Turk J Psychiatry (2012).
Negative Symptoms

Cognitive Symptoms
• Inability to focus and sustain attention. • Find it hard to filter out all the various stimuli in their
environment. (sounds, lights).
• Impaired concentration• Slower speed in focussing on & processing information and
then reacting
• Difficulty with memory especially remembering things they are told (verbal memory)
• Difficulty in organizing and planning activities (executive functions)
• For example to plan and manage the time and tasks of everyday life (i.e. schoolwork, money management).

Mood Symptoms
• Symptoms can include depersonalization; derealization; irritability; anger; anxiety; dysphoria & depression; suicidal ideation; excitement; mood swings
• Can occur at all phases of illness

Substance Use and Schizophrenia

Substance Use: Epidemiology
• ECA Study (Regier et al., 1990)– Lifetime prevalence of substance use
disorders in individuals with schizophrenia was 47% compared to 16.7% in general population
– Odds of having any substance use disorder 4.6 times greater in individuals with schizophrenia compared to general population
• National Comorbidity Study (Kessler et al. 1996)– 58% of persons with non-affective psychosis
had one or more lifetime substance use disorders

Substance Use: Epidemiology
• The most common concurrent disorder among
individuals with schizophrenia is a substance use
disorder (SUD)
• Inpatients range from 48 - 72% (lifetime)
– Cantwell et al, 1999 (inpatients, first episode)
• 37% lifetime diagnosis of a SUD
• Outpatients range from 32 - 60% (lifetime)
– Fowler et al, 1998 (outpatients)
• 59.8% lifetime diagnosis of SUD
• Highest rates found in services attending to less
stable, more severe cases (ER; walk-in clinics)

Substance Use: Epidemiology
• Prevalence rates in large epidemiological studies
(excluding nicotine and caffeine)
– 44.8% - 47%
• Cigarette smoking reported in 60% - 90%
– Rates declining
• Alcohol and cannabis most frequently used
substances (excluding nicotine and caffeine)
• Substance use is risk factor for developing
psychosis
– Met-analysis: Persons who used cannabis
developed psychosis 2.7 years earlier
• Negative impact on course and outcome

Schizophrenia & Substance Use Disorders
• Binge rather than regular use
– i.e. polymorphous, chaotic, opportunistic use
• Use is highly sensitive to environmental prompting
• Dependence more likely with the more accessible
drugs (nicotine, alcohol, cannabis, Rx drugs)
• Specific vulnerability for DA-agonist substances
(nicotine, cocaine)
– augment positive symptoms
– reduce negative symptoms
– counteract DA-blockade of antipsychotics

Substance Use and First Episode Psychosis
• Substance use is very common in first episode psychosis
• Lifetime use rates of up to 70%1
• Rates of substance use in first episode psychosis are higher than in the age comparable general population2
• Alcohol, cannabinoids and tobacco are the most commonly used substances
1. Power et al; Br J Psychiat 1998: 172:Suppl 33, 71-76
2. Van Mastrigt et al; Soc Psych Psych Epid 2004; 39:69-72

Substance Abuse and
First Episode Psychosis
• Substance abuse disorders are also very common in first episode psychosis patients
• Rates of substance abuse disorders in 203 consecutive admissions to the Calgary early psychosis program:*
– Any substance use disorder: 51%
– Alcohol use disorder: 35%
– Cannabis use disorder: 33%
*Addington J, Addington D; Acta Psychiat Scand 2007; 15(4):304-309

Cannabis
• Medical marijuana
– “Cure-all”?
• Upcoming legalization
– Harmless or harmful?
• Risk factor for schizophrenia

Cannabis: Rates of UseCanadian Alcohol & Drug Use Monitoring Survey
2012
– Rates of cannabis abuse/dependence exceeded rates of all
othersubstance abuse/dependence combined (6.8% vs. 4.0%)
55
All
Canadians
Youth
(15-24)
Adults
(25+)
Lifetime 41.5% 34.8% 42.8%
Past Year 10.2% 20.3% 8.4%
Age at
initiation
18.6 16.1 19

Cannabis Use
Canadian Alcohol & Drug Use Monitoring Survey
2012
• Increase in prevalence of cannabis use in
Canada over past 2 decades
– ~ 34% of Canadians (12 million) have used
cannabis in their lifetime
• Rates of cannabis abuse/dependence
exceed rates of all other substance
abuse/dependence combined
• 6.8% vs. 4.0%

Cannabis UseCanadian Alcohol & Drug Use Monitoring Survey
2012
• In Canada 12 month prevalence rate of cannabis use in youth (ages 11 – 15) is highest out of 29 countries1
• Canada: 28%; US: 23% (recreational use legal in Alaska, Colorado, Oregon, Washington, Washington DC); Netherlands: 17%
• 5% of all Canadian adolescents and 10% of Grade 12 students use pot daily
• Younger users (< age 16) smoke more often (~25 times/wk. & smoke more (~15 grams/wk)2
1United Nations Childrens’ Fund Study 20132Psychology of Addictive Behaviors 2012

Cannabis: Chemical Constituents
• 4 main cannabinoids in cannabis
– Delta-9 THC; Cannabidiol (CBD); Cannabinol
(CBN); Delta-8 THC
• Delta-9 THC
– Psychoactive constituent
• “Positive” effects: Euphoria
• Negative effects: Anxiety; panic attacks; paranoia;
acute psychosis
– Potency ↑ from 4.56% 1996 to 11.75% in 2008 (Burdoff et al; 2011)
– Constituted 1% of cannabis in 1960’s vs. 10-30%
today (Health Canada 2014)58

Shatter
• Very potent type of cannabis
• Concentration of THC ~ 80%

Synthetic Cannabinoids
• JWH-0184
– Analgesic compound acts on cannabinoid
receptors
– Effects similar to THC
– Component of various “street drugs” e.g.
“Spice”, “Kronic”, “Incense”
– Can cause psychosis
60

Cannabis: Effect on the Brain
• Cannabis acts on cannabinoid 1 and cannabinoid 2
endogenous brain receptors
• Receptors are widespread in both grey and white matter
– Involved in memory, mood and reward processing
• Endogenous cannabinoid system is still developing
during adolescence
– ↑ sensitivity to effects of cannabis on brain
development
• Effects on cortical development; neural migration;
connectivity; synaptogenesis; white matter development
(brain circuitry)
• Effects on dopamine

Cannabis: Effect on the Brain
• Effects peak at onset of adolescence decreasing
during adulthood
• Neuroimaging and neuropsychological studies have
demonstrated adverse effects of initiation of regular
cannabis use in adolescence
• Evidence of structural and functional brain
abnormalities (Psychopharmacology, 2013; Journal of Neuroscience
2014)
– Cognitive effects (↓ in IQ)
– ↑ risk with earlier age of use (<16 y.o.)

Cannabis: Effects
• Cannabis use disorders
– Addiction
• Cannabis induced psychosis
– Delusions or hallucinations develop within 1 mo. of substance intoxication or withdrawal
– Etiologically related to substance use
• ↑ risk for schizophrenia

Cannabis Use and Risk of Psychosis:
A Systematic Review*
• Included 35 longitudinal population based studies in meta-analysis
• Concluded that:
– Cannabis use increases the relative risk for psychotic disorders by 1.4
– Is a dose-response effect with an increased risk of 50-200% in the most frequent users
– In UK ~14% of psychotic disorders in young adults could be avoided if cannabis was never consumed
*Moore et al; Lancet 2007; 370:319-328

Cannabis Use and Risk of Psychosis
• Study* reviewed the evidence of cannabis as
a causal risk factor for psychosis
• Concluded that:
– Cannabis use in adolescence leads to a 2-3 X
increase in the relative risk for SZ in adulthood
– Cannabis use is not necessary nor sufficient
cause, but forms part of a causal constellation
– ~8% of schizophrenia could be avoided with the
elimination of cannabis use in the population
*Arseneault et al; Br J Psychiat 2004; 184:110-117

Cannabis Use and Risk of Psychosis
• Swedish longitudinal study
• Higher frequency of cannabis use associated
with increased risk of psychosis
• Risk increased 6 fold in heavy users
compared to non-users
– Heavy use defined as greater than 50
occasions by age 18

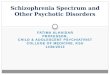
Cannabis Use and Risk of Psychosis
• Genetic vulnerability
• 3 polymorphisms for COMT gene
– Val/Val, Val/Met, Met/Met
• Individuals homozygous for wild type Val158
polymorphism vs. Met158 have higher activity enzyme resulting in faster dopamine breakdown (thus lower sustained prefrontal cortical synaptic levels of dopamine)

Gene Polymorphism and Cannabis Use:
Risk of Schizophreniform Psychosis
Adapted from Caspi et al, Biol Psychiatry 57:1117-27, 2005
0
2
4
6
8
10
12
14
met/met met/val val/valno yes no yes no yes Adolescent cannabis use
Genotype
Perc
ent
with D
isord
er

Legalization of Cannabis in Canada
Impact?

Cannabis Legalization:
March 19 2018
• The Trudeau government's proposals include:
– Restrictions on the colour of packaging and the depiction of branding
– Requirements for mandatory warning labels
– Ban on packaging designed to appeal to young people.
• Mandatory warning labels
– Require producers to include one of 14 mandatory health warnings on each package.
– Producers and/or cultivators would be required to make sure all messages appear on their products by rotating the various warnings "on each package of each brand name with equal frequency in a calendar year."

Cannabis Legalization:
Warning Labels: March 19 2018

Cannabis Legalization:
March 19 2018

XXIX W.O. MCCORMICK
ACADEMIC DAY CONFERENCE
Psychiatric Aspects of Cannabis
Friday, April 27, 2018
Marriott Halifax Harbourfront
www.psych.dal.ca

Canadian Schizophrenia Guidelines:Schizophrenia and Other Psychotic
Disorders with Coexisting Substance Use Disorders
David Crockford MD, FRCPC & Donald Addington MD
Canadian Journal of Psychiatry, Volume 62, Number 9, September 2017, 624 - 634

Canadian Guidelines:
Substance Use Disorders
• 43 recommendations
• Recommendation 1: (NICE STRONG)
– Importance of engagement
– Direct, nonjudgmental approach
– Motivational interviewing techniques
– Awareness of likelihood of denial of psychosis,
substance use or both
• Stigma

Canadian Guidelines:
Substance Use Disorders• Recommendation 9:
– Adults and young people with psychosis and coexisting
substance use should not be excluded from age appropriate
mental health care because of substance use disorder
• Recommendation 10:
– Adults and young people with psychosis and coexisting
substance use should not be excluded from age appropriate
substance use services because of psychosis
• Recommendation 11: (Modified from NICE STRONG)
– For most adults and young people with psychosis and
substance use disorder treatment for both conditions
should be provided by mental health care professionals

Canadian Guidelines:
Tobacco Use Disorders• Recommendation 21: (NICE STRONG)
– Offer help to stop smoking even if previous attempts have
been unsuccessful
– Be aware of potentially significant effect of reducing cigarette
smoking on metabolism of other drugs (olanzapine;
clozapine)
• Recommendation 22: Smoking cessation strategies
(NICE STRONG)
– Nicotine replacement therapies (psychosis or schizophrenia)
– Buproprion (schizophrenia)
– Varenicline (psychosis or schizophrenia)
– Increased risk of neuropsychiatric symptoms with buproprion
and varenicline esp. in 1st 2-3 wks.
• Need to warn patients and monitor closely

Canadian Guidelines:
Smoking Cessation Strategies• Strong evidence to support benefits of smoking cessation
strategies in schizophrenia1
• Most effective when patients stable and motivated
– Precontemplative or contemplative: Motivational interviewing
– Preparatory or action stages: Psychosocial counseling;
Pharmacologic treatments
• NRTs well tolerated but limited evidence of benefit1, 2
• Buproprion:
– Most evidence for benefit in schizophrenia1,2
– Monitor for sleep impairment, suicidality and reemergence of
psychosis
• 1 TsoiDT, Porwai M, Webster AC Cochrane Databse Syst. Rev.
2013;(2):CDOO7253
• 2 Tidley JW, Miller ME BMJ. 2015;351: h4065

Canadian Guidelines:
Smoking Cessation Strategies• Varenicline
– Greatest efficacy in individuals without schizophrenia
– Recommended as second-line to buproprion in
schizophrenia1,2
– Limited evidence of increased risk of suicidality or
reemergence of psychotic symptoms but need to monitor
closely3
• 1 TsoiDT, Porwai M, Webster AC Cochrane Databse Syst. Rev.
2013;(2):CDOO7253
• 2 Tidley JW, Miller ME BMJ. 2015;351: h4065
• 3 Thomas KH, Martin RM, Knipe DW et al. BMJ 2015;350:h1109

Resources
• PDF copy of today’s slides:
– http://cme.medicine.dal.ca/chp.htm
– Will be available for one month
• Canadian Schizophrenia Guidelines
– The Canadian Journal of Psychiatry September 2017, Volume 62, Number 9
– http://journals.sagepub.com/toc/cpab/62/9
• Milliken H.I. “Psychoses” in Compendium of Therapeutic Choices 2017 Edition
– https://www.pharmacists.ca/products-services/therapeutic-choices/

Suggested Future Topics
• “Management of Schizophrenia with Comorbid Physical Health Conditions”
• “Antipsychotic Polypharmacy: What Are We Treating?”





![Studying Psychological Disorders - … Psychological Disorders: ... Schizophrenia (group of psychotic disorders) ... disorders.ppt [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/5afbf38c7f8b9a444f8b7406/studying-psychological-disorders-psychological-disorders-schizophrenia.jpg)