Embed Size (px)
Citation preview

Pearls amp Oy-stersThe medial longitudinal fasciculus inocular motor physiology
TC Frohman BAS Galetta MDR Fox MDD Solomon MD PhDD Straumann MDM Filippi MDD Zee MDEM Frohman MDPhD
ABSTRACT
Objective To review the role played by the medial longitudinal fasciculus (MLF) in ocular motorphysiology and to characterize a number of syndromes that result from lesions in this eloquentbrainstem tract system
Background The MLF is responsible for transmitting information that is crucial for the coordina-tion and synchronization of all major classes of eye movements A number of disease processescan produce lesions within this small yet highly strategic white matter pathway resulting in amyriad of neuro-ophthalmologic signs and symptoms
Methods We carefully reviewed both the literature and our collective experiences to systemati-cally consider the neuroanatomy and physiology of the MLF and the pathophysiologic mecha-nisms that underlie syndromes deriving from lesions in this pathway
Results The MLF is an important structure and is composed of numerous projection systemsinvolved in the regulation of eye movements Pathology at this location can produce a constella-tion of abnormalities many of which can be identified upon careful bedside neurologic examina-tion
Conclusion This review of the medial longitudinal fasciculus and its constituent path-ways is germane to understanding a number of important principles in neuro-ophthal-mology Neurologyreg 200870e57ndashe67
GLOSSARYFEF frontal eye field FPA first-pass amplitude INC interstitial nucleus of Cajal INO internuclear ophthalmoparesisMLF medial longitudinal fasciculus MS multiple sclerosis NPH nucleus prepositus hypoglossi NRTP nucleus reticu-laris tegmenti pontis OD right eye OS left eye OTR ocular tilt reaction PPRF paramedian pontine reticular forma-tion PSP progressive supranuclear palsy r-VOR rotational vestibular ocular reflex riMLF rostral interstitial nucleus ofthe MLF SC superior colliculus SVN superior vestibular nucleus VDI versional disconjugacy index VLVN ventrallateral vestibular nucleus
The medial longitudinal fasciculus (MLF) is organized as a pair of white matter fiber tracts that extendthrough the brainstem and lie near the midline just ventral to the fourth ventricle (in the medulla andpons) and cerebral aqueduct (in the midbrain) The MLF contains fibers that ascend and some thatdescend within the brainstem tegmentum and interact with ocular motor control circuitries involved inthe coordination of horizontal vertical and torsional eye movements12
TheMLF is a central conduit for many brainstem pathways and is the final common pathway for allclasses of conjugate eye movements including saccades (rapid refixations) smooth pursuit and ves-tibuloocular reflexes including semicircular and otolith mediated ocular motor reflexes The six ocu-
From the Departments of Neurology (TCF EMF) and Ophthalmology (EMF) University of Texas Southwestern Medical Center atDallas Department of Neurology University of Pennsylvania (SG) Philadelphia Mellen Center for Multiple Sclerosis (RF) Departmentof Neurology Cleveland Clinic OH Department of Neurology (D Solomon DZ) The Johns Hopkins Hospital Baltimore MDDepartment of Neurology (D Straumann) Zurich University Hospital Switzerland and Department of Neurology (MF) ScientificInstitute Neuroimaging Research Unit University Ospedale San Raffaele Milan Italy
Supported by the National Multiple Sclerosis Society (Lone Star Chapter) the ldquoOnce Upon A Timerdquo the CainDenius Comprehensive Centerfor Mobility Research the Irene Wadel and Robert Atha fund the Kenney Marie Dixon Pickens fund and the Jean Ann and Steve BrockFund for Medical Sciences
Disclosure Teresa Frohman has no conflicts to declare Steven Galetta has received lecture fees from Biogen Idec Dr Fox has received grantor research support from Biogen Idec Genentech Merck National Institutes of Health and National MS Society Bob Fox has served as aconsultant for Biogen Idec Genentech Merck Questcor and Teva Neuroscience David Solomon has no conflicts to declare DominikStraumann has no conflicts to declare Massimo Filippi has received grantscontracts and honorariaconsultation fees from TEVANeuroscience Dompe Biogen Bayer-Shering and Merck-Serono David Zee has no conflicts to declare Elliot Frohman has received lecturefees from Biogen Idec TEVA and Serono and consulting fees from Biogen Idec
Address correspondence andreprint requests to Dr Elliot MFrohman Department ofNeurology University of TexasSouthwestern Medical Center atDallas 5323 Harry Hines BlvdDallas TX 75235elliotfrohmanutsouthwesternedu
RESIDENTamp FELLOWSECTION
Section EditorMitchell SV ElkindMD MS
Copyright copy 2008 by AAN Enterprises Inc e57
lar motor nuclei (pairs of cranial nerve III IV VI)are interconnected via the MLF which transmitsvital information for the purpose of coordinatedand synchronized movements of the eyes to a vi-sual target Within this system are both excitatoryas well as reciprocal inhibitory projections thatserve to precisely regulate the interplay betweenagonist and antagonist muscles of the eyes
In this review we characterize the physiologyof the component tract systems contained withinthis central ocular motor circuitry and provide adetailed discussion of the most common neuro-logic signs and symptoms associated with lesionsof this structure
MLF CIRCUITRY OF SACCADIC EYE MOVE-MENTS The saccadic apparatus includes neuronsin the frontal eye field (FEF) which project to anumber of subcortical structures that serve to me-diate rapid gaze shifts to remembered targets3
The FEF sends a signal to the ipsilateral superiorcolliculus (SC) and to the contralateral paramed-ian pontine reticular formation (PPRF) for hori-zontal saccades and to the rostral interstitialnucleus of the MLF (riMLF) for vertical saccadesThe PPRF contains excitatory burst neurons thatproduce the supranuclear horizontal saccadic eyevelocity command sequence (the pulse)4 Theseneurons project to the adjacent VI (abducens)nerve nucleus The abducens nucleus consists oftwo types of neurons that mediate conjugate hor-izontal eye movements Abducens motoneuronsinnervate the ipsilateral lateral rectus musclewhereas axons from abducens interneurons crossto the contralateral pons and ascend via the MLFto innervate the medial rectus subnucleus of cra-nial nerve III which ultimately projects to the me-dial rectus muscle (figure 1) The parietal cortex iscentral in the production of smooth pursuit eyemovements but also participates in the produc-tion of saccades and has a direct projection to theSC In contrast to the FEF the parietal cortex ismore involved in the production of saccades tonovel visual stimuli rather than to rememberedtargets3 As with saccades smooth pursuit path-ways ultimately converge upon the MLF for theexecution of both horizontal and vertical eyemovements
VESTIBULAR COMPONENTS OF THE MLF Ca-nal system afferents The MLF is the principaltract system by which signals reach the ocularmotoneurons for eye movements generated inresponse to vestibular stimuli3 There may how-ever be differences in the anatomic circuitry un-derlying these reflexes depending upon whether
the eye movements are compensatory for angularmotion of the head mediated by the semicircularcanals (called the rotational vestibular ocular re-flex r-VOR) or for linear acceleration of thehead mediated by the otolith organs (utriculusand sacculus)
Lateral semicircular canal projections in the MLFThe pathways underlying the angular VOR arereasonably well understood For the lateral canalsystem the r-VOR is mediated by the same path-way carrying information for the other conjugateeye movement systems (saccade and pursuit) Theabducens nucleus is the gaze center for the finalpathway of horizontal eye movements Stimula-tion of the lateral semicircular canal results intransmission of information (from horizontalhead motion or caloric activation) within the ipsi-lateral VIII nerve and nucleus5 Projections thenemanate from the medial vestibular nucleus to in-nervate the contralateral VI nucleus Abducens
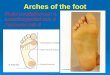
Figure 1 Details of the descending projectioninvolved in the volitional control ofhorizontal saccadic eye movements
Excitatory pathways are shown in orange and the reciprocalinhibitory pathways are shown in blue The particular path-way shown emanates from the frontal eye field (FEF) whichprojects through the anterior limb of the internal capsule de-cussates to the opposite side at the midbrain-pontine junc-tion and then innervates the paramedian pontine reticularformation (PPRF) From there projections directly innervatethe lateral rectus (ipsilateral to the PPRF) A second decussa-tion back to the side of origin of FEF activation via the MLFinnervates the medial rectus subnucleus of cranial nerve IIIand then neurons here project to innervate the medial rectusmuscle The right FEF command to trigger a saccade culmi-nates in conjugate eye movements to the left According toHerringrsquos law the horizontal yoke pair the medial and lateralrecti are activated in synchrony
e58 Neurology 70 April 22 2008
motoneurons then project to the lateral rectusmuscle while abducens interneurons project intothe contralateral MLF where their axons inner-vate the medical rectus subnucleus of the ocularmotor nucleus with a final projection to the me-dial rectus muscle (figure 2)
Anterior semicircular canal projections in the MLFFor the anterior canal system there may be threeexcitatory pathways by which information is car-ried rostrally for the vertical r-VOR Excitatorycells in the medial vestibular nucleus or adjacentventral lateral vestibular nucleus (VLVN) projectmedially and dorsally crossing the midline cau-dally5 After crossing they ascend in or just belowthe MLF to contact the superior rectus and infe-rior oblique subdivisions of the oculomotor com-plex Importantly the superior rectus subnucleussends fibers that decussate to innervate the supe-rior rectus muscle on the side of anterior canalactivation (figure 3) In this way one semicircularcanal can innervate muscles in both eyes for ap-propriate yoking of eye movements Inhibitory
neurons for the anterior canal system lie in thesuperior vestibular nucleus (SVN) Their axonsexit from the rostromedial aspect of this nucleusand course medially and rostrally in the lateralwing of the ipsilateral MLF to contact superioroblique motoneurons in the trochlear nucleusand inferior rectus neurons in the oculomotor nu-cleus to antagonize those eye movements medi-ated by an activated anterior canal system3
Another cell group that may contribute excita-tory inputs from the anterior canal system lies inthe SVN Their axons cross the midline in theventral tegmental tract close to the medial lem-niscus at the rostral pole of the nucleus reticularistegmenti pontis (NRTP) and then abruptly turnrostrally passing through the decussation of thesuperior cerebellar peduncle to terminate mainlyon the superior rectus and inferior oblique subdi-visions of the oculomotor complex3 Also insome species (perhaps also in humans) the SVNprojects rostrally just near the brachium conjunc-
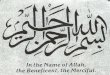
Figure 2 Projections involved in the activationof the left lateral semicircular canal
This figure illustrates the projections involved during the ac-tivation of the left lateral semicircular canal For instanceduring a leftward rotation of the head while attempting tomaintain straight ahead gaze axons from left lateral canal(on the right side of the figure) canal neurons project to ipsi-lateral vestibular nucleus (primarily the medial) which thenprojects across the brainstem to innervate the opposite rightabducens (VI) nucleus This nucleus has two populations ofneurons a direct projection to the same side lateral rectus(right) and an interneuronal projection that crosses back tothe left side via the MLF and then innervates the medial rec-tus subnucleus of cranial nerve III which ultimately inner-vates the left medial rectus muscle
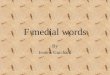
Figure 3 Projections involved in the activationof the left anterior canal
Axons from anterior semicircular canal neurons project tothe ipsilateral vestibular nucleus and from there decussateacross the brainstem to innervate the contralateral inferioroblique nucleus of cranial nerve III (and then the muscle itself)and the ipsilateral superior rectus muscle via a second de-cussation from the superior rectus subnucleus on the rightwhich completely crosses back to the left (on the right side ofthe figure) The excitatory pathways are shown in orange andthe reciprocal inhibitory pathways are shown in blue Activa-tion of both canals (as with pitching the head downward andattempting straight ahead fixation) will result in cancellationof the torsional vector components but addition of the verti-cal vector components resulting in upward movement of theeyes
Neurology 70 April 22 2008 e59
tivum to the oculomotor nuclei Thus threepathways may contribute to the generation of eyemovements during stimulation of the anteriorsemicircular canal
Posterior semicircular canal projections in the MLFFor the posterior canal system excitatory neu-rons project from the vestibular nuclei at the junc-tion of the MVN and VLVN rostrally mediallyand dorsally through MVN until at the level ofthe caudal abducens nucleus they turn mediallyand cross the midline beneath the nucleus prep-ositus hypoglossi (NPH) and abducens nucleusventral to the MLF After crossing the midlinethey enter the MLF and project rostrally to thetrochlear nucleus and inferior rectus subdivisionof the oculomotor complex5 The trochlear axonswithin cranial nerve IV then exit the brainstemposteriorly (the only cranial nerve to do so) andcompletely decussate before projecting forwardto innervate the superior oblique muscle (on theside of posterior canal activation) (figure 4) In-hibitory neurons subserving the posterior semicir-cular canals are found in the SVN and rostral
MVN Their axons project through the pontinereticular formation to reach the ipsilateral MLFand then contact the superior rectus and inferioroblique subdivisions of the oculomotor complexin order to avoid movements antagonistic tothose mediated by the posterior canal system
An important clinical implication of the differ-ence in anatomic projections of the posterior andanterior canal pathways is that patients withMLF lesions may have a dissociated vertical nys-tagmus and relative sparing of response to up-ward vs downward rotation of the head67
Otolithic projections in the MLF The otolith or-gans detect linear acceleration The projectionsfrom the vestibular nuclei that mediate otolith-ocular reflexes are less well defined and there is apaucity of evidence for a direct three neuron arc(eg otolith organ vestibular nucleus ocularmotor neuron) comparable to the three neuronarc for semicircular canal mediated reflexes Pre-sumably the horizontal translational VOR is me-diated by the same abducens nucleus pathway asare the other conjugate systems though there issome evidence for a direct projection of utricularafferents to the abducens nucleus
Responses to static head tilt especially lateraltilt of the head (ear to shoulder) have been longknown to produce ocular counterrolling due toactivation of the cyclovertical ocular muscles8
Under normal circumstances when the head istilted to the left the eyes counterroll in the oppo-site direction (upper poles of the eyes slowly mov-ing away from the side of the tilt) This reflex ismediated by projections that innervate the left eyeintorters (superior rectus and superior oblique)and the right eye extorters (inferior rectus and in-ferior oblique) (figure 5) Following the slowphase counterroll there is a fast torsional move-ment in the opposite direction (upper poles beat-ing to the side of the head tilt) which is mediatedby the riMLF in the rostral midbrain9
Anatomically these graviceptive pathwayscross to the other side of the brainstem approxi-mately in the middle of the pons and further as-cend in the MLF to the ocular motor nuclei(nuclei III and IV) and the premotor gaze centersin the rostra1 midbrain (interstitial nucleus of Ca-jal [INC] and riMLF)10 From there further con-nections reach multiple cortical areas throughthalamic projections
A common clinical finding in patients withunilateral MLF lesions involving the central oto-lith pathway is the ocular tilt reaction (OTR)which consists of a head tilt ocular counter-rolling (generally with the upper pole of the eyes
Figure 4 Projections from the left posteriorsemicircular canal
Axons from the canal project to the ipsilateral vestibular nu-clei and then decussate to innervate the contralateral infe-rior rectus subnucleus of the oculomotor complex of cranialnerve III and the trochlear nucleus The trochlear neuronsthen exit the brainstem posteriorly and decussate back tothe left side innervating the superior oblique muscle Activa-tion of both canals (as with pitching the head upward andattempting straight ahead fixation) will result in cancellationof the torsional vector components but addition of the verti-cal vector components resulting in downward movement ofthe eyes
e60 Neurology 70 April 22 2008
rotating toward a lesion below the pons and awayfrom a lesion at the level of the pons or midbrain)and skew deviation (a supranuclear vertical mis-alignment of the two eyes)11 The head tilt is typi-cally away from the side of the higher eye
In typical skew deviations the higher eye iscontralateral to a medullary lesion and ipsilateralto a mid pontine (the level at which otolith projec-tions decussate the brainstem) or midbrain lesionOcular counterroll may be recognized during fun-duscopic examination where the nearly horizon-tal plane between the optic disc and macula (themacula-disc line) is now deviated12 For examplein the case of a left lateral medullary syndromean ocular tilt reaction might involve left head tiltright hyperdeviation and counterroll of the eyes
(upper poles) toward the left shoulder (or clock-wise rotation with respect to the observer) In es-sence the macula of the left eye is now furtherbelow the disc than usual and the macula of theright eye is further above the disc (figure 6)
Tilting the head relative to gravity from up-right in an ear-down direction so called head rollelicits dissociated changes of eye position Inhealthy subjects both eyes counterroll (upperpoles of the eyes moving away from the side of thehead tilt) by roughly 10 of the head roll but theextorting eye rotates about 1 to 2 deg more thanthe intorting eye (figure 5)813 Furthermore asmall skew deviation (vertical misalignment) ofabout 05 deg appears with hypertropia of the in-torting eye10
Unilateral peripheral or pontomedullary le-sions below the pontine crossing of the gravicep-tive pathways produce a skew deviation andbinocular torsion (combination of these signs issometimes called skew torsion) For instance apatient with a left medullary lesion will have aright hypertropia and counterroll of the eyes to-ward the left shoulder (figure 7) Lesions of thelower graviceptive pathways tend to produce dis-conjugate torsion which is typically greatest inthe excyclotorted eye In contrast a unilateralpontomesencephalic brainstem lesion leads tocontraversive skew torsion10 In this case the hy-pertropic eye is ipsilateral to the lesion and theocular torsion is usually conjugate and to theshoulder opposite the side of the lesion If skewtorsion is associated with a head tilt in the direc-tion of the lower eye this configuration of clinicalsigns is called ocular tilt reaction Since bothgraviceptive pathways and internuclear connec-tions between ocular motor nuclei travel alongthe MLF skew torsion due to pontomesence-phalic lesions is frequently associated with inter-nuclear ophthalmoparesis (INO) (see INOsection)2 The hypertropic eye is generally on theside of the INO (figure 8)
INTERNUCLEAR OPHTHALMOPARESIS Themost commonly recognized syndrome that resultsfromMLF damage is INO and is characterized byslowing or limitation of adduction (on the sameside as the MLF lesion) during horizontal eyemovements (figures 8 and 9)1214-17
In patients with INO the contralateral ab-ducting eye will usually exhibit a disassociatedhorizontal nystagmus although this does notalways occur6 One hypothesis to explain ab-duction nystagmus implicates an adaptive re-sponse to overcome the weakness of the
Figure 5 Pathways involved in the counterroll of the eyes (dotted arrows) duringa head tilt
In this example a left head tilt results in a counterclockwise (with respect to the examiner)torsional counterroll of the upper poles of the eyes This response is mediated by a crossedotolith projection to the extorters in the patientrsquos right eye (the inferior oblique and inferiorrectus muscles) and a double crossed projection to the intorters of the left eye (the superioroblique and superior rectus muscles) These slow phases are punctuated by torsional fastphases that are mediated by the rostral interstitial nucleus of the medial longitudinal fascicu-lus The interstitial nucleus of Cajal (INC) is also shown (without connections) This importantmidbrain structure contains circuitry important for neural integration of vertical and torsionalgaze eye-head coordination during roll movements and contains inhibitory burst neurons forvertical eye movements3 Lesions of these otolith projections result in the opposite reciprocaleffects leading to intorsion and elevation of the right eye and extorsion and depression of theleft eye the so-called skew deviation If the lesion occurs prior to the otolith pathway de-cussation (here on the left) then the lower left eye is on the side of the lesion Alternately ifthe lesion is within this pathway after the decussation (in the pons or midbrain) then thehigher eye is on the side of the lesion
Neurology 70 April 22 2008 e61
contralateral medial rectus6 This is explainedby Heringrsquos law of equal innervation whichstates that attempts to increase innervation tothe weak muscle in one eye must be accompa-nied by a commensurate increase in innervationto the yoke muscle in the other eye Subclinicalnystagmus in the adducting eye (not appreci-ated on bedside examination) has been demon-strated with electro-ocular techniques1819
NEUROPHYSIOLOGY OF INO The diagnosis ofINO can now be precisely confirmed neurophysi-ologically by a number of eye movement trackingtechniques such as infrared oculography18-24
These techniques can identify a variety of abnor-malities in patients with INO including slowingof adduction saccades abduction nystagmus anddiminished adduction saccadic amplitude (figure10) The ratio of saccade metrics between the ab-ducting and adducting eyes the versional discon-jugacy index (VDI) can be measured by infraredoculography and represents a sensitive measure ofthe disconjugacy seen in patients with INO21-23
We have recently defined quantitative oculo-graphic diagnostic criteria for confirming thepresence and severity of INO utilizing a VDI ve-locity Z-score methodology in order to comparepatients with multiple sclerosis (MS) with INOwith a normal control reference population23
Further we have defined a new amplitude mea-sure of disconjugacy in INO the first-pass ampli-tude (FPA)24 The FPA is the ratio of theabductingadducting eye at the point where theabducting eye first achieves the eccentric visualtarget (figure 10)
In the most subtle form of INO the range ofadduction is normal whereas only the velocity isreduced This mild form of INO can often beoverlooked on clinical examination and may onlybe evident on formal oculographic recording Inone study more than 80 of patients with MSwith INO had only slight or no restriction of ad-duction25 Neurologic examination for detectingthe subtle adduction lag INO can be improved bythe use of an optokinetic tape
In a recent study we assessed the accuracy ofclinical detection of INO by 279 physician evalua-tors who were asked to identify the syndromewhen viewing a video of 18 subjects (some ofwhom had unilateral or bilateral INO of varyingseverity and normal subjects without INO)19
The utilization of infrared oculography allowedus to validate the presence of this syndrome byspecific criteria and to quantitatively characterizethe relationship between the severity of the syn-drome and the accuracy of clinical detection Thedetection rates were highly accurate across all
Figure 6 Another consequence of otolithic imbalance that accompanies skewdeviation is the phenomenon of ocular counterroll
These fundus photographs show the extorsion (upper pole of the eye rotated away from thenose or toward the left shoulder) of the left eye (OS) with the disc-macular line rotated clock-wise (according to the examiner) and the right eye (OD) intorted (upper pole of the eye towardthe nose or toward the left shoulder) with the macular-disc line rotated clockwise (againaccording to the examiner) A lesion within the otolith projections in the medial longitudinalfasciculus at the level of the left medulla (the side of the lower eye) or right pons or midbrain(side of the higher eye) would result in this appearance
Figure 7 A patient with a marked skew deviationand symptomatic complaints ofvertical diplopia
Note the severe vertical misalignment of the two eyes Thisabnormality is the consequence of otolith disruption and issupranuclear in mechanism (ductions were intact for all indi-vidual eye muscles)
Figure 8 One of our patients with multiplesclerosis had a dorsal midbrainsyndrome that included a lefthyperdeviation consistent withskew deviation and a leftinternuclear ophthalmoparesis (onattempted right gaze as seen in thelower figure)
The lesion was at the level of the left midbrain (after the de-cussation of the rightward originating otolith pathways) andinvolved the medial longitudinal fasciculus Also note the en-larged left pupil which exhibited the characteristics of near-light dissociation
e62 Neurology 70 April 22 2008
physician groups when the degree of adductionslowing was severe Alternately milder cases ofINO were frequently not identified by the major-ity of evaluators
Most demyelinating lesions of the MLF are lo-cated in the pons or midbrain often sparing thevergence pathways including the fibers project-ing from the medial rectus subnucleus of cranialnerve III2 As a result convergence is intact in themajority of patients despite adduction weaknesson lateral gaze This finding can help distinguishan INO from partial third nerve palsy Furtherthe two eyes are typically well aligned in the pri-mary position (nearly orthophoric or slightly exo-phoric on cross cover testing with one eyeviewing) compared to third nerve palsies whichcommonly produce a conspicuous exotropia (amisalignment with both eyes viewing) along withabnormalities of the eyelid and pupil and otherextraocular muscles
INO can produce a modest slowing of abduc-tion as well as adduction in the same affectedeye2 In an extreme example it has been reportedthat a complete horizontal monocular failure ofeye movement can occur (affecting the ipsilateralmedial longitudinal fasciculus and possibly theabducens nerve fascicle as well) in associationwith a dorsolateral pontine tegmentum lesion asthe first event of MS26
INO SYNDROMES One-and-a-half syndromeThis syndrome consists of a gaze palsy in one direc-tion with an INO when executing a saccade to theopposite side It is produced by damage to the PPRFor abducens nucleus and the MLF on the same sidewithin the pontine tegmentum27 Convergence isgenerally spared as cranial nerve III is spared bilater-ally Given the preserved abduction of the eye con-tralateral to the lesion one commonly observes aprimary position exotropia also known as paralyticpontine exotropia (figure 11)28
Wall-eyed bilateral INO syndrome If the lesion af-fects the MLF within the pons or midbrain ver-gence pathways and the oculomotor apparatuscan be coincidentally disrupted resulting in a va-riety of eye movement abnormalities that includeimpaired convergence29 These lesions are typi-cally bilateral and produce divergence of the eyes(wall-eyed) (figure 12)
INO and trochlear syndrome A highly unusualsyndrome involves a unilateral lesion of the MLFat the level of the caudal midbrain with extensioninto the trochlear nucleus on the same side30
This lesion produces an INO and contralateralhyperdeviation secondary to a IV nerve palsy (re-member the trochlear nerve exits and decussatesto innervate the opposite side superior obliquemuscle) This syndrome can be confused with a
Figure 9 Volitional saccadic pathway with alesion in the right medial longitudinalfasciculus (MLF) that results in aninternuclear ophthalmoparesis (INO)
Volitional saccadic pathway with a lesion in the right MLFthat results in an INO during an attempted saccade to thepatientrsquos left
Figure 10 Infrared oculogram derived from a patient with multiple sclerosiswith bilateral internuclear ophthalmoparesis
In this case a rightward (upward tracing) 20 deg saccade results in interocular disconjugacy(note separation of the two tracings) Observe that the right eye (OD in blue) achieves the 20deg target rapidly whereas the left eye (OS in red) lags behind The ratio of the eyes when theabducting right eye achieves the target to the position of the adducting eye at that time isreferred to as the first pass amplitude (FPA) Ultimately both eyes achieve the fixation targetthe final amplitude (FA) During the trajectory of the saccade the divergence of the two eyescan result in loss of stereoscopy diplopia (transiently) difficulty reading visual blur and riskof fall while turning or motor vehicle accident with head turning while driving
Neurology 70 April 22 2008 e63
skew deviation however in the case of INO andskew deviation the hyperdeviation is generally onthe side of the INO
ABNORMAL VERTICAL EYE MOVEMENTSWITH MLF LESIONS The MLF contains path-ways involved in the regulation of vertical pur-suit vertical vestibular signals and vertical
alignment2931-33 Patients with INO will thereforeoften exhibit abnormalities with vertical eyemovements including the following diminishedvertical gaze holding abnormal optokinetic andpursuit responses decreased vertical VOR gainvertical gaze-evoked nystagmus convergent-retraction nystagmus decreased vertical smoothpursuit and skew deviation
CLINICAL MANIFESTATIONS OF INO The clin-ical manifestations associated with INO includediplopia (typically horizontal binocular) visualconfusion the illusion of environmental move-ment during horizontal saccades (oscillopsia)vertigo and blurring of visual image acuity par-ticularly with reading2 A less conspicuous butpotentially dangerous feature includes worseningdisconjugacy and a resultant break in binocularfusion during head active turning (which pro-duces a contraversive slow phase punctuated bysaccades in the direction of head movement)while head turning during driving (eg changinglanes) and while ambulating
RADIOGRAPHIC IDENTIFICATION OF MLFLESIONS Several pathologic studies have showna clear anatomic relationship between the pres-ence of lesions along the ipsilateral MLF and thepresence of INO114-17 Due to its high spatial reso-lution MRI has allowed us to depict in vivo theanatomic organization of the human oculomotornerve complex theMLF and related structures inthe brainstem (typically white matter tracts havelow signal intensity and nuclei have higher signalintensity)34 Moreover MRI has also contributedto a better understanding of the different stages ofmyelination of these structures in the pretermbrain35
In patients with INO MRI has shown hyper-intense lesions in the region of the MLF on T2-weighted images that were not detected usingCT36 T2-hyperintensities in the pontine and mid-brain tegmentum portion of the MLF have beenshown in a high percentage of patients with INOderived from different neurologic disorders (fig-ure 13) In one study involving 58 patients withMS with INO MRI with proton density imagingdetected a higher percentage of MLF involvement(100) than T2 (88) and fast-FLAIR (48)37
We have recently studied the relationship be-tween the severity of INO and correspondingmeasures of brain tissue injury within the MLFderived from the advanced neuroradiologic tech-niques diffusion tensor imaging and magnetiza-tion transfer imaging38 The application ofneurophysiologic methods in the quantitative
Figure 11 An example of the one-and-a-half syndrome in one of our patientswith multiple sclerosis
The patient was unable to elicit saccades to the right (ie a right gaze palsy) and had evi-dence of a right internuclear ophthalmoparesis (INO) upon attempted gaze to the left In thisphotograph the patient is looking straight ahead We can observe an exotropia the so-calledparalytic pontine exotropia with the left eye in exo (the only remaining movement possible) Inthis circumstance there is an attempted leftward preference However only left eye abduc-tion is possible given the right INO (with slowing and significant ocular limitation) Below is theT2-weighted axial MRI showing the responsible lesion involving the right pontine tegmentum(arrow)
Figure 12 The syndrome of wall-eyed bilateralinternuclear ophthalmoparesis(INO) in an patient with multiplesclerosis with progressive diseaseand a history of a severeinflammatory demyelinatingsyndrome involving thetegmentum of the ponto-mesencephalic junction whichaffected the medial longitudinalfasciculus (MLF) bilaterally
Note the exotropic appearance of both eyes (ie wall-eyed)Attempted gaze to the right or left revealed adduction slow-ing and limitation consistent with bilateral INO There wasalso reduced vertical smooth pursuit and vertical vestibulo-ocular reflexes (both pathways course through the MLF)
e64 Neurology 70 April 22 2008
analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

lar motor nuclei (pairs of cranial nerve III IV VI)are interconnected via the MLF which transmitsvital information for the purpose of coordinatedand synchronized movements of the eyes to a vi-sual target Within this system are both excitatoryas well as reciprocal inhibitory projections thatserve to precisely regulate the interplay betweenagonist and antagonist muscles of the eyes
In this review we characterize the physiologyof the component tract systems contained withinthis central ocular motor circuitry and provide adetailed discussion of the most common neuro-logic signs and symptoms associated with lesionsof this structure
MLF CIRCUITRY OF SACCADIC EYE MOVE-MENTS The saccadic apparatus includes neuronsin the frontal eye field (FEF) which project to anumber of subcortical structures that serve to me-diate rapid gaze shifts to remembered targets3
The FEF sends a signal to the ipsilateral superiorcolliculus (SC) and to the contralateral paramed-ian pontine reticular formation (PPRF) for hori-zontal saccades and to the rostral interstitialnucleus of the MLF (riMLF) for vertical saccadesThe PPRF contains excitatory burst neurons thatproduce the supranuclear horizontal saccadic eyevelocity command sequence (the pulse)4 Theseneurons project to the adjacent VI (abducens)nerve nucleus The abducens nucleus consists oftwo types of neurons that mediate conjugate hor-izontal eye movements Abducens motoneuronsinnervate the ipsilateral lateral rectus musclewhereas axons from abducens interneurons crossto the contralateral pons and ascend via the MLFto innervate the medial rectus subnucleus of cra-nial nerve III which ultimately projects to the me-dial rectus muscle (figure 1) The parietal cortex iscentral in the production of smooth pursuit eyemovements but also participates in the produc-tion of saccades and has a direct projection to theSC In contrast to the FEF the parietal cortex ismore involved in the production of saccades tonovel visual stimuli rather than to rememberedtargets3 As with saccades smooth pursuit path-ways ultimately converge upon the MLF for theexecution of both horizontal and vertical eyemovements
VESTIBULAR COMPONENTS OF THE MLF Ca-nal system afferents The MLF is the principaltract system by which signals reach the ocularmotoneurons for eye movements generated inresponse to vestibular stimuli3 There may how-ever be differences in the anatomic circuitry un-derlying these reflexes depending upon whether
the eye movements are compensatory for angularmotion of the head mediated by the semicircularcanals (called the rotational vestibular ocular re-flex r-VOR) or for linear acceleration of thehead mediated by the otolith organs (utriculusand sacculus)
Lateral semicircular canal projections in the MLFThe pathways underlying the angular VOR arereasonably well understood For the lateral canalsystem the r-VOR is mediated by the same path-way carrying information for the other conjugateeye movement systems (saccade and pursuit) Theabducens nucleus is the gaze center for the finalpathway of horizontal eye movements Stimula-tion of the lateral semicircular canal results intransmission of information (from horizontalhead motion or caloric activation) within the ipsi-lateral VIII nerve and nucleus5 Projections thenemanate from the medial vestibular nucleus to in-nervate the contralateral VI nucleus Abducens
Figure 1 Details of the descending projectioninvolved in the volitional control ofhorizontal saccadic eye movements
Excitatory pathways are shown in orange and the reciprocalinhibitory pathways are shown in blue The particular path-way shown emanates from the frontal eye field (FEF) whichprojects through the anterior limb of the internal capsule de-cussates to the opposite side at the midbrain-pontine junc-tion and then innervates the paramedian pontine reticularformation (PPRF) From there projections directly innervatethe lateral rectus (ipsilateral to the PPRF) A second decussa-tion back to the side of origin of FEF activation via the MLFinnervates the medial rectus subnucleus of cranial nerve IIIand then neurons here project to innervate the medial rectusmuscle The right FEF command to trigger a saccade culmi-nates in conjugate eye movements to the left According toHerringrsquos law the horizontal yoke pair the medial and lateralrecti are activated in synchrony
e58 Neurology 70 April 22 2008
motoneurons then project to the lateral rectusmuscle while abducens interneurons project intothe contralateral MLF where their axons inner-vate the medical rectus subnucleus of the ocularmotor nucleus with a final projection to the me-dial rectus muscle (figure 2)
Anterior semicircular canal projections in the MLFFor the anterior canal system there may be threeexcitatory pathways by which information is car-ried rostrally for the vertical r-VOR Excitatorycells in the medial vestibular nucleus or adjacentventral lateral vestibular nucleus (VLVN) projectmedially and dorsally crossing the midline cau-dally5 After crossing they ascend in or just belowthe MLF to contact the superior rectus and infe-rior oblique subdivisions of the oculomotor com-plex Importantly the superior rectus subnucleussends fibers that decussate to innervate the supe-rior rectus muscle on the side of anterior canalactivation (figure 3) In this way one semicircularcanal can innervate muscles in both eyes for ap-propriate yoking of eye movements Inhibitory
neurons for the anterior canal system lie in thesuperior vestibular nucleus (SVN) Their axonsexit from the rostromedial aspect of this nucleusand course medially and rostrally in the lateralwing of the ipsilateral MLF to contact superioroblique motoneurons in the trochlear nucleusand inferior rectus neurons in the oculomotor nu-cleus to antagonize those eye movements medi-ated by an activated anterior canal system3
Another cell group that may contribute excita-tory inputs from the anterior canal system lies inthe SVN Their axons cross the midline in theventral tegmental tract close to the medial lem-niscus at the rostral pole of the nucleus reticularistegmenti pontis (NRTP) and then abruptly turnrostrally passing through the decussation of thesuperior cerebellar peduncle to terminate mainlyon the superior rectus and inferior oblique subdi-visions of the oculomotor complex3 Also insome species (perhaps also in humans) the SVNprojects rostrally just near the brachium conjunc-
Figure 2 Projections involved in the activationof the left lateral semicircular canal
This figure illustrates the projections involved during the ac-tivation of the left lateral semicircular canal For instanceduring a leftward rotation of the head while attempting tomaintain straight ahead gaze axons from left lateral canal(on the right side of the figure) canal neurons project to ipsi-lateral vestibular nucleus (primarily the medial) which thenprojects across the brainstem to innervate the opposite rightabducens (VI) nucleus This nucleus has two populations ofneurons a direct projection to the same side lateral rectus(right) and an interneuronal projection that crosses back tothe left side via the MLF and then innervates the medial rec-tus subnucleus of cranial nerve III which ultimately inner-vates the left medial rectus muscle
Figure 3 Projections involved in the activationof the left anterior canal
Axons from anterior semicircular canal neurons project tothe ipsilateral vestibular nucleus and from there decussateacross the brainstem to innervate the contralateral inferioroblique nucleus of cranial nerve III (and then the muscle itself)and the ipsilateral superior rectus muscle via a second de-cussation from the superior rectus subnucleus on the rightwhich completely crosses back to the left (on the right side ofthe figure) The excitatory pathways are shown in orange andthe reciprocal inhibitory pathways are shown in blue Activa-tion of both canals (as with pitching the head downward andattempting straight ahead fixation) will result in cancellationof the torsional vector components but addition of the verti-cal vector components resulting in upward movement of theeyes
Neurology 70 April 22 2008 e59
tivum to the oculomotor nuclei Thus threepathways may contribute to the generation of eyemovements during stimulation of the anteriorsemicircular canal
Posterior semicircular canal projections in the MLFFor the posterior canal system excitatory neu-rons project from the vestibular nuclei at the junc-tion of the MVN and VLVN rostrally mediallyand dorsally through MVN until at the level ofthe caudal abducens nucleus they turn mediallyand cross the midline beneath the nucleus prep-ositus hypoglossi (NPH) and abducens nucleusventral to the MLF After crossing the midlinethey enter the MLF and project rostrally to thetrochlear nucleus and inferior rectus subdivisionof the oculomotor complex5 The trochlear axonswithin cranial nerve IV then exit the brainstemposteriorly (the only cranial nerve to do so) andcompletely decussate before projecting forwardto innervate the superior oblique muscle (on theside of posterior canal activation) (figure 4) In-hibitory neurons subserving the posterior semicir-cular canals are found in the SVN and rostral
MVN Their axons project through the pontinereticular formation to reach the ipsilateral MLFand then contact the superior rectus and inferioroblique subdivisions of the oculomotor complexin order to avoid movements antagonistic tothose mediated by the posterior canal system
An important clinical implication of the differ-ence in anatomic projections of the posterior andanterior canal pathways is that patients withMLF lesions may have a dissociated vertical nys-tagmus and relative sparing of response to up-ward vs downward rotation of the head67
Otolithic projections in the MLF The otolith or-gans detect linear acceleration The projectionsfrom the vestibular nuclei that mediate otolith-ocular reflexes are less well defined and there is apaucity of evidence for a direct three neuron arc(eg otolith organ vestibular nucleus ocularmotor neuron) comparable to the three neuronarc for semicircular canal mediated reflexes Pre-sumably the horizontal translational VOR is me-diated by the same abducens nucleus pathway asare the other conjugate systems though there issome evidence for a direct projection of utricularafferents to the abducens nucleus
Responses to static head tilt especially lateraltilt of the head (ear to shoulder) have been longknown to produce ocular counterrolling due toactivation of the cyclovertical ocular muscles8
Under normal circumstances when the head istilted to the left the eyes counterroll in the oppo-site direction (upper poles of the eyes slowly mov-ing away from the side of the tilt) This reflex ismediated by projections that innervate the left eyeintorters (superior rectus and superior oblique)and the right eye extorters (inferior rectus and in-ferior oblique) (figure 5) Following the slowphase counterroll there is a fast torsional move-ment in the opposite direction (upper poles beat-ing to the side of the head tilt) which is mediatedby the riMLF in the rostral midbrain9
Anatomically these graviceptive pathwayscross to the other side of the brainstem approxi-mately in the middle of the pons and further as-cend in the MLF to the ocular motor nuclei(nuclei III and IV) and the premotor gaze centersin the rostra1 midbrain (interstitial nucleus of Ca-jal [INC] and riMLF)10 From there further con-nections reach multiple cortical areas throughthalamic projections
A common clinical finding in patients withunilateral MLF lesions involving the central oto-lith pathway is the ocular tilt reaction (OTR)which consists of a head tilt ocular counter-rolling (generally with the upper pole of the eyes
Figure 4 Projections from the left posteriorsemicircular canal
Axons from the canal project to the ipsilateral vestibular nu-clei and then decussate to innervate the contralateral infe-rior rectus subnucleus of the oculomotor complex of cranialnerve III and the trochlear nucleus The trochlear neuronsthen exit the brainstem posteriorly and decussate back tothe left side innervating the superior oblique muscle Activa-tion of both canals (as with pitching the head upward andattempting straight ahead fixation) will result in cancellationof the torsional vector components but addition of the verti-cal vector components resulting in downward movement ofthe eyes
e60 Neurology 70 April 22 2008
rotating toward a lesion below the pons and awayfrom a lesion at the level of the pons or midbrain)and skew deviation (a supranuclear vertical mis-alignment of the two eyes)11 The head tilt is typi-cally away from the side of the higher eye
In typical skew deviations the higher eye iscontralateral to a medullary lesion and ipsilateralto a mid pontine (the level at which otolith projec-tions decussate the brainstem) or midbrain lesionOcular counterroll may be recognized during fun-duscopic examination where the nearly horizon-tal plane between the optic disc and macula (themacula-disc line) is now deviated12 For examplein the case of a left lateral medullary syndromean ocular tilt reaction might involve left head tiltright hyperdeviation and counterroll of the eyes
(upper poles) toward the left shoulder (or clock-wise rotation with respect to the observer) In es-sence the macula of the left eye is now furtherbelow the disc than usual and the macula of theright eye is further above the disc (figure 6)
Tilting the head relative to gravity from up-right in an ear-down direction so called head rollelicits dissociated changes of eye position Inhealthy subjects both eyes counterroll (upperpoles of the eyes moving away from the side of thehead tilt) by roughly 10 of the head roll but theextorting eye rotates about 1 to 2 deg more thanthe intorting eye (figure 5)813 Furthermore asmall skew deviation (vertical misalignment) ofabout 05 deg appears with hypertropia of the in-torting eye10
Unilateral peripheral or pontomedullary le-sions below the pontine crossing of the gravicep-tive pathways produce a skew deviation andbinocular torsion (combination of these signs issometimes called skew torsion) For instance apatient with a left medullary lesion will have aright hypertropia and counterroll of the eyes to-ward the left shoulder (figure 7) Lesions of thelower graviceptive pathways tend to produce dis-conjugate torsion which is typically greatest inthe excyclotorted eye In contrast a unilateralpontomesencephalic brainstem lesion leads tocontraversive skew torsion10 In this case the hy-pertropic eye is ipsilateral to the lesion and theocular torsion is usually conjugate and to theshoulder opposite the side of the lesion If skewtorsion is associated with a head tilt in the direc-tion of the lower eye this configuration of clinicalsigns is called ocular tilt reaction Since bothgraviceptive pathways and internuclear connec-tions between ocular motor nuclei travel alongthe MLF skew torsion due to pontomesence-phalic lesions is frequently associated with inter-nuclear ophthalmoparesis (INO) (see INOsection)2 The hypertropic eye is generally on theside of the INO (figure 8)
INTERNUCLEAR OPHTHALMOPARESIS Themost commonly recognized syndrome that resultsfromMLF damage is INO and is characterized byslowing or limitation of adduction (on the sameside as the MLF lesion) during horizontal eyemovements (figures 8 and 9)1214-17
In patients with INO the contralateral ab-ducting eye will usually exhibit a disassociatedhorizontal nystagmus although this does notalways occur6 One hypothesis to explain ab-duction nystagmus implicates an adaptive re-sponse to overcome the weakness of the
Figure 5 Pathways involved in the counterroll of the eyes (dotted arrows) duringa head tilt
In this example a left head tilt results in a counterclockwise (with respect to the examiner)torsional counterroll of the upper poles of the eyes This response is mediated by a crossedotolith projection to the extorters in the patientrsquos right eye (the inferior oblique and inferiorrectus muscles) and a double crossed projection to the intorters of the left eye (the superioroblique and superior rectus muscles) These slow phases are punctuated by torsional fastphases that are mediated by the rostral interstitial nucleus of the medial longitudinal fascicu-lus The interstitial nucleus of Cajal (INC) is also shown (without connections) This importantmidbrain structure contains circuitry important for neural integration of vertical and torsionalgaze eye-head coordination during roll movements and contains inhibitory burst neurons forvertical eye movements3 Lesions of these otolith projections result in the opposite reciprocaleffects leading to intorsion and elevation of the right eye and extorsion and depression of theleft eye the so-called skew deviation If the lesion occurs prior to the otolith pathway de-cussation (here on the left) then the lower left eye is on the side of the lesion Alternately ifthe lesion is within this pathway after the decussation (in the pons or midbrain) then thehigher eye is on the side of the lesion
Neurology 70 April 22 2008 e61
contralateral medial rectus6 This is explainedby Heringrsquos law of equal innervation whichstates that attempts to increase innervation tothe weak muscle in one eye must be accompa-nied by a commensurate increase in innervationto the yoke muscle in the other eye Subclinicalnystagmus in the adducting eye (not appreci-ated on bedside examination) has been demon-strated with electro-ocular techniques1819
NEUROPHYSIOLOGY OF INO The diagnosis ofINO can now be precisely confirmed neurophysi-ologically by a number of eye movement trackingtechniques such as infrared oculography18-24
These techniques can identify a variety of abnor-malities in patients with INO including slowingof adduction saccades abduction nystagmus anddiminished adduction saccadic amplitude (figure10) The ratio of saccade metrics between the ab-ducting and adducting eyes the versional discon-jugacy index (VDI) can be measured by infraredoculography and represents a sensitive measure ofthe disconjugacy seen in patients with INO21-23
We have recently defined quantitative oculo-graphic diagnostic criteria for confirming thepresence and severity of INO utilizing a VDI ve-locity Z-score methodology in order to comparepatients with multiple sclerosis (MS) with INOwith a normal control reference population23
Further we have defined a new amplitude mea-sure of disconjugacy in INO the first-pass ampli-tude (FPA)24 The FPA is the ratio of theabductingadducting eye at the point where theabducting eye first achieves the eccentric visualtarget (figure 10)
In the most subtle form of INO the range ofadduction is normal whereas only the velocity isreduced This mild form of INO can often beoverlooked on clinical examination and may onlybe evident on formal oculographic recording Inone study more than 80 of patients with MSwith INO had only slight or no restriction of ad-duction25 Neurologic examination for detectingthe subtle adduction lag INO can be improved bythe use of an optokinetic tape
In a recent study we assessed the accuracy ofclinical detection of INO by 279 physician evalua-tors who were asked to identify the syndromewhen viewing a video of 18 subjects (some ofwhom had unilateral or bilateral INO of varyingseverity and normal subjects without INO)19
The utilization of infrared oculography allowedus to validate the presence of this syndrome byspecific criteria and to quantitatively characterizethe relationship between the severity of the syn-drome and the accuracy of clinical detection Thedetection rates were highly accurate across all
Figure 6 Another consequence of otolithic imbalance that accompanies skewdeviation is the phenomenon of ocular counterroll
These fundus photographs show the extorsion (upper pole of the eye rotated away from thenose or toward the left shoulder) of the left eye (OS) with the disc-macular line rotated clock-wise (according to the examiner) and the right eye (OD) intorted (upper pole of the eye towardthe nose or toward the left shoulder) with the macular-disc line rotated clockwise (againaccording to the examiner) A lesion within the otolith projections in the medial longitudinalfasciculus at the level of the left medulla (the side of the lower eye) or right pons or midbrain(side of the higher eye) would result in this appearance
Figure 7 A patient with a marked skew deviationand symptomatic complaints ofvertical diplopia
Note the severe vertical misalignment of the two eyes Thisabnormality is the consequence of otolith disruption and issupranuclear in mechanism (ductions were intact for all indi-vidual eye muscles)
Figure 8 One of our patients with multiplesclerosis had a dorsal midbrainsyndrome that included a lefthyperdeviation consistent withskew deviation and a leftinternuclear ophthalmoparesis (onattempted right gaze as seen in thelower figure)
The lesion was at the level of the left midbrain (after the de-cussation of the rightward originating otolith pathways) andinvolved the medial longitudinal fasciculus Also note the en-larged left pupil which exhibited the characteristics of near-light dissociation
e62 Neurology 70 April 22 2008
physician groups when the degree of adductionslowing was severe Alternately milder cases ofINO were frequently not identified by the major-ity of evaluators
Most demyelinating lesions of the MLF are lo-cated in the pons or midbrain often sparing thevergence pathways including the fibers project-ing from the medial rectus subnucleus of cranialnerve III2 As a result convergence is intact in themajority of patients despite adduction weaknesson lateral gaze This finding can help distinguishan INO from partial third nerve palsy Furtherthe two eyes are typically well aligned in the pri-mary position (nearly orthophoric or slightly exo-phoric on cross cover testing with one eyeviewing) compared to third nerve palsies whichcommonly produce a conspicuous exotropia (amisalignment with both eyes viewing) along withabnormalities of the eyelid and pupil and otherextraocular muscles
INO can produce a modest slowing of abduc-tion as well as adduction in the same affectedeye2 In an extreme example it has been reportedthat a complete horizontal monocular failure ofeye movement can occur (affecting the ipsilateralmedial longitudinal fasciculus and possibly theabducens nerve fascicle as well) in associationwith a dorsolateral pontine tegmentum lesion asthe first event of MS26
INO SYNDROMES One-and-a-half syndromeThis syndrome consists of a gaze palsy in one direc-tion with an INO when executing a saccade to theopposite side It is produced by damage to the PPRFor abducens nucleus and the MLF on the same sidewithin the pontine tegmentum27 Convergence isgenerally spared as cranial nerve III is spared bilater-ally Given the preserved abduction of the eye con-tralateral to the lesion one commonly observes aprimary position exotropia also known as paralyticpontine exotropia (figure 11)28
Wall-eyed bilateral INO syndrome If the lesion af-fects the MLF within the pons or midbrain ver-gence pathways and the oculomotor apparatuscan be coincidentally disrupted resulting in a va-riety of eye movement abnormalities that includeimpaired convergence29 These lesions are typi-cally bilateral and produce divergence of the eyes(wall-eyed) (figure 12)
INO and trochlear syndrome A highly unusualsyndrome involves a unilateral lesion of the MLFat the level of the caudal midbrain with extensioninto the trochlear nucleus on the same side30
This lesion produces an INO and contralateralhyperdeviation secondary to a IV nerve palsy (re-member the trochlear nerve exits and decussatesto innervate the opposite side superior obliquemuscle) This syndrome can be confused with a
Figure 9 Volitional saccadic pathway with alesion in the right medial longitudinalfasciculus (MLF) that results in aninternuclear ophthalmoparesis (INO)
Volitional saccadic pathway with a lesion in the right MLFthat results in an INO during an attempted saccade to thepatientrsquos left
Figure 10 Infrared oculogram derived from a patient with multiple sclerosiswith bilateral internuclear ophthalmoparesis
In this case a rightward (upward tracing) 20 deg saccade results in interocular disconjugacy(note separation of the two tracings) Observe that the right eye (OD in blue) achieves the 20deg target rapidly whereas the left eye (OS in red) lags behind The ratio of the eyes when theabducting right eye achieves the target to the position of the adducting eye at that time isreferred to as the first pass amplitude (FPA) Ultimately both eyes achieve the fixation targetthe final amplitude (FA) During the trajectory of the saccade the divergence of the two eyescan result in loss of stereoscopy diplopia (transiently) difficulty reading visual blur and riskof fall while turning or motor vehicle accident with head turning while driving
Neurology 70 April 22 2008 e63
skew deviation however in the case of INO andskew deviation the hyperdeviation is generally onthe side of the INO
ABNORMAL VERTICAL EYE MOVEMENTSWITH MLF LESIONS The MLF contains path-ways involved in the regulation of vertical pur-suit vertical vestibular signals and vertical
alignment2931-33 Patients with INO will thereforeoften exhibit abnormalities with vertical eyemovements including the following diminishedvertical gaze holding abnormal optokinetic andpursuit responses decreased vertical VOR gainvertical gaze-evoked nystagmus convergent-retraction nystagmus decreased vertical smoothpursuit and skew deviation
CLINICAL MANIFESTATIONS OF INO The clin-ical manifestations associated with INO includediplopia (typically horizontal binocular) visualconfusion the illusion of environmental move-ment during horizontal saccades (oscillopsia)vertigo and blurring of visual image acuity par-ticularly with reading2 A less conspicuous butpotentially dangerous feature includes worseningdisconjugacy and a resultant break in binocularfusion during head active turning (which pro-duces a contraversive slow phase punctuated bysaccades in the direction of head movement)while head turning during driving (eg changinglanes) and while ambulating
RADIOGRAPHIC IDENTIFICATION OF MLFLESIONS Several pathologic studies have showna clear anatomic relationship between the pres-ence of lesions along the ipsilateral MLF and thepresence of INO114-17 Due to its high spatial reso-lution MRI has allowed us to depict in vivo theanatomic organization of the human oculomotornerve complex theMLF and related structures inthe brainstem (typically white matter tracts havelow signal intensity and nuclei have higher signalintensity)34 Moreover MRI has also contributedto a better understanding of the different stages ofmyelination of these structures in the pretermbrain35
In patients with INO MRI has shown hyper-intense lesions in the region of the MLF on T2-weighted images that were not detected usingCT36 T2-hyperintensities in the pontine and mid-brain tegmentum portion of the MLF have beenshown in a high percentage of patients with INOderived from different neurologic disorders (fig-ure 13) In one study involving 58 patients withMS with INO MRI with proton density imagingdetected a higher percentage of MLF involvement(100) than T2 (88) and fast-FLAIR (48)37
We have recently studied the relationship be-tween the severity of INO and correspondingmeasures of brain tissue injury within the MLFderived from the advanced neuroradiologic tech-niques diffusion tensor imaging and magnetiza-tion transfer imaging38 The application ofneurophysiologic methods in the quantitative
Figure 11 An example of the one-and-a-half syndrome in one of our patientswith multiple sclerosis
The patient was unable to elicit saccades to the right (ie a right gaze palsy) and had evi-dence of a right internuclear ophthalmoparesis (INO) upon attempted gaze to the left In thisphotograph the patient is looking straight ahead We can observe an exotropia the so-calledparalytic pontine exotropia with the left eye in exo (the only remaining movement possible) Inthis circumstance there is an attempted leftward preference However only left eye abduc-tion is possible given the right INO (with slowing and significant ocular limitation) Below is theT2-weighted axial MRI showing the responsible lesion involving the right pontine tegmentum(arrow)
Figure 12 The syndrome of wall-eyed bilateralinternuclear ophthalmoparesis(INO) in an patient with multiplesclerosis with progressive diseaseand a history of a severeinflammatory demyelinatingsyndrome involving thetegmentum of the ponto-mesencephalic junction whichaffected the medial longitudinalfasciculus (MLF) bilaterally
Note the exotropic appearance of both eyes (ie wall-eyed)Attempted gaze to the right or left revealed adduction slow-ing and limitation consistent with bilateral INO There wasalso reduced vertical smooth pursuit and vertical vestibulo-ocular reflexes (both pathways course through the MLF)
e64 Neurology 70 April 22 2008
analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

motoneurons then project to the lateral rectusmuscle while abducens interneurons project intothe contralateral MLF where their axons inner-vate the medical rectus subnucleus of the ocularmotor nucleus with a final projection to the me-dial rectus muscle (figure 2)
Anterior semicircular canal projections in the MLFFor the anterior canal system there may be threeexcitatory pathways by which information is car-ried rostrally for the vertical r-VOR Excitatorycells in the medial vestibular nucleus or adjacentventral lateral vestibular nucleus (VLVN) projectmedially and dorsally crossing the midline cau-dally5 After crossing they ascend in or just belowthe MLF to contact the superior rectus and infe-rior oblique subdivisions of the oculomotor com-plex Importantly the superior rectus subnucleussends fibers that decussate to innervate the supe-rior rectus muscle on the side of anterior canalactivation (figure 3) In this way one semicircularcanal can innervate muscles in both eyes for ap-propriate yoking of eye movements Inhibitory
neurons for the anterior canal system lie in thesuperior vestibular nucleus (SVN) Their axonsexit from the rostromedial aspect of this nucleusand course medially and rostrally in the lateralwing of the ipsilateral MLF to contact superioroblique motoneurons in the trochlear nucleusand inferior rectus neurons in the oculomotor nu-cleus to antagonize those eye movements medi-ated by an activated anterior canal system3
Another cell group that may contribute excita-tory inputs from the anterior canal system lies inthe SVN Their axons cross the midline in theventral tegmental tract close to the medial lem-niscus at the rostral pole of the nucleus reticularistegmenti pontis (NRTP) and then abruptly turnrostrally passing through the decussation of thesuperior cerebellar peduncle to terminate mainlyon the superior rectus and inferior oblique subdi-visions of the oculomotor complex3 Also insome species (perhaps also in humans) the SVNprojects rostrally just near the brachium conjunc-
Figure 2 Projections involved in the activationof the left lateral semicircular canal
This figure illustrates the projections involved during the ac-tivation of the left lateral semicircular canal For instanceduring a leftward rotation of the head while attempting tomaintain straight ahead gaze axons from left lateral canal(on the right side of the figure) canal neurons project to ipsi-lateral vestibular nucleus (primarily the medial) which thenprojects across the brainstem to innervate the opposite rightabducens (VI) nucleus This nucleus has two populations ofneurons a direct projection to the same side lateral rectus(right) and an interneuronal projection that crosses back tothe left side via the MLF and then innervates the medial rec-tus subnucleus of cranial nerve III which ultimately inner-vates the left medial rectus muscle
Figure 3 Projections involved in the activationof the left anterior canal
Axons from anterior semicircular canal neurons project tothe ipsilateral vestibular nucleus and from there decussateacross the brainstem to innervate the contralateral inferioroblique nucleus of cranial nerve III (and then the muscle itself)and the ipsilateral superior rectus muscle via a second de-cussation from the superior rectus subnucleus on the rightwhich completely crosses back to the left (on the right side ofthe figure) The excitatory pathways are shown in orange andthe reciprocal inhibitory pathways are shown in blue Activa-tion of both canals (as with pitching the head downward andattempting straight ahead fixation) will result in cancellationof the torsional vector components but addition of the verti-cal vector components resulting in upward movement of theeyes
Neurology 70 April 22 2008 e59
tivum to the oculomotor nuclei Thus threepathways may contribute to the generation of eyemovements during stimulation of the anteriorsemicircular canal
Posterior semicircular canal projections in the MLFFor the posterior canal system excitatory neu-rons project from the vestibular nuclei at the junc-tion of the MVN and VLVN rostrally mediallyand dorsally through MVN until at the level ofthe caudal abducens nucleus they turn mediallyand cross the midline beneath the nucleus prep-ositus hypoglossi (NPH) and abducens nucleusventral to the MLF After crossing the midlinethey enter the MLF and project rostrally to thetrochlear nucleus and inferior rectus subdivisionof the oculomotor complex5 The trochlear axonswithin cranial nerve IV then exit the brainstemposteriorly (the only cranial nerve to do so) andcompletely decussate before projecting forwardto innervate the superior oblique muscle (on theside of posterior canal activation) (figure 4) In-hibitory neurons subserving the posterior semicir-cular canals are found in the SVN and rostral
MVN Their axons project through the pontinereticular formation to reach the ipsilateral MLFand then contact the superior rectus and inferioroblique subdivisions of the oculomotor complexin order to avoid movements antagonistic tothose mediated by the posterior canal system
An important clinical implication of the differ-ence in anatomic projections of the posterior andanterior canal pathways is that patients withMLF lesions may have a dissociated vertical nys-tagmus and relative sparing of response to up-ward vs downward rotation of the head67
Otolithic projections in the MLF The otolith or-gans detect linear acceleration The projectionsfrom the vestibular nuclei that mediate otolith-ocular reflexes are less well defined and there is apaucity of evidence for a direct three neuron arc(eg otolith organ vestibular nucleus ocularmotor neuron) comparable to the three neuronarc for semicircular canal mediated reflexes Pre-sumably the horizontal translational VOR is me-diated by the same abducens nucleus pathway asare the other conjugate systems though there issome evidence for a direct projection of utricularafferents to the abducens nucleus
Responses to static head tilt especially lateraltilt of the head (ear to shoulder) have been longknown to produce ocular counterrolling due toactivation of the cyclovertical ocular muscles8
Under normal circumstances when the head istilted to the left the eyes counterroll in the oppo-site direction (upper poles of the eyes slowly mov-ing away from the side of the tilt) This reflex ismediated by projections that innervate the left eyeintorters (superior rectus and superior oblique)and the right eye extorters (inferior rectus and in-ferior oblique) (figure 5) Following the slowphase counterroll there is a fast torsional move-ment in the opposite direction (upper poles beat-ing to the side of the head tilt) which is mediatedby the riMLF in the rostral midbrain9
Anatomically these graviceptive pathwayscross to the other side of the brainstem approxi-mately in the middle of the pons and further as-cend in the MLF to the ocular motor nuclei(nuclei III and IV) and the premotor gaze centersin the rostra1 midbrain (interstitial nucleus of Ca-jal [INC] and riMLF)10 From there further con-nections reach multiple cortical areas throughthalamic projections
A common clinical finding in patients withunilateral MLF lesions involving the central oto-lith pathway is the ocular tilt reaction (OTR)which consists of a head tilt ocular counter-rolling (generally with the upper pole of the eyes
Figure 4 Projections from the left posteriorsemicircular canal
Axons from the canal project to the ipsilateral vestibular nu-clei and then decussate to innervate the contralateral infe-rior rectus subnucleus of the oculomotor complex of cranialnerve III and the trochlear nucleus The trochlear neuronsthen exit the brainstem posteriorly and decussate back tothe left side innervating the superior oblique muscle Activa-tion of both canals (as with pitching the head upward andattempting straight ahead fixation) will result in cancellationof the torsional vector components but addition of the verti-cal vector components resulting in downward movement ofthe eyes
e60 Neurology 70 April 22 2008
rotating toward a lesion below the pons and awayfrom a lesion at the level of the pons or midbrain)and skew deviation (a supranuclear vertical mis-alignment of the two eyes)11 The head tilt is typi-cally away from the side of the higher eye
In typical skew deviations the higher eye iscontralateral to a medullary lesion and ipsilateralto a mid pontine (the level at which otolith projec-tions decussate the brainstem) or midbrain lesionOcular counterroll may be recognized during fun-duscopic examination where the nearly horizon-tal plane between the optic disc and macula (themacula-disc line) is now deviated12 For examplein the case of a left lateral medullary syndromean ocular tilt reaction might involve left head tiltright hyperdeviation and counterroll of the eyes
(upper poles) toward the left shoulder (or clock-wise rotation with respect to the observer) In es-sence the macula of the left eye is now furtherbelow the disc than usual and the macula of theright eye is further above the disc (figure 6)
Tilting the head relative to gravity from up-right in an ear-down direction so called head rollelicits dissociated changes of eye position Inhealthy subjects both eyes counterroll (upperpoles of the eyes moving away from the side of thehead tilt) by roughly 10 of the head roll but theextorting eye rotates about 1 to 2 deg more thanthe intorting eye (figure 5)813 Furthermore asmall skew deviation (vertical misalignment) ofabout 05 deg appears with hypertropia of the in-torting eye10
Unilateral peripheral or pontomedullary le-sions below the pontine crossing of the gravicep-tive pathways produce a skew deviation andbinocular torsion (combination of these signs issometimes called skew torsion) For instance apatient with a left medullary lesion will have aright hypertropia and counterroll of the eyes to-ward the left shoulder (figure 7) Lesions of thelower graviceptive pathways tend to produce dis-conjugate torsion which is typically greatest inthe excyclotorted eye In contrast a unilateralpontomesencephalic brainstem lesion leads tocontraversive skew torsion10 In this case the hy-pertropic eye is ipsilateral to the lesion and theocular torsion is usually conjugate and to theshoulder opposite the side of the lesion If skewtorsion is associated with a head tilt in the direc-tion of the lower eye this configuration of clinicalsigns is called ocular tilt reaction Since bothgraviceptive pathways and internuclear connec-tions between ocular motor nuclei travel alongthe MLF skew torsion due to pontomesence-phalic lesions is frequently associated with inter-nuclear ophthalmoparesis (INO) (see INOsection)2 The hypertropic eye is generally on theside of the INO (figure 8)
INTERNUCLEAR OPHTHALMOPARESIS Themost commonly recognized syndrome that resultsfromMLF damage is INO and is characterized byslowing or limitation of adduction (on the sameside as the MLF lesion) during horizontal eyemovements (figures 8 and 9)1214-17
In patients with INO the contralateral ab-ducting eye will usually exhibit a disassociatedhorizontal nystagmus although this does notalways occur6 One hypothesis to explain ab-duction nystagmus implicates an adaptive re-sponse to overcome the weakness of the
Figure 5 Pathways involved in the counterroll of the eyes (dotted arrows) duringa head tilt
In this example a left head tilt results in a counterclockwise (with respect to the examiner)torsional counterroll of the upper poles of the eyes This response is mediated by a crossedotolith projection to the extorters in the patientrsquos right eye (the inferior oblique and inferiorrectus muscles) and a double crossed projection to the intorters of the left eye (the superioroblique and superior rectus muscles) These slow phases are punctuated by torsional fastphases that are mediated by the rostral interstitial nucleus of the medial longitudinal fascicu-lus The interstitial nucleus of Cajal (INC) is also shown (without connections) This importantmidbrain structure contains circuitry important for neural integration of vertical and torsionalgaze eye-head coordination during roll movements and contains inhibitory burst neurons forvertical eye movements3 Lesions of these otolith projections result in the opposite reciprocaleffects leading to intorsion and elevation of the right eye and extorsion and depression of theleft eye the so-called skew deviation If the lesion occurs prior to the otolith pathway de-cussation (here on the left) then the lower left eye is on the side of the lesion Alternately ifthe lesion is within this pathway after the decussation (in the pons or midbrain) then thehigher eye is on the side of the lesion
Neurology 70 April 22 2008 e61
contralateral medial rectus6 This is explainedby Heringrsquos law of equal innervation whichstates that attempts to increase innervation tothe weak muscle in one eye must be accompa-nied by a commensurate increase in innervationto the yoke muscle in the other eye Subclinicalnystagmus in the adducting eye (not appreci-ated on bedside examination) has been demon-strated with electro-ocular techniques1819
NEUROPHYSIOLOGY OF INO The diagnosis ofINO can now be precisely confirmed neurophysi-ologically by a number of eye movement trackingtechniques such as infrared oculography18-24
These techniques can identify a variety of abnor-malities in patients with INO including slowingof adduction saccades abduction nystagmus anddiminished adduction saccadic amplitude (figure10) The ratio of saccade metrics between the ab-ducting and adducting eyes the versional discon-jugacy index (VDI) can be measured by infraredoculography and represents a sensitive measure ofthe disconjugacy seen in patients with INO21-23
We have recently defined quantitative oculo-graphic diagnostic criteria for confirming thepresence and severity of INO utilizing a VDI ve-locity Z-score methodology in order to comparepatients with multiple sclerosis (MS) with INOwith a normal control reference population23
Further we have defined a new amplitude mea-sure of disconjugacy in INO the first-pass ampli-tude (FPA)24 The FPA is the ratio of theabductingadducting eye at the point where theabducting eye first achieves the eccentric visualtarget (figure 10)
In the most subtle form of INO the range ofadduction is normal whereas only the velocity isreduced This mild form of INO can often beoverlooked on clinical examination and may onlybe evident on formal oculographic recording Inone study more than 80 of patients with MSwith INO had only slight or no restriction of ad-duction25 Neurologic examination for detectingthe subtle adduction lag INO can be improved bythe use of an optokinetic tape
In a recent study we assessed the accuracy ofclinical detection of INO by 279 physician evalua-tors who were asked to identify the syndromewhen viewing a video of 18 subjects (some ofwhom had unilateral or bilateral INO of varyingseverity and normal subjects without INO)19
The utilization of infrared oculography allowedus to validate the presence of this syndrome byspecific criteria and to quantitatively characterizethe relationship between the severity of the syn-drome and the accuracy of clinical detection Thedetection rates were highly accurate across all
Figure 6 Another consequence of otolithic imbalance that accompanies skewdeviation is the phenomenon of ocular counterroll
These fundus photographs show the extorsion (upper pole of the eye rotated away from thenose or toward the left shoulder) of the left eye (OS) with the disc-macular line rotated clock-wise (according to the examiner) and the right eye (OD) intorted (upper pole of the eye towardthe nose or toward the left shoulder) with the macular-disc line rotated clockwise (againaccording to the examiner) A lesion within the otolith projections in the medial longitudinalfasciculus at the level of the left medulla (the side of the lower eye) or right pons or midbrain(side of the higher eye) would result in this appearance
Figure 7 A patient with a marked skew deviationand symptomatic complaints ofvertical diplopia
Note the severe vertical misalignment of the two eyes Thisabnormality is the consequence of otolith disruption and issupranuclear in mechanism (ductions were intact for all indi-vidual eye muscles)
Figure 8 One of our patients with multiplesclerosis had a dorsal midbrainsyndrome that included a lefthyperdeviation consistent withskew deviation and a leftinternuclear ophthalmoparesis (onattempted right gaze as seen in thelower figure)
The lesion was at the level of the left midbrain (after the de-cussation of the rightward originating otolith pathways) andinvolved the medial longitudinal fasciculus Also note the en-larged left pupil which exhibited the characteristics of near-light dissociation
e62 Neurology 70 April 22 2008
physician groups when the degree of adductionslowing was severe Alternately milder cases ofINO were frequently not identified by the major-ity of evaluators
Most demyelinating lesions of the MLF are lo-cated in the pons or midbrain often sparing thevergence pathways including the fibers project-ing from the medial rectus subnucleus of cranialnerve III2 As a result convergence is intact in themajority of patients despite adduction weaknesson lateral gaze This finding can help distinguishan INO from partial third nerve palsy Furtherthe two eyes are typically well aligned in the pri-mary position (nearly orthophoric or slightly exo-phoric on cross cover testing with one eyeviewing) compared to third nerve palsies whichcommonly produce a conspicuous exotropia (amisalignment with both eyes viewing) along withabnormalities of the eyelid and pupil and otherextraocular muscles
INO can produce a modest slowing of abduc-tion as well as adduction in the same affectedeye2 In an extreme example it has been reportedthat a complete horizontal monocular failure ofeye movement can occur (affecting the ipsilateralmedial longitudinal fasciculus and possibly theabducens nerve fascicle as well) in associationwith a dorsolateral pontine tegmentum lesion asthe first event of MS26
INO SYNDROMES One-and-a-half syndromeThis syndrome consists of a gaze palsy in one direc-tion with an INO when executing a saccade to theopposite side It is produced by damage to the PPRFor abducens nucleus and the MLF on the same sidewithin the pontine tegmentum27 Convergence isgenerally spared as cranial nerve III is spared bilater-ally Given the preserved abduction of the eye con-tralateral to the lesion one commonly observes aprimary position exotropia also known as paralyticpontine exotropia (figure 11)28
Wall-eyed bilateral INO syndrome If the lesion af-fects the MLF within the pons or midbrain ver-gence pathways and the oculomotor apparatuscan be coincidentally disrupted resulting in a va-riety of eye movement abnormalities that includeimpaired convergence29 These lesions are typi-cally bilateral and produce divergence of the eyes(wall-eyed) (figure 12)
INO and trochlear syndrome A highly unusualsyndrome involves a unilateral lesion of the MLFat the level of the caudal midbrain with extensioninto the trochlear nucleus on the same side30
This lesion produces an INO and contralateralhyperdeviation secondary to a IV nerve palsy (re-member the trochlear nerve exits and decussatesto innervate the opposite side superior obliquemuscle) This syndrome can be confused with a
Figure 9 Volitional saccadic pathway with alesion in the right medial longitudinalfasciculus (MLF) that results in aninternuclear ophthalmoparesis (INO)
Volitional saccadic pathway with a lesion in the right MLFthat results in an INO during an attempted saccade to thepatientrsquos left
Figure 10 Infrared oculogram derived from a patient with multiple sclerosiswith bilateral internuclear ophthalmoparesis
In this case a rightward (upward tracing) 20 deg saccade results in interocular disconjugacy(note separation of the two tracings) Observe that the right eye (OD in blue) achieves the 20deg target rapidly whereas the left eye (OS in red) lags behind The ratio of the eyes when theabducting right eye achieves the target to the position of the adducting eye at that time isreferred to as the first pass amplitude (FPA) Ultimately both eyes achieve the fixation targetthe final amplitude (FA) During the trajectory of the saccade the divergence of the two eyescan result in loss of stereoscopy diplopia (transiently) difficulty reading visual blur and riskof fall while turning or motor vehicle accident with head turning while driving
Neurology 70 April 22 2008 e63
skew deviation however in the case of INO andskew deviation the hyperdeviation is generally onthe side of the INO
ABNORMAL VERTICAL EYE MOVEMENTSWITH MLF LESIONS The MLF contains path-ways involved in the regulation of vertical pur-suit vertical vestibular signals and vertical
alignment2931-33 Patients with INO will thereforeoften exhibit abnormalities with vertical eyemovements including the following diminishedvertical gaze holding abnormal optokinetic andpursuit responses decreased vertical VOR gainvertical gaze-evoked nystagmus convergent-retraction nystagmus decreased vertical smoothpursuit and skew deviation
CLINICAL MANIFESTATIONS OF INO The clin-ical manifestations associated with INO includediplopia (typically horizontal binocular) visualconfusion the illusion of environmental move-ment during horizontal saccades (oscillopsia)vertigo and blurring of visual image acuity par-ticularly with reading2 A less conspicuous butpotentially dangerous feature includes worseningdisconjugacy and a resultant break in binocularfusion during head active turning (which pro-duces a contraversive slow phase punctuated bysaccades in the direction of head movement)while head turning during driving (eg changinglanes) and while ambulating
RADIOGRAPHIC IDENTIFICATION OF MLFLESIONS Several pathologic studies have showna clear anatomic relationship between the pres-ence of lesions along the ipsilateral MLF and thepresence of INO114-17 Due to its high spatial reso-lution MRI has allowed us to depict in vivo theanatomic organization of the human oculomotornerve complex theMLF and related structures inthe brainstem (typically white matter tracts havelow signal intensity and nuclei have higher signalintensity)34 Moreover MRI has also contributedto a better understanding of the different stages ofmyelination of these structures in the pretermbrain35
In patients with INO MRI has shown hyper-intense lesions in the region of the MLF on T2-weighted images that were not detected usingCT36 T2-hyperintensities in the pontine and mid-brain tegmentum portion of the MLF have beenshown in a high percentage of patients with INOderived from different neurologic disorders (fig-ure 13) In one study involving 58 patients withMS with INO MRI with proton density imagingdetected a higher percentage of MLF involvement(100) than T2 (88) and fast-FLAIR (48)37
We have recently studied the relationship be-tween the severity of INO and correspondingmeasures of brain tissue injury within the MLFderived from the advanced neuroradiologic tech-niques diffusion tensor imaging and magnetiza-tion transfer imaging38 The application ofneurophysiologic methods in the quantitative
Figure 11 An example of the one-and-a-half syndrome in one of our patientswith multiple sclerosis
The patient was unable to elicit saccades to the right (ie a right gaze palsy) and had evi-dence of a right internuclear ophthalmoparesis (INO) upon attempted gaze to the left In thisphotograph the patient is looking straight ahead We can observe an exotropia the so-calledparalytic pontine exotropia with the left eye in exo (the only remaining movement possible) Inthis circumstance there is an attempted leftward preference However only left eye abduc-tion is possible given the right INO (with slowing and significant ocular limitation) Below is theT2-weighted axial MRI showing the responsible lesion involving the right pontine tegmentum(arrow)
Figure 12 The syndrome of wall-eyed bilateralinternuclear ophthalmoparesis(INO) in an patient with multiplesclerosis with progressive diseaseand a history of a severeinflammatory demyelinatingsyndrome involving thetegmentum of the ponto-mesencephalic junction whichaffected the medial longitudinalfasciculus (MLF) bilaterally
Note the exotropic appearance of both eyes (ie wall-eyed)Attempted gaze to the right or left revealed adduction slow-ing and limitation consistent with bilateral INO There wasalso reduced vertical smooth pursuit and vertical vestibulo-ocular reflexes (both pathways course through the MLF)
e64 Neurology 70 April 22 2008
analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

tivum to the oculomotor nuclei Thus threepathways may contribute to the generation of eyemovements during stimulation of the anteriorsemicircular canal
Posterior semicircular canal projections in the MLFFor the posterior canal system excitatory neu-rons project from the vestibular nuclei at the junc-tion of the MVN and VLVN rostrally mediallyand dorsally through MVN until at the level ofthe caudal abducens nucleus they turn mediallyand cross the midline beneath the nucleus prep-ositus hypoglossi (NPH) and abducens nucleusventral to the MLF After crossing the midlinethey enter the MLF and project rostrally to thetrochlear nucleus and inferior rectus subdivisionof the oculomotor complex5 The trochlear axonswithin cranial nerve IV then exit the brainstemposteriorly (the only cranial nerve to do so) andcompletely decussate before projecting forwardto innervate the superior oblique muscle (on theside of posterior canal activation) (figure 4) In-hibitory neurons subserving the posterior semicir-cular canals are found in the SVN and rostral
MVN Their axons project through the pontinereticular formation to reach the ipsilateral MLFand then contact the superior rectus and inferioroblique subdivisions of the oculomotor complexin order to avoid movements antagonistic tothose mediated by the posterior canal system
An important clinical implication of the differ-ence in anatomic projections of the posterior andanterior canal pathways is that patients withMLF lesions may have a dissociated vertical nys-tagmus and relative sparing of response to up-ward vs downward rotation of the head67
Otolithic projections in the MLF The otolith or-gans detect linear acceleration The projectionsfrom the vestibular nuclei that mediate otolith-ocular reflexes are less well defined and there is apaucity of evidence for a direct three neuron arc(eg otolith organ vestibular nucleus ocularmotor neuron) comparable to the three neuronarc for semicircular canal mediated reflexes Pre-sumably the horizontal translational VOR is me-diated by the same abducens nucleus pathway asare the other conjugate systems though there issome evidence for a direct projection of utricularafferents to the abducens nucleus
Responses to static head tilt especially lateraltilt of the head (ear to shoulder) have been longknown to produce ocular counterrolling due toactivation of the cyclovertical ocular muscles8
Under normal circumstances when the head istilted to the left the eyes counterroll in the oppo-site direction (upper poles of the eyes slowly mov-ing away from the side of the tilt) This reflex ismediated by projections that innervate the left eyeintorters (superior rectus and superior oblique)and the right eye extorters (inferior rectus and in-ferior oblique) (figure 5) Following the slowphase counterroll there is a fast torsional move-ment in the opposite direction (upper poles beat-ing to the side of the head tilt) which is mediatedby the riMLF in the rostral midbrain9
Anatomically these graviceptive pathwayscross to the other side of the brainstem approxi-mately in the middle of the pons and further as-cend in the MLF to the ocular motor nuclei(nuclei III and IV) and the premotor gaze centersin the rostra1 midbrain (interstitial nucleus of Ca-jal [INC] and riMLF)10 From there further con-nections reach multiple cortical areas throughthalamic projections
A common clinical finding in patients withunilateral MLF lesions involving the central oto-lith pathway is the ocular tilt reaction (OTR)which consists of a head tilt ocular counter-rolling (generally with the upper pole of the eyes
Figure 4 Projections from the left posteriorsemicircular canal
Axons from the canal project to the ipsilateral vestibular nu-clei and then decussate to innervate the contralateral infe-rior rectus subnucleus of the oculomotor complex of cranialnerve III and the trochlear nucleus The trochlear neuronsthen exit the brainstem posteriorly and decussate back tothe left side innervating the superior oblique muscle Activa-tion of both canals (as with pitching the head upward andattempting straight ahead fixation) will result in cancellationof the torsional vector components but addition of the verti-cal vector components resulting in downward movement ofthe eyes
e60 Neurology 70 April 22 2008
rotating toward a lesion below the pons and awayfrom a lesion at the level of the pons or midbrain)and skew deviation (a supranuclear vertical mis-alignment of the two eyes)11 The head tilt is typi-cally away from the side of the higher eye
In typical skew deviations the higher eye iscontralateral to a medullary lesion and ipsilateralto a mid pontine (the level at which otolith projec-tions decussate the brainstem) or midbrain lesionOcular counterroll may be recognized during fun-duscopic examination where the nearly horizon-tal plane between the optic disc and macula (themacula-disc line) is now deviated12 For examplein the case of a left lateral medullary syndromean ocular tilt reaction might involve left head tiltright hyperdeviation and counterroll of the eyes
(upper poles) toward the left shoulder (or clock-wise rotation with respect to the observer) In es-sence the macula of the left eye is now furtherbelow the disc than usual and the macula of theright eye is further above the disc (figure 6)
Tilting the head relative to gravity from up-right in an ear-down direction so called head rollelicits dissociated changes of eye position Inhealthy subjects both eyes counterroll (upperpoles of the eyes moving away from the side of thehead tilt) by roughly 10 of the head roll but theextorting eye rotates about 1 to 2 deg more thanthe intorting eye (figure 5)813 Furthermore asmall skew deviation (vertical misalignment) ofabout 05 deg appears with hypertropia of the in-torting eye10
Unilateral peripheral or pontomedullary le-sions below the pontine crossing of the gravicep-tive pathways produce a skew deviation andbinocular torsion (combination of these signs issometimes called skew torsion) For instance apatient with a left medullary lesion will have aright hypertropia and counterroll of the eyes to-ward the left shoulder (figure 7) Lesions of thelower graviceptive pathways tend to produce dis-conjugate torsion which is typically greatest inthe excyclotorted eye In contrast a unilateralpontomesencephalic brainstem lesion leads tocontraversive skew torsion10 In this case the hy-pertropic eye is ipsilateral to the lesion and theocular torsion is usually conjugate and to theshoulder opposite the side of the lesion If skewtorsion is associated with a head tilt in the direc-tion of the lower eye this configuration of clinicalsigns is called ocular tilt reaction Since bothgraviceptive pathways and internuclear connec-tions between ocular motor nuclei travel alongthe MLF skew torsion due to pontomesence-phalic lesions is frequently associated with inter-nuclear ophthalmoparesis (INO) (see INOsection)2 The hypertropic eye is generally on theside of the INO (figure 8)
INTERNUCLEAR OPHTHALMOPARESIS Themost commonly recognized syndrome that resultsfromMLF damage is INO and is characterized byslowing or limitation of adduction (on the sameside as the MLF lesion) during horizontal eyemovements (figures 8 and 9)1214-17
In patients with INO the contralateral ab-ducting eye will usually exhibit a disassociatedhorizontal nystagmus although this does notalways occur6 One hypothesis to explain ab-duction nystagmus implicates an adaptive re-sponse to overcome the weakness of the
Figure 5 Pathways involved in the counterroll of the eyes (dotted arrows) duringa head tilt
In this example a left head tilt results in a counterclockwise (with respect to the examiner)torsional counterroll of the upper poles of the eyes This response is mediated by a crossedotolith projection to the extorters in the patientrsquos right eye (the inferior oblique and inferiorrectus muscles) and a double crossed projection to the intorters of the left eye (the superioroblique and superior rectus muscles) These slow phases are punctuated by torsional fastphases that are mediated by the rostral interstitial nucleus of the medial longitudinal fascicu-lus The interstitial nucleus of Cajal (INC) is also shown (without connections) This importantmidbrain structure contains circuitry important for neural integration of vertical and torsionalgaze eye-head coordination during roll movements and contains inhibitory burst neurons forvertical eye movements3 Lesions of these otolith projections result in the opposite reciprocaleffects leading to intorsion and elevation of the right eye and extorsion and depression of theleft eye the so-called skew deviation If the lesion occurs prior to the otolith pathway de-cussation (here on the left) then the lower left eye is on the side of the lesion Alternately ifthe lesion is within this pathway after the decussation (in the pons or midbrain) then thehigher eye is on the side of the lesion
Neurology 70 April 22 2008 e61
contralateral medial rectus6 This is explainedby Heringrsquos law of equal innervation whichstates that attempts to increase innervation tothe weak muscle in one eye must be accompa-nied by a commensurate increase in innervationto the yoke muscle in the other eye Subclinicalnystagmus in the adducting eye (not appreci-ated on bedside examination) has been demon-strated with electro-ocular techniques1819
NEUROPHYSIOLOGY OF INO The diagnosis ofINO can now be precisely confirmed neurophysi-ologically by a number of eye movement trackingtechniques such as infrared oculography18-24
These techniques can identify a variety of abnor-malities in patients with INO including slowingof adduction saccades abduction nystagmus anddiminished adduction saccadic amplitude (figure10) The ratio of saccade metrics between the ab-ducting and adducting eyes the versional discon-jugacy index (VDI) can be measured by infraredoculography and represents a sensitive measure ofthe disconjugacy seen in patients with INO21-23
We have recently defined quantitative oculo-graphic diagnostic criteria for confirming thepresence and severity of INO utilizing a VDI ve-locity Z-score methodology in order to comparepatients with multiple sclerosis (MS) with INOwith a normal control reference population23
Further we have defined a new amplitude mea-sure of disconjugacy in INO the first-pass ampli-tude (FPA)24 The FPA is the ratio of theabductingadducting eye at the point where theabducting eye first achieves the eccentric visualtarget (figure 10)
In the most subtle form of INO the range ofadduction is normal whereas only the velocity isreduced This mild form of INO can often beoverlooked on clinical examination and may onlybe evident on formal oculographic recording Inone study more than 80 of patients with MSwith INO had only slight or no restriction of ad-duction25 Neurologic examination for detectingthe subtle adduction lag INO can be improved bythe use of an optokinetic tape
In a recent study we assessed the accuracy ofclinical detection of INO by 279 physician evalua-tors who were asked to identify the syndromewhen viewing a video of 18 subjects (some ofwhom had unilateral or bilateral INO of varyingseverity and normal subjects without INO)19
The utilization of infrared oculography allowedus to validate the presence of this syndrome byspecific criteria and to quantitatively characterizethe relationship between the severity of the syn-drome and the accuracy of clinical detection Thedetection rates were highly accurate across all
Figure 6 Another consequence of otolithic imbalance that accompanies skewdeviation is the phenomenon of ocular counterroll
These fundus photographs show the extorsion (upper pole of the eye rotated away from thenose or toward the left shoulder) of the left eye (OS) with the disc-macular line rotated clock-wise (according to the examiner) and the right eye (OD) intorted (upper pole of the eye towardthe nose or toward the left shoulder) with the macular-disc line rotated clockwise (againaccording to the examiner) A lesion within the otolith projections in the medial longitudinalfasciculus at the level of the left medulla (the side of the lower eye) or right pons or midbrain(side of the higher eye) would result in this appearance
Figure 7 A patient with a marked skew deviationand symptomatic complaints ofvertical diplopia
Note the severe vertical misalignment of the two eyes Thisabnormality is the consequence of otolith disruption and issupranuclear in mechanism (ductions were intact for all indi-vidual eye muscles)
Figure 8 One of our patients with multiplesclerosis had a dorsal midbrainsyndrome that included a lefthyperdeviation consistent withskew deviation and a leftinternuclear ophthalmoparesis (onattempted right gaze as seen in thelower figure)
The lesion was at the level of the left midbrain (after the de-cussation of the rightward originating otolith pathways) andinvolved the medial longitudinal fasciculus Also note the en-larged left pupil which exhibited the characteristics of near-light dissociation
e62 Neurology 70 April 22 2008
physician groups when the degree of adductionslowing was severe Alternately milder cases ofINO were frequently not identified by the major-ity of evaluators
Most demyelinating lesions of the MLF are lo-cated in the pons or midbrain often sparing thevergence pathways including the fibers project-ing from the medial rectus subnucleus of cranialnerve III2 As a result convergence is intact in themajority of patients despite adduction weaknesson lateral gaze This finding can help distinguishan INO from partial third nerve palsy Furtherthe two eyes are typically well aligned in the pri-mary position (nearly orthophoric or slightly exo-phoric on cross cover testing with one eyeviewing) compared to third nerve palsies whichcommonly produce a conspicuous exotropia (amisalignment with both eyes viewing) along withabnormalities of the eyelid and pupil and otherextraocular muscles
INO can produce a modest slowing of abduc-tion as well as adduction in the same affectedeye2 In an extreme example it has been reportedthat a complete horizontal monocular failure ofeye movement can occur (affecting the ipsilateralmedial longitudinal fasciculus and possibly theabducens nerve fascicle as well) in associationwith a dorsolateral pontine tegmentum lesion asthe first event of MS26
INO SYNDROMES One-and-a-half syndromeThis syndrome consists of a gaze palsy in one direc-tion with an INO when executing a saccade to theopposite side It is produced by damage to the PPRFor abducens nucleus and the MLF on the same sidewithin the pontine tegmentum27 Convergence isgenerally spared as cranial nerve III is spared bilater-ally Given the preserved abduction of the eye con-tralateral to the lesion one commonly observes aprimary position exotropia also known as paralyticpontine exotropia (figure 11)28
Wall-eyed bilateral INO syndrome If the lesion af-fects the MLF within the pons or midbrain ver-gence pathways and the oculomotor apparatuscan be coincidentally disrupted resulting in a va-riety of eye movement abnormalities that includeimpaired convergence29 These lesions are typi-cally bilateral and produce divergence of the eyes(wall-eyed) (figure 12)
INO and trochlear syndrome A highly unusualsyndrome involves a unilateral lesion of the MLFat the level of the caudal midbrain with extensioninto the trochlear nucleus on the same side30
This lesion produces an INO and contralateralhyperdeviation secondary to a IV nerve palsy (re-member the trochlear nerve exits and decussatesto innervate the opposite side superior obliquemuscle) This syndrome can be confused with a
Figure 9 Volitional saccadic pathway with alesion in the right medial longitudinalfasciculus (MLF) that results in aninternuclear ophthalmoparesis (INO)
Volitional saccadic pathway with a lesion in the right MLFthat results in an INO during an attempted saccade to thepatientrsquos left
Figure 10 Infrared oculogram derived from a patient with multiple sclerosiswith bilateral internuclear ophthalmoparesis
In this case a rightward (upward tracing) 20 deg saccade results in interocular disconjugacy(note separation of the two tracings) Observe that the right eye (OD in blue) achieves the 20deg target rapidly whereas the left eye (OS in red) lags behind The ratio of the eyes when theabducting right eye achieves the target to the position of the adducting eye at that time isreferred to as the first pass amplitude (FPA) Ultimately both eyes achieve the fixation targetthe final amplitude (FA) During the trajectory of the saccade the divergence of the two eyescan result in loss of stereoscopy diplopia (transiently) difficulty reading visual blur and riskof fall while turning or motor vehicle accident with head turning while driving
Neurology 70 April 22 2008 e63
skew deviation however in the case of INO andskew deviation the hyperdeviation is generally onthe side of the INO
ABNORMAL VERTICAL EYE MOVEMENTSWITH MLF LESIONS The MLF contains path-ways involved in the regulation of vertical pur-suit vertical vestibular signals and vertical
alignment2931-33 Patients with INO will thereforeoften exhibit abnormalities with vertical eyemovements including the following diminishedvertical gaze holding abnormal optokinetic andpursuit responses decreased vertical VOR gainvertical gaze-evoked nystagmus convergent-retraction nystagmus decreased vertical smoothpursuit and skew deviation
CLINICAL MANIFESTATIONS OF INO The clin-ical manifestations associated with INO includediplopia (typically horizontal binocular) visualconfusion the illusion of environmental move-ment during horizontal saccades (oscillopsia)vertigo and blurring of visual image acuity par-ticularly with reading2 A less conspicuous butpotentially dangerous feature includes worseningdisconjugacy and a resultant break in binocularfusion during head active turning (which pro-duces a contraversive slow phase punctuated bysaccades in the direction of head movement)while head turning during driving (eg changinglanes) and while ambulating
RADIOGRAPHIC IDENTIFICATION OF MLFLESIONS Several pathologic studies have showna clear anatomic relationship between the pres-ence of lesions along the ipsilateral MLF and thepresence of INO114-17 Due to its high spatial reso-lution MRI has allowed us to depict in vivo theanatomic organization of the human oculomotornerve complex theMLF and related structures inthe brainstem (typically white matter tracts havelow signal intensity and nuclei have higher signalintensity)34 Moreover MRI has also contributedto a better understanding of the different stages ofmyelination of these structures in the pretermbrain35
In patients with INO MRI has shown hyper-intense lesions in the region of the MLF on T2-weighted images that were not detected usingCT36 T2-hyperintensities in the pontine and mid-brain tegmentum portion of the MLF have beenshown in a high percentage of patients with INOderived from different neurologic disorders (fig-ure 13) In one study involving 58 patients withMS with INO MRI with proton density imagingdetected a higher percentage of MLF involvement(100) than T2 (88) and fast-FLAIR (48)37
We have recently studied the relationship be-tween the severity of INO and correspondingmeasures of brain tissue injury within the MLFderived from the advanced neuroradiologic tech-niques diffusion tensor imaging and magnetiza-tion transfer imaging38 The application ofneurophysiologic methods in the quantitative
Figure 11 An example of the one-and-a-half syndrome in one of our patientswith multiple sclerosis
The patient was unable to elicit saccades to the right (ie a right gaze palsy) and had evi-dence of a right internuclear ophthalmoparesis (INO) upon attempted gaze to the left In thisphotograph the patient is looking straight ahead We can observe an exotropia the so-calledparalytic pontine exotropia with the left eye in exo (the only remaining movement possible) Inthis circumstance there is an attempted leftward preference However only left eye abduc-tion is possible given the right INO (with slowing and significant ocular limitation) Below is theT2-weighted axial MRI showing the responsible lesion involving the right pontine tegmentum(arrow)
Figure 12 The syndrome of wall-eyed bilateralinternuclear ophthalmoparesis(INO) in an patient with multiplesclerosis with progressive diseaseand a history of a severeinflammatory demyelinatingsyndrome involving thetegmentum of the ponto-mesencephalic junction whichaffected the medial longitudinalfasciculus (MLF) bilaterally
Note the exotropic appearance of both eyes (ie wall-eyed)Attempted gaze to the right or left revealed adduction slow-ing and limitation consistent with bilateral INO There wasalso reduced vertical smooth pursuit and vertical vestibulo-ocular reflexes (both pathways course through the MLF)
e64 Neurology 70 April 22 2008
analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

rotating toward a lesion below the pons and awayfrom a lesion at the level of the pons or midbrain)and skew deviation (a supranuclear vertical mis-alignment of the two eyes)11 The head tilt is typi-cally away from the side of the higher eye
In typical skew deviations the higher eye iscontralateral to a medullary lesion and ipsilateralto a mid pontine (the level at which otolith projec-tions decussate the brainstem) or midbrain lesionOcular counterroll may be recognized during fun-duscopic examination where the nearly horizon-tal plane between the optic disc and macula (themacula-disc line) is now deviated12 For examplein the case of a left lateral medullary syndromean ocular tilt reaction might involve left head tiltright hyperdeviation and counterroll of the eyes
(upper poles) toward the left shoulder (or clock-wise rotation with respect to the observer) In es-sence the macula of the left eye is now furtherbelow the disc than usual and the macula of theright eye is further above the disc (figure 6)
Tilting the head relative to gravity from up-right in an ear-down direction so called head rollelicits dissociated changes of eye position Inhealthy subjects both eyes counterroll (upperpoles of the eyes moving away from the side of thehead tilt) by roughly 10 of the head roll but theextorting eye rotates about 1 to 2 deg more thanthe intorting eye (figure 5)813 Furthermore asmall skew deviation (vertical misalignment) ofabout 05 deg appears with hypertropia of the in-torting eye10
Unilateral peripheral or pontomedullary le-sions below the pontine crossing of the gravicep-tive pathways produce a skew deviation andbinocular torsion (combination of these signs issometimes called skew torsion) For instance apatient with a left medullary lesion will have aright hypertropia and counterroll of the eyes to-ward the left shoulder (figure 7) Lesions of thelower graviceptive pathways tend to produce dis-conjugate torsion which is typically greatest inthe excyclotorted eye In contrast a unilateralpontomesencephalic brainstem lesion leads tocontraversive skew torsion10 In this case the hy-pertropic eye is ipsilateral to the lesion and theocular torsion is usually conjugate and to theshoulder opposite the side of the lesion If skewtorsion is associated with a head tilt in the direc-tion of the lower eye this configuration of clinicalsigns is called ocular tilt reaction Since bothgraviceptive pathways and internuclear connec-tions between ocular motor nuclei travel alongthe MLF skew torsion due to pontomesence-phalic lesions is frequently associated with inter-nuclear ophthalmoparesis (INO) (see INOsection)2 The hypertropic eye is generally on theside of the INO (figure 8)
INTERNUCLEAR OPHTHALMOPARESIS Themost commonly recognized syndrome that resultsfromMLF damage is INO and is characterized byslowing or limitation of adduction (on the sameside as the MLF lesion) during horizontal eyemovements (figures 8 and 9)1214-17
In patients with INO the contralateral ab-ducting eye will usually exhibit a disassociatedhorizontal nystagmus although this does notalways occur6 One hypothesis to explain ab-duction nystagmus implicates an adaptive re-sponse to overcome the weakness of the
Figure 5 Pathways involved in the counterroll of the eyes (dotted arrows) duringa head tilt
In this example a left head tilt results in a counterclockwise (with respect to the examiner)torsional counterroll of the upper poles of the eyes This response is mediated by a crossedotolith projection to the extorters in the patientrsquos right eye (the inferior oblique and inferiorrectus muscles) and a double crossed projection to the intorters of the left eye (the superioroblique and superior rectus muscles) These slow phases are punctuated by torsional fastphases that are mediated by the rostral interstitial nucleus of the medial longitudinal fascicu-lus The interstitial nucleus of Cajal (INC) is also shown (without connections) This importantmidbrain structure contains circuitry important for neural integration of vertical and torsionalgaze eye-head coordination during roll movements and contains inhibitory burst neurons forvertical eye movements3 Lesions of these otolith projections result in the opposite reciprocaleffects leading to intorsion and elevation of the right eye and extorsion and depression of theleft eye the so-called skew deviation If the lesion occurs prior to the otolith pathway de-cussation (here on the left) then the lower left eye is on the side of the lesion Alternately ifthe lesion is within this pathway after the decussation (in the pons or midbrain) then thehigher eye is on the side of the lesion
Neurology 70 April 22 2008 e61
contralateral medial rectus6 This is explainedby Heringrsquos law of equal innervation whichstates that attempts to increase innervation tothe weak muscle in one eye must be accompa-nied by a commensurate increase in innervationto the yoke muscle in the other eye Subclinicalnystagmus in the adducting eye (not appreci-ated on bedside examination) has been demon-strated with electro-ocular techniques1819
NEUROPHYSIOLOGY OF INO The diagnosis ofINO can now be precisely confirmed neurophysi-ologically by a number of eye movement trackingtechniques such as infrared oculography18-24
These techniques can identify a variety of abnor-malities in patients with INO including slowingof adduction saccades abduction nystagmus anddiminished adduction saccadic amplitude (figure10) The ratio of saccade metrics between the ab-ducting and adducting eyes the versional discon-jugacy index (VDI) can be measured by infraredoculography and represents a sensitive measure ofthe disconjugacy seen in patients with INO21-23
We have recently defined quantitative oculo-graphic diagnostic criteria for confirming thepresence and severity of INO utilizing a VDI ve-locity Z-score methodology in order to comparepatients with multiple sclerosis (MS) with INOwith a normal control reference population23
Further we have defined a new amplitude mea-sure of disconjugacy in INO the first-pass ampli-tude (FPA)24 The FPA is the ratio of theabductingadducting eye at the point where theabducting eye first achieves the eccentric visualtarget (figure 10)
In the most subtle form of INO the range ofadduction is normal whereas only the velocity isreduced This mild form of INO can often beoverlooked on clinical examination and may onlybe evident on formal oculographic recording Inone study more than 80 of patients with MSwith INO had only slight or no restriction of ad-duction25 Neurologic examination for detectingthe subtle adduction lag INO can be improved bythe use of an optokinetic tape
In a recent study we assessed the accuracy ofclinical detection of INO by 279 physician evalua-tors who were asked to identify the syndromewhen viewing a video of 18 subjects (some ofwhom had unilateral or bilateral INO of varyingseverity and normal subjects without INO)19
The utilization of infrared oculography allowedus to validate the presence of this syndrome byspecific criteria and to quantitatively characterizethe relationship between the severity of the syn-drome and the accuracy of clinical detection Thedetection rates were highly accurate across all
Figure 6 Another consequence of otolithic imbalance that accompanies skewdeviation is the phenomenon of ocular counterroll
These fundus photographs show the extorsion (upper pole of the eye rotated away from thenose or toward the left shoulder) of the left eye (OS) with the disc-macular line rotated clock-wise (according to the examiner) and the right eye (OD) intorted (upper pole of the eye towardthe nose or toward the left shoulder) with the macular-disc line rotated clockwise (againaccording to the examiner) A lesion within the otolith projections in the medial longitudinalfasciculus at the level of the left medulla (the side of the lower eye) or right pons or midbrain(side of the higher eye) would result in this appearance
Figure 7 A patient with a marked skew deviationand symptomatic complaints ofvertical diplopia
Note the severe vertical misalignment of the two eyes Thisabnormality is the consequence of otolith disruption and issupranuclear in mechanism (ductions were intact for all indi-vidual eye muscles)
Figure 8 One of our patients with multiplesclerosis had a dorsal midbrainsyndrome that included a lefthyperdeviation consistent withskew deviation and a leftinternuclear ophthalmoparesis (onattempted right gaze as seen in thelower figure)
The lesion was at the level of the left midbrain (after the de-cussation of the rightward originating otolith pathways) andinvolved the medial longitudinal fasciculus Also note the en-larged left pupil which exhibited the characteristics of near-light dissociation
e62 Neurology 70 April 22 2008
physician groups when the degree of adductionslowing was severe Alternately milder cases ofINO were frequently not identified by the major-ity of evaluators
Most demyelinating lesions of the MLF are lo-cated in the pons or midbrain often sparing thevergence pathways including the fibers project-ing from the medial rectus subnucleus of cranialnerve III2 As a result convergence is intact in themajority of patients despite adduction weaknesson lateral gaze This finding can help distinguishan INO from partial third nerve palsy Furtherthe two eyes are typically well aligned in the pri-mary position (nearly orthophoric or slightly exo-phoric on cross cover testing with one eyeviewing) compared to third nerve palsies whichcommonly produce a conspicuous exotropia (amisalignment with both eyes viewing) along withabnormalities of the eyelid and pupil and otherextraocular muscles
INO can produce a modest slowing of abduc-tion as well as adduction in the same affectedeye2 In an extreme example it has been reportedthat a complete horizontal monocular failure ofeye movement can occur (affecting the ipsilateralmedial longitudinal fasciculus and possibly theabducens nerve fascicle as well) in associationwith a dorsolateral pontine tegmentum lesion asthe first event of MS26
INO SYNDROMES One-and-a-half syndromeThis syndrome consists of a gaze palsy in one direc-tion with an INO when executing a saccade to theopposite side It is produced by damage to the PPRFor abducens nucleus and the MLF on the same sidewithin the pontine tegmentum27 Convergence isgenerally spared as cranial nerve III is spared bilater-ally Given the preserved abduction of the eye con-tralateral to the lesion one commonly observes aprimary position exotropia also known as paralyticpontine exotropia (figure 11)28
Wall-eyed bilateral INO syndrome If the lesion af-fects the MLF within the pons or midbrain ver-gence pathways and the oculomotor apparatuscan be coincidentally disrupted resulting in a va-riety of eye movement abnormalities that includeimpaired convergence29 These lesions are typi-cally bilateral and produce divergence of the eyes(wall-eyed) (figure 12)
INO and trochlear syndrome A highly unusualsyndrome involves a unilateral lesion of the MLFat the level of the caudal midbrain with extensioninto the trochlear nucleus on the same side30
This lesion produces an INO and contralateralhyperdeviation secondary to a IV nerve palsy (re-member the trochlear nerve exits and decussatesto innervate the opposite side superior obliquemuscle) This syndrome can be confused with a
Figure 9 Volitional saccadic pathway with alesion in the right medial longitudinalfasciculus (MLF) that results in aninternuclear ophthalmoparesis (INO)
Volitional saccadic pathway with a lesion in the right MLFthat results in an INO during an attempted saccade to thepatientrsquos left
Figure 10 Infrared oculogram derived from a patient with multiple sclerosiswith bilateral internuclear ophthalmoparesis
In this case a rightward (upward tracing) 20 deg saccade results in interocular disconjugacy(note separation of the two tracings) Observe that the right eye (OD in blue) achieves the 20deg target rapidly whereas the left eye (OS in red) lags behind The ratio of the eyes when theabducting right eye achieves the target to the position of the adducting eye at that time isreferred to as the first pass amplitude (FPA) Ultimately both eyes achieve the fixation targetthe final amplitude (FA) During the trajectory of the saccade the divergence of the two eyescan result in loss of stereoscopy diplopia (transiently) difficulty reading visual blur and riskof fall while turning or motor vehicle accident with head turning while driving
Neurology 70 April 22 2008 e63
skew deviation however in the case of INO andskew deviation the hyperdeviation is generally onthe side of the INO
ABNORMAL VERTICAL EYE MOVEMENTSWITH MLF LESIONS The MLF contains path-ways involved in the regulation of vertical pur-suit vertical vestibular signals and vertical
alignment2931-33 Patients with INO will thereforeoften exhibit abnormalities with vertical eyemovements including the following diminishedvertical gaze holding abnormal optokinetic andpursuit responses decreased vertical VOR gainvertical gaze-evoked nystagmus convergent-retraction nystagmus decreased vertical smoothpursuit and skew deviation
CLINICAL MANIFESTATIONS OF INO The clin-ical manifestations associated with INO includediplopia (typically horizontal binocular) visualconfusion the illusion of environmental move-ment during horizontal saccades (oscillopsia)vertigo and blurring of visual image acuity par-ticularly with reading2 A less conspicuous butpotentially dangerous feature includes worseningdisconjugacy and a resultant break in binocularfusion during head active turning (which pro-duces a contraversive slow phase punctuated bysaccades in the direction of head movement)while head turning during driving (eg changinglanes) and while ambulating
RADIOGRAPHIC IDENTIFICATION OF MLFLESIONS Several pathologic studies have showna clear anatomic relationship between the pres-ence of lesions along the ipsilateral MLF and thepresence of INO114-17 Due to its high spatial reso-lution MRI has allowed us to depict in vivo theanatomic organization of the human oculomotornerve complex theMLF and related structures inthe brainstem (typically white matter tracts havelow signal intensity and nuclei have higher signalintensity)34 Moreover MRI has also contributedto a better understanding of the different stages ofmyelination of these structures in the pretermbrain35
In patients with INO MRI has shown hyper-intense lesions in the region of the MLF on T2-weighted images that were not detected usingCT36 T2-hyperintensities in the pontine and mid-brain tegmentum portion of the MLF have beenshown in a high percentage of patients with INOderived from different neurologic disorders (fig-ure 13) In one study involving 58 patients withMS with INO MRI with proton density imagingdetected a higher percentage of MLF involvement(100) than T2 (88) and fast-FLAIR (48)37
We have recently studied the relationship be-tween the severity of INO and correspondingmeasures of brain tissue injury within the MLFderived from the advanced neuroradiologic tech-niques diffusion tensor imaging and magnetiza-tion transfer imaging38 The application ofneurophysiologic methods in the quantitative
Figure 11 An example of the one-and-a-half syndrome in one of our patientswith multiple sclerosis
The patient was unable to elicit saccades to the right (ie a right gaze palsy) and had evi-dence of a right internuclear ophthalmoparesis (INO) upon attempted gaze to the left In thisphotograph the patient is looking straight ahead We can observe an exotropia the so-calledparalytic pontine exotropia with the left eye in exo (the only remaining movement possible) Inthis circumstance there is an attempted leftward preference However only left eye abduc-tion is possible given the right INO (with slowing and significant ocular limitation) Below is theT2-weighted axial MRI showing the responsible lesion involving the right pontine tegmentum(arrow)
Figure 12 The syndrome of wall-eyed bilateralinternuclear ophthalmoparesis(INO) in an patient with multiplesclerosis with progressive diseaseand a history of a severeinflammatory demyelinatingsyndrome involving thetegmentum of the ponto-mesencephalic junction whichaffected the medial longitudinalfasciculus (MLF) bilaterally
Note the exotropic appearance of both eyes (ie wall-eyed)Attempted gaze to the right or left revealed adduction slow-ing and limitation consistent with bilateral INO There wasalso reduced vertical smooth pursuit and vertical vestibulo-ocular reflexes (both pathways course through the MLF)
e64 Neurology 70 April 22 2008
analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

contralateral medial rectus6 This is explainedby Heringrsquos law of equal innervation whichstates that attempts to increase innervation tothe weak muscle in one eye must be accompa-nied by a commensurate increase in innervationto the yoke muscle in the other eye Subclinicalnystagmus in the adducting eye (not appreci-ated on bedside examination) has been demon-strated with electro-ocular techniques1819
NEUROPHYSIOLOGY OF INO The diagnosis ofINO can now be precisely confirmed neurophysi-ologically by a number of eye movement trackingtechniques such as infrared oculography18-24
These techniques can identify a variety of abnor-malities in patients with INO including slowingof adduction saccades abduction nystagmus anddiminished adduction saccadic amplitude (figure10) The ratio of saccade metrics between the ab-ducting and adducting eyes the versional discon-jugacy index (VDI) can be measured by infraredoculography and represents a sensitive measure ofthe disconjugacy seen in patients with INO21-23
We have recently defined quantitative oculo-graphic diagnostic criteria for confirming thepresence and severity of INO utilizing a VDI ve-locity Z-score methodology in order to comparepatients with multiple sclerosis (MS) with INOwith a normal control reference population23
Further we have defined a new amplitude mea-sure of disconjugacy in INO the first-pass ampli-tude (FPA)24 The FPA is the ratio of theabductingadducting eye at the point where theabducting eye first achieves the eccentric visualtarget (figure 10)
In the most subtle form of INO the range ofadduction is normal whereas only the velocity isreduced This mild form of INO can often beoverlooked on clinical examination and may onlybe evident on formal oculographic recording Inone study more than 80 of patients with MSwith INO had only slight or no restriction of ad-duction25 Neurologic examination for detectingthe subtle adduction lag INO can be improved bythe use of an optokinetic tape
In a recent study we assessed the accuracy ofclinical detection of INO by 279 physician evalua-tors who were asked to identify the syndromewhen viewing a video of 18 subjects (some ofwhom had unilateral or bilateral INO of varyingseverity and normal subjects without INO)19
The utilization of infrared oculography allowedus to validate the presence of this syndrome byspecific criteria and to quantitatively characterizethe relationship between the severity of the syn-drome and the accuracy of clinical detection Thedetection rates were highly accurate across all
Figure 6 Another consequence of otolithic imbalance that accompanies skewdeviation is the phenomenon of ocular counterroll
These fundus photographs show the extorsion (upper pole of the eye rotated away from thenose or toward the left shoulder) of the left eye (OS) with the disc-macular line rotated clock-wise (according to the examiner) and the right eye (OD) intorted (upper pole of the eye towardthe nose or toward the left shoulder) with the macular-disc line rotated clockwise (againaccording to the examiner) A lesion within the otolith projections in the medial longitudinalfasciculus at the level of the left medulla (the side of the lower eye) or right pons or midbrain(side of the higher eye) would result in this appearance
Figure 7 A patient with a marked skew deviationand symptomatic complaints ofvertical diplopia
Note the severe vertical misalignment of the two eyes Thisabnormality is the consequence of otolith disruption and issupranuclear in mechanism (ductions were intact for all indi-vidual eye muscles)
Figure 8 One of our patients with multiplesclerosis had a dorsal midbrainsyndrome that included a lefthyperdeviation consistent withskew deviation and a leftinternuclear ophthalmoparesis (onattempted right gaze as seen in thelower figure)
The lesion was at the level of the left midbrain (after the de-cussation of the rightward originating otolith pathways) andinvolved the medial longitudinal fasciculus Also note the en-larged left pupil which exhibited the characteristics of near-light dissociation
e62 Neurology 70 April 22 2008
physician groups when the degree of adductionslowing was severe Alternately milder cases ofINO were frequently not identified by the major-ity of evaluators
Most demyelinating lesions of the MLF are lo-cated in the pons or midbrain often sparing thevergence pathways including the fibers project-ing from the medial rectus subnucleus of cranialnerve III2 As a result convergence is intact in themajority of patients despite adduction weaknesson lateral gaze This finding can help distinguishan INO from partial third nerve palsy Furtherthe two eyes are typically well aligned in the pri-mary position (nearly orthophoric or slightly exo-phoric on cross cover testing with one eyeviewing) compared to third nerve palsies whichcommonly produce a conspicuous exotropia (amisalignment with both eyes viewing) along withabnormalities of the eyelid and pupil and otherextraocular muscles
INO can produce a modest slowing of abduc-tion as well as adduction in the same affectedeye2 In an extreme example it has been reportedthat a complete horizontal monocular failure ofeye movement can occur (affecting the ipsilateralmedial longitudinal fasciculus and possibly theabducens nerve fascicle as well) in associationwith a dorsolateral pontine tegmentum lesion asthe first event of MS26
INO SYNDROMES One-and-a-half syndromeThis syndrome consists of a gaze palsy in one direc-tion with an INO when executing a saccade to theopposite side It is produced by damage to the PPRFor abducens nucleus and the MLF on the same sidewithin the pontine tegmentum27 Convergence isgenerally spared as cranial nerve III is spared bilater-ally Given the preserved abduction of the eye con-tralateral to the lesion one commonly observes aprimary position exotropia also known as paralyticpontine exotropia (figure 11)28
Wall-eyed bilateral INO syndrome If the lesion af-fects the MLF within the pons or midbrain ver-gence pathways and the oculomotor apparatuscan be coincidentally disrupted resulting in a va-riety of eye movement abnormalities that includeimpaired convergence29 These lesions are typi-cally bilateral and produce divergence of the eyes(wall-eyed) (figure 12)
INO and trochlear syndrome A highly unusualsyndrome involves a unilateral lesion of the MLFat the level of the caudal midbrain with extensioninto the trochlear nucleus on the same side30
This lesion produces an INO and contralateralhyperdeviation secondary to a IV nerve palsy (re-member the trochlear nerve exits and decussatesto innervate the opposite side superior obliquemuscle) This syndrome can be confused with a
Figure 9 Volitional saccadic pathway with alesion in the right medial longitudinalfasciculus (MLF) that results in aninternuclear ophthalmoparesis (INO)
Volitional saccadic pathway with a lesion in the right MLFthat results in an INO during an attempted saccade to thepatientrsquos left
Figure 10 Infrared oculogram derived from a patient with multiple sclerosiswith bilateral internuclear ophthalmoparesis
In this case a rightward (upward tracing) 20 deg saccade results in interocular disconjugacy(note separation of the two tracings) Observe that the right eye (OD in blue) achieves the 20deg target rapidly whereas the left eye (OS in red) lags behind The ratio of the eyes when theabducting right eye achieves the target to the position of the adducting eye at that time isreferred to as the first pass amplitude (FPA) Ultimately both eyes achieve the fixation targetthe final amplitude (FA) During the trajectory of the saccade the divergence of the two eyescan result in loss of stereoscopy diplopia (transiently) difficulty reading visual blur and riskof fall while turning or motor vehicle accident with head turning while driving
Neurology 70 April 22 2008 e63
skew deviation however in the case of INO andskew deviation the hyperdeviation is generally onthe side of the INO
ABNORMAL VERTICAL EYE MOVEMENTSWITH MLF LESIONS The MLF contains path-ways involved in the regulation of vertical pur-suit vertical vestibular signals and vertical
alignment2931-33 Patients with INO will thereforeoften exhibit abnormalities with vertical eyemovements including the following diminishedvertical gaze holding abnormal optokinetic andpursuit responses decreased vertical VOR gainvertical gaze-evoked nystagmus convergent-retraction nystagmus decreased vertical smoothpursuit and skew deviation
CLINICAL MANIFESTATIONS OF INO The clin-ical manifestations associated with INO includediplopia (typically horizontal binocular) visualconfusion the illusion of environmental move-ment during horizontal saccades (oscillopsia)vertigo and blurring of visual image acuity par-ticularly with reading2 A less conspicuous butpotentially dangerous feature includes worseningdisconjugacy and a resultant break in binocularfusion during head active turning (which pro-duces a contraversive slow phase punctuated bysaccades in the direction of head movement)while head turning during driving (eg changinglanes) and while ambulating
RADIOGRAPHIC IDENTIFICATION OF MLFLESIONS Several pathologic studies have showna clear anatomic relationship between the pres-ence of lesions along the ipsilateral MLF and thepresence of INO114-17 Due to its high spatial reso-lution MRI has allowed us to depict in vivo theanatomic organization of the human oculomotornerve complex theMLF and related structures inthe brainstem (typically white matter tracts havelow signal intensity and nuclei have higher signalintensity)34 Moreover MRI has also contributedto a better understanding of the different stages ofmyelination of these structures in the pretermbrain35
In patients with INO MRI has shown hyper-intense lesions in the region of the MLF on T2-weighted images that were not detected usingCT36 T2-hyperintensities in the pontine and mid-brain tegmentum portion of the MLF have beenshown in a high percentage of patients with INOderived from different neurologic disorders (fig-ure 13) In one study involving 58 patients withMS with INO MRI with proton density imagingdetected a higher percentage of MLF involvement(100) than T2 (88) and fast-FLAIR (48)37
We have recently studied the relationship be-tween the severity of INO and correspondingmeasures of brain tissue injury within the MLFderived from the advanced neuroradiologic tech-niques diffusion tensor imaging and magnetiza-tion transfer imaging38 The application ofneurophysiologic methods in the quantitative
Figure 11 An example of the one-and-a-half syndrome in one of our patientswith multiple sclerosis
The patient was unable to elicit saccades to the right (ie a right gaze palsy) and had evi-dence of a right internuclear ophthalmoparesis (INO) upon attempted gaze to the left In thisphotograph the patient is looking straight ahead We can observe an exotropia the so-calledparalytic pontine exotropia with the left eye in exo (the only remaining movement possible) Inthis circumstance there is an attempted leftward preference However only left eye abduc-tion is possible given the right INO (with slowing and significant ocular limitation) Below is theT2-weighted axial MRI showing the responsible lesion involving the right pontine tegmentum(arrow)
Figure 12 The syndrome of wall-eyed bilateralinternuclear ophthalmoparesis(INO) in an patient with multiplesclerosis with progressive diseaseand a history of a severeinflammatory demyelinatingsyndrome involving thetegmentum of the ponto-mesencephalic junction whichaffected the medial longitudinalfasciculus (MLF) bilaterally
Note the exotropic appearance of both eyes (ie wall-eyed)Attempted gaze to the right or left revealed adduction slow-ing and limitation consistent with bilateral INO There wasalso reduced vertical smooth pursuit and vertical vestibulo-ocular reflexes (both pathways course through the MLF)
e64 Neurology 70 April 22 2008
analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

physician groups when the degree of adductionslowing was severe Alternately milder cases ofINO were frequently not identified by the major-ity of evaluators
Most demyelinating lesions of the MLF are lo-cated in the pons or midbrain often sparing thevergence pathways including the fibers project-ing from the medial rectus subnucleus of cranialnerve III2 As a result convergence is intact in themajority of patients despite adduction weaknesson lateral gaze This finding can help distinguishan INO from partial third nerve palsy Furtherthe two eyes are typically well aligned in the pri-mary position (nearly orthophoric or slightly exo-phoric on cross cover testing with one eyeviewing) compared to third nerve palsies whichcommonly produce a conspicuous exotropia (amisalignment with both eyes viewing) along withabnormalities of the eyelid and pupil and otherextraocular muscles
INO can produce a modest slowing of abduc-tion as well as adduction in the same affectedeye2 In an extreme example it has been reportedthat a complete horizontal monocular failure ofeye movement can occur (affecting the ipsilateralmedial longitudinal fasciculus and possibly theabducens nerve fascicle as well) in associationwith a dorsolateral pontine tegmentum lesion asthe first event of MS26
INO SYNDROMES One-and-a-half syndromeThis syndrome consists of a gaze palsy in one direc-tion with an INO when executing a saccade to theopposite side It is produced by damage to the PPRFor abducens nucleus and the MLF on the same sidewithin the pontine tegmentum27 Convergence isgenerally spared as cranial nerve III is spared bilater-ally Given the preserved abduction of the eye con-tralateral to the lesion one commonly observes aprimary position exotropia also known as paralyticpontine exotropia (figure 11)28
Wall-eyed bilateral INO syndrome If the lesion af-fects the MLF within the pons or midbrain ver-gence pathways and the oculomotor apparatuscan be coincidentally disrupted resulting in a va-riety of eye movement abnormalities that includeimpaired convergence29 These lesions are typi-cally bilateral and produce divergence of the eyes(wall-eyed) (figure 12)
INO and trochlear syndrome A highly unusualsyndrome involves a unilateral lesion of the MLFat the level of the caudal midbrain with extensioninto the trochlear nucleus on the same side30
This lesion produces an INO and contralateralhyperdeviation secondary to a IV nerve palsy (re-member the trochlear nerve exits and decussatesto innervate the opposite side superior obliquemuscle) This syndrome can be confused with a
Figure 9 Volitional saccadic pathway with alesion in the right medial longitudinalfasciculus (MLF) that results in aninternuclear ophthalmoparesis (INO)
Volitional saccadic pathway with a lesion in the right MLFthat results in an INO during an attempted saccade to thepatientrsquos left
Figure 10 Infrared oculogram derived from a patient with multiple sclerosiswith bilateral internuclear ophthalmoparesis
In this case a rightward (upward tracing) 20 deg saccade results in interocular disconjugacy(note separation of the two tracings) Observe that the right eye (OD in blue) achieves the 20deg target rapidly whereas the left eye (OS in red) lags behind The ratio of the eyes when theabducting right eye achieves the target to the position of the adducting eye at that time isreferred to as the first pass amplitude (FPA) Ultimately both eyes achieve the fixation targetthe final amplitude (FA) During the trajectory of the saccade the divergence of the two eyescan result in loss of stereoscopy diplopia (transiently) difficulty reading visual blur and riskof fall while turning or motor vehicle accident with head turning while driving
Neurology 70 April 22 2008 e63
skew deviation however in the case of INO andskew deviation the hyperdeviation is generally onthe side of the INO
ABNORMAL VERTICAL EYE MOVEMENTSWITH MLF LESIONS The MLF contains path-ways involved in the regulation of vertical pur-suit vertical vestibular signals and vertical
alignment2931-33 Patients with INO will thereforeoften exhibit abnormalities with vertical eyemovements including the following diminishedvertical gaze holding abnormal optokinetic andpursuit responses decreased vertical VOR gainvertical gaze-evoked nystagmus convergent-retraction nystagmus decreased vertical smoothpursuit and skew deviation
CLINICAL MANIFESTATIONS OF INO The clin-ical manifestations associated with INO includediplopia (typically horizontal binocular) visualconfusion the illusion of environmental move-ment during horizontal saccades (oscillopsia)vertigo and blurring of visual image acuity par-ticularly with reading2 A less conspicuous butpotentially dangerous feature includes worseningdisconjugacy and a resultant break in binocularfusion during head active turning (which pro-duces a contraversive slow phase punctuated bysaccades in the direction of head movement)while head turning during driving (eg changinglanes) and while ambulating
RADIOGRAPHIC IDENTIFICATION OF MLFLESIONS Several pathologic studies have showna clear anatomic relationship between the pres-ence of lesions along the ipsilateral MLF and thepresence of INO114-17 Due to its high spatial reso-lution MRI has allowed us to depict in vivo theanatomic organization of the human oculomotornerve complex theMLF and related structures inthe brainstem (typically white matter tracts havelow signal intensity and nuclei have higher signalintensity)34 Moreover MRI has also contributedto a better understanding of the different stages ofmyelination of these structures in the pretermbrain35
In patients with INO MRI has shown hyper-intense lesions in the region of the MLF on T2-weighted images that were not detected usingCT36 T2-hyperintensities in the pontine and mid-brain tegmentum portion of the MLF have beenshown in a high percentage of patients with INOderived from different neurologic disorders (fig-ure 13) In one study involving 58 patients withMS with INO MRI with proton density imagingdetected a higher percentage of MLF involvement(100) than T2 (88) and fast-FLAIR (48)37
We have recently studied the relationship be-tween the severity of INO and correspondingmeasures of brain tissue injury within the MLFderived from the advanced neuroradiologic tech-niques diffusion tensor imaging and magnetiza-tion transfer imaging38 The application ofneurophysiologic methods in the quantitative
Figure 11 An example of the one-and-a-half syndrome in one of our patientswith multiple sclerosis
The patient was unable to elicit saccades to the right (ie a right gaze palsy) and had evi-dence of a right internuclear ophthalmoparesis (INO) upon attempted gaze to the left In thisphotograph the patient is looking straight ahead We can observe an exotropia the so-calledparalytic pontine exotropia with the left eye in exo (the only remaining movement possible) Inthis circumstance there is an attempted leftward preference However only left eye abduc-tion is possible given the right INO (with slowing and significant ocular limitation) Below is theT2-weighted axial MRI showing the responsible lesion involving the right pontine tegmentum(arrow)
Figure 12 The syndrome of wall-eyed bilateralinternuclear ophthalmoparesis(INO) in an patient with multiplesclerosis with progressive diseaseand a history of a severeinflammatory demyelinatingsyndrome involving thetegmentum of the ponto-mesencephalic junction whichaffected the medial longitudinalfasciculus (MLF) bilaterally
Note the exotropic appearance of both eyes (ie wall-eyed)Attempted gaze to the right or left revealed adduction slow-ing and limitation consistent with bilateral INO There wasalso reduced vertical smooth pursuit and vertical vestibulo-ocular reflexes (both pathways course through the MLF)
e64 Neurology 70 April 22 2008
analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

skew deviation however in the case of INO andskew deviation the hyperdeviation is generally onthe side of the INO
ABNORMAL VERTICAL EYE MOVEMENTSWITH MLF LESIONS The MLF contains path-ways involved in the regulation of vertical pur-suit vertical vestibular signals and vertical
alignment2931-33 Patients with INO will thereforeoften exhibit abnormalities with vertical eyemovements including the following diminishedvertical gaze holding abnormal optokinetic andpursuit responses decreased vertical VOR gainvertical gaze-evoked nystagmus convergent-retraction nystagmus decreased vertical smoothpursuit and skew deviation
CLINICAL MANIFESTATIONS OF INO The clin-ical manifestations associated with INO includediplopia (typically horizontal binocular) visualconfusion the illusion of environmental move-ment during horizontal saccades (oscillopsia)vertigo and blurring of visual image acuity par-ticularly with reading2 A less conspicuous butpotentially dangerous feature includes worseningdisconjugacy and a resultant break in binocularfusion during head active turning (which pro-duces a contraversive slow phase punctuated bysaccades in the direction of head movement)while head turning during driving (eg changinglanes) and while ambulating
RADIOGRAPHIC IDENTIFICATION OF MLFLESIONS Several pathologic studies have showna clear anatomic relationship between the pres-ence of lesions along the ipsilateral MLF and thepresence of INO114-17 Due to its high spatial reso-lution MRI has allowed us to depict in vivo theanatomic organization of the human oculomotornerve complex theMLF and related structures inthe brainstem (typically white matter tracts havelow signal intensity and nuclei have higher signalintensity)34 Moreover MRI has also contributedto a better understanding of the different stages ofmyelination of these structures in the pretermbrain35
In patients with INO MRI has shown hyper-intense lesions in the region of the MLF on T2-weighted images that were not detected usingCT36 T2-hyperintensities in the pontine and mid-brain tegmentum portion of the MLF have beenshown in a high percentage of patients with INOderived from different neurologic disorders (fig-ure 13) In one study involving 58 patients withMS with INO MRI with proton density imagingdetected a higher percentage of MLF involvement(100) than T2 (88) and fast-FLAIR (48)37
We have recently studied the relationship be-tween the severity of INO and correspondingmeasures of brain tissue injury within the MLFderived from the advanced neuroradiologic tech-niques diffusion tensor imaging and magnetiza-tion transfer imaging38 The application ofneurophysiologic methods in the quantitative
Figure 11 An example of the one-and-a-half syndrome in one of our patientswith multiple sclerosis
The patient was unable to elicit saccades to the right (ie a right gaze palsy) and had evi-dence of a right internuclear ophthalmoparesis (INO) upon attempted gaze to the left In thisphotograph the patient is looking straight ahead We can observe an exotropia the so-calledparalytic pontine exotropia with the left eye in exo (the only remaining movement possible) Inthis circumstance there is an attempted leftward preference However only left eye abduc-tion is possible given the right INO (with slowing and significant ocular limitation) Below is theT2-weighted axial MRI showing the responsible lesion involving the right pontine tegmentum(arrow)
Figure 12 The syndrome of wall-eyed bilateralinternuclear ophthalmoparesis(INO) in an patient with multiplesclerosis with progressive diseaseand a history of a severeinflammatory demyelinatingsyndrome involving thetegmentum of the ponto-mesencephalic junction whichaffected the medial longitudinalfasciculus (MLF) bilaterally
Note the exotropic appearance of both eyes (ie wall-eyed)Attempted gaze to the right or left revealed adduction slow-ing and limitation consistent with bilateral INO There wasalso reduced vertical smooth pursuit and vertical vestibulo-ocular reflexes (both pathways course through the MLF)
e64 Neurology 70 April 22 2008
analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

analysis of a clinically discrete syndrome and thecharacterization of its corresponding neuroradio-logic measures of tissue injury provide a strategyfor studying the relationship between clinical dis-ability and the spectrum of brain tissue histopa-thology in MS
Two structures responsible for the generationand gaze stability of vertical and torsional eyemovements the riMLF and the INC are locatedin the mesencephalon In 11 patients with MRI-identified mesencephalic lesions and clinicalevidence of torsionalvertical spontaneous nys-tagmus Helmchen and colleagues showed thatcombined lesions of riMLF and INC are muchmore frequent than riMLF and INC lesionsalone39
More recently modern MR-based techniqueshave been used to achieve a better in vivo pictureof the underlying pathologic changes of manyneurologic conditions Diffusion tensor MRI canidentify infarctions involving the MLF and alsoreveals detailed information regarding white mat-ter fibers tract anatomy and direction40 Using linescan diffusion MRI Mamata and colleagues visu-alized in six healthy volunteers the principal fi-ber tracts of white matter including the MLF41
DISEASES TARGETING THE MLF Cerebrovascu-lar disease The most common cause of INO in anolder patient is ischemic infarction These pa-tients are typically older than patients with MSwith an average age of 62ndash66 years42 In contrastto MS most (87 to 93) INO syndromes in thissetting are unilateral In a large case series of 410cases of INO evaluated by the same observer
stroke was the most common cause of INO(38)42 In this series individual cases of INO arereported with varied stroke subtypes includinghemorrhage (hypertensive vascular malforma-tion) vertebral artery dissection temporal arteri-tis and other vasculitides
Multiple sclerosis MS constitutes the second mostcommon cause of INO representing approxi-mately one-third of cases (34) and is the mostcommon cause in a young person (45 years)where most are bilateral42
Inflammation in MS is contingent upon traf-ficking of mononuclear cells across the cerebro-vascular endothelium in a process mediated bywell-characterized adhesion molecules Post-capillary venules provide the scaffolding for adhe-sion and trafficking into the CNS and have theirgreatest concentration in areas around theperiventricular zones4344 As such the brainstemtegmentum is an area of high predilection for dis-ease activity in MS
Other etiologies A large number of causes makeup the one-quarter to one-third of INO cases thatare not due to MS or cerebrovascular disease (ta-ble) The most common of these are infectiontrauma and tumor In some remarkable exam-ples mild head injury can produce an isolatedunilateral or bilateral INO4546 A partial thirdnerve palsy with prominent medial rectus weak-ness may be confused with an INO Distinguish-ing features include other third nerve deficits(weakness of elevation ptosis pupil dilation) im-
Figure 13 A highly conspicuous lesion in the midbrain tegmentum just ventral tothe cerebral aqueduct (left image arrow) and a highlycharacteristic lesion in the MLF of the pontomesencephalicjunction (right image arrow) (3 mm thick axial proton densityweighted sequences) was noted
Both images were derived from patients with multiple sclerosis and bilateral internuclearophthalmoparesis Both lesions demonstrate the eloquence principal of periventricular demy-elinating lesions that are localized to the brainstem in contrast to the non-eloquence of manycerebral periventricular lesions (that often do not correspond to any concomitant clinicalmanifestations)
Table Etiology of internuclear ophthalmoparesis
Brainstem infarction (commonly unilateral)
Multiple sclerosis (commonly bilateral)
Brainstem and fourth ventricle tumors
Arnold-Chiari malformation
Infection bacterial viral and other forms ofmeningoencephalitis
Hydrocephalus subdural hematoma supratentorialarteriovenous malformation
Nutritional disorders Wernicke encephalopathy andpernicious anemia
Metabolic disorders hepatic encephalopathy maple syrupurine disease abetalipoproteinemia Fabry disease
Drug intoxications tricyclic antidepressantsphenothiazines narcotics lithium barbiturates propranolol
Cancer
Head trauma
Degenerative conditions progressive supranuclear palsy
Syphilis
Pseudointernuclear ophthalmoplegia of myasthenia gravisand Fisher syndrome
Neurology 70 April 22 2008 e65
paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

paired convergence and absence of the contralat-eral abduction nystagmus all of which point to athird nerve palsy rather than an INO
Eye movement abnormalities including INOhave been reported in progressive supranuclearpalsy (PSP)47 Parkinsonism and other features ofPSP are present in these individuals and most eyemovement abnormality can be overcome withoculocephalic maneuvers (confirming its su-pranuclear character) but not in an INO (con-firming its nuclear character)
A pseudo-INO is a well-described phenome-non in patients with myasthenia gravis andGuillain-Barre syndrome4849 The presence ofptosis and lid fatigue will alert the clinician to my-asthenia while areflexia usually with ataxia orlimb weakness will suggest Guillain-Barre syn-drome The Miller-Fisher syndrome involves ocu-lar motor dysfunction (potentially with INO)ataxia and diminished or absent reflexes49 Find-ings suggestive of bilateral INO have also beenreported in the setting of drug overdose howeverthese individuals would be expected to have se-verely impaired level of consciousness50
PROGNOSIS AND TREATMENT The deficits as-sociated with INO often resolve over a few weeksto months51 In one series patients with a cerebro-vascular etiology were less likely to recover 63had persistent symptoms after 3 years Howeverothers have observed a better prognosis with INOdue to brainstem infarction with 79 to 87 re-covery in 2 to 3 months5253
Patients may be treated with patching of oneeye for symptomatic relief Patching of the af-fected eye may be helpful for those persons whoexperience diplopia as a result of their INOWhen the syndrome is secondary to MS cortico-steroids can serve to accelerate recovery albeitlimited in many Since most patients are wellaligned in primary position of gaze (with goodbinocular fusion) and the double vision is typi-cally provoked in eccentric gaze the use of prismsis usually not helpful However a concomitantand stable skew deviation may be amenable toprismatic correction to abolish the vertical mis-alignment (and consequent diplopia) of the eyes
RECENT ADVANCES AND FUTURE DIREC-TIONS INO is one MLF-related syndrome thatrepresents a useful model by which to objectivelycharacterize a distinctive neurologic syndromeand its corresponding disability with associatedimaging measures of brain tissue injury Thisstrategy may represent a useful proof of principlemodel of pathophysiology upon which to test
neuroprotective and neurorestorative therapiessuch as promoters of axonal sprouting and stemcell remyelination initiatives This is of particularinterest given the periventricular location of theMLF and that stem cells may be effectively deliv-ered into the ventricular system
ACKNOWLEDGMENTThe authors thank Klara Zapotocka from the Graphic De-sign Department at Prague College in the Czech Republic forthe concept design and rendering of the artwork for theillustrated figures in this review
REFERENCES1 Ross AT DeMyer WE Isolated syndrome of the me-
dial longitudinal fasciculus in man anatomical confir-mation Arch Neurol 196615203ndash205
2 Zee DS Internuclear ophthalmoplegia pathophysiol-ogy and diagnosis Baillieres Clin Neurol 19921455ndash470
3 Leigh RJ Zee DS The Neurology of Eye Movementsfourth edition New York Oxford University Press2006
4 Cohen B Komatsuzaki A Eye movements induced bystimulation of the pontine reticular formation evi-dence for integration in oculomotor pathways ExpNeurol 197236101ndash117
5 Carpenter MB Vestibular nuclei afferent and efferentprojections Prog Brain Res 1988765ndash15
6 Zee DS Hain TC Carl JR Abduction nystagmus ininternuclear ophthalmoplegia Ann Neurol 198721383
7 Baloh RW Yee RD Honrubia V Internuclear oph-thalmoplegia I saccades and dissociated nystagmusArch Neurol 197835484
8 Collewijn H Van der Steen J Ferman L Jansen TCHuman ocular counterroll assessment of static and dy-namic properties from electromagnetic scleral coil re-cordings Exp Brain Res 198559185ndash196
9 Bhidayasiri R Plant GT Leigh RJ A hypotheticalscheme for the brainstem control of vertical gaze Neu-rology 200054185ndash193
10 Crawford JD Cadera W Vilis T Generation of tor-sional and vertical eye position signals by the intersti-tial nucleus of Cajal Science 19912521551ndash1553
11 Brodsky MC Donahue SP Vaphiades M Brandt TSkew deviation revisited Surv Ophthalmol 200651105ndash128
12 Galetta SL Liu GT Raps EC Solomon D Volpe NJCyclodeviation in skew deviation Am J Ophthalmol1994118509ndash514
13 Vogel R Thumler R Baumgarten RJ Ocular counter-rolling some practical considerations of a new evalua-tion method for diagnostic purposes Acta Otolaryngol1986102457ndash462
14 Cogan DG Kubic CS Smith WL Unilateral internu-clear ophthalmoplegia report of 8 clinical cases withone postmortem study AMA Arch Ophthalmol 195044783ndash796
15 Smith JL David NJ Internuclear ophthalmoplegiatwo new clinical signs Neurology 196414307
e66 Neurology 70 April 22 2008
16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

16 Harrington RB Hollenhorst RW Sayre GP Unilateralinternuclear ophthalmoplegia report of a case includ-ing pathology Arch Neurol 19661529ndash34
17 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
18 Solingen LD Baloh RW Myers L Ellison G Subclini-cal eye movement disorders in patients with multiplesclerosis Neurology 197727614
19 Frohman TC Frohman EM OrsquoSuilleabhain P et alThe accuracy of clinical detection of INO in MS cor-roboration with quantitative infrared oculographyNeurology 200361848ndash850
20 Meienberg O Muri R Rabineau PA Clinical and ocu-lographic examinations of saccadic eye movements inthe diagnosis of multiple sclerosis Arch Neurol 198643438
21 Ventre J Vighetto A Bailly G et al Saccade metrics inmultiple sclerosis versional velocity dysconjugacy asthe best clue J Neurol Sci 1991102144ndash149
22 Flipse JP Straathof CS Van der Steen J et al Binocu-lar saccadic eye movements in multiple sclerosisJ Neurol Sci 199714853
23 Frohman EM Frohman TC Zhang H et al Quantita-tive oculographic characterization of INO in MSJ Neurol Neurosurg Psychiatry 20027351ndash55
24 Frohman EM Frohman TC OrsquoSuilleabhean P DeweyRB Kramer PD A new measure of dysconjugacy inINO the first-pass amplitude J Neurol Sci 200321065ndash71
25 Muri RM Meienberg O The clinical spectrum of in-ternuclear ophthalmoplegia in multiple sclerosis ArchNeurol 198542851
26 Frohman EM Frohman TC Horizontal monocularfailure a novel clinically isolated syndrome progress-ing to MS Multiple Sclerosis 2003955ndash58
27 Wall M Wray SH The one-and-a-half syndrome aunilateral disorder of the pontine tegmentum a studyof 20 cases and review of the literature Neurology198333971ndash980
28 Sharpe JA Rosenberg MA Hoyt WF Daroff RB Par-alytic pontine exotropia a sign of acute unilateral pon-tine gaze palsy and internuclear ophthalmoplegiaNeurology 1974241076ndash1081
29 Chen CM Lin SH Wall-eye bilateral internuclear oph-thalmoplegia from lesions at different levels of thebrainstem J Neuro-ophthalmol 2007279ndash15
30 Vanooteghem P Dehaene I Van Zandycke M Cassel-man J Combined trochlear nerve palsy and internu-clear ophthalmoplegia Arch Neurol 199249108ndash109
31 Ranalli PJ Sharpe JA Vertical vestibulo-ocular reflexsmooth pursuit and eye-head tracking dysfunction ininternuclear ophthalmoplegia Brain 1988111(Pt 6)1299
32 Cremer PD Migliaccio AA Halmagyi GM CurthoysIS Vestibulo-ocular reflex pathways in internuclearophthalmoplegia Ann Neurol 199945529
33 Frohman EM Dewey RB Frohman TC An unusualvariant of the dorsal midbrain syndrome inMS clinicalcharacteristics and pathophysiologic mechanismsMult Scler 200410322ndash325
34 Miller MJ Mark LP Ho KC Haughton VM Ana-tomic relationship of the oculomotor nuclear complex
and medial longitudinal fasciculus in the midbrainAJNR Am J Neuroradiol 199718111ndash113
35 Counsell SJ Maalouf EF Fletcher AM et al MR im-aging assessment of myelination in the very pretermbrain AJNR Am J Neuroradiol 200223872ndash881
36 Atlas SW Grossman RI Savino PJ et al Internuclearophthalmoplegia MR-anatomic correlation AJNRAm J Neuroradiol 19878243ndash247
37 Frohman EM Zhang H Kramer PD et al MRI char-acteristics of the MLF in MS patients with chronic in-ternuclear ophthalmoparesis Neurology 200157762ndash768
38 Fox RJ McColl R Lee JC Frohman TC FrohmanEM Validating diffusion tensor imaging as a measureof physiologic disruption Neurology 200768A53 Ab-stract
39 Helmchen C Rambold H Kempermann U et al Lo-calizing value of torsional nystagmus in small midbrainlesions Neurology 2002591956ndash1964
40 Marx JJ Thoemke F Fitzek S et al A new method toinvestigate brain stem structural-functional correla-tions using digital post-processing MRI-reliability inischemic internuclear ophthalmoplegia Eur J Neurol20018489ndash493
41 Mamata H Mamata Y Westin CF et al High-resolution line scan diffusion tensor MR imaging ofwhite matter fiber tract anatomy AJNR Am J Neuro-radiol 20022367ndash75
42 Keane JR Internuclear ophthalmoplegia unusualcauses in 114 of 410 patients Arch Neurol 200562714
43 Noseworthy JH Lucchinetti C Rodriguez M Weinsh-enker BG Multiple sclerosis N Engl J Med 2000343938ndash952
44 Frohman EM Raine C Racke MK Multiple sclerosisthe plaque and its pathogenesis N Engl J Med 2006354942ndash955
45 Gray M Forbes RB Morrow JI Primary isolatedbrainstem injury producing internuclear ophthalmo-plegia Br J Neurosurg 200115432ndash434
46 Constantoyannis C Tzortzidis F Papadakis N Inter-nuclear ophthalmoplegia following minor head injurya case report Br J Neurosurg 199812377ndash379
47 Flint AC Williams O Bilateral internuclear ophthal-moplegia in progressive supranuclear palsy with anoverriding oculocephalic maneuver Mov Disord 2005201069ndash1071
48 Barton JJ Fouladvand M Ocular aspects of myasthe-nia gravis Semin Neurol 2000207ndash20
49 al-Din SN Anderson M Eeg-Olofsson O Trontelj JVNeuro-ophthalmic manifestations of the syndrome ofophthalmoplegia ataxia and areflexia a review ActaNeurol Scand 199489157ndash163
50 Lifshitz M Gavrilov V Sofer S Signs and symptoms ofcarbamazepine overdose in young children PediatrEmerg Care 20001626ndash27
51 Bolanos I Lozano D Cantu C Internuclear ophthal-moplegia causes and long-term follow-up in 65 pa-tients Acta Neurol Scand 2004110161
52 Kim JS Internuclear ophthalmoplegia as an isolated orpredominant symptom of brainstem infarction Neu-rology 2004621491
53 Eggenberger E Golnik K Lee A et al Prognosis ofischemic internuclear ophthalmoplegia Ophthalmol-ogy 20021091676
Neurology 70 April 22 2008 e67
DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

DOI 10121201wnl000031064037810b3200870e57-e67 Neurology
T C Frohman S Galetta R Fox et al Pearls amp Oy-sters The medial longitudinal fasciculus in ocular motor physiology
This information is current as of May 20 2008
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

ServicesUpdated Information amp
httpnneurologyorgcontent7017e57fullincluding high resolution figures can be found at
References httpnneurologyorgcontent7017e57fullref-list-1
This article cites 52 articles 15 of which you can access for free at
Citations httpnneurologyorgcontent7017e57fullotherarticles
This article has been cited by 6 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionocular_motilityOcular motility
httpnneurologyorgcgicollectionnystagmusNystagmus
httpnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnneurologyorgcgicollectiondiplopia_double_visionDiplopia (double vision)
httpnneurologyorgcgicollectionclinical_neurology_historyClinical neurology history
httpnneurologyorgcgicollectionclinical_neurology_examinationClinical neurology examination
httpnneurologyorgcgicollectionall_neuroophthalmologyAll Neuro-ophthalmology
httpnneurologyorgcgicollectionall_educationAll Education
httpnneurologyorgcgicollectionall_clinical_neurologyAll Clinical Neurology e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology