Embed Size (px)
Citation preview
Prosthodontics
 combined impression technique for a partial Implant-supportedfixed-detachable restoration
Davitd Koliavi*
Abstract Á passiveßl between o.'iseointegrated implatits and the prosthesis .-iupported by themis crticial to the correct distribution ofthe stress exerted on the implants. Theaccuracy ofthe Impression procedure in duplicating the exact position oftiieimpiant abutment is one ofthe main contributors to passive fit. An impressiontechnique is presented whereby the deniate and edentulous parts are duplicated inelastomeric material, providing boih theflexlbihty needed to remove the impressionand the ivquired accuracy Subsequent duplication ofthe implant zone with plaster,without removal ofthe tray, affords a high degree of accuracy. (Quintessence Int!9V7:2S:I77-ISL)
Clinical relevance
This article offers a reliable technique for achievingpassive fit of serew-retained. implant-sup portedrestorations.
lntrodnction
The primary objective in constructing the metalstructure supported by osseointegrated implant fix-tures is to achieve a passively fitting prosthesis. Thismeans thai when the restoration is screwed to theabutment in the unloaded state, no stress is transmittedto fixtures and no excessive stress is built up in thescrews connecting the restoration to the abutments. Toachieve the passive fit, it is necessary to eliminate asmueh distortion as possible in the transfer andimpression procedures.
A technique to reduce the cumulative distortion inthe transfer stage was suggested by Henry' andRasmussen,- They connected the gold copings directlyto the abutments and picked them up in an impression.
' Senior Lecturer, Coordinator, Oral Impiatit Center, Department ofProsthodonlics, Hebrew University, Hadassah School nf DentalMedicine, Jerusalem, Israel.
Reprint requests: Dr David Kohavi, Oral Implanls Center, Hebrewtiniversity, Hadassah School of Dental Medicine, PO Bos 1172, IL91010 Jerusalem. Israel.
thus using parts ofthe final restoration as a means oftransfer, Zarb and Jansson' described a method inwhich the guide pin-retained transfer coping wasunited with autopolymerizing acrylic resin and dentalfioss. An impression was then made with a polyethermaterial in an acrylic resin open-top custom tray.Comparing this method with those utilizing impres-sion materials alone. Spector et al'' suggested that thistechnique may cause distortion as a result ofthe releaseof residual stress, even after removal of the transfercopings from the integrated implants, when the resin isalready solid,
Phillips et al," in a recent three-dimensional anal-ysis, found that the connection to resin does notsignificantly change the accuracy ofthe impression. Heconeluded that the extra time and difficulties involvedin fahricating the resin splint are probably unnecessary.
In completely edentulous arches restored by implant-supported prostheses, severe undercuts in the anteriorregion are rare. In such cases, some elinicians prefer touse impression plaster. However, in partially edent-ulous arches, where there is a need to duplicate the finedetails of occlusion and contours and to overcometissue undercuts, plaster is not suitable. If a combina-tion of teeth and implants has to be registered, there isa need for a technique similar tn the one used forpartial dentures, where there is a combination of teethand edentulous ridges,*" ' This article presents animpression technique whereby the implant zone isduplicated in plaster, thereby providing a high degree
Qjintessenee internationai Volume 28, Number 3/1997 177
Kohavi
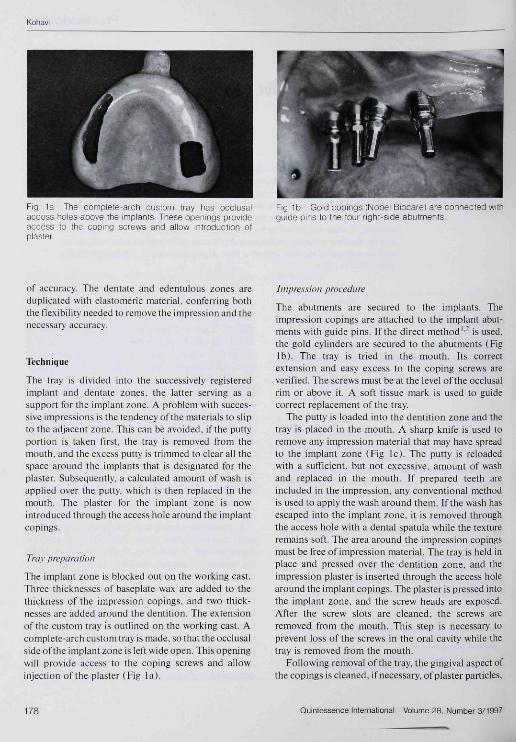
Fig 1a The complete-arch custom Iray has ocolusalaccess holes above the implants These openings provideaccess to the ooping screws and allow iniroduction ofplaster.
Fig lb Gold copings (Nobel Biocarei are connected wilhgutde pins lo the four right-side abutments
of accuracy. The dentate and edentulous zones areduplicated with elastomeric material, conferring boththe tlexibiiity needed to remove the impression and thenecessary accuracy.
Technique
The tray is divided into the successively registeredimplant and dentate zones, the latter serving as asupport for the implant zone. A prohlem with succes-sive impressions is the tendency ofthe materials to slipto the adjacent zone. This can be avoided, if the puttyportion is taken first, the tray is removed from themouth, and the e\cess putty is trimmed to clear all thespace around the implants that is designated for theplaster. Subsequently, a calculated amount of wash isapplied over the putty, which is then replaced in themouth. The plaster for the implant zone is nowintroduced through the access hole around the implantcopings.
Tray preparation
The implant zone is blocked out on the working cast.Three thicknesses of baseplate wax are added to thethickness ofthe impression copings, and two thick-nesses are added around the dentition. The extensionofthe custom tray is outlined on the working cast, Acomplete-arch custom tray is made, so that the occlusalsideoftheimplant zone is left wide open. This openingwill provide access to the coping screws and allowinjection ofthe plaster (Fig la).
Impression procedure
The abutments are secured to the implants. Theimpression copings are attached to the implant abut-ments with guide pins, if the direct method'- is used,the gold cylinders are secured to the abutments (Figlb). The tray is tried in the mouth. Its correctextension and easy excess to the coping screws areverified. The screws must be at the level ofthe occlusalrim or above it, A soft tissue mark is used to guidecorrect replacement ofthe tray
The putty is loaded into the dentition zone and thetray is placed in the mouth, A sharp knife is used toremove any impression material that may have spreadto the implant zone (Fig Ic). The putty is reloadedwith a sufficient, but not excessive, amount of washand replaced in the mouth. If prepared teeth areincluded in the impression, any conventional methodis used to appiy the wash around them. If the wash hasescaped into the implant zone, it is removed throughthe access hole with a dental spatula while the textureremains soft. The area around the impression copingsmust be free of impression material. The tray is held inplace and pressed over the dentition zone, and theimpression plaster is inserted through the access holearound the implant copings. The plaster is pressed intothe implant zone, and tiie screw heads are exposed.After the screw slots are cleaned, the screws areremoved from the mouth. This step is necessary toprevent loss ofthe screws in the oral cavity while thetray is removed from the mouth.
Following removal ofthe tray, the gingival aspect ofthe copings is cleaned, if necessary, of plaster particles.
178 Quintessence International Volume 2a, Nutnber 3/1997
Kohaui
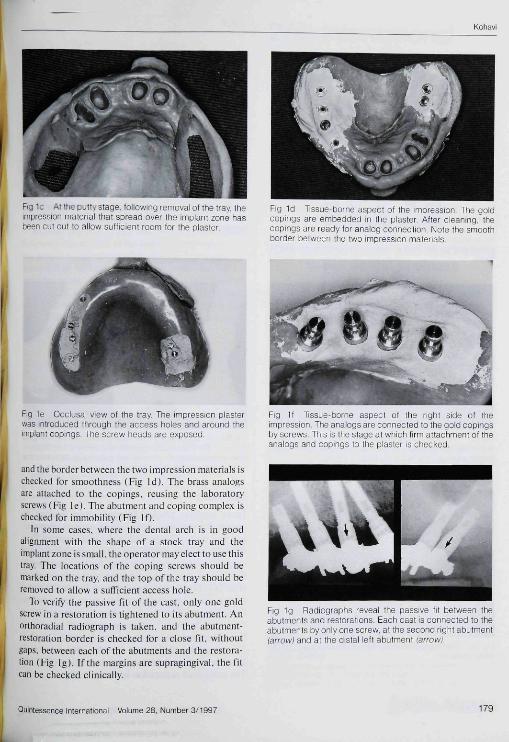
. •• " . ¡-JI!, L-iaçic iollowing removal oí the tray, theimpression material Ihat spread over the impiant zone hasbeen cut out to aiiow sufficieni room for the plaster.
Fig 1d Tissue-borne aspect ot the impression The goldcopings are embedded in the plaster, Atter cieaning, thecopings are ready for analog connection. Note the smoothborder between the two impression materials.
Fig ie Occlusal view o! the tray. The impression plasterwas introduced through the access holes and around theimplant copings. The screw heads are exposed
Fig It Tissue-borne aspect ot the right side ot theimpresston The analogs are connected to the gold copingsby screws This is the stage at which tirm attachment ot theanalogs and copings to the plaster is checked.
and the border between the two impression materials ischecked for smoothness (Fig Id). The brass analogsare attached lo the copings, reusing the laboratoryscrews (Fig Ie). The abutment and coping complex ischecked for immobility (Fig If),
In some cases, where the dental arch is in goodalignment with the shape of a stock tray and theimplant zone is small, the operator may elect to use thistray. The locations of the coping screws should bemarked on the tray, and the top ofthe tray should beremoved to allow a sufficient access hole.
To verify the passive fit ofthe casL only one goldscrew in a restoration is tightened to its abutment. Anorlhoradia! radiograph is taken, and the abuimcnt-restoration border is checked for a close tit, withoutgaps, between each ofthe abutments and the restora-tion (Fig ]g). If the margins are supragingival, the fitcan be checked clinically.
Fig 1g Radiographs reveal the passive tit between theabutments and restorations. Each cast is connected to theabutments by only one screw, at the second right abutment(arrow) and at Ihe distai iett abutment (arrow)
Quintessence International Volume 28, Number 3/1997 179
Kotiavi
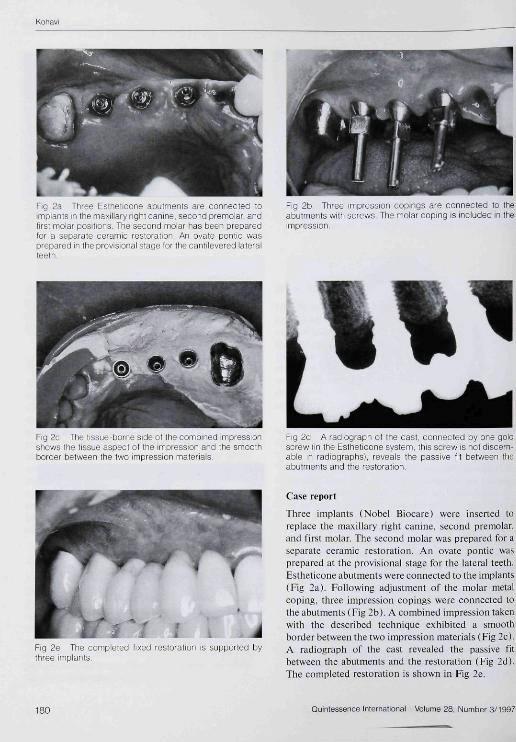
Fig 2_i hree Estheticone abulments are connected toimplants m ihe rria!<illary right canine, second premolar, andtirst molar positions The second molar has been preparedfor a sepárale ceramic restoration. An ovate pontic wasprepared in Ibe provisional stage tor the cantilevered lateralteeth.
Fig 2b Three impression copings are connected to theabutments with screws The molar coping is included in theimpression.
Fig 2c The tissue-borne side of the combined impressionshows the tissue aspect ol the impression and the smoothborder between the two impression materials
Fig 2d A radiograph ot tbe cast, connected by one goldscrew (in the Estheticone system, this screw is not discern-able in radiographs), reveals the passive fit between theabutments and the restoration.
Fig 2e The completed tixed restoration is supported bythree implants.
Case report
Three implants (Nobel Biocare) were inserted toreplace the maxillary right canine, second premolar,and first molar. The second molar was prepared for aseparate ceramic restoration. An ovate pontic wasprepared at the provisional stage for the lateral teeth,Estheticone abutments were connected to the implants(Fig 2a). Following adjustment ofthe molar metalcoping, three impression copings were connected tothe abutments ( Fig 2b). A combined impression takenwith the described technique exhibited a smoothborder between the two impression materials (Fig 2c).A radiograph of the cast revealed the passive fitbetween the abutments and the restoration (Fig 2d).The completed restoration is shown in Fig 2e.
180 Quintessence International Volume 28, Number 3/t997
Kohavi
Discussion
Partially edentulous moutlis restored by fixed-detachable prostlieses present lhe challenge of accur-ately registering two components as dissimilar asosseointegrated impliinl abutments and natural teeih.The first component demands a highly accurate,passively Utted restoration. The second enablesphysiologic movement oí the tooth, because of theperiodontal ligament, and permits minordiserepanciesbetween lhe metal framework and the prepared teeth.The teelinique offered here allows prodtiction of animplant impression with stable and accurate materials.The fine details of the leeth and soft tissue areregistered in elastomeric materials.
Because the tray is not removed from the mouthfollowing registration ofthe teeth and soft tissue, andthe plasler is introduced while the tray is in place, therelationship between the implant zone and the re-mainder ofthe dentition is maintained and faithfullyreproduced. In addilion. the second impression mate-rial does not slip under the impression of the firstzone. This results in even and smooth distribution ofthe impression materials.
References
1. Itenrv PJ. A n allernalive method ror the produetion of accurate castsand occlusal records in osseoin teg rated implant rehabilitation. JProsthet Dem l987:5S;694-697.
2, Rjsmussen EJ, Alternative prosthodontie teehnique for tibsiit-implanted prostheses, J Proslhet Denl 1987:57:198-204.
1. ZarbGA, JanssonTJ, Prosthetic procedure. In: Brjnemark P t. ZarbGA, Albrektsson T (eds). Tissue Integrated Prostheses: Osseointt-gration in Ctinical Dentistry. Chicago; Quintessenee, 19R5 241.
4, Speetor MR, Donovan TE, Niehol lsJl , An evattiatioii of impressionteehniques Ibr osseointeurated implants. J Proslhet Dent 1990:6J:444-447.
5, Phillips K M , Nicol lsJI, Rubcnstein I. The accuracy oflhree implantimpression leehnigues: A threi;-dimension3l análisis. !nt J OralMaxillofae Implanls 1994:^:533-540,
6, Von Krammer R. A two-stage impression technique for distal-esiension removable partiiil dentures, J Prosthel Dent 19SK:6II: 199-201,
7, Miller T f l . LInsicker BL . Improved method to alter casts in partialdemure impression making J Prosthet Dent 1986,55:135-136,
•
27thL internationalDental Show
Cologne 8_12 April 1997' " ' " « ' « • • r , , .
1997IDS for advances and marketing
in the dental business
Dental care for patients has become a marketfor all involved, in which attitude and marketcompetitiveness matter.
For dental medicine and technology,for practice, laboratory and trade.
Every two years advances in dental treatmentare shown at IDS, 1997 vi/ill be no exception.It's where you will find innovation and directionon all that's really important
How to reduce costs!How to enhance petiormance!How to gain competitive edge!
More than 900 exhibiting companies from34 countries are expecting in excess of 55,000professiona! visitors from some 80 countries.That's why IDS is the most importantinternational forum for the dental world.
Face up to the competitionCome to Cologne, ,
/ ^ \ Association[ V ^ ot GermanVal/s] Dental Manufacturers
For further information about IDS '97 please contact:Köln M esseMesse- und Ausstellungs-Ges,m.b,H. Köln
RO. Box 210750, D-50532 CologneFax reply: +49 / 21 61-93 67-5 50Inlernet: http://www,ids-int-dental-show,com
For further information about the12th International Dental Technicians' Congressplease contact:
VDZI ¡Verband deutscner Zahntechniker Innungen)Max-Planck-Str. 25, D-63303 Dreieich,phone' +49/61 03-3 70 70. fax: +49/61 03-37 07 33
Quintessence International Volume 28, Number3/1997