Embed Size (px)
Citation preview
1European Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Prof. Cees H.A. Wittens, MD PhDHead of Venous SurgeryMaastricht University Medical CenterUniklinik AachenUniklinik Aachen
What is new in Deep Venous Disease
VE C
2
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
IntroductionIntroduction New in Deep Venous Thrombosis (DVT)New in Deep Venous Thrombosis (DVT)
Standard care DVTStandard care DVT
Etiology PTSEtiology PTS
Diagnostics DVTDiagnostics DVT
Scoring system DVTScoring system DVT
Treatment OptionsTreatment Options
○ Conservative Conservative
○ InvasiveInvasive
○ New in Deep Venous Obstruction (DVO = > 80% PTS)New in Deep Venous Obstruction (DVO = > 80% PTS)○ DiagnosticsDiagnostics
○ Indications for treatmentIndications for treatment
○ Treatment optionsTreatment options○ StentingStenting
○ EndophlebectomyEndophlebectomy
○ Miscellaneous Miscellaneous
○ ConclusionConclusion
Complications of standard (level1 Complications of standard (level1 evidence) DVT treatment:evidence) DVT treatment:
Pulmonary embolism (5% lethality)Pulmonary embolism (5% lethality)
Recurrent thrombosis (30%)Recurrent thrombosis (30%)
Overall 25% PTS within 1 year.Overall 25% PTS within 1 year.
Iliofemoral thrombosis is associated Iliofemoral thrombosis is associated with a twofold increased risk of with a twofold increased risk of developing PTS >> 50%.developing PTS >> 50%.11
Early thrombolysis may decrease Early thrombolysis may decrease incidence PTS.incidence PTS.
1: Kahn, Ginsberg. Arch Intern Med 2004 3 33European Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
VE C
3
Standard care in DVTStandard care in DVT
4
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Etiology of PTSEtiology of PTS 20-82% of pt’s develop PTS after DVT20-82% of pt’s develop PTS after DVT PTS due to deep venous PTS due to deep venous obstructionobstruction::
Calf: Calf: PTS is rarePTS is rarePopliteal: Popliteal: PTS is rarePTS is rareFemoral: Femoral: commoncommonIliac/caval: Iliac/caval: commoncommon
○ Only 20-30% of thrombosed iliac veins Only 20-30% of thrombosed iliac veins completely recanalize with anticoagulant completely recanalize with anticoagulant therapytherapy
44% claudication 5 years post iliac DVT44% claudication 5 years post iliac DVT15% ulcers 5 years post iliac DVT15% ulcers 5 years post iliac DVT
5
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Diagnostics in DVTDiagnostics in DVT
Due to changed therapeutic Due to changed therapeutic options there is a need to options there is a need to change diagnostics in DVT change diagnostics in DVT 2 point compression ultrasound 2 point compression ultrasound
(not enough!!)(not enough!!)
Complete venous roadmap !!Complete venous roadmap !!Full duplex examinationFull duplex examinationMRVMRVCTVCTV
A Standardized A Standardized classif icationclassif ication
6European Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
VE C
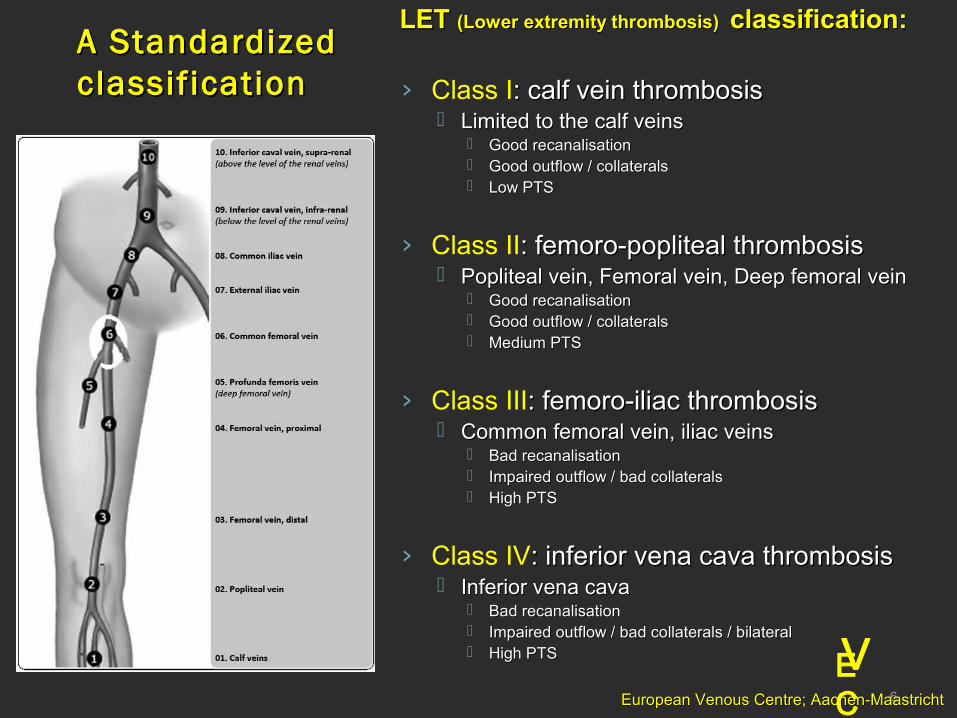
LET LET (Lower extremity thrombosis) (Lower extremity thrombosis) classification:classification:
› Class I: calf vein thrombosis: calf vein thrombosis Limited to the calf veinsLimited to the calf veins
Good recanalisationGood recanalisation Good outflow / collateralsGood outflow / collaterals Low PTSLow PTS
› Class II: femoro-popliteal thrombosis: femoro-popliteal thrombosis Popliteal vein, Femoral vein, Deep femoral veinPopliteal vein, Femoral vein, Deep femoral vein
Good recanalisationGood recanalisation Good outflow / collateralsGood outflow / collaterals Medium PTSMedium PTS
› Class III: femoro-iliac thrombosis: femoro-iliac thrombosis Common femoral vein, iliac veinsCommon femoral vein, iliac veins
Bad recanalisationBad recanalisation Impaired outflow / bad collateralsImpaired outflow / bad collaterals High PTSHigh PTS
› Class IV: inferior vena cava thrombosis: inferior vena cava thrombosis Inferior vena cavaInferior vena cava
Bad recanalisationBad recanalisation Impaired outflow / bad collaterals / bilateralImpaired outflow / bad collaterals / bilateral High PTSHigh PTS
7
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Scoring system in DVTScoring system in DVT
This system will help to document the This system will help to document the pathology in a standardized fashionpathology in a standardized fashion
Make individual clinical decisions Make individual clinical decisions possible depending on the classificationpossible depending on the classification
Makes future research comparable Makes future research comparable (Meta-analyses)(Meta-analyses)
8
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
•Why intervention:Why intervention:•Reduction symptoms (acute stage)Reduction symptoms (acute stage)•Reduction recurrent DVTReduction recurrent DVT•Reduction PTS (by recanalisation and valve Reduction PTS (by recanalisation and valve preservation)preservation)
•In whom:In whom:•Iliofemoral (cava) thrombosisIliofemoral (cava) thrombosis
•Poor recanalisation causing:Poor recanalisation causing: Venous hypertension (95%)Venous hypertension (95%) DVI (90%)DVI (90%) Calve muscle pump dysfunction (50%)Calve muscle pump dysfunction (50%) Venous claudication (15%)Venous claudication (15%) Ulcers (15%)Ulcers (15%) >50 %PTS>50 %PTS
DVT: DVT: interventionintervention
9
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
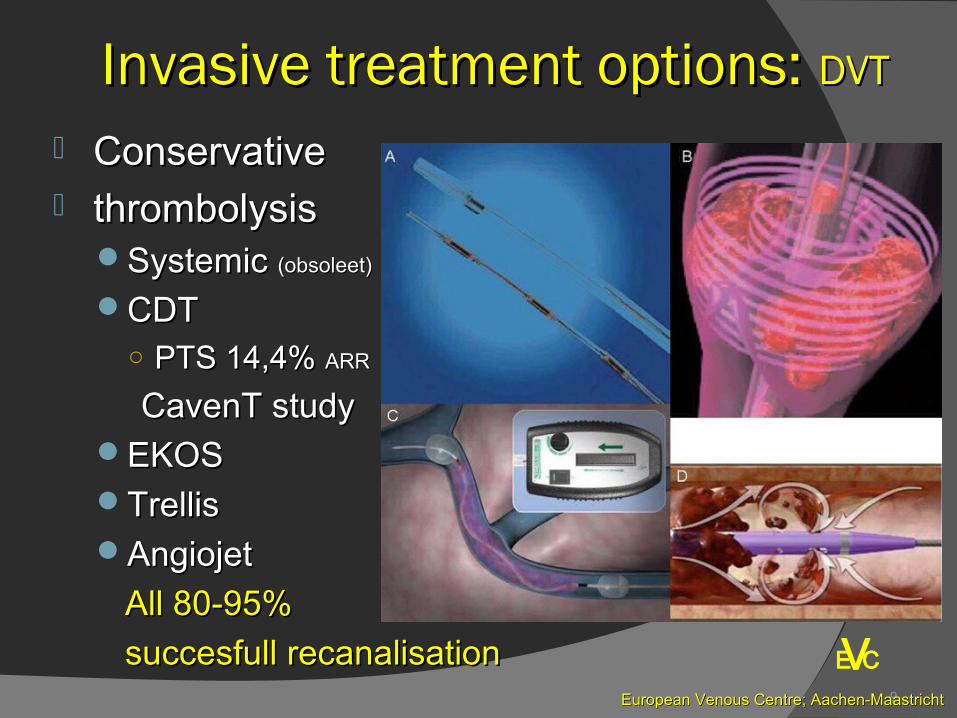
Invasive treatment options: Invasive treatment options: DVTDVT
ConservativeConservative thrombolysisthrombolysis
Systemic Systemic (obsoleet)(obsoleet)
CDTCDT○ PTS 14,4% PTS 14,4% ARRARR
CavenT studyCavenT studyEKOSEKOSTrellisTrellisAngiojetAngiojet
All 80-95% All 80-95%
succesfull recanalisationsuccesfull recanalisation
Vasculaire SpecialisatieE CV
Maastricht-Aken

E CV
ANGIOJET
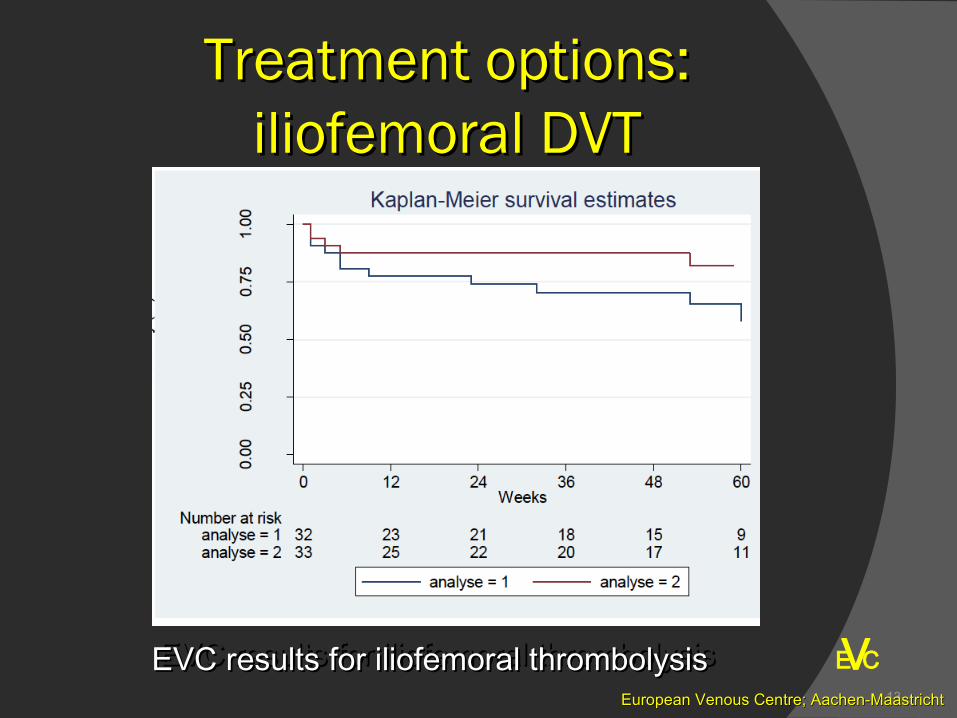
EVC results for iliofemoral thrombolysisEVC results for iliofemoral thrombolysisEVC results for iliofemoral thrombolysisEVC results for iliofemoral thrombolysis13
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Treatment options: Treatment options: iliofemoral DVTiliofemoral DVT
14
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Treatment options: Treatment options: DVTDVT
If it has been shown that a successful thrombus If it has been shown that a successful thrombus removal significantly improves outcome (removal significantly improves outcome (PTS, PTS, recurrent DVT and QoL)recurrent DVT and QoL) CavenTCavenT
AttractAttract
CAVACAVA
We need better dedicated devicesWe need better dedicated devices○ Ideally as a 1 hour out patient procedureIdeally as a 1 hour out patient procedure○ Without thrombolyticsWithout thrombolytics
ComplicationsComplications Medium care admission Medium care admission Costs Costs Malignancies can be treated !Malignancies can be treated ! Postoperative patients can be treated !Postoperative patients can be treated !
15
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
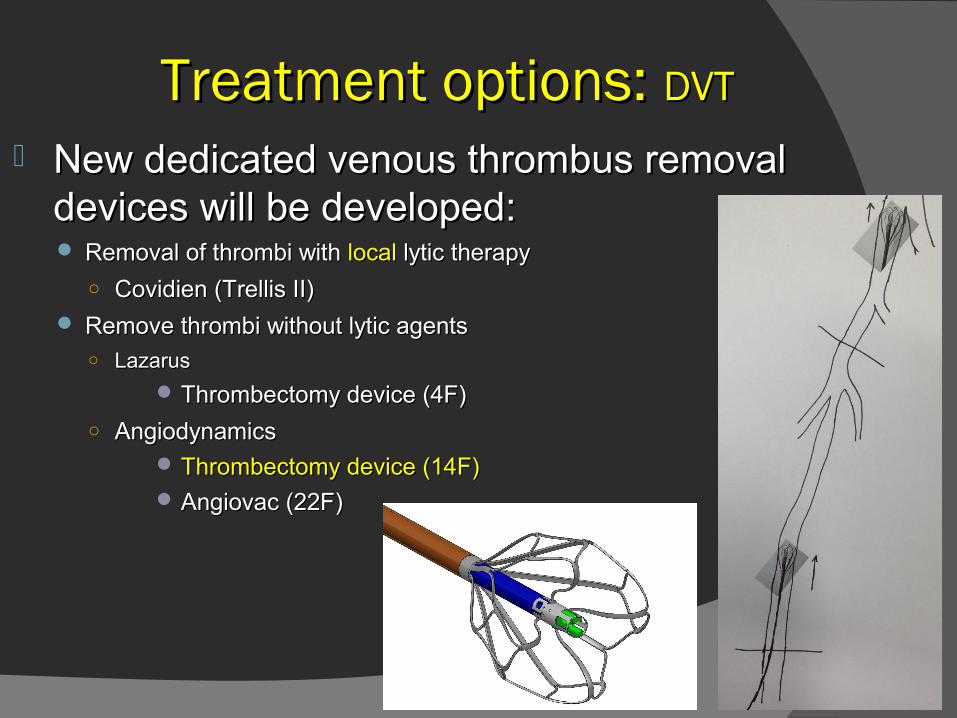
Treatment options: Treatment options: DVTDVT
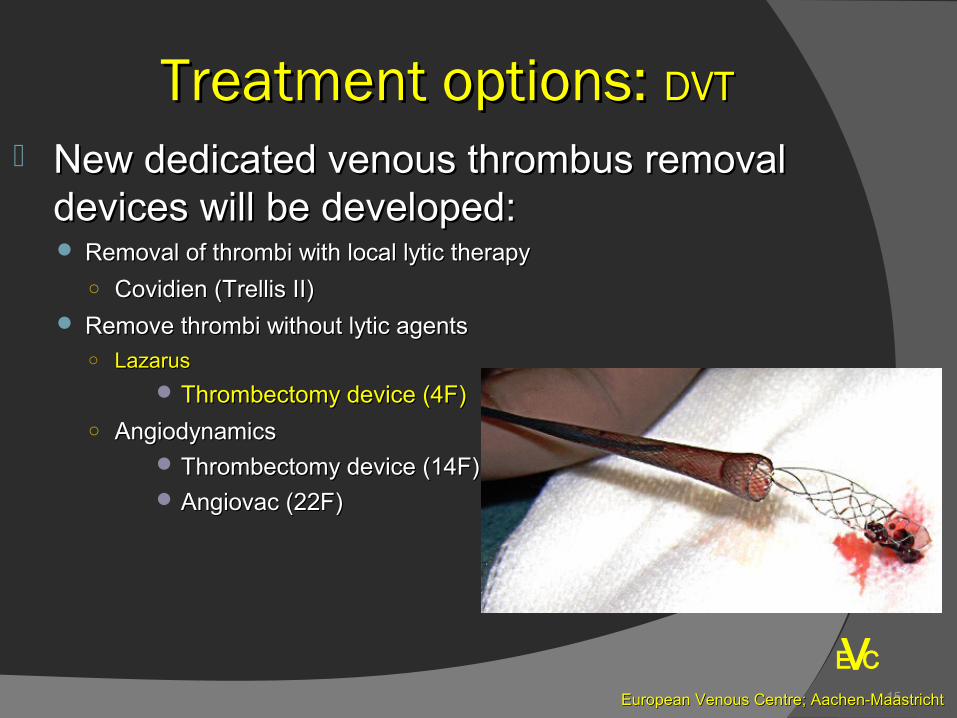
New dedicated venous thrombus removal New dedicated venous thrombus removal devices will be developed:devices will be developed: Removal of thrombi with local lytic therapyRemoval of thrombi with local lytic therapy
○ Covidien (Trellis II)Covidien (Trellis II) Remove thrombi without lytic agentsRemove thrombi without lytic agents
○ Lazarus Lazarus
Thrombectomy device (4F)Thrombectomy device (4F)
○ AngiodynamicsAngiodynamics Thrombectomy device (14F)Thrombectomy device (14F) Angiovac (22F)Angiovac (22F)
16
VE C
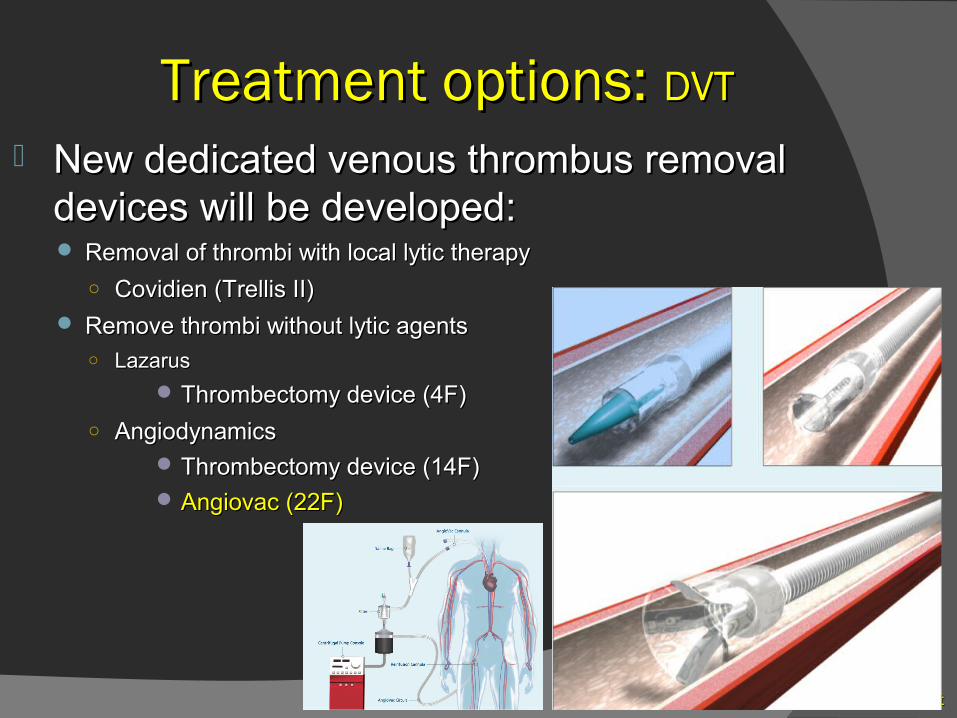
Treatment options: Treatment options: DVTDVT
New dedicated venous thrombus removal New dedicated venous thrombus removal devices will be developed:devices will be developed: Removal of thrombi with Removal of thrombi with locallocal lytic therapy lytic therapy
○ Covidien (Trellis II)Covidien (Trellis II) Remove thrombi without lytic agentsRemove thrombi without lytic agents
○ Lazarus Lazarus
Thrombectomy device (4F)Thrombectomy device (4F)
○ AngiodynamicsAngiodynamics Thrombectomy device (14F)Thrombectomy device (14F) Angiovac (22F)Angiovac (22F)

17
VE C
Treatment options: Treatment options: DVTDVT
18
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Treatment options: Treatment options: DVTDVT
New dedicated venous thrombus removal New dedicated venous thrombus removal devices will be developed:devices will be developed: Removal of thrombi with local lytic therapyRemoval of thrombi with local lytic therapy
○ Covidien (Trellis II)Covidien (Trellis II) Remove thrombi without lytic agentsRemove thrombi without lytic agents
○ LazarusLazarus
Thrombectomy device (4F)Thrombectomy device (4F)
○ AngiodynamicsAngiodynamics Thrombectomy device (14F)Thrombectomy device (14F) Angiovac (22F)Angiovac (22F)
19
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
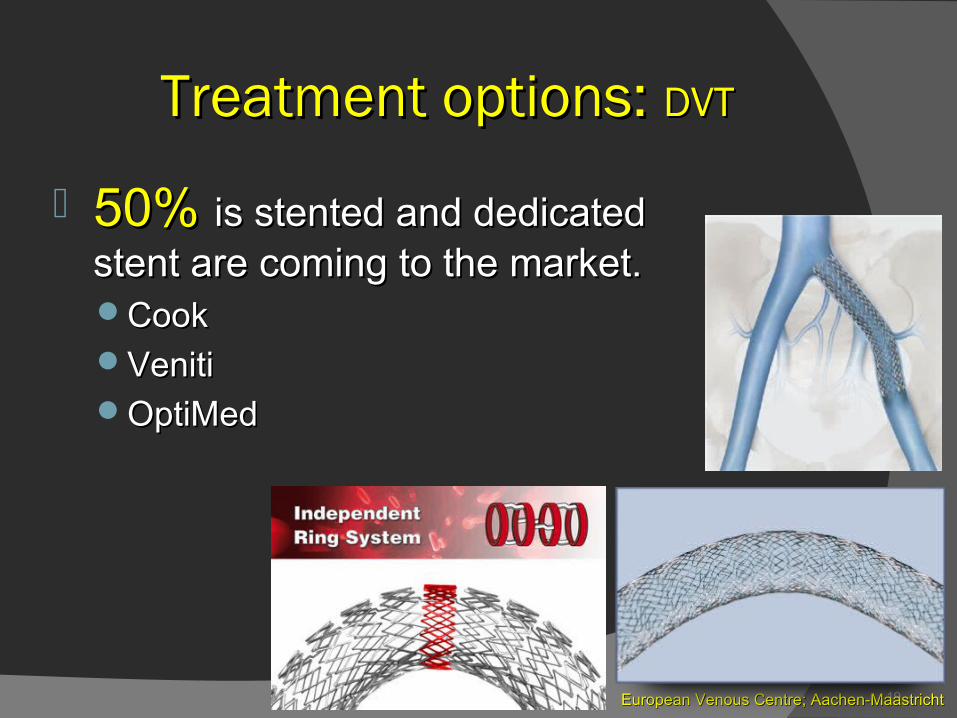
50% 50% is stented and dedicated is stented and dedicated stent are coming to the market.stent are coming to the market.CookCookVenitiVenitiOptiMedOptiMed
Treatment options: Treatment options: DVTDVT
20
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
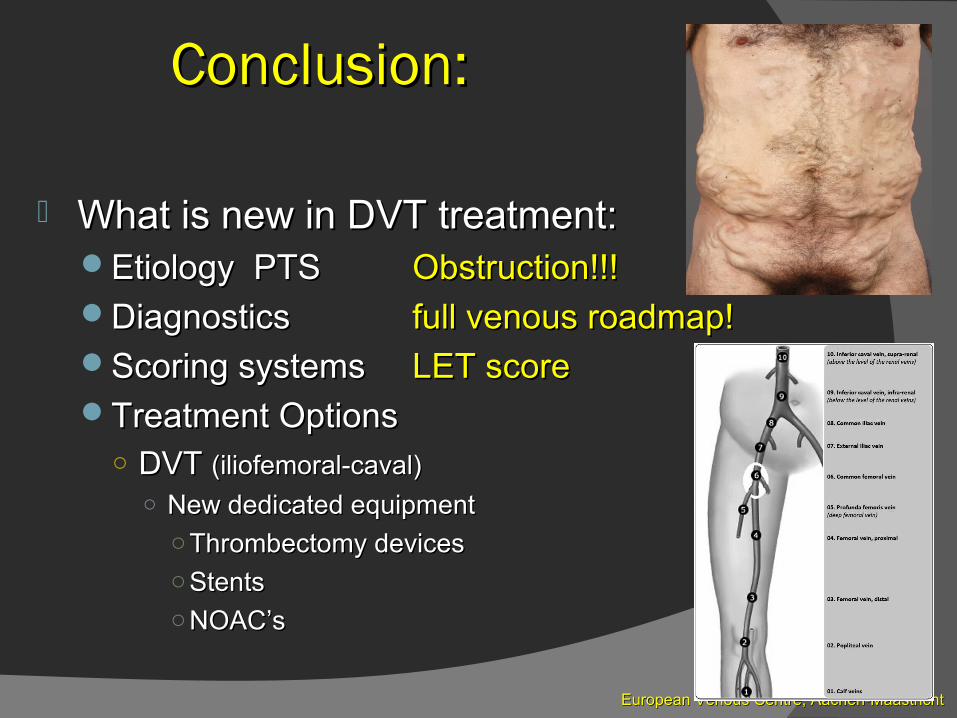
Conclusion:Conclusion:
What is new in DVT treatment:What is new in DVT treatment:Etiology PTSEtiology PTS Obstruction!!!Obstruction!!!DiagnosticsDiagnostics full venous roadmap!full venous roadmap!Scoring systemsScoring systems LET scoreLET scoreTreatment OptionsTreatment Options
○ DVT DVT (iliofemoral-caval)(iliofemoral-caval)○ New dedicated equipmentNew dedicated equipment
○ Thrombectomy devicesThrombectomy devices○ StentsStents○ NOAC’sNOAC’s
21
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Conclusion:Conclusion:
What is new DVT treatment:What is new DVT treatment:
Potential impact on practice to treat Potential impact on practice to treat
DVT and prevent PTS:DVT and prevent PTS:
○ DVT 1/1000/yearDVT 1/1000/year
25 % ilio-femoral25 % ilio-femoral 25/100.000/year 25/100.000/year
Turkey: >>20.000 / yearTurkey: >>20.000 / year
Major impact if this treatment become routineMajor impact if this treatment become routine
22
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
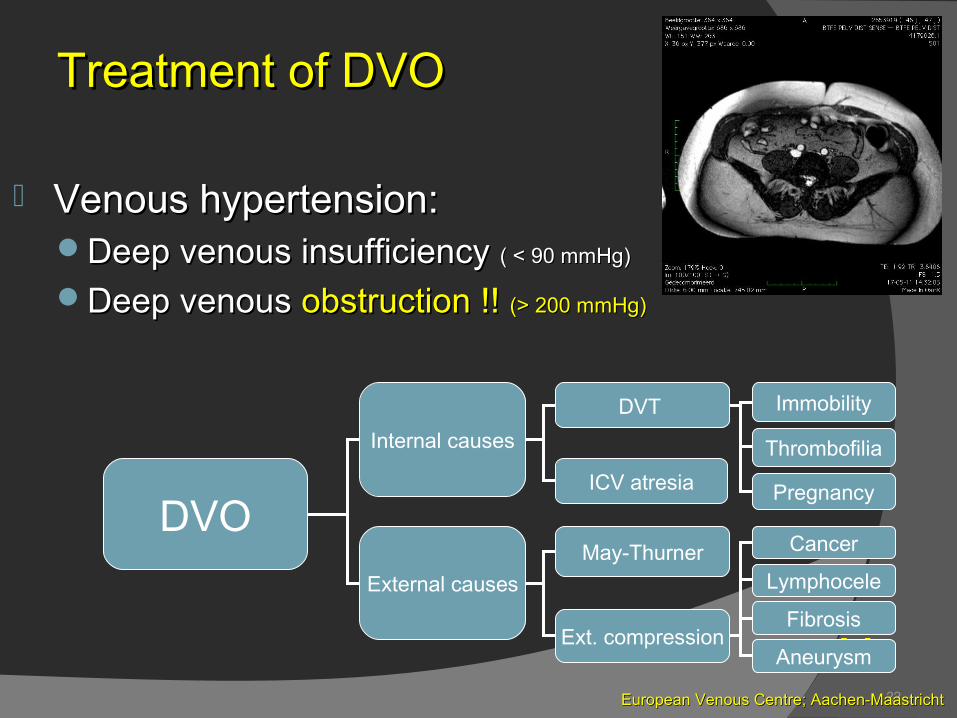
Venous hypertension:Venous hypertension:Deep venous insufficiency Deep venous insufficiency ( < 90 mmHg)( < 90 mmHg)
Deep venous Deep venous obstruction !! obstruction !! (> 200 mmHg)(> 200 mmHg)
DVO
Internal causes
External causes
DVT
May-Thurner
Ext. compression
Cancer
Lymphocele
Fibrosis
Aneurysm
ICV atresia
Immobility
Thrombofilia
Pregnancy
Treatment of DVOTreatment of DVO
23
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
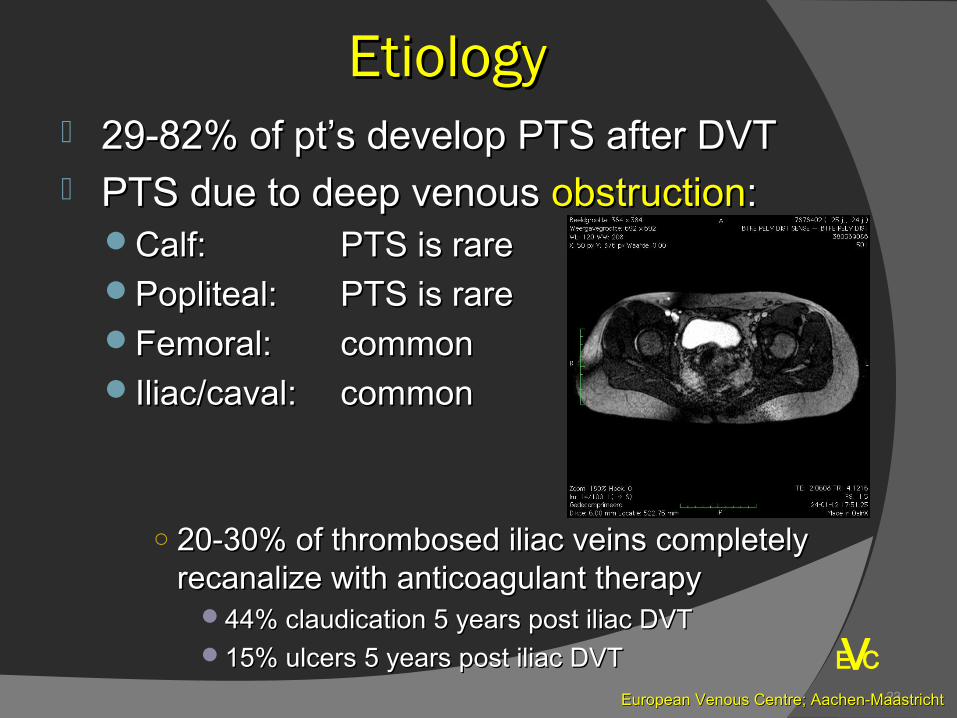
EtiologyEtiology 29-82% of pt’s develop PTS after DVT29-82% of pt’s develop PTS after DVT PTS due to deep venous PTS due to deep venous obstructionobstruction::
Calf: Calf: PTS is rarePTS is rarePopliteal: Popliteal: PTS is rarePTS is rareFemoral: Femoral: commoncommonIliac/caval: Iliac/caval: commoncommon
○ 20-30% of thrombosed iliac veins completely 20-30% of thrombosed iliac veins completely recanalize with anticoagulant therapyrecanalize with anticoagulant therapy
44% claudication 5 years post iliac DVT44% claudication 5 years post iliac DVT15% ulcers 5 years post iliac DVT15% ulcers 5 years post iliac DVT
24
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
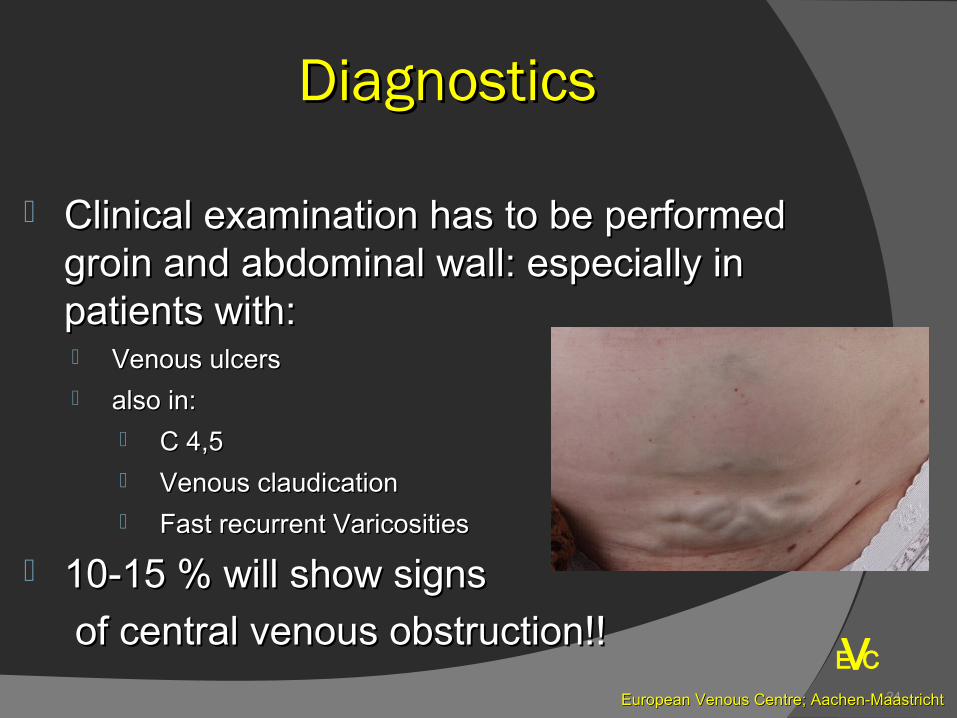
DiagnosticsDiagnostics
Clinical examination has to be performed Clinical examination has to be performed groin and abdominal wall: especially in groin and abdominal wall: especially in patients with:patients with: Venous ulcersVenous ulcers also in:also in:
C 4,5C 4,5 Venous claudicationVenous claudication Fast recurrent VaricositiesFast recurrent Varicosities
10-15 % will show signs10-15 % will show signs
of central venous obstruction!!of central venous obstruction!!

25
VEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
E C
26
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
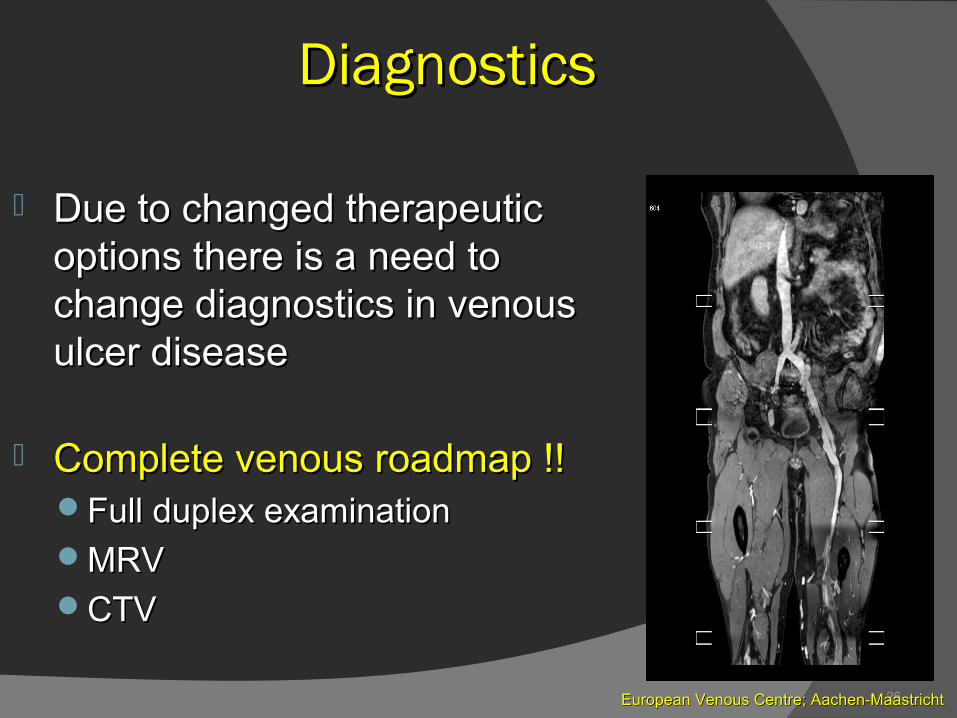
DiagnosticsDiagnostics
Due to changed therapeutic Due to changed therapeutic options there is a need to options there is a need to change diagnostics in venous change diagnostics in venous ulcer diseaseulcer disease
Complete venous roadmap !!Complete venous roadmap !!Full duplex examinationFull duplex examinationMRVMRVCTVCTV
27
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
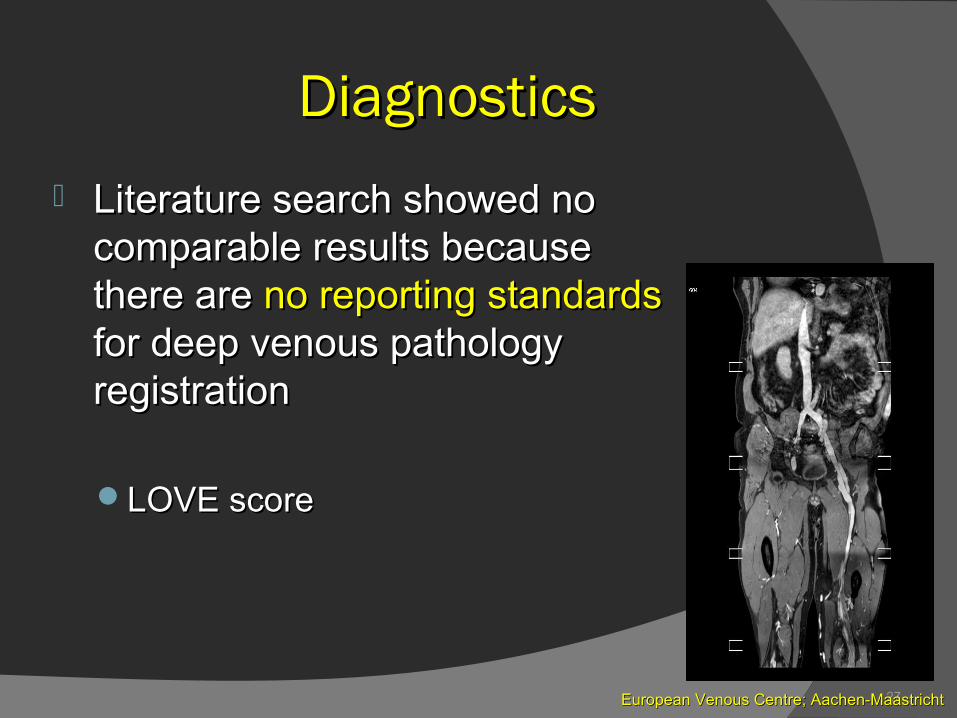
DiagnosticsDiagnostics
Literature search showed no Literature search showed no comparable results because comparable results because there are there are no reporting standards no reporting standards for deep venous pathology for deep venous pathology registrationregistration
LOVE scoreLOVE score
28
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
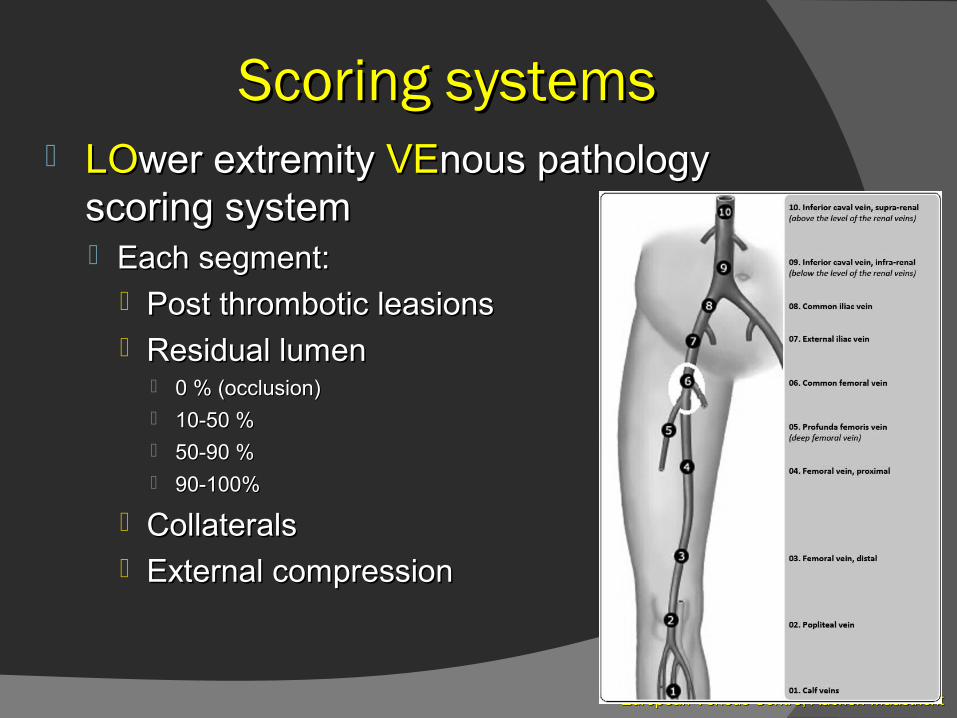
Scoring systemsScoring systems LOLOwer extremity wer extremity VEVEnous pathology nous pathology
scoring systemscoring system Each segment:Each segment:
Post thrombotic leasionsPost thrombotic leasions Residual lumenResidual lumen
0 % (occlusion)0 % (occlusion) 10-50 %10-50 % 50-90 %50-90 % 90-100%90-100%
CollateralsCollaterals External compressionExternal compression
29
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
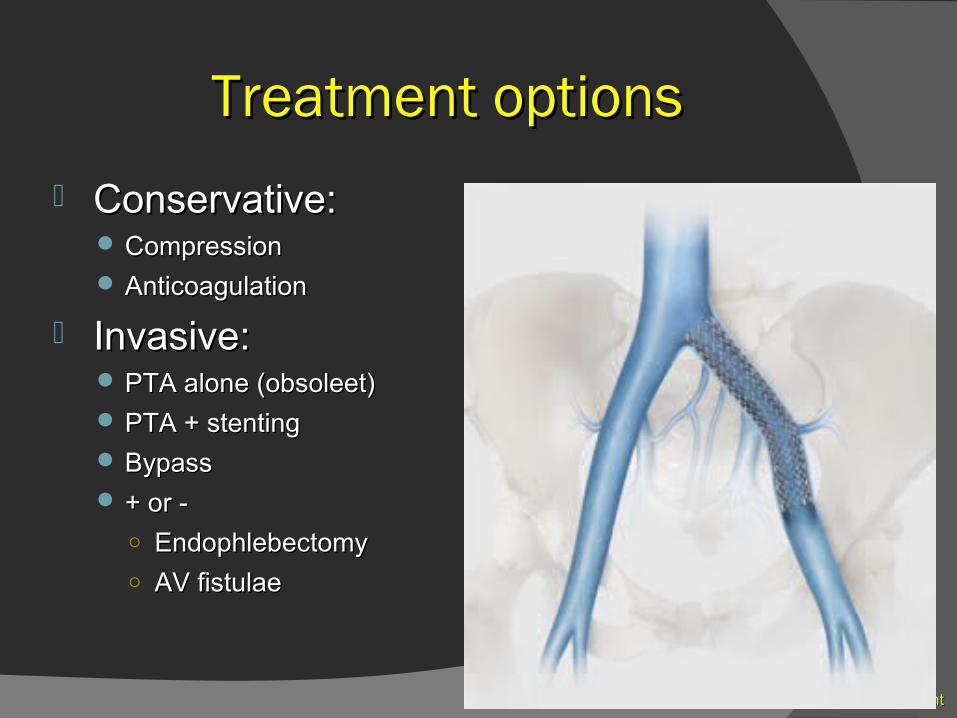
Treatment optionsTreatment options
Conservative:Conservative: CompressionCompression AnticoagulationAnticoagulation
Invasive:Invasive: PTA alone (obsoleet)PTA alone (obsoleet) PTA + stentingPTA + stenting BypassBypass + or -+ or -
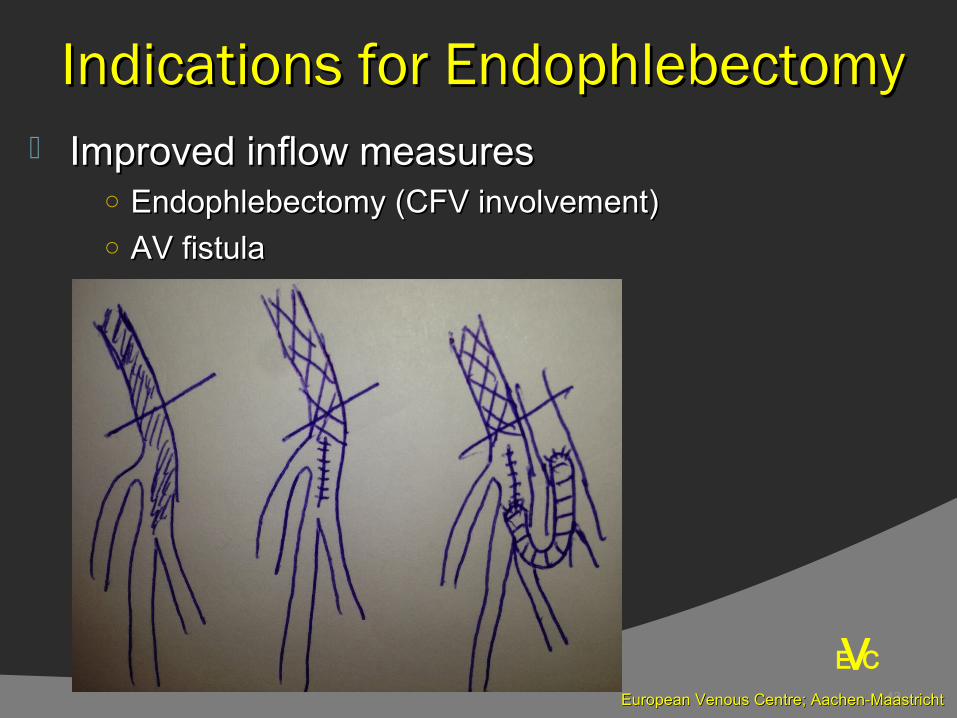
○ EndophlebectomyEndophlebectomy
○ AV fistulaeAV fistulae

30
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Indications for treatment:Indications for treatment:
Improve QoL!!Improve QoL!!Skin problemsSkin problemsVenous claudication !Venous claudication !Swollen legsSwollen legsPainPain
31
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Inferior vena cava: Inferior vena cava: High radial force, minimal flexibility, large diameterHigh radial force, minimal flexibility, large diameter..
Common iliac vein: Common iliac vein: High radial force, high flexibility, large length of stent.High radial force, high flexibility, large length of stent.
External iliac vein: External iliac vein: High radial force, high flexibility, large length of stent.High radial force, high flexibility, large length of stent.
Common femoral vein: Common femoral vein: fracture resistant?!fracture resistant?!
Requirements for stents per segment Requirements for stents per segment
32
E CV
European Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
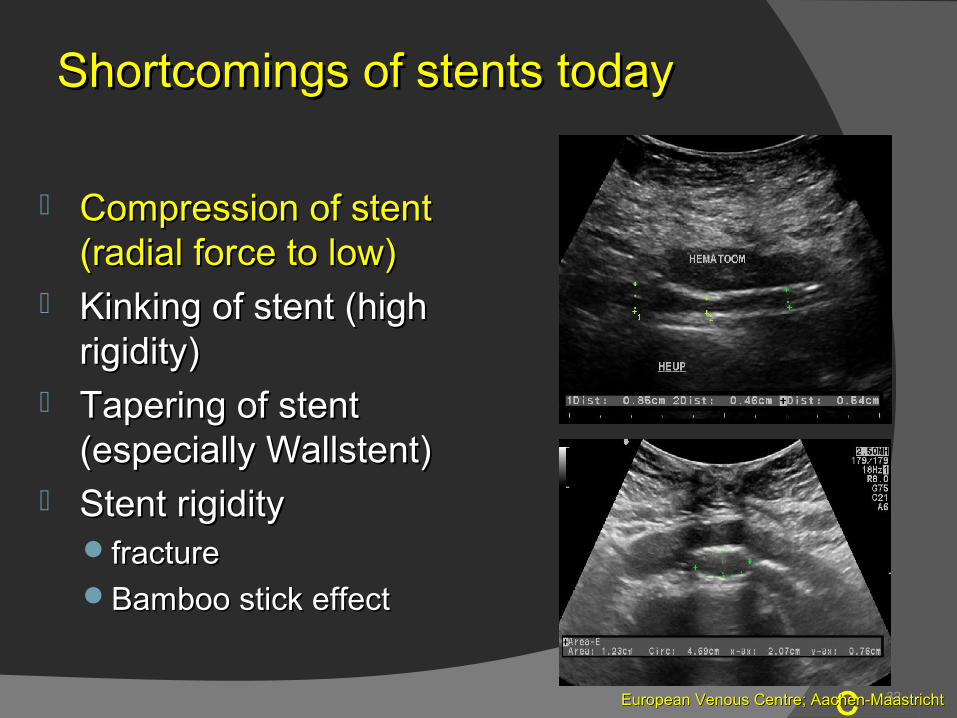
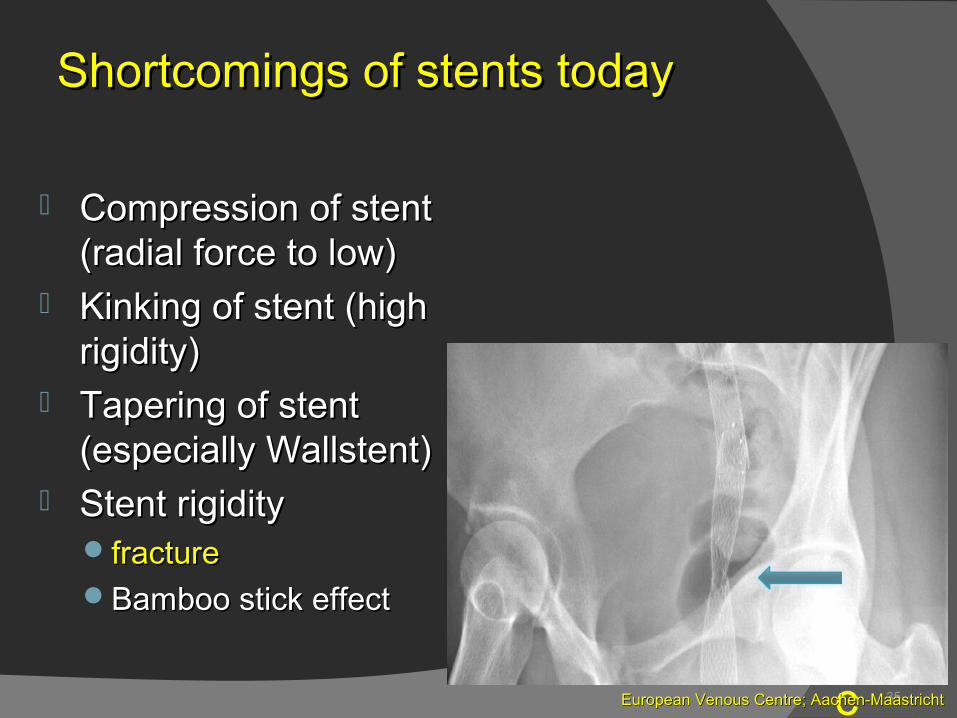
Compression of stent Compression of stent (radial force to low)(radial force to low)
Kinking of stent (high Kinking of stent (high rigidity) rigidity)
Tapering of stent Tapering of stent (especially Wallstent)(especially Wallstent)
Stent rigidityStent rigidityfracturefractureBamboo stick effect Bamboo stick effect
Shortcomings of stents todayShortcomings of stents today
33
E CV
European Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
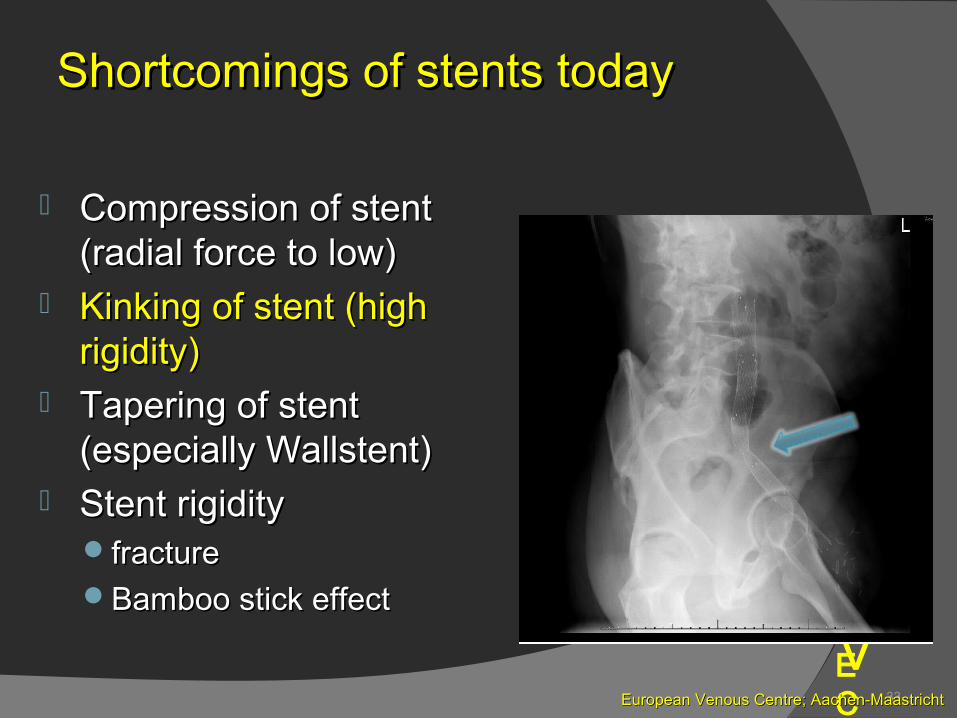
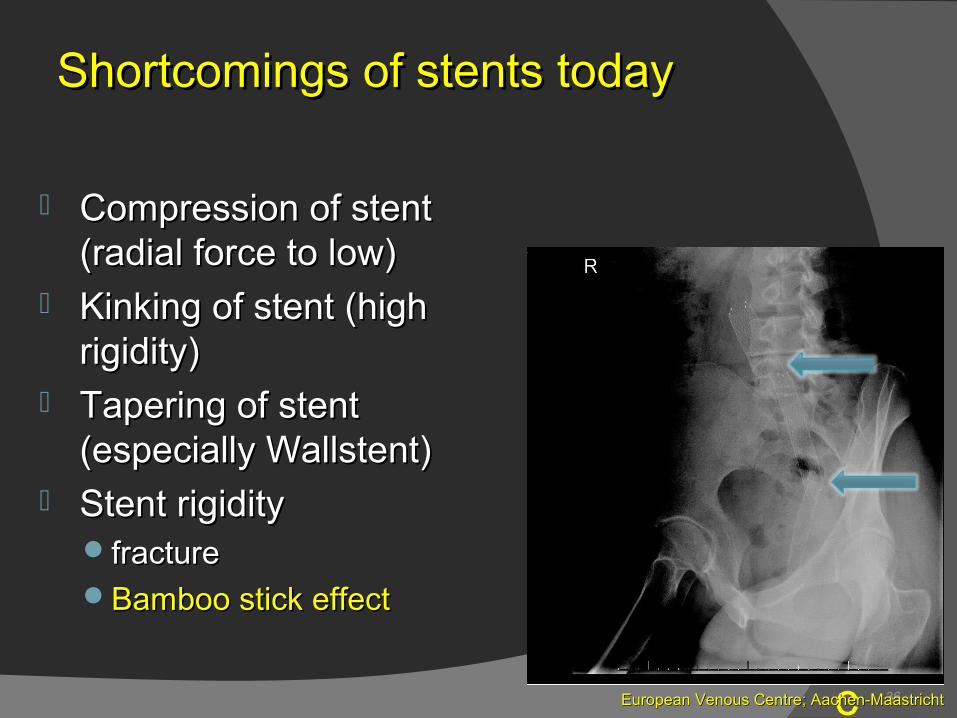
Compression of stent Compression of stent (radial force to low)(radial force to low)
Kinking of stent (high Kinking of stent (high rigidity) rigidity)
Tapering of stent Tapering of stent (especially Wallstent)(especially Wallstent)
Stent rigidityStent rigidityfracturefractureBamboo stick effect Bamboo stick effect
Shortcomings of stents todayShortcomings of stents today
34
E CV
European Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
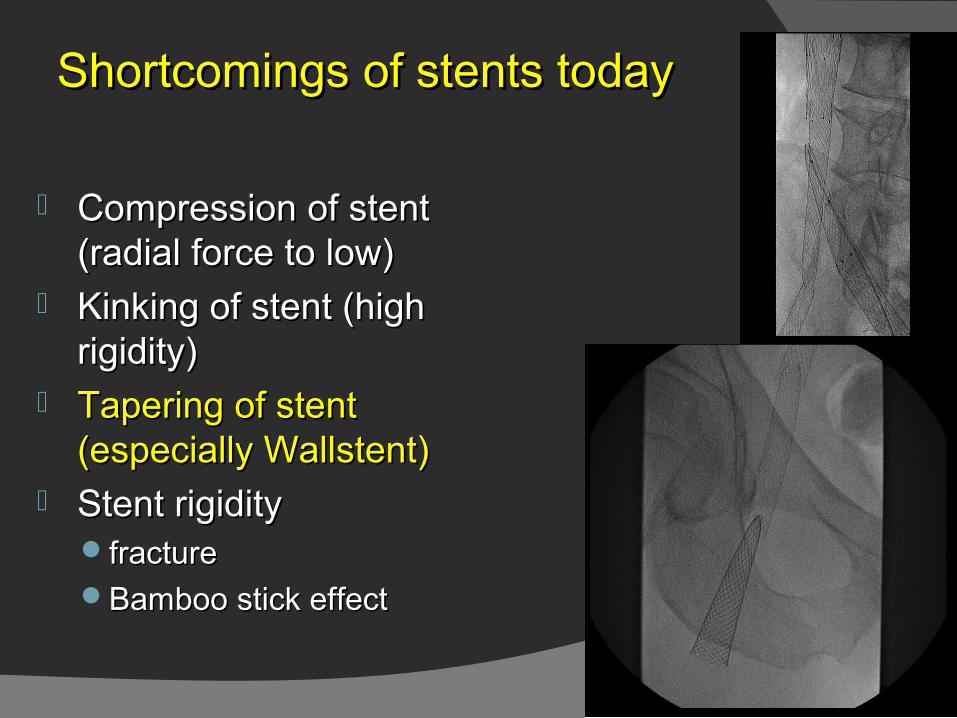
Compression of stent Compression of stent (radial force to low)(radial force to low)
Kinking of stent (high Kinking of stent (high rigidity) rigidity)
Tapering of stent Tapering of stent (especially Wallstent)(especially Wallstent)
Stent rigidityStent rigidityfracturefractureBamboo stick effect Bamboo stick effect
Shortcomings of stents todayShortcomings of stents today
35
E CV
European Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Compression of stent Compression of stent (radial force to low)(radial force to low)
Kinking of stent (high Kinking of stent (high rigidity) rigidity)
Tapering of stent Tapering of stent (especially Wallstent)(especially Wallstent)
Stent rigidityStent rigidityfracturefractureBamboo stick effect Bamboo stick effect
Shortcomings of stents todayShortcomings of stents today
36
E CV
European Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Compression of stent Compression of stent (radial force to low)(radial force to low)
Kinking of stent (high Kinking of stent (high rigidity) rigidity)
Tapering of stent Tapering of stent (especially Wallstent)(especially Wallstent)
Stent rigidityStent rigidityfracturefractureBamboo stick effect Bamboo stick effect
Shortcomings of stents todayShortcomings of stents today
37
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
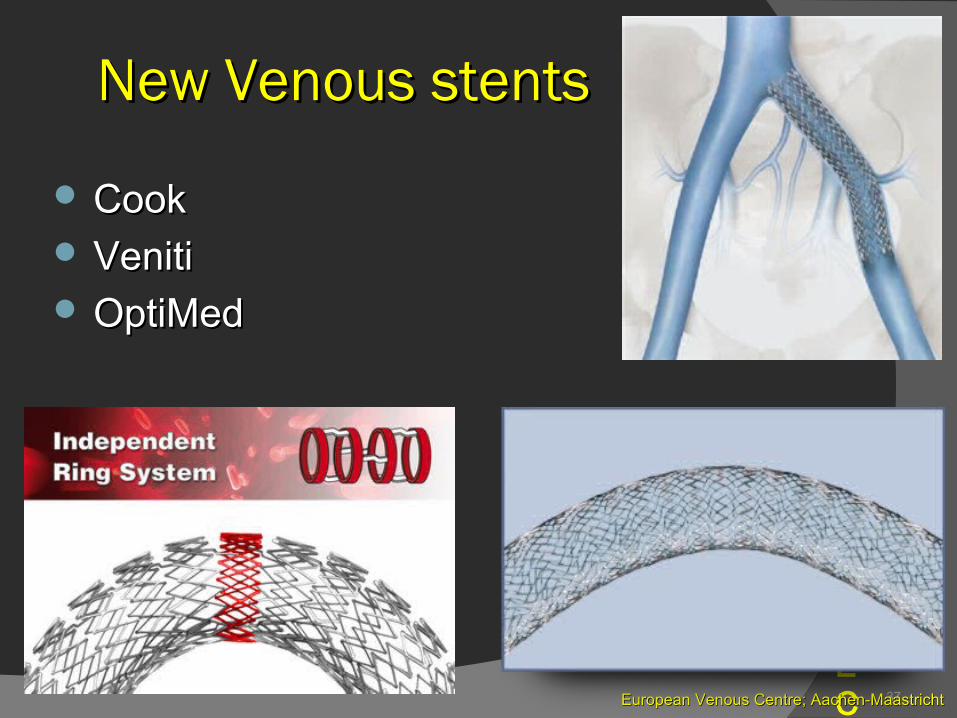
CookCook VenitiVeniti OptiMedOptiMed
New Venous stentsNew Venous stents
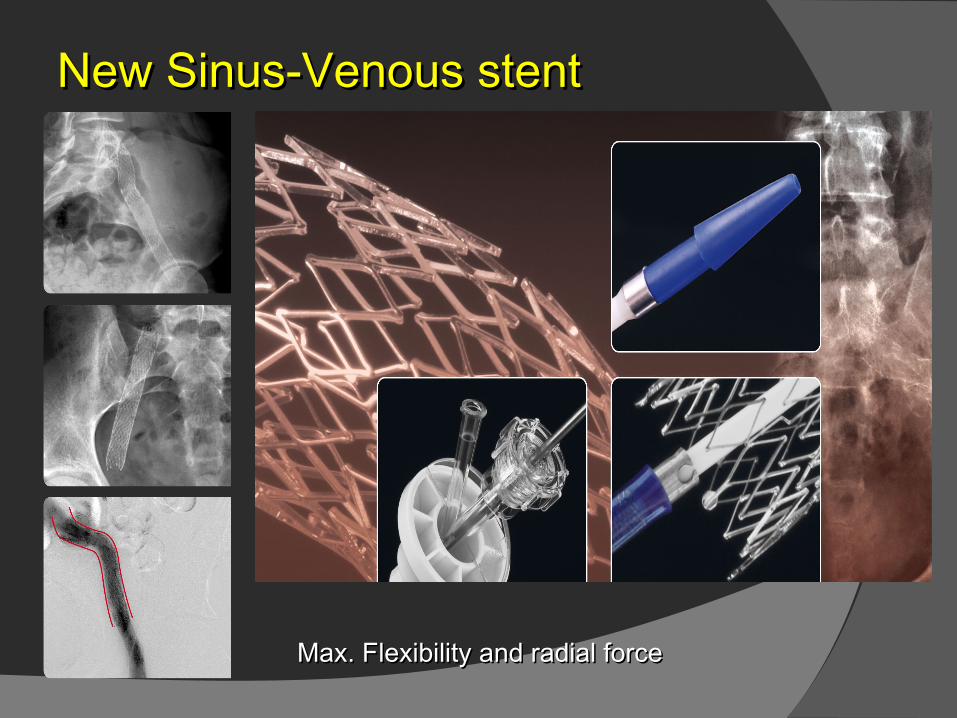
New Sinus-Venous stentNew Sinus-Venous stent
Max. Flexibility and radial forceMax. Flexibility and radial force
39 23
New Sinus-Venous stentNew Sinus-Venous stent
40 23
New Sinus-Venous stentNew Sinus-Venous stent
41
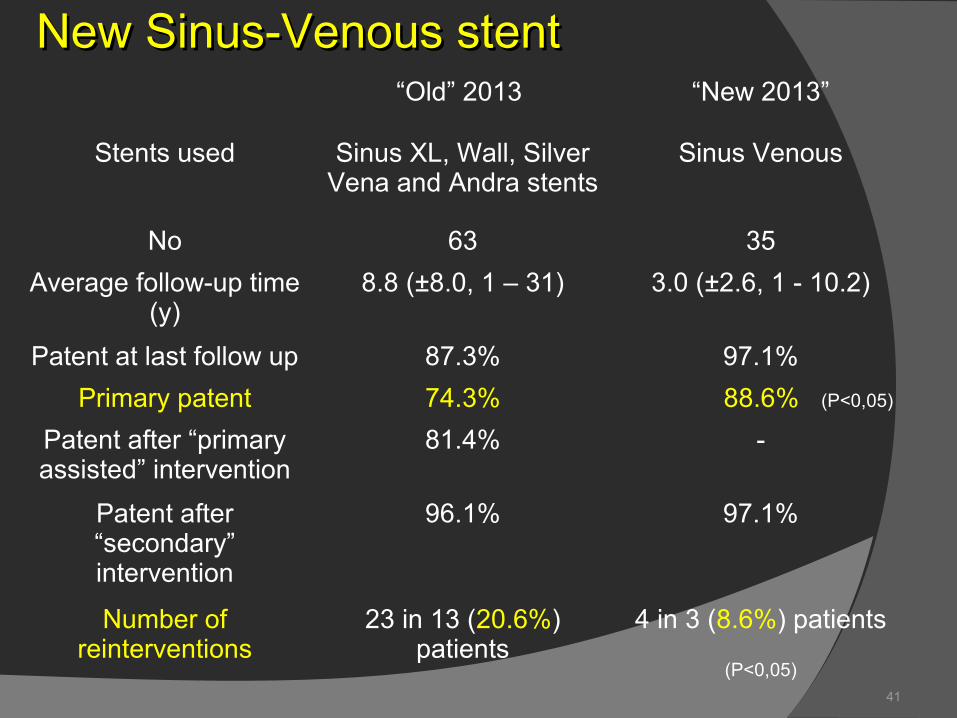
New Sinus-Venous stentNew Sinus-Venous stent“Old” 2013 “New 2013”
Stents used Sinus XL, Wall, Silver Vena and Andra stents
Sinus Venous
No 63 35
Average follow-up time (y)
8.8 (±8.0, 1 – 31) 3.0 (±2.6, 1 - 10.2)
Patent at last follow up 87.3% 97.1%
Primary patent 74.3% 88.6% (P<0,05)
Patent after “primary assisted” intervention
81.4% -
Patent after “secondary” intervention
96.1% 97.1%
Number of reinterventions
23 in 13 (20.6%) patients
4 in 3 (8.6%) patients
(P<0,05)
42
V
New dedicated venous stent available!New dedicated venous stent available!Silver Vena ?Silver Vena ?Veniti ?Veniti ?Sinus-Venous (OptiMed): Sinus-Venous (OptiMed):
better primary and secondary patencybetter primary and secondary patencyEasy deployment and positioningEasy deployment and positioningHigh flexibility with good alignmentHigh flexibility with good alignmentHigh radial forceHigh radial force
E C
ConclusionConclusion
43
VEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Improved inflow measures Improved inflow measures ○ Endophlebectomy (CFV involvement)Endophlebectomy (CFV involvement)○ AV fistulaAV fistula
E C
Indications for EndophlebectomyIndications for Endophlebectomy
44
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
ExperienceExperience
35 Patients35 Patients
Patients withPatients with
○CEAP C4-6CEAP C4-6
○Severe venous claudicationSevere venous claudication
Diagnosis of occlusion/obstructionDiagnosis of occlusion/obstruction
○Duplex ultrasoundDuplex ultrasound
○Magnetic resonance venographyMagnetic resonance venography
○Per-procedural venographyPer-procedural venography
Patency controlPatency control
○Duplex ultrasoundDuplex ultrasound
V
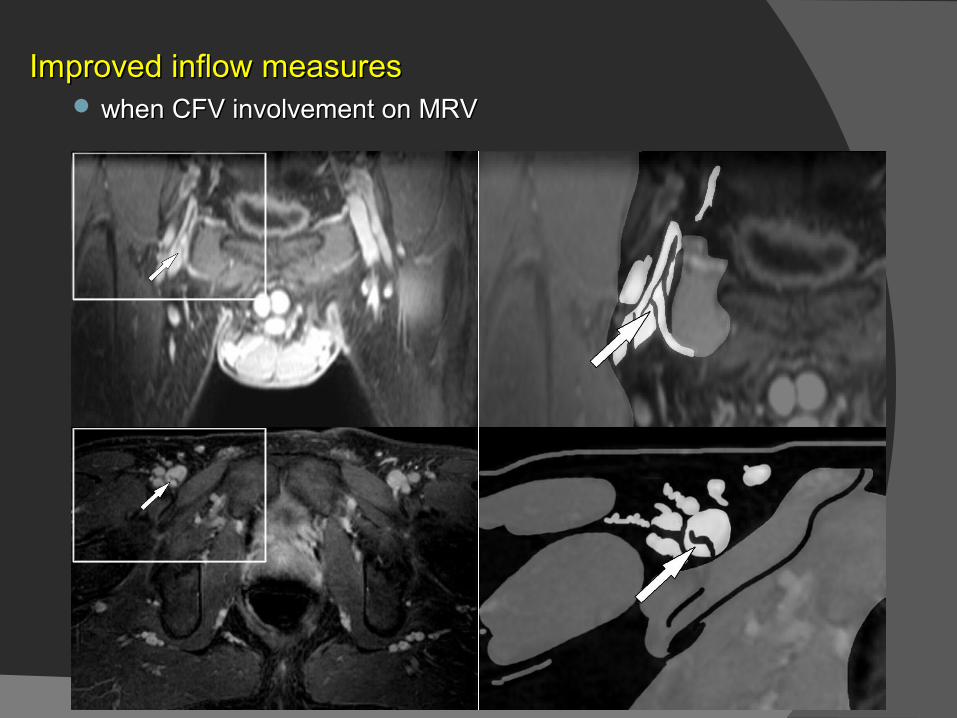
Improved inflow measures Improved inflow measures when CFV involvement on MRV when CFV involvement on MRV
E C
46
Desobstructie VFC with iliac stent
VEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
E C
47
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
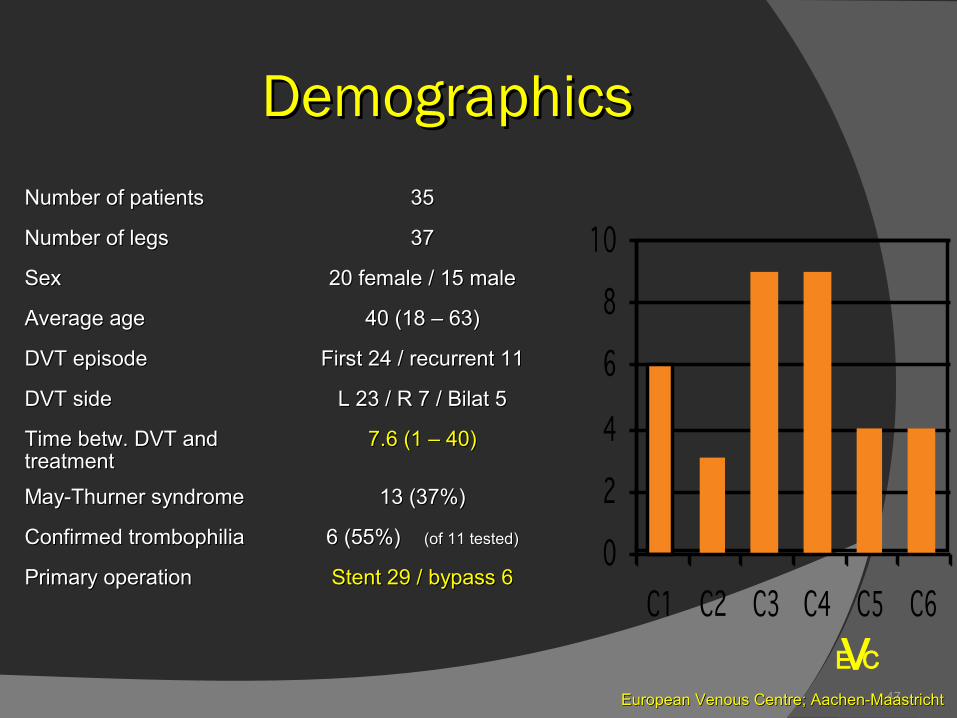
DemographicsDemographics
Number of patientsNumber of patients 3535
Number of legsNumber of legs 3737
SexSex 20 female / 15 male20 female / 15 male
Average ageAverage age 40 (18 – 63)40 (18 – 63)
DVT episodeDVT episode First 24 / recurrent 11First 24 / recurrent 11
DVT sideDVT side L 23 / R 7 / Bilat 5L 23 / R 7 / Bilat 5
Time betw. DVT and Time betw. DVT and treatmenttreatment
7.6 (1 – 40)7.6 (1 – 40)
May-Thurner syndromeMay-Thurner syndrome 13 (37%)13 (37%)
Confirmed trombophiliaConfirmed trombophilia 6 (55%) 6 (55%) (of 11 tested)(of 11 tested)
Primary operationPrimary operation Stent 29 / bypass 6Stent 29 / bypass 6
48
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
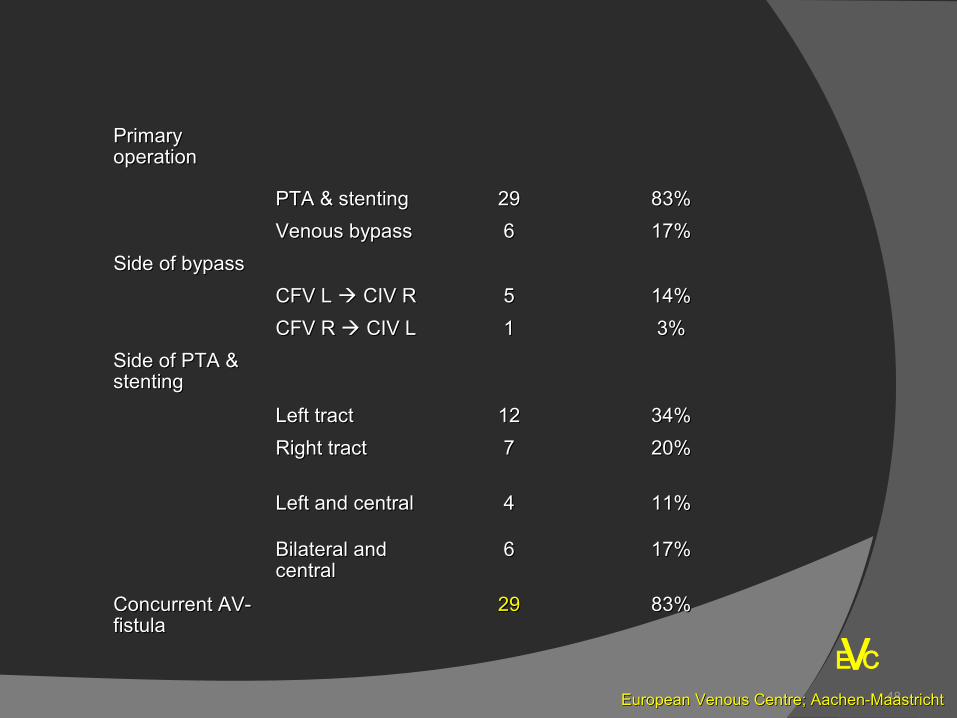
Primary Primary operationoperation
PTA & stentingPTA & stenting 2929 83%83%
Venous bypassVenous bypass 66 17%17%
Side of bypassSide of bypass
CFV L CFV L CIV R CIV R 55 14%14%
CFV R CFV R CIV L CIV L 11 3%3%
Side of PTA & Side of PTA & stentingstenting
Left tractLeft tract 1212 34%34%
Right tractRight tract 77 20%20%
Left and centralLeft and central 44 11%11%
Bilateral and Bilateral and centralcentral
66 17%17%
Concurrent AV-Concurrent AV-fistulafistula
2929 83%83%

49
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Results - interventionResults - intervention
ReocclusionReocclusion 1111 31%31%
Wound infectionWound infection 33 9%9%
Lymph leakageLymph leakage 33 9%9%
SeromaSeroma 22 6%6%
Bleeding majorBleeding major 11 3%3%
Bleeding minorBleeding minor 11 3%3%
Pulmonary embolismPulmonary embolism 00 0%0%
MortalityMortality 00 0%0%
50
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
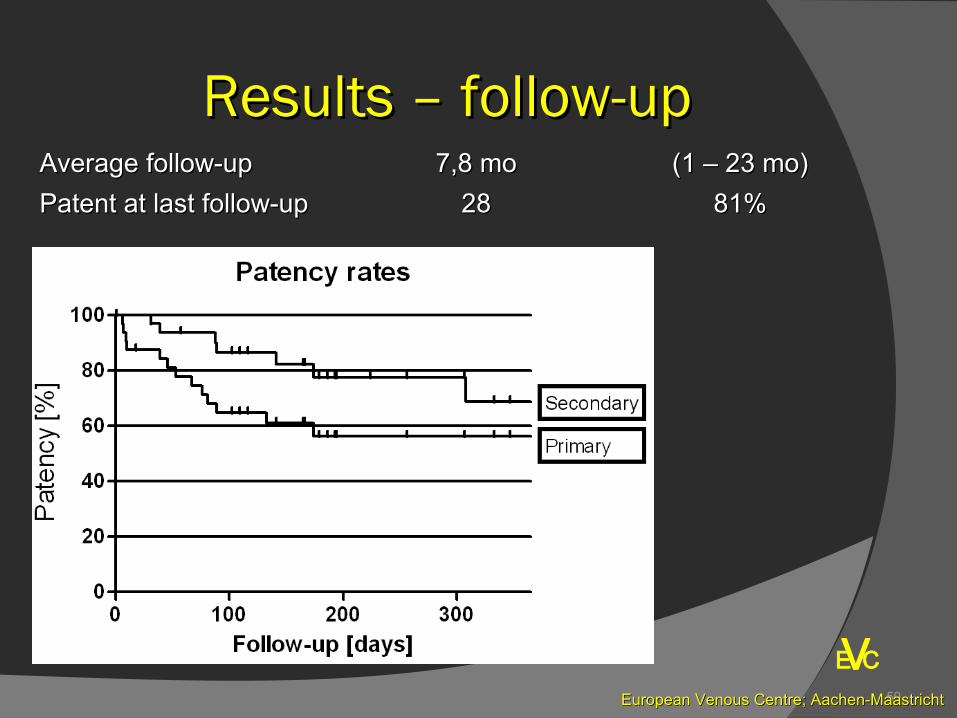
Results – follow-upResults – follow-upAverage follow-upAverage follow-up 7,8 mo7,8 mo (1 – 23 mo)(1 – 23 mo)
Patent at last follow-upPatent at last follow-up 2828 81%81%
51
VEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Treatment options: Treatment options: miscellaneousmiscellaneous
Improved inflow measures / timingImproved inflow measures / timing○ AV fistulaeAV fistulae
SurgicalSurgicalPercutaneous (future)Percutaneous (future)
○ Postoperative pneumatic compression !!Postoperative pneumatic compression !!
Improved anticoagulationImproved anticoagulation○ Oral “Heparines”Oral “Heparines”
E C
52
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Conclusion on Conclusion on endophlebectomyendophlebectomy
Endophlebectomy is relatively safeEndophlebectomy is relatively safe
○ Associated with low complications rates Associated with low complications rates
○ Except reocclusionExcept reocclusion However good secondary patency rateHowever good secondary patency rate
○ Indications AV fistulae ?Indications AV fistulae ?
Future:Future:
○Stenting into CFV or endophlebectomy tract?Stenting into CFV or endophlebectomy tract?
○Better AV fistulae?Better AV fistulae?
○Need for patches?Need for patches?
53
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Conclusion in DVO:Conclusion in DVO:
What is new DVO treatment:What is new DVO treatment:
Potential impact on practice to treat Potential impact on practice to treat
DVO and PTS:DVO and PTS:
○ In Turkey In Turkey > 500.000 people> 500.000 people
have a significant deep venous outflow have a significant deep venous outflow
obstrucion:obstrucion:
Major impact if this treatment become routineMajor impact if this treatment become routine
54
VE CEuropean Venous Centre; Aachen-MaastrichtEuropean Venous Centre; Aachen-Maastricht
Overall ConclusionOverall Conclusion
New DVT treatment optionsNew DVT treatment optionsIn patients with a LET III or IV DVTIn patients with a LET III or IV DVT
Better thrombectomie devicesBetter thrombectomie devices
Better stentsBetter stents
Improve QoLImprove QoL
Acute symptome relieveAcute symptome relieve
Reduce PTSReduce PTS
Reduce recurrent DVTReduce recurrent DVT
New DVO treatment optionsNew DVO treatment optionsIn patients with iliofemoral/caval occlusive diseaseIn patients with iliofemoral/caval occlusive disease
Better stentsBetter stents
EndophlebectomyEndophlebectomy
AV fistulaeAV fistulae
NOAC’sNOAC’s
Improve QoL !! Improve QoL !! Thank youThank you