Embed Size (px)
Citation preview

Collaborating for Better
Care Partnership
Master Class: ‘Using implementation science to transform patient care’
1st September 2014
International Centre for Life
@AHSN_NENC@JPresseau

Welcome and Introduction
Dr Jackie Gray
on behalf of
Ian Renwick
Chair, Collaborating for Better Care Partnership
(Chief Executive, Gateshead Health NHS Foundation Trust)

Programme09.00 Welcome
09.15 ‘Reducing variation of avoidable deaths through NIV interventions: a working case study’ Avril Lowery, Head of SafeCare, Gateshead Health NHS Foundation Trust
09.35 An overview of the ‘Knowledge to Action’ model of Implementation Science
Professor Jeremy Grimshaw
10.15 Refreshment Break
10.30 Implementation of Guidance Workshop
Workshop 1 - COPD - facilitated by Professor Jeremy Grimshaw
Workshop 2 - End of Life Care for Frail Elderly – facilitated by Dr Justin Presseau
12.00 Lunch
12.45 Implementation Workshop (Group Work and feedback)
Workshop 1 - COPD- facilitated by Professor Jeremy Grimshaw
Workshop 2 - End of Life Care for Frail Elderly – facilitated by Dr Justin Presseau
13.45 Workshop Feedback
14.15 Building organisational capacity to address clinical variation and raise standards of care
(including Q & A session)
14.45 Conclusions, Professor Jeremy Grimshaw
14.55 Next steps – action planning
15.00 Close

Reducing variation of avoidable
deaths through NIV interventions:
a working case study
Avril Lowery
Head of SafeCare,
Gateshead Health NHS Foundation Trust

Reducing variation of avoidable deaths through NIV interventions: a working case study’
Avril Lowery
Head of SafeCare
Gateshead Health NHS Foundation Trust

Background Chronic Obstructive Pulmonary Disease (COPD) is an overarching term used to
describe a number of conditions including chronic bronchitis, emphysema, chronic obstructive airways disease and chronic airflow limitation.
COPD affects 3 million people in the UK and remains the 5th most common cause of death
More than 9% of > 45year olds in Gateshead area will suffer from this condition and 25 % will die from it.
NICE Quality Standard 10 COPD Statement 11- People admitted to hospital with an exacerbation of COPD with a persistent acidotic ventilatory failure are promptly assessed for, and receive, non invasive ventilation delivered by appropriately trained staff in a dedicated setting
Prompt assessment and receipt of NIV should be defined as: assessment and receipt of NIV within 3 hours of presentation, and receipt of NIV within 1 hour of the decision being made to administer NIV.

Background Non-invasive ventilation (NIV) is a method of providing ventilatory support that
does not require the placement of an endotracheal tube. It is usually delivered via a mask that covers the nose, but occasionally a full face mask covering the nose and the mouth is required. NIV is most commonly used to treat acute respiratory failure during exacerbations of COPD
Large body of evidence illustrates that when used well, ward-based Non Invasive Ventilation has many positive outcomes :
Reduces mortality rate from AECOPD by 50% (i.e. reducing in-patient mortality from 20 to 10% and number needed to treat to save 1 life is 10 – similar to thrombolysis benefit in Acute myocardial infarction)
Reduce critical care department (CCD) admissions for respiratory failure secondary to AECOPD by 44%,
Improves survival of these patients at three months and one year, Is cost effective via preventing CCD admissions, Reduced length of stay by average 4.5 days for NIV treated patients
A need to improve delivery and timing of NIV for AECOPD across QEH

Patient pathway to NIV at QE Gateshead
Drivers for change at Gateshead NIV service set up in early 2000’s and unchanged since 1,115 patients/year admitted with AECOPD. 71 patients/year receive NIV for AECOPD National audit data would suggest that we should expect to treat
290 patients/year with NIV. Missing up to 19 patients/ month due to bed pressures &
requirement for NIV not being recognised in all appropriate patients
Limited to being delivered on respiratory ward or CCD Provision for only 3 patients at any one time Rarely beds immediately available on respiratory ward Sub-optimal initial treatment Delay in commencement of NIV Staffing – relied on ward nursing staff -24 beds

Drivers for Change Poor outcomes compared to national audit results:
Mortality - for all NIV patients 40% in 2012 (31% nationally)
Readmissions - e.g. 1 of the 4 patients who potentially could have benefited from NIV in one month readmitted within 30 days of discharge
LOS - patients treated on CCD have delays in transfer to respiratory ward for ongoing care – slows discharge home
Failure to meet target of NIV within 1 hour of failed maximal medical therapy
• time to NIV for A&E admissions 5 hours
• Time to NIV for patients admitted to CCD from A&E median of 2.5 hours
What did we do ? Weekly multidisciplinary ward base case review well
established - Hogan and NCEPOD outcome scores introduced more recently
Presentation of cases and key learning at M&M steering group – supported business case for development of NIV service
Funding for 4 new IV machines (£300,000)
4.8 WTE band 6 specialist nurses to provide 24/7 NIV nurse led service (£300,000)
Further non- recurrent funding £15,000 ( training & education etc.)
Some minor structural changes
Anticipated benefits of new nurse led service
Early involvement in AECOPD across whole TrustOptimisation of treatment ( preventing oxygen toxicity)Early arterial blood gases Commencement of NIV in A&E and any ward areaPrompt transfer to respiratory ward for ongoing care Identification of patients who may benefit from critical
care involvementContinued support and follow up for patients
established on NIV Education and teaching throughout Trust Potential reduced LOS = cost savings Timely, safe, streamlined patient pathway
Early results
Early evidence that the service is working well for patients and meeting national standards
Service is now seeing and assessing 100 patients per month An average of 15 patients per month starting treatment with Non-
Invasive Ventilation - double the number of patients previously. This is being achieved within one hour in 100% of patients in line
with BTS guideline recommendations. Our data indicates that NIV is successful in 76% of patients, an
improvement on 66% in 2012. Our COPD patients treated with NIV now match trial mortality rates
(10% in-patient mortality) and all cause in-patient mortality matches other large cohorts within the literature (33%, previously being 40% in 2012).

Key enablers
Trust commitment to high quality care
Development of the Trust Morality and Morbidity governance framework
Leadership and clinical ‘buy in’
Learning from multidisciplinary case reviews
Key challenges
Funding
Staffing
Clinical expertise and availability
Some resistance from non clinical to set up costs

The Future…
Expansion of service
Growth of team
Protected NIV beds
Widen patient criteria
Education &
Awareness

The future for improvement
Continue to develop and embed multidisciplinary review of deaths
Ensure key learning is shared and developed into action to improve patient care and pathways
Continue to develop systems for meaningful data collection to provide assurance on the quality of the care we provide our patients/ identify deficits in service provision including the patient & staff perspectives
Encourage collective efforts and team working to enable effective and sustainable change
‘Knowledge to Action’ model
of Implementation ScienceReducing clinical variation
Raising standards of care
Professor Jeremy GrimshawSenior Scientist, Ottawa Hospital Research Institute
Professor, Department of Medicine, University of Ottawa
Canada Research Chair in Health Knowledge Transfer and Uptake
Background
• Consistent evidence of failure to implement evidence based recommendations into clinical practice
– 30-40% patients do not get treatments of proven effectiveness
– 20–25% patients get care that is not needed or potentially harmful
• Suggests that implementation of evidence based recommendations is fundamental challenge for healthcare systems to optimise care, outcomes and costs
Schuster, McGlynn, Brook (1998). Milbank Memorial Quarterly
Grol R (2001). Med Care
Approaches to implementation
ISLAGIATT
principle
Martin P Eccles
‘It Seemed
Like A Good
Idea At The
Time’

Implementation science
• Implementation is a human enterprise that can be studied to understand and improve knowledge translation approaches
• Implementation science is the scientific study of the determinants, processes and outcomes of knowledge translation.
• Goal is to develop a generalisable empirical and theoretical basis to optimise implementation activities
Developing implementation science in the Academic Health
Science Network
Developing implementation
science in the Academic Health
Science Network• To facilitate participants’ use of implementation
science theory & tools to address clinical variation and raise standards of care
• To enable participants to explore their organisational capability with respect to the skills, knowledge, and resources required to address clinical variation and raise standards of care
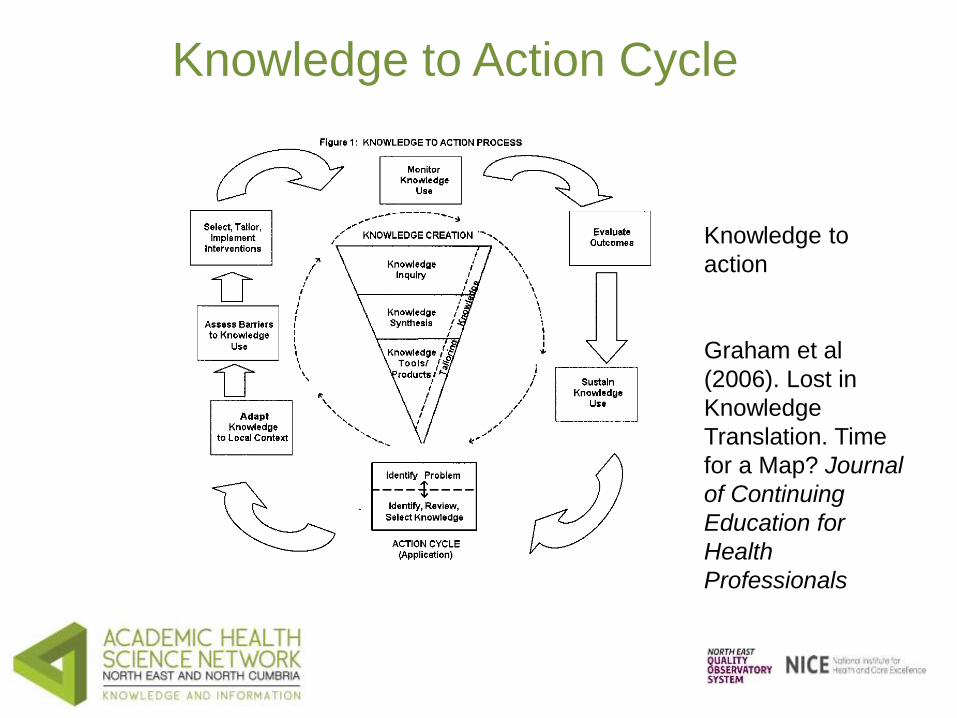
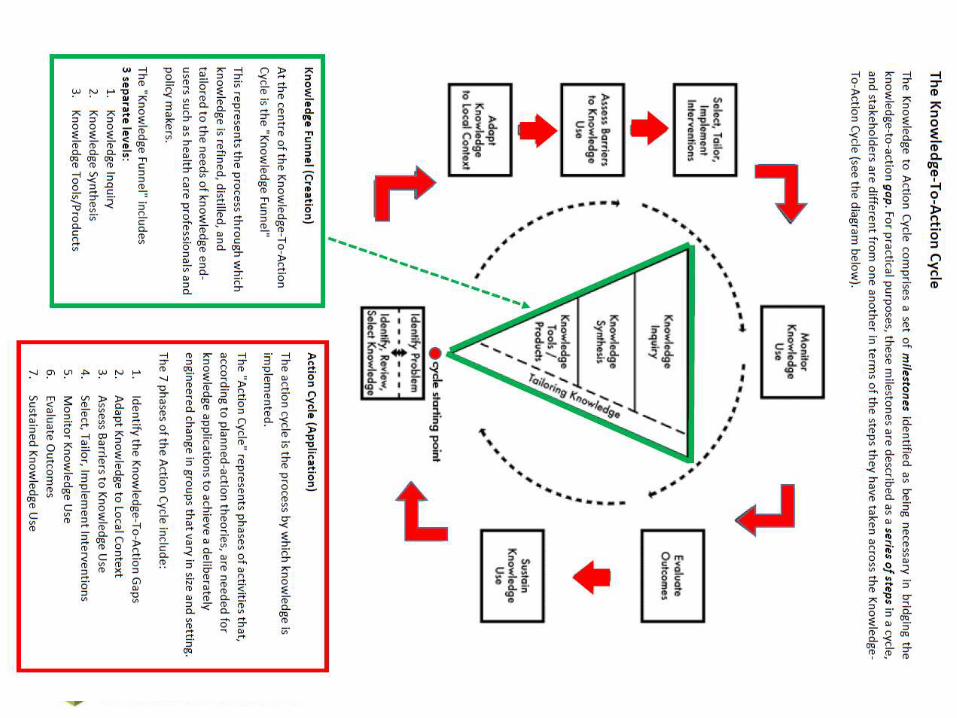
Knowledge to Action Cycle
Knowledge to
action
Graham et al
(2006). Lost in
Knowledge
Translation. Time
for a Map? Journal
of Continuing
Education for
Health
Professionals

Knowledge to Action Cycle

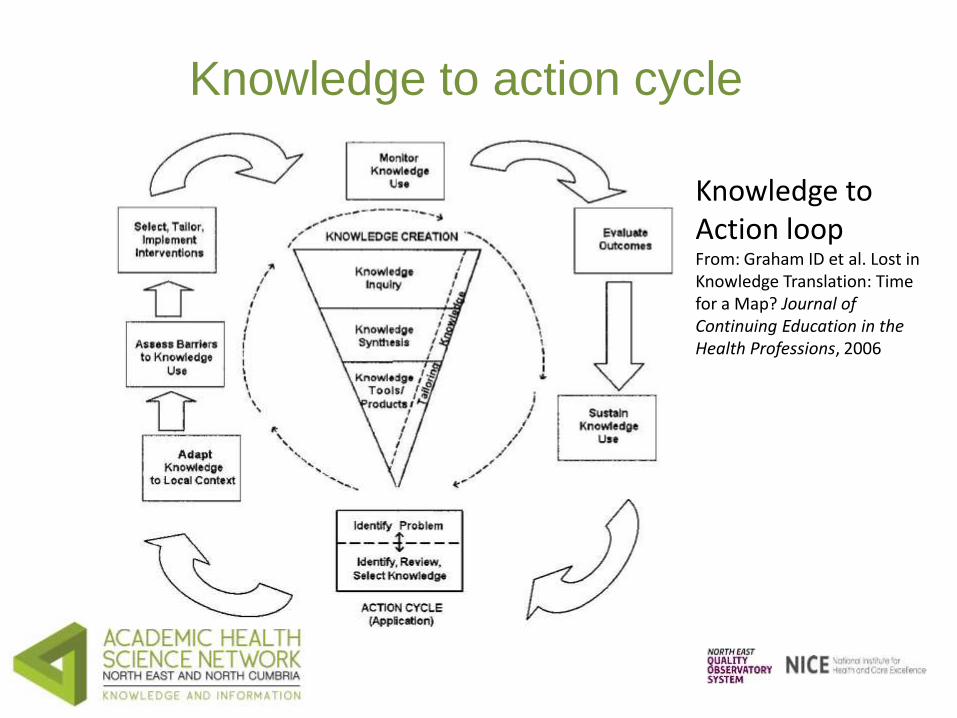
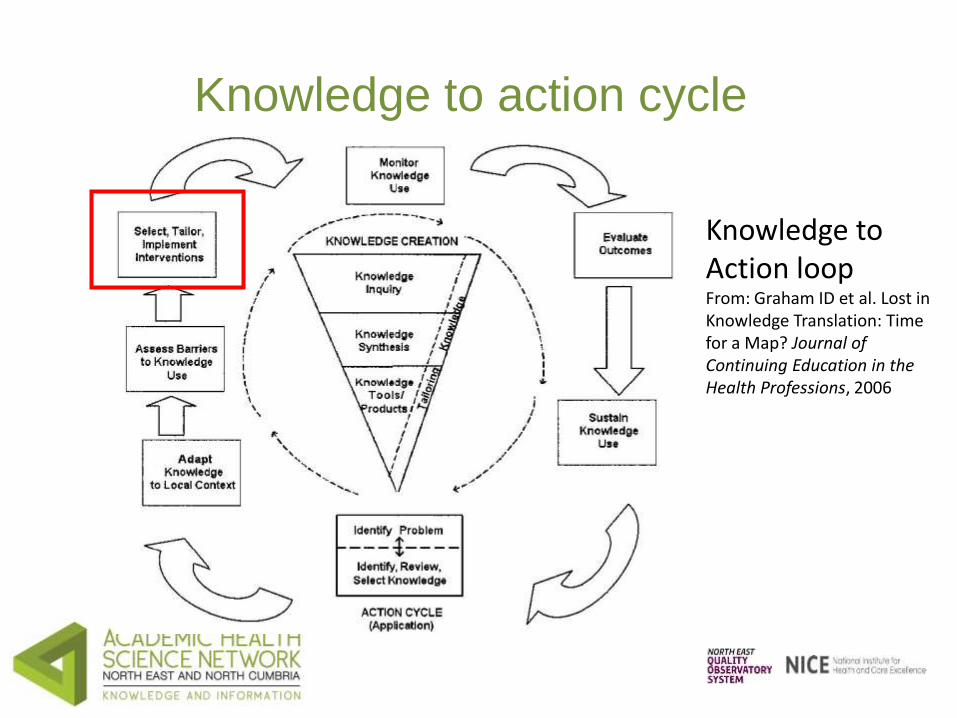
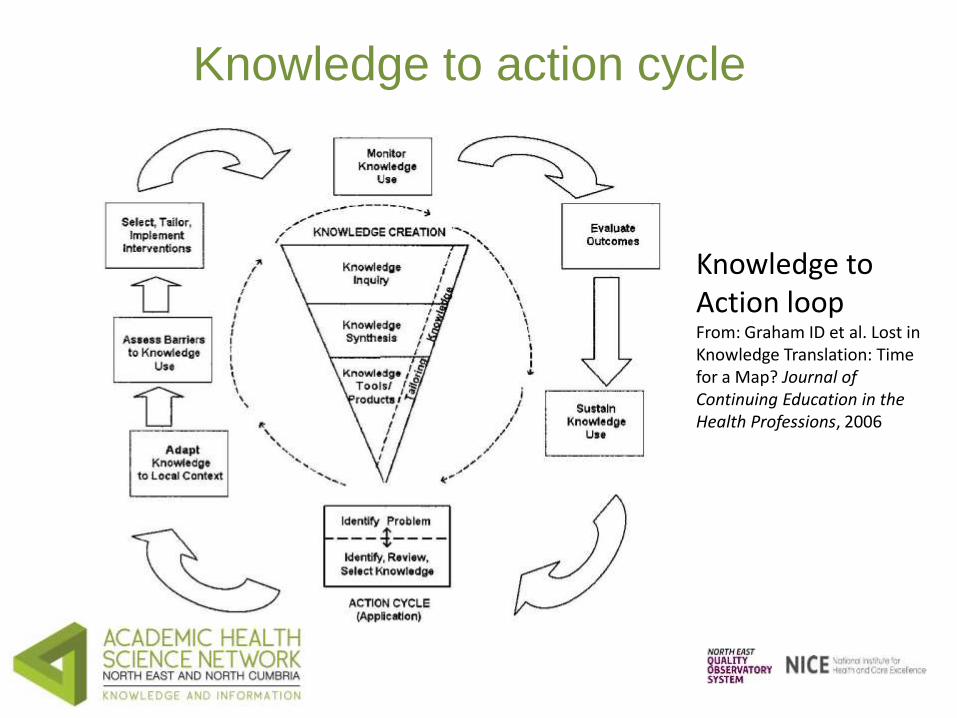
Knowledge to action cycle
Knowledge to
Action loopFrom: Graham ID et al.
Lost in Knowledge
Translation: Time for a
Map? Journal of
Continuing Education in
the Health Professions,
2006
Knowledge creation funnel

Knowledge creation funnel
Knowledge to action cycle
Knowledge to Action loopFrom: Graham ID et al. Lost in Knowledge Translation: Time for a Map? Journal of Continuing Education in the Health Professions, 2006

Knowledge to action cycle
Knowledge to Action loopFrom: Graham ID et al. Lost in Knowledge Translation: Time for a Map? Journal of Continuing Education in the Health Professions, 2006

Specifying behaviours of interest
• What is the behavior (or series of linked behaviors) that you are trying to change?
• Who performs the behavior(s)? (potential adopter)
• When and where does the potential adopter perform the behavior?
• Are there obvious practical barriers to performing the behavior?
• Is the behavior usually performed in stressful circumstances? (potential for acts of omission)
Specifying behaviours of interest
• Often useful to specify target behaviours in terms of:
– Action being performed
– Target at which the action is directed
– Context in which action is performed
– Time during which the action is performed.

Knowledge to action cycle
Knowledge to Action loopFrom: Graham ID et al. Lost in Knowledge Translation: Time for a Map? Journal of Continuing Education in the Health Professions, 2006
Adapting knowledge to local
context
• May require additional data collection to assess applicability of knowledge to local context
• May require modification of recommended actions based upon applicability, resources and contextual issues

Knowledge to action cycle
Knowledge to Action loopFrom: Graham ID et al. Lost in Knowledge Translation: Time for a Map? Journal of Continuing Education in the Health Professions, 2006
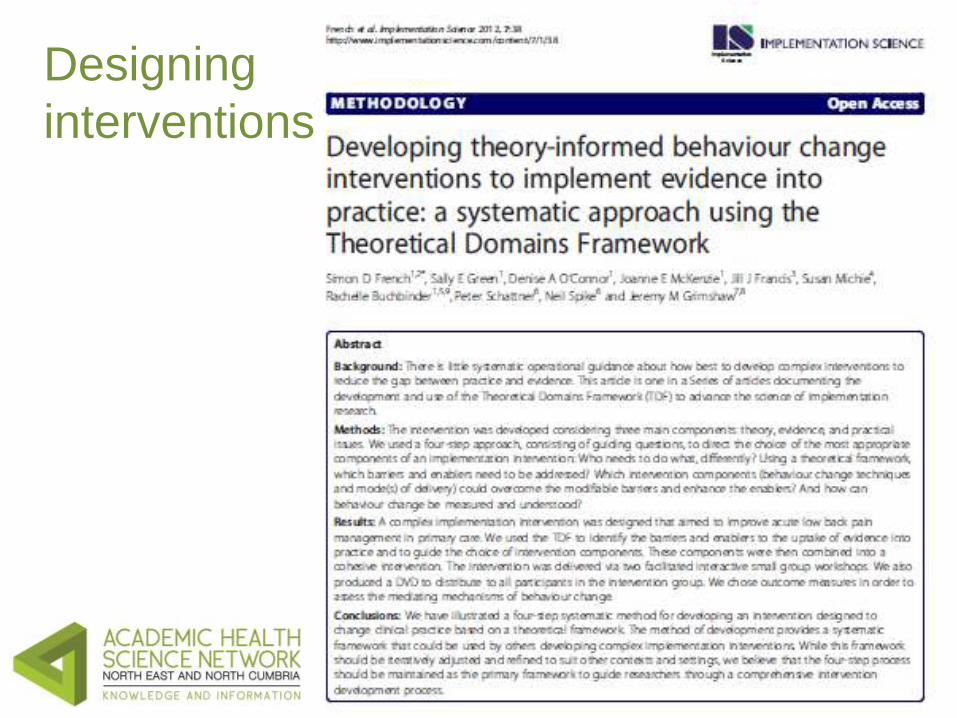
Designing
interventions

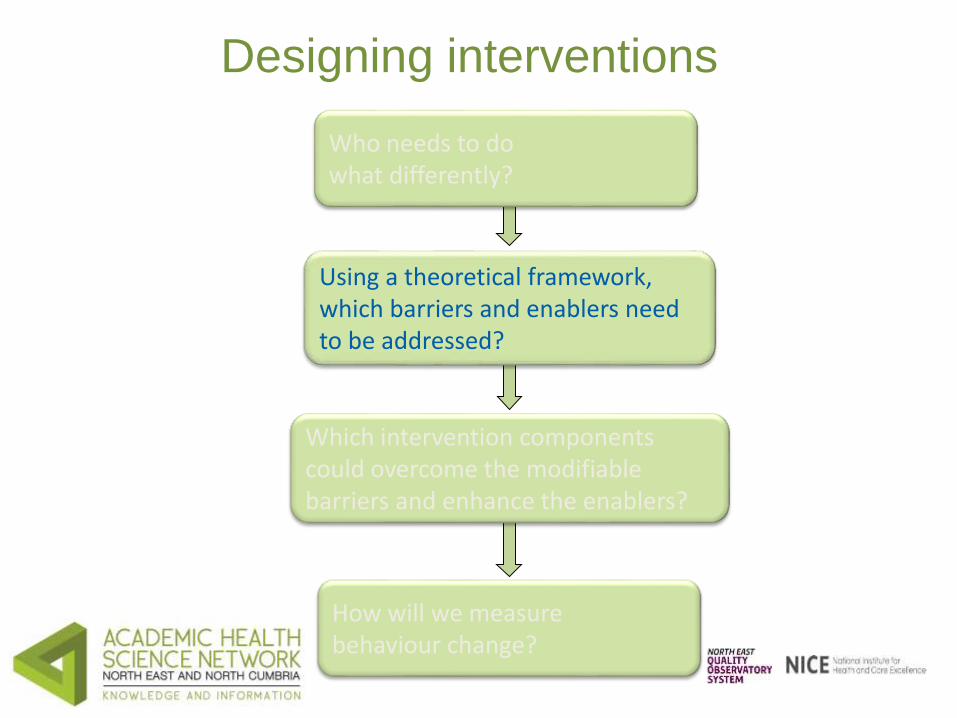
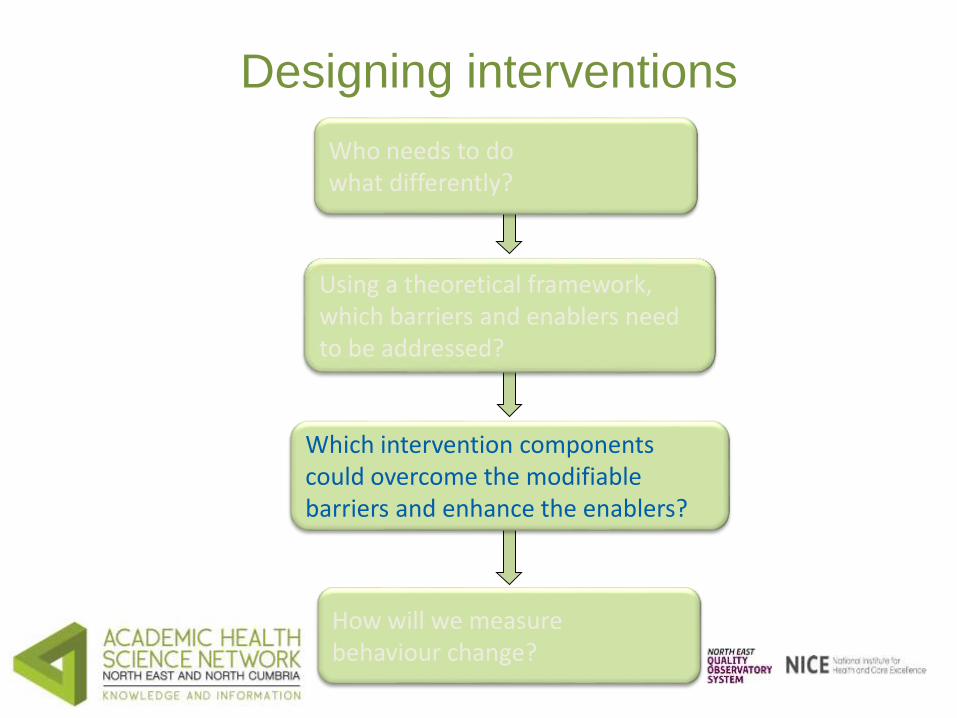
Designing interventions
Who needs to do what differently?
Using a theoretical framework, which barriers and enablers need to be addressed?
Which intervention components could overcome the modifiable barriers and enhance the enablers?
How will we measurebehaviour change?

Knowledge to action cycle
Knowledge to Action loopFrom: Graham ID et al. Lost in Knowledge Translation: Time for a Map? Journal of Continuing Education in the Health Professions, 2006
Designing interventions
Who needs to do what differently?
Using a theoretical framework, which barriers and enablers need to be addressed?
Which intervention components could overcome the modifiable barriers and enhance the enablers?
How will we measurebehaviour change?

Assessing barriers to implementation
• Formal assessment of context, likely barriers to implementation
• Mixed methods
– Literature review
– Informal consultation
– Focus groups
– Surveys
• Needs interdisciplinary perspective

Barriers to implementation
• Structural (e.g. financial disincentives)
• Organisational (e.g. inappropriate skill mix, lack of facilities or equipment)
• Peer group (e.g. local standards of care not in line with desired practice)
• Individual (e.g. knowledge, attitudes, skills)
• Professional - patient interaction (e.g. problems with information processing)
Theoretical
Domains
framework
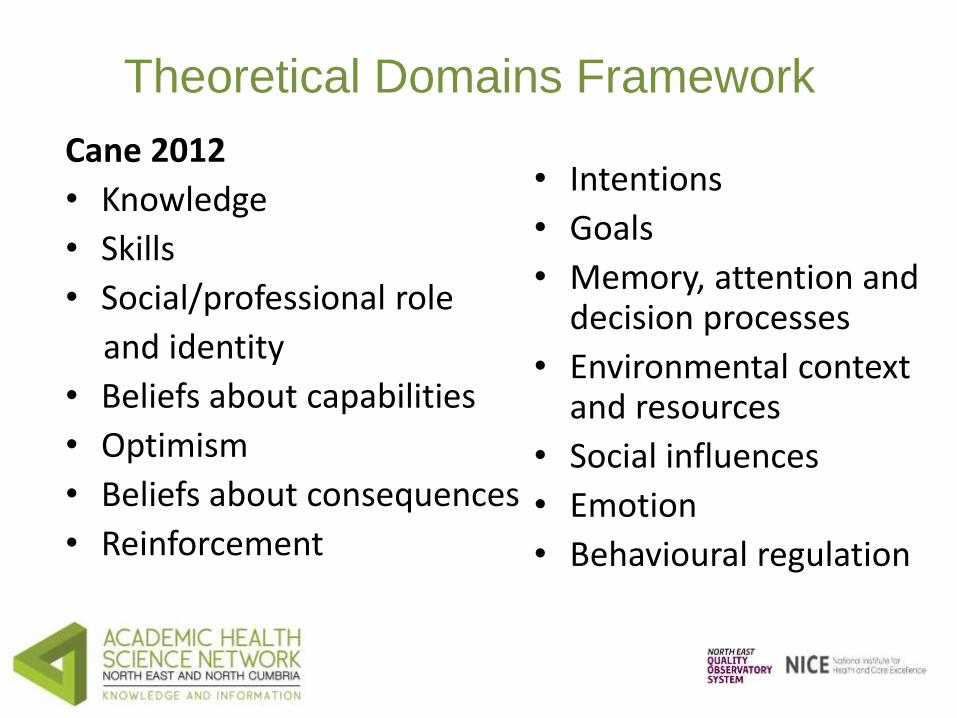
Theoretical Domains Framework
Cane 2012
• Knowledge
• Skills
• Social/professional role
and identity
• Beliefs about capabilities
• Optimism
• Beliefs about consequences
• Reinforcement
• Intentions
• Goals
• Memory, attention and decision processes
• Environmental context and resources
• Social influences
• Emotion
• Behavioural regulation
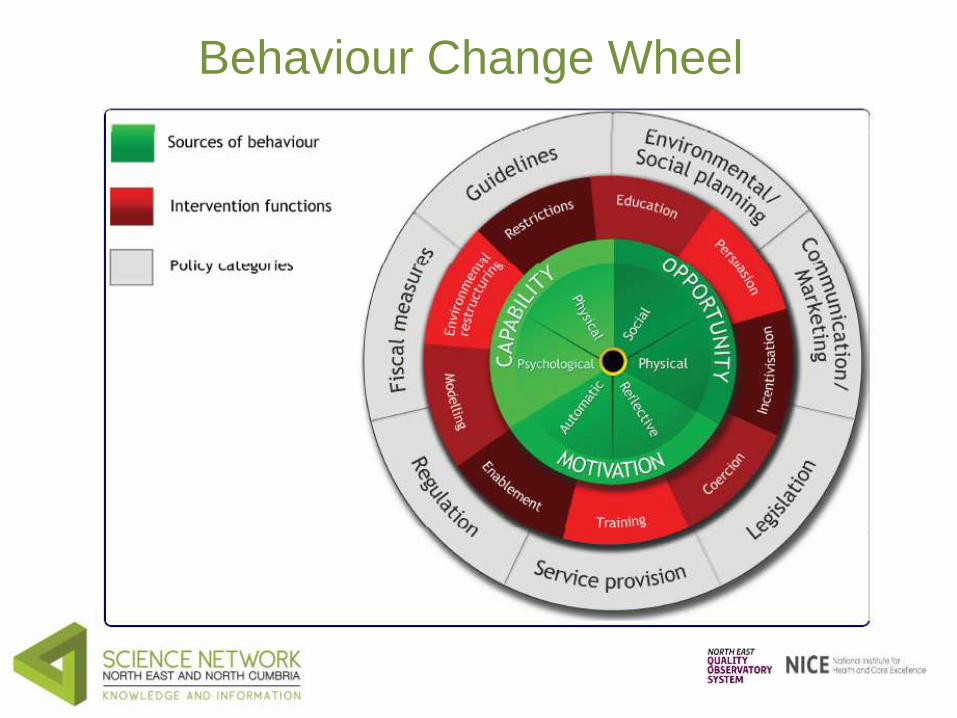
Behaviour Change Wheel

Behaviour Change Wheel
Ability• Physical • Psychological
Conscious and automatic decision processes
Environmental factors • Physical• Social
Knowledge to action cycle
Knowledge to Action loopFrom: Graham ID et al. Lost in Knowledge Translation: Time for a Map? Journal of Continuing Education in the Health Professions, 2006
Designing interventions
Who needs to do what differently?
Using a theoretical framework, which barriers and enablers need to be addressed?
Which intervention components could overcome the modifiable barriers and enhance the enablers?
How will we measurebehaviour change?

Designing interventions

Designing interventions
• Scheduled consequences• Reward and threat• Repetition and substitution• Antecedents• Associations• Covert learning• Natural consequences
• Health consequences• Feedback and monitoring• Goals and planning• Social support• Comparison of behaviour• Self belief• Comparison of outcomes• Identity• Shaping knowledge• Regulation

Designing interventions
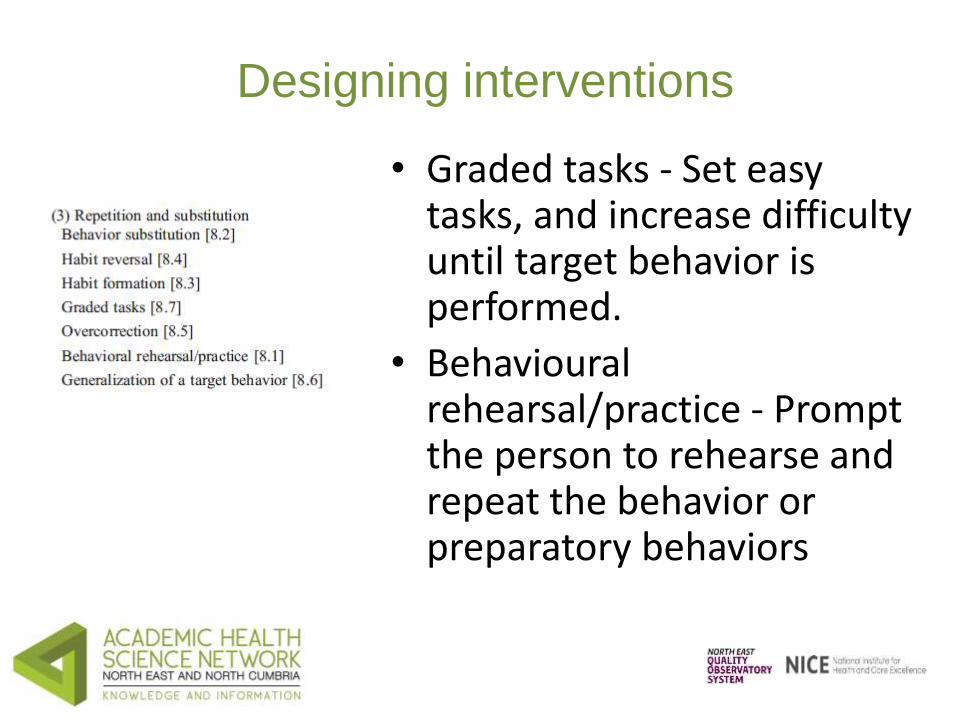
Designing interventions
• Graded tasks - Set easy tasks, and increase difficulty until target behavior is performed.
• Behaviouralrehearsal/practice - Prompt the person to rehearse and repeat the behavior or preparatory behaviors

Designing interventions
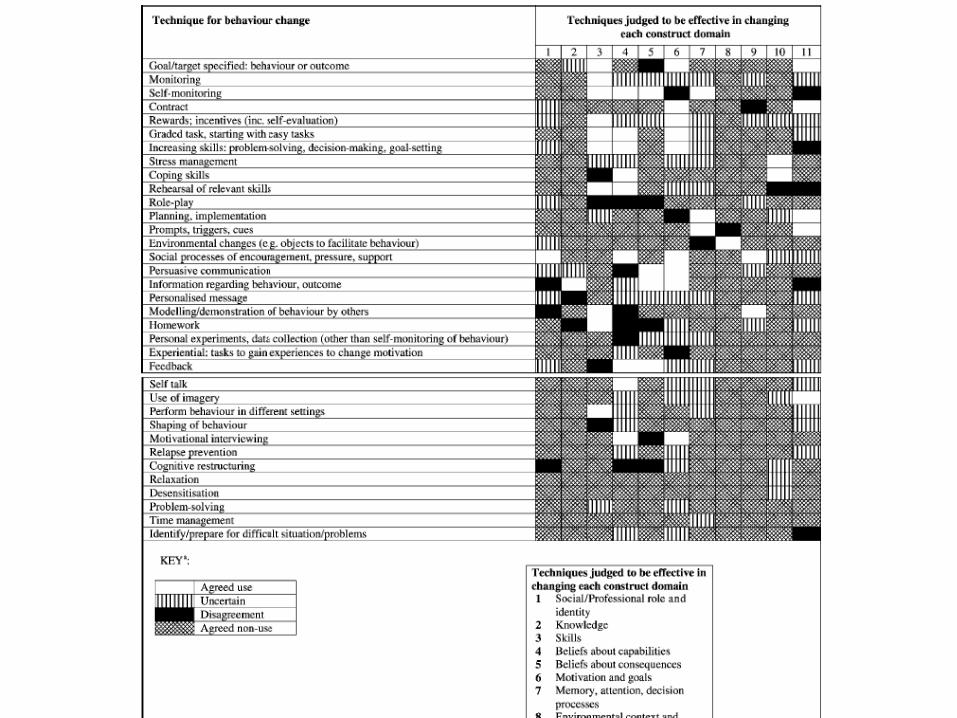

Designing interventions
Behaviour Change Techniques
Modes of Delivery
Theory / Mediators
Designing interventions
Usability studies• Develop prototype intervention• Test prototype in 5 to 8 subjects to review content and
format using ‘think aloud’ methodology. These sessions will be audio recorded and the results transcribed and analysed.
• In general a modest number of subjects are required for usability testing (e.g. 8-9 subjects), and often 4 to 5 are necessary to identify 80% of the usability problems.
• Cycles of design, development and testing will be completed until no further major revisions are needed.
Knowledge to action cycle
Knowledge to Action loopFrom: Graham ID et al. Lost in Knowledge Translation: Time for a Map? Journal of Continuing Education in the Health Professions, 2006
Implementation of Guidance
Workshops:
Workshop 1 COPD – facilitated by Prof Jeremy Grimshaw
Workshop 2 End of Life Care for Frail Elderly –facilitated by Dr Justin Presseau

Workshop Feedback
Building organisational capacity
to address clinical variation and
raise standards of care
(including Q & A session)

Conclusions
Professor Jeremy Grimshaw
Next steps – action planning/
future Master Class

Promoting use of implementation
science beyond this session

How many of you are motivated to
use the tools we used today in
your own setting?
Motivation is rarely enough to
ensure change
Two simple but remarkably
effective strategies
• Clearly, concrete description of when, where, and how you will perform an action
• Anticipated barriers to you performing that action, and realistic solutions to circumvent the barrier
• Demonstrated to help promote good intentions being translated into action

Taking today’s insights forward into your
organisation: when, where & how
• Step 1: choose and write an action that you want to take in your organisation to apply what we have covered today.
• Step 2: Write:– When you will do it (be specific)
– Where you will do it (be specific)
– How you will do it (be specific)
• 3 mins
The best laid plans…
• Now, imagine yourself enacting that when, when and how plan.
• Can you envisage anything preventing you from doing it?
• How would you feasibly address that barrier?
• Write:– IF barrier __________________________ occurs– THEN I WILL ________________________ to ensure I
can enact my plan

Closing remarks
Dr Jackie Gray
NEQOS
Get involved in the Work
Programme
• Sign up at the registration desk (in main foyer)
or
• Email Dr Jackie Gray [email protected]

Keep up to date with developments:• Sign up for the e- bulletin at the registration desk
(if you haven’t already)
Resources will be available on:
You Tube - video will be uploaded (a link included in next e- bulletin)
Slide Share - slide deck will be uploaded (link included in next e-bulletin)
AHSN web site www.ahsn-nenc.org.uk
NEQOS web site www.neqos.nhs.uk/
Twitter - @AHSN_NENC
Additional materials from the
workshop sessions
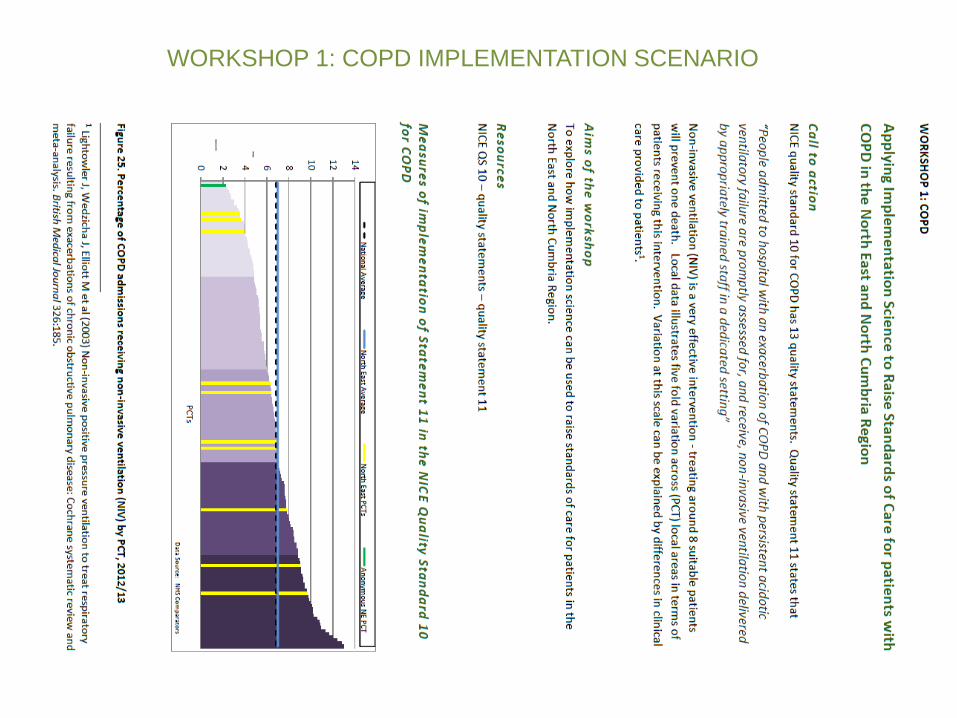
WORKSHOP 1: COPD IMPLEMENTATION SCENARIO
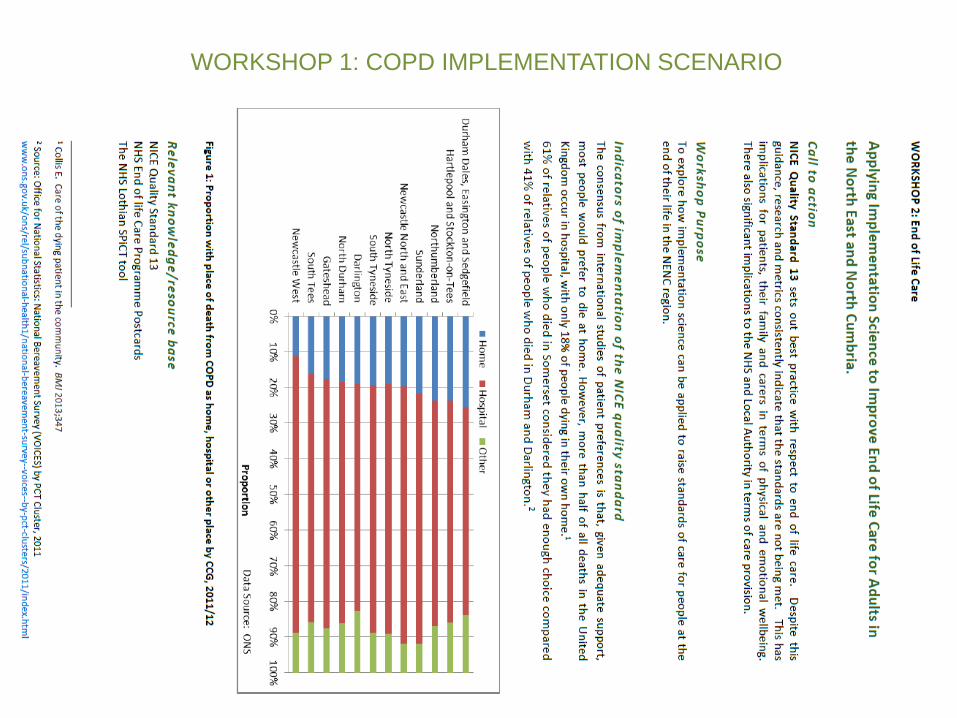
WORKSHOP 1: COPD IMPLEMENTATION SCENARIO




Thank you





























