Embed Size (px)
Citation preview
Contemporary Management Of Primary Varicose Veins
Mohamed SalahVascular Surgery Department
Mataryia Teaching Hospital
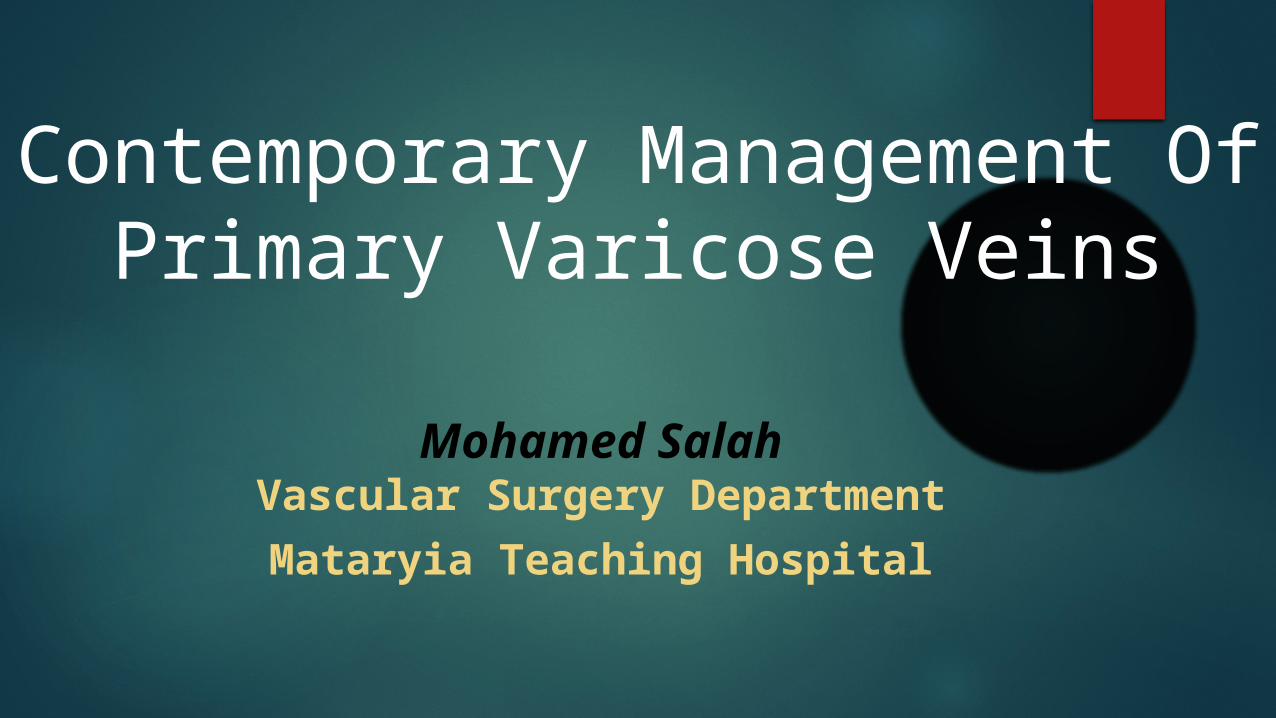
CLASSIFYING VENOUS DISEASECEAP
The classification was based on clinical manifestations (C), etiological factors (E), anatomic distribution of disease (A), and the underlying pathophysiologic findings (P)
CLINICAL CLASSIFICATION:
C0: No visible or palpable signs of venous disease
C1: Telangiectasias or reticular veins:
Telangiectasia : A confluence of dilated intradermal venules of less than 1 mm in caliber. Synonyms include “spider veins,” “hyphen webs,” and “thread veins ”.
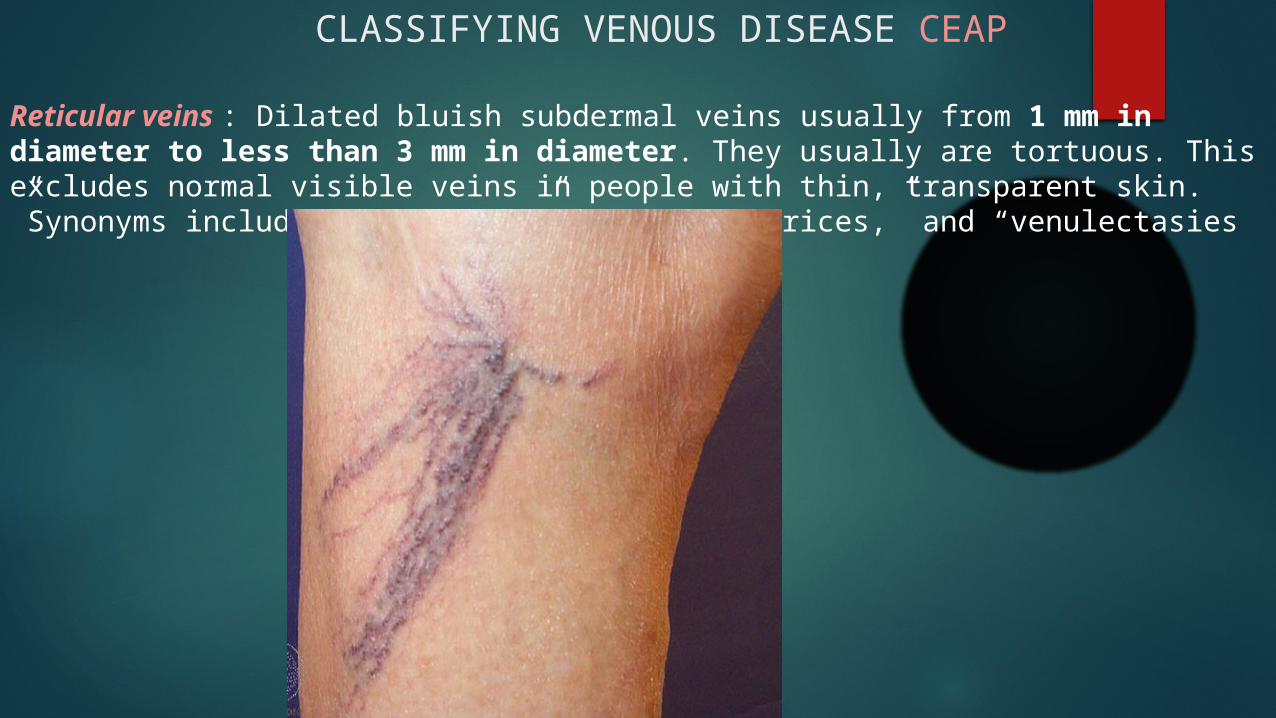
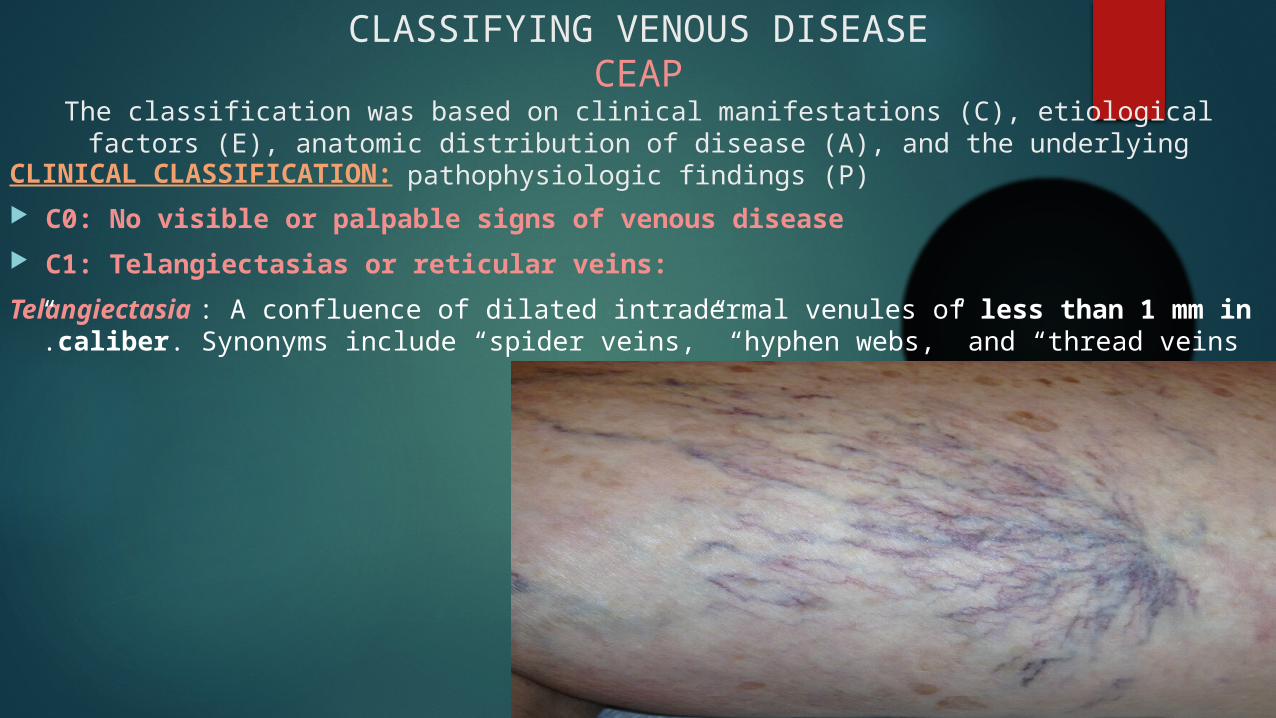
Reticular veins : Dilated bluish subdermal veins usually from 1 mm in diameter to less than 3 mm in diameter. They usually are tortuous. This excludes normal visible veins in people with thin, transparent skin. Synonyms include “blue veins,” subdermal varices,” and “venulectasies”
CLASSIFYING VENOUS DISEASE CEAP
CLASSIFYING VENOUS DISEASE CEAP CLINICAL CLASSIFICATION:
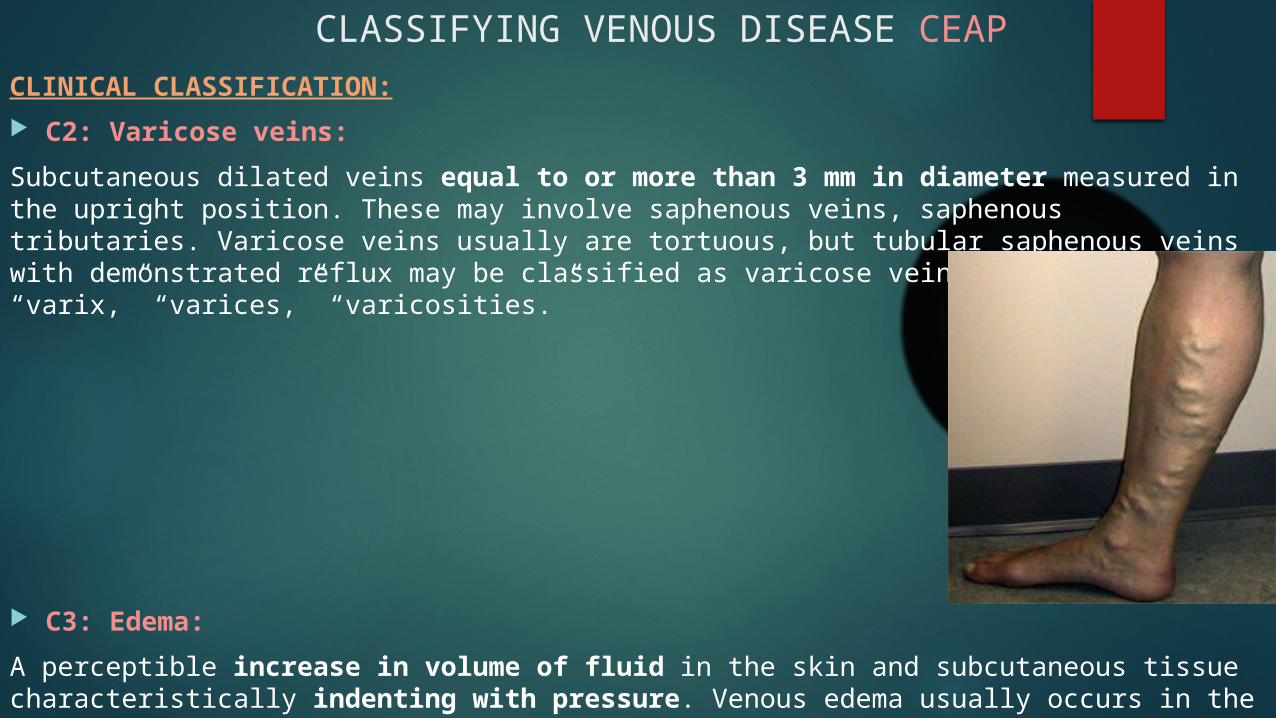
C2: Varicose veins:
Subcutaneous dilated veins equal to or more than 3 mm in diameter measured in the upright position. These may involve saphenous veins, saphenous tributaries. Varicose veins usually are tortuous, but tubular saphenous veins with demonstrated reflux may be classified as varicose veins. Synonyms include “varix,” “varices,” “varicosities.”
C3: Edema:
A perceptible increase in volume of fluid in the skin and subcutaneous tissue characteristically indenting with pressure. Venous edema usually occurs in the ankle region, but it may extend to the leg and foot.
CLINICAL CLASSIFICATION:
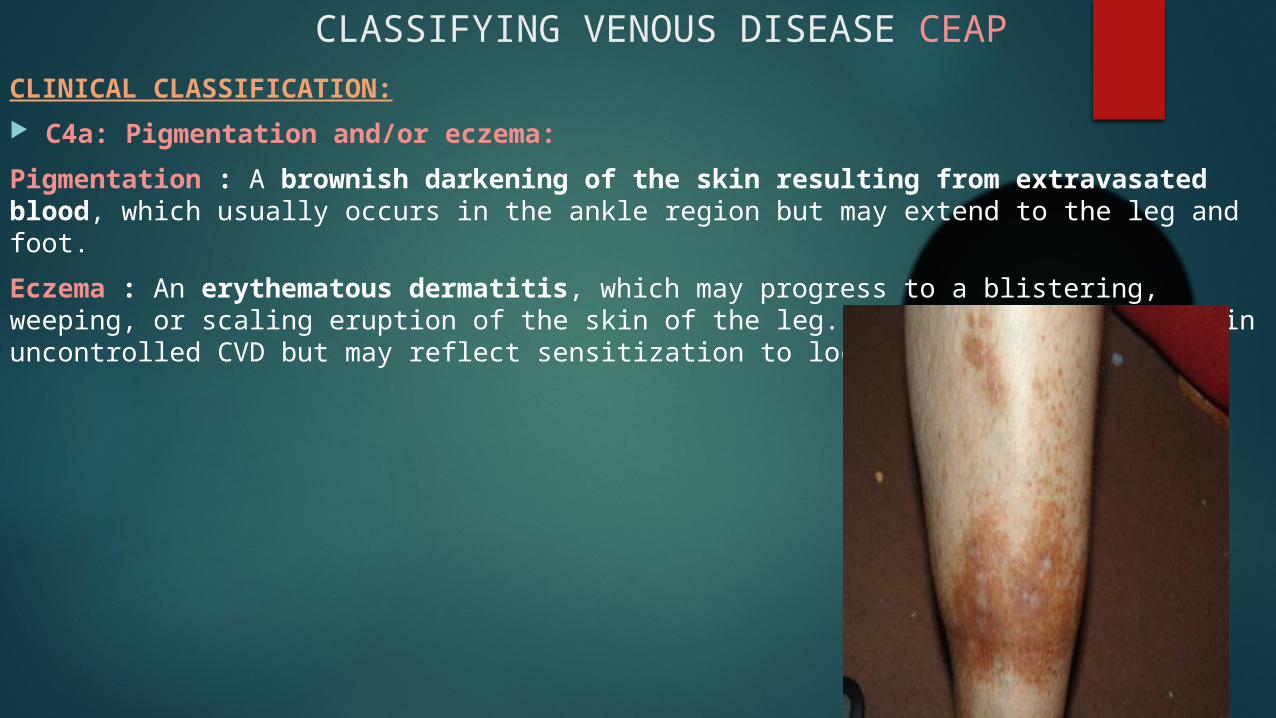
C4a: Pigmentation and/or eczema:
Pigmentation : A brownish darkening of the skin resulting from extravasated blood, which usually occurs in the ankle region but may extend to the leg and foot.
Eczema : An erythematous dermatitis, which may progress to a blistering, weeping, or scaling eruption of the skin of the leg. Eczema usually is seen in uncontrolled CVD but may reflect sensitization to local therapy.
CLASSIFYING VENOUS DISEASE CEAP
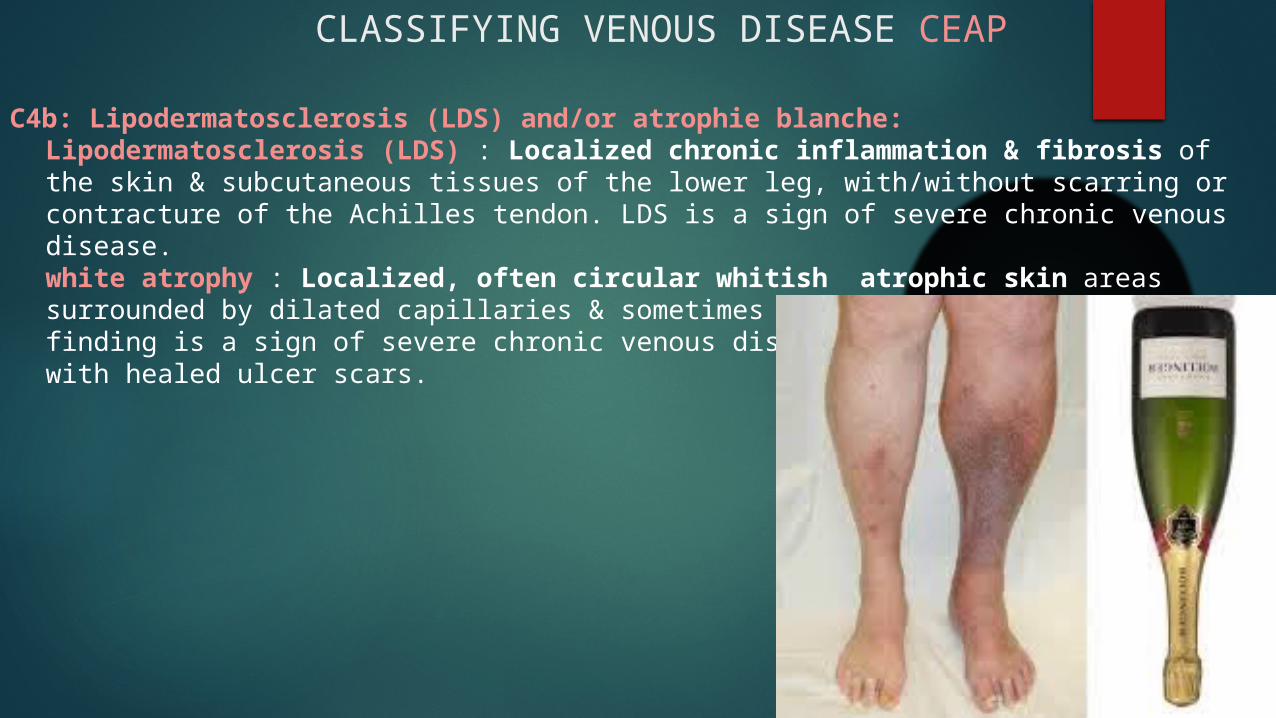
C4b: Lipodermatosclerosis (LDS) and/or atrophie blanche:Lipodermatosclerosis (LDS) : Localized chronic inflammation & fibrosis of the skin & subcutaneous tissues of the lower leg, with/without scarring or contracture of the Achilles tendon. LDS is a sign of severe chronic venous disease.white atrophy : Localized, often circular whitish atrophic skin areas surrounded by dilated capillaries & sometimes hyperpigmentation. This finding is a sign of severe chronic venous disease and not to be confused with healed ulcer scars.
CLASSIFYING VENOUS DISEASE CEAP
CLINICAL CLASSIFICATION:
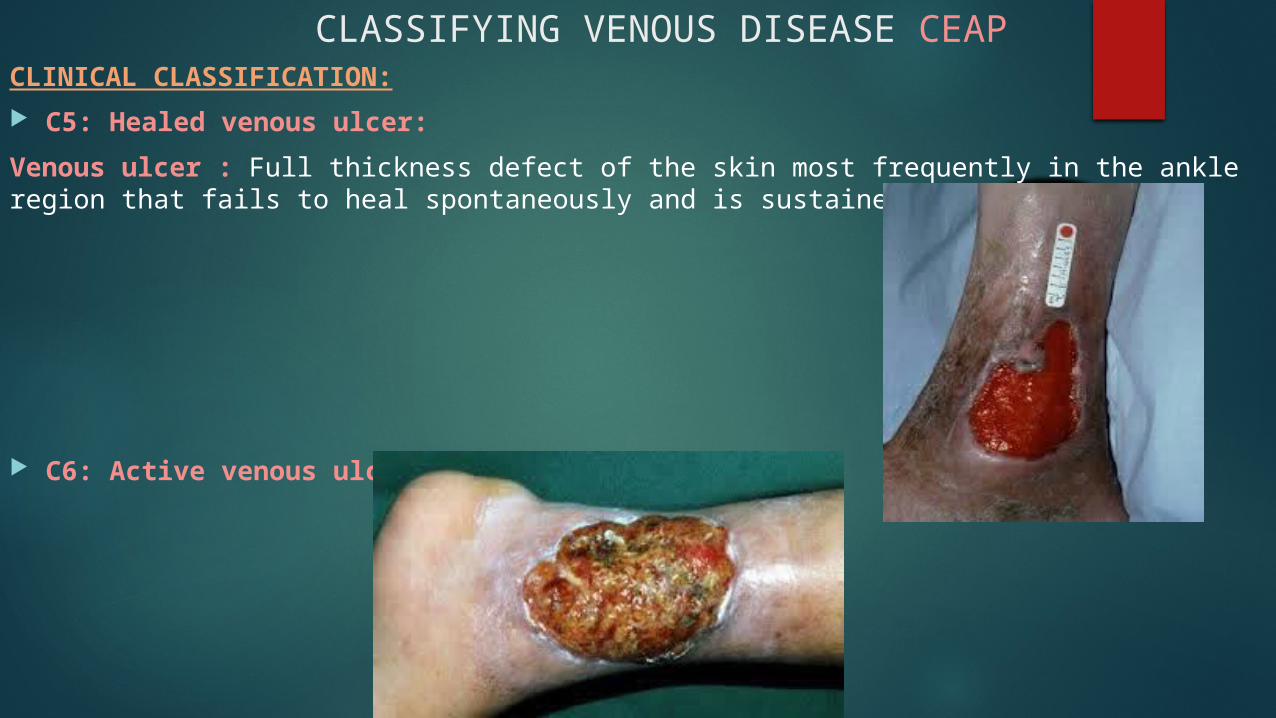
C5: Healed venous ulcer:
Venous ulcer : Full thickness defect of the skin most frequently in the ankle region that fails to heal spontaneously and is sustained by CVD.
C6: Active venous ulcer:
CLASSIFYING VENOUS DISEASE CEAP
ETIOLOGIC CLASSIFICATION:
Ec: Congenital
Ep: Primary
Es: Secondary (post-thrombotic)
En: No venous etiology identified
ANATOMIC CLASSIFICATION:
As: Superficial veins
Ap: Perforator veins
Ad: Deep veins
An: No venous location identified
PATHOPHYSIOLOGIC CLASSIFICATION:
Pr: Reflux
Po: Obstruction
Pr,o: Reflux and obstruction
Pn: No venous pathophysiology identifiable
CLASSIFYING VENOUS DISEASE CEAP
PATIENT WITH PRIMARY VENOUS INSUFFICIENCYHow to Examine?
SYMPTOMS OF VARICOSE VEINS AND TELANGIECTASIAS:
Aching Heaviness (on standing, prolonged sitting) Aching Pain (on standing, prolonged sitting) Burning (venous neuropathy) Itching (cutaneous inflammation) Nocturnal Cramps (recumbent edema reduction)
PATIENT WITH PRIMARY VENOUS INSUFFICIENCYHow to Examine?
PHYSICAL EXAMINATION:
These tests have been laid aside largely because of their lack of specificity and sensitivity. The continuous-wave Doppler examination has replaced most of these tests, yet a trained physician should have a medical background of these tests:
Trendelenburg Test
A tourniquet may be placed around the patient’s proximal thigh while the patient is standing. The patient then assumes the supine position with the affected leg elevated 45 degrees. The tourniquet is removed, and the time required for the leg veins to empty, which is indicative of the adequacy of venous drainage, is recorded.
Cough Test
One hand is placed gently over the GSV or saphenofemoral junction (SFJ), and the patient is asked to cough or perform a Valsalva maneuver. Simply palpating an impulse over the vein being examined may be indicative of insufficiency of the valve at the SFJ and below to the level of the palpating hand.
Schwartz Test
One hand is placed over the SFJ or saphenopopliteal junction (SPJ), and the other hand is used to tap very lightly on a distal segment of the GSV or small saphenous vein (SSV). The production of an impulse in this manner implies insufficiency of the valves in the segment between the two hands. Confirmation of the valvular insufficiency can be achieved by tapping proximally while palpating distally.
Management of a patient with primary varicose veins: Duplex study, what to know!?
Selection criteria: CEAP clinical stages from 2 to 6 The Edinborough Vein Study showed there was a significant trend between grade of
telangiectasia and reflux in the GSV, they demonstrated either GSV or SSV reflux in 46% of patients with CEAP 1 telangiectasia
Patients who have failed spider vein treatment should also be evaluated for an underlying source of venous reflux
Recommendations & Tips: ultrasound examination is carried out with the patient standing in an upright position,
It is further recommended that the patient stand for several minutes prior to a duplex examination
Transverse rather than longitudinal scans, and continuous scanning are performed in order to provide a clear mapping of the venous system.
Evidence-Based Summary of Guidelines from the American Venous Forum and the Society for vascular surgery
Management of C1-C3 Chronic Venous Disease:
1. We suggest the use of venoactive drugs such as horse chestnut seed extract for amelioration of the symptoms of pain and swelling.
2. We suggest the use of 20–30 mm Hg compression stockings for patients with symptomatic varicose veins who are not candidates for superficial venous intervention.
3. We recommend stripping or ablation of the saphenous vein in preference to compression stockings in patients who are suitable candidates.
4. We recommend endothermal venous ablation in preference to high ligation and stripping or foam sclerotherapy for the management of saphenous vein incompetence.
5. We recommend sclerotherapy for the treatment of reticular veins, telangiectasias, and recurrent varicose veins.
6. We recommend phlebectomy over sclerotherapy for the treatment of tributary varicosities once axial reflux has been addressed.
7. We recommend against the treatment of incompetent perforating veins in patients with C2 CVD.
Surgical Management of 1rry Varicose Vein Current practice is to perform GSV stripping below knee rather than GSV
high ligation. Duplex scanning showed a much lower incidence of residual reflux in the remaining GSV when the proximal vein had been stripped to the knee than when it had not been stripped.
Jones et al demonstrated After 2 years, 43% of those who had not had GSV stripping demonstrated recurrent varicose veins as opposed to 25% who had.
The Winterborn study postulated recurrence rate of 62% over 5 years in 113 limb with follow up by duplex scanning and clinical examination
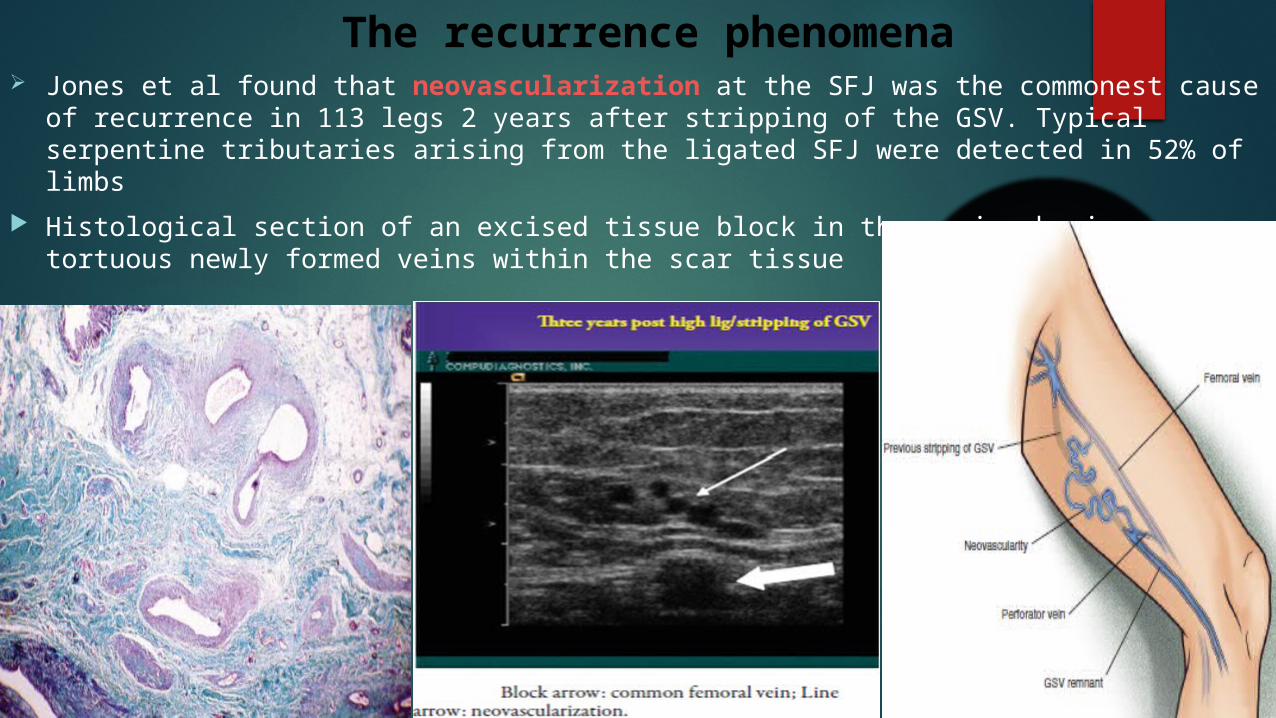
The recurrence phenomena Jones et al found that neovascularization at the SFJ was the commonest cause of
recurrence in 113 legs 2 years after stripping of the GSV. Typical serpentine tributaries arising from the ligated SFJ were detected in 52% of limbs
Histological section of an excised tissue block in the groin showing tortuous newly formed veins within the scar tissue
The recurrence phenomena Postulated theories:
1. Angiogenic stimulation in the free endothelial stump of the GSV
2. Trans-nodal lymphovenous connection
3. Disturbed venous drainage of ligated tributaries
4. Dilatation of small adventitial vessels in the vasa vasorum
5. Other risk factors: female gender, left -sided disease, associated deep vein incompetence, severe chronic venous disease (C4–C6 of the CEAP classification), obesity, and subsequent pregnancies after surgery
sources of reflux associated with recurrence of varicose veins after surgical ligation and stripping:
1. recurrence of reflux at the SFJ or SPJ because of neovascularization or inadequate ligation
2. incompetent thigh or calf perforating veins
3. incompetent gastrocnemius veins
4. persistent varicose tributaries or duplication of the GSV in the thigh, with these medial thigh veins receiving reflux from pelvic tributaries.
The recurrence phenomena
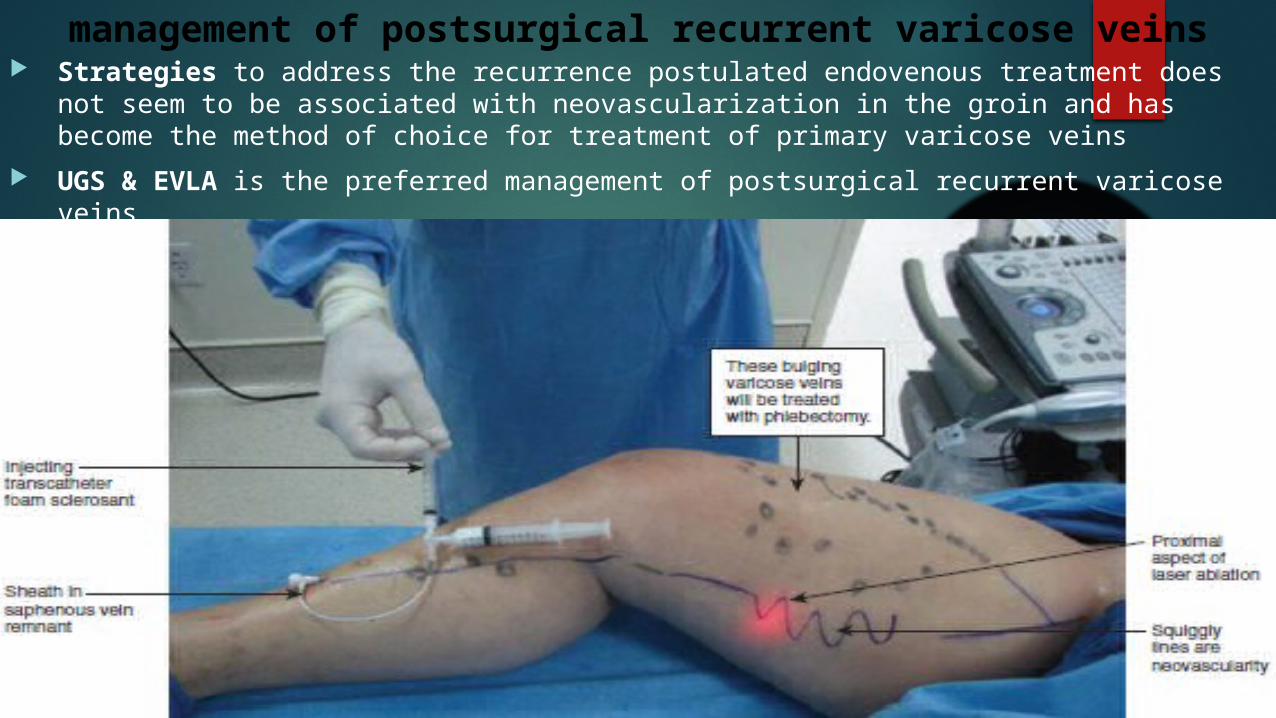
management of postsurgical recurrent varicose veins Strategies to address the recurrence postulated endovenous treatment does not seem
to be associated with neovascularization in the groin and has become the method of choice for treatment of primary varicose veins
UGS & EVLA is the preferred management of postsurgical recurrent varicose veins
Surgical Ambulatory Phlebectomy Minor operation done to remove varicose vein clusters located close to the
skin surface performed with the use of local tumescent anesthesia ccc by absence of venous ligature or skin sutures as it’s done by 2mm stab incisions and hooking of venous clusters
Tumescent anesthesia involves infiltration of the subdermal compartment with generous volumes of a 0.1% solution of lidocaine with epinephrine. 50-cc vial of 1% lidocaine with added 1:100,000 mg of epinephrine mixed with 500 cc of Ringer’s lactate.
The anesthetic preparation is administered subdermally under pressure. The doctor pushes the fluid until a characteristic peau-d’orange effect is visualized on the skin. The tumescent fluid hydrodissects the subcutaneous fat from the venous tissue as it enters, thus facilitating vein extraction afterward
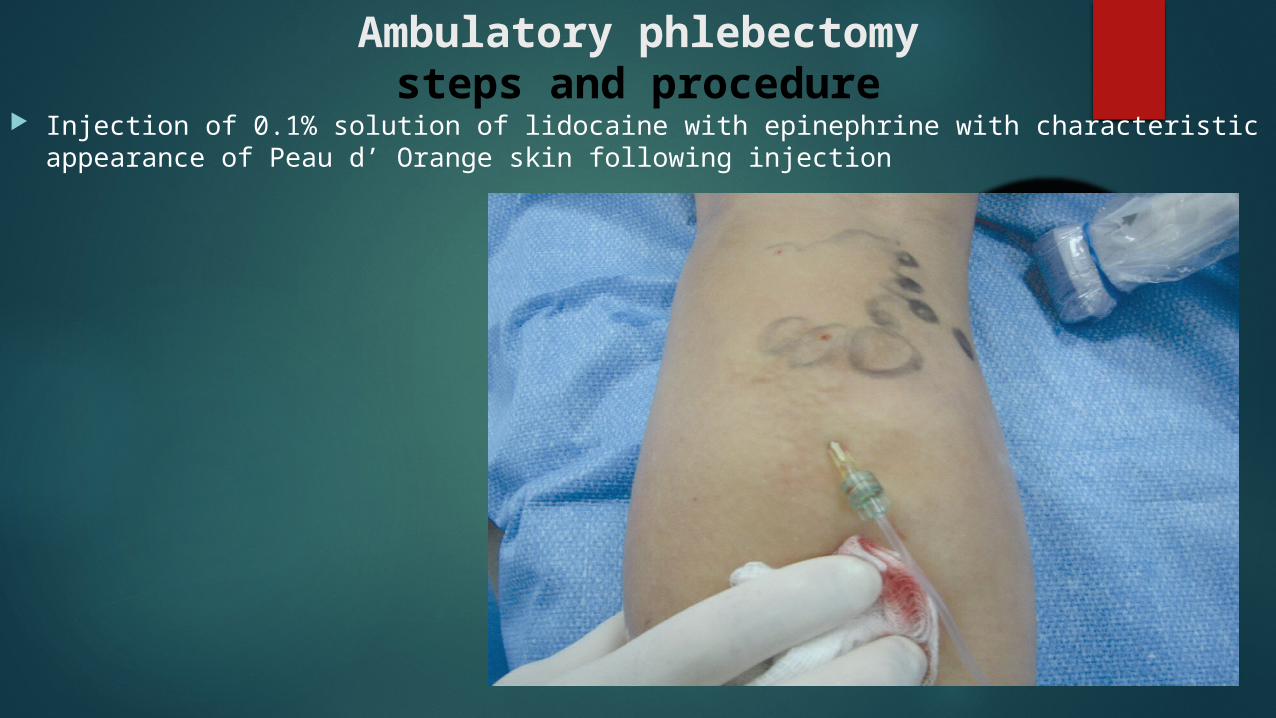
Injection of 0.1% solution of lidocaine with epinephrine with characteristic appearance of Peau d’ Orange skin following injection
Ambulatory phlebectomysteps and procedure
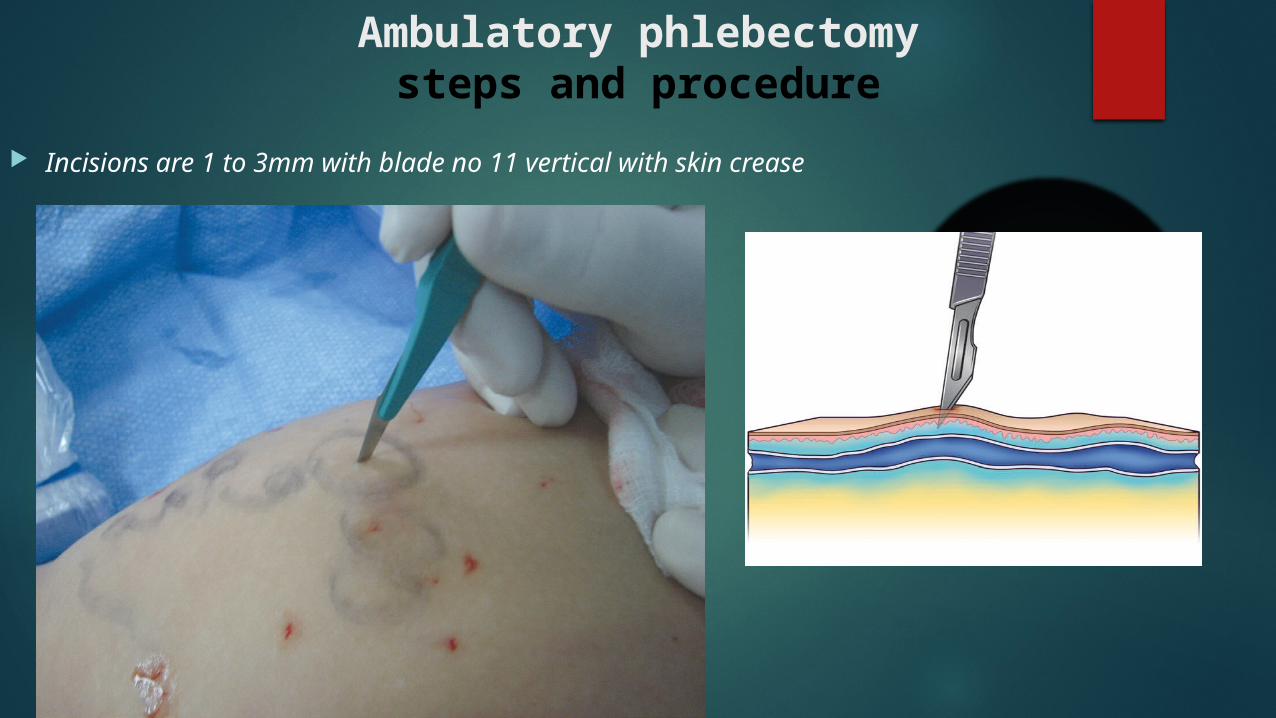
Incisions are 1 to 3mm with blade no 11 vertical with skin crease
Ambulatory phlebectomysteps and procedure

Vein hooking is done with hook and a hemostat where vein is exteriorized and hooked then gentle circular motion by hemostat to exteriorize a long segment of the vein
Ambulatory phlebectomysteps and procedure
Ambulatory phlebectomysteps and procedure
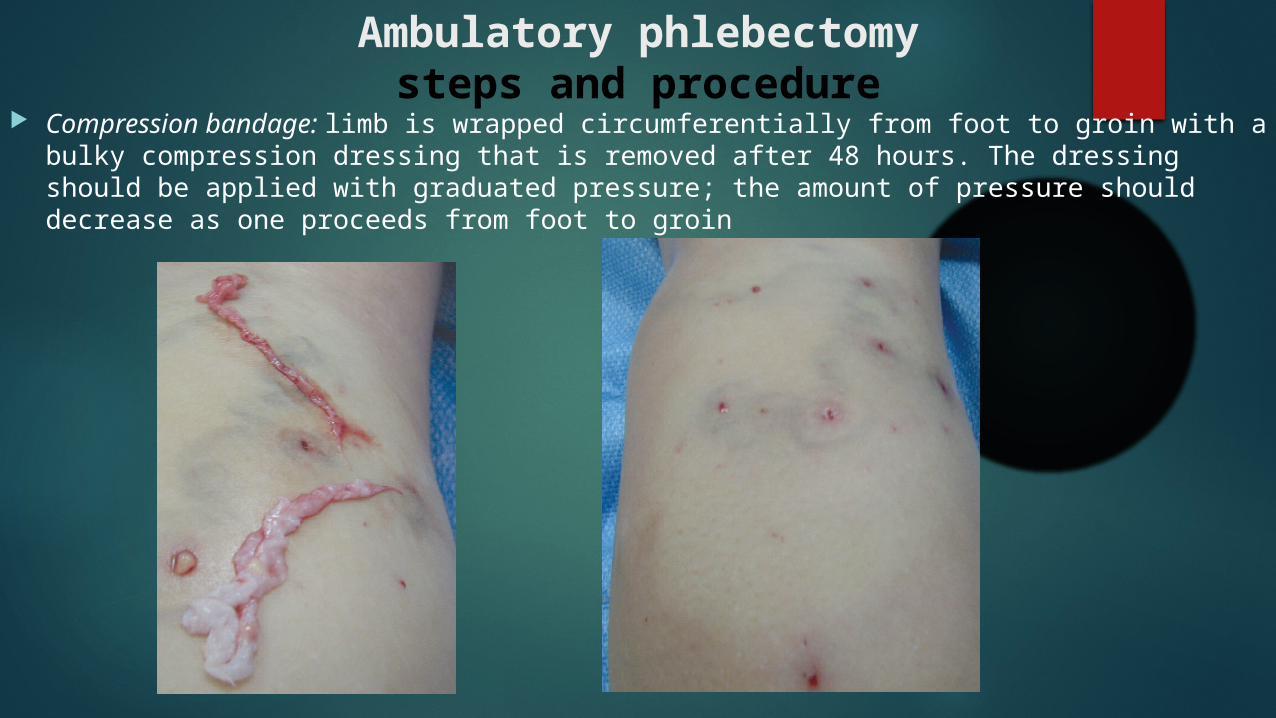
Compression bandage: limb is wrapped circumferentially from foot to groin with a bulky compression dressing that is removed after 48 hours. The dressing should be applied with graduated pressure; the amount of pressure should decrease as one proceeds from foot to groin
Ambulatory phlebectomypostoperative complications
Most frequently encountered complications were:
telangiectasia (1.5%)
blister formation (1%)
phlebitis (0.05%)
hyperpigmentation (0.03%)
postoperative bleeding (0.03%)
temporary nerve damage (0.05%)
ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS)
Patient selection:
1. the treatment of choice in spider telangiectasias and isolated reticular veins.
2. nonsaphenous varicose veins, residual veins after surgical correction of axial vein reflux.
3. recurrent varicose veins secondary to neovascularization .
4. incompetent perforating veins.
5. Foam UGS has been reported to be an effective method for accelerating healing of venous ulcers associated with superficial venous incompetence
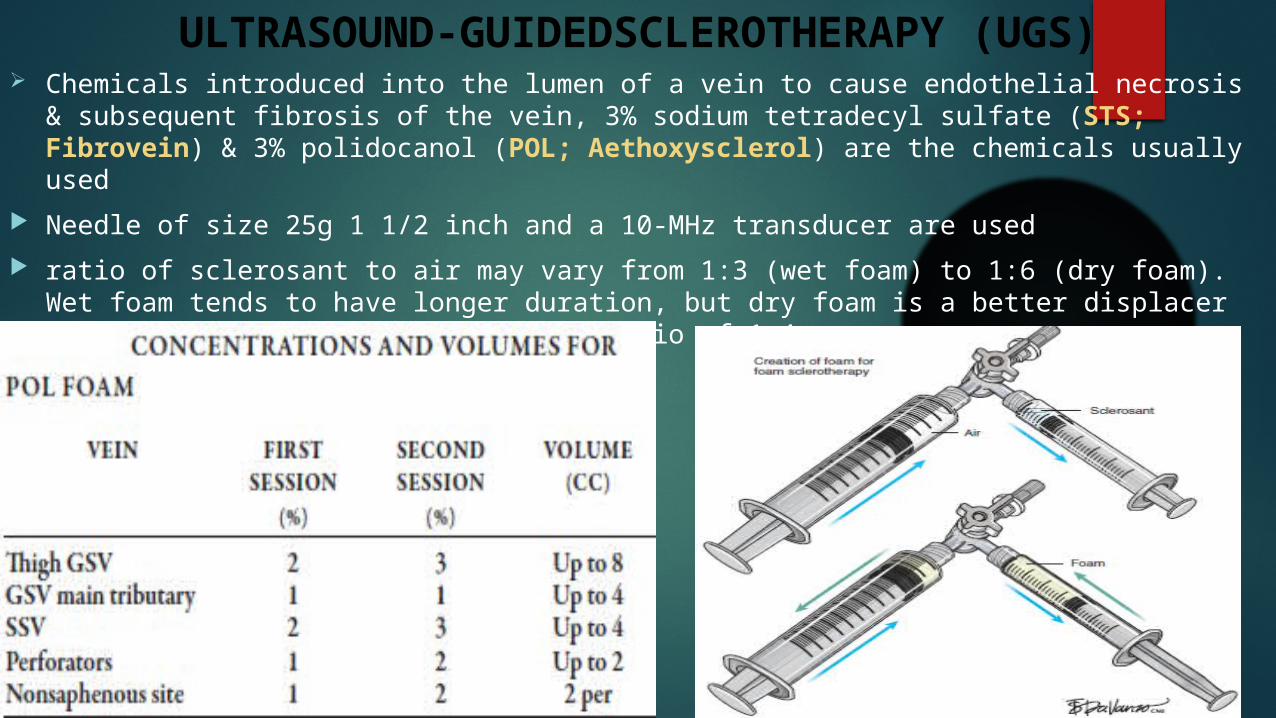
ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS) Chemicals introduced into the lumen of a vein to cause endothelial necrosis & subsequent
fibrosis of the vein, 3% sodium tetradecyl sulfate (STS; Fibrovein) & 3% polidocanol (POL; Aethoxysclerol) are the chemicals usually used
Needle of size 25g 1 1/2 inch and a 10-MHz transducer are used
ratio of sclerosant to air may vary from 1:3 (wet foam) to 1:6 (dry foam). Wet foam tends to have longer duration, but dry foam is a better displacer of blood yet most recommend is the ratio of 1:4.
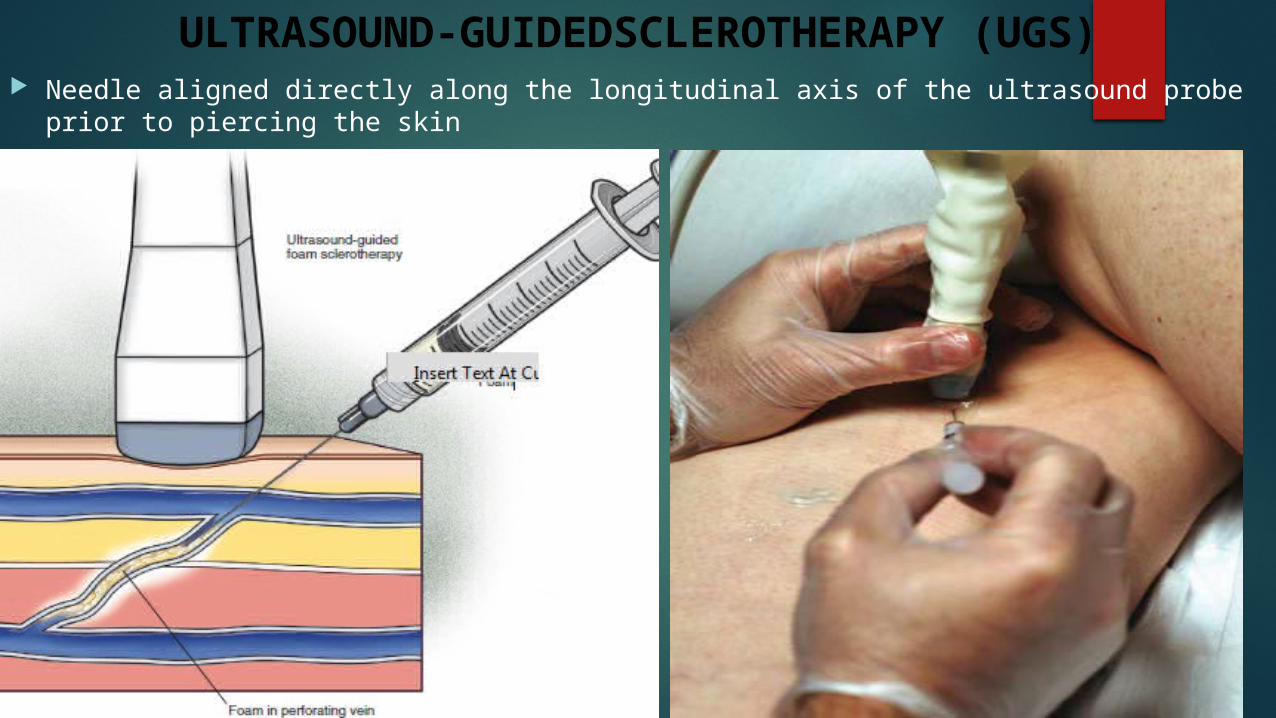
ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS) Needle aligned directly along the longitudinal axis of the ultrasound probe prior to piercing
the skin
ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS)
ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS)
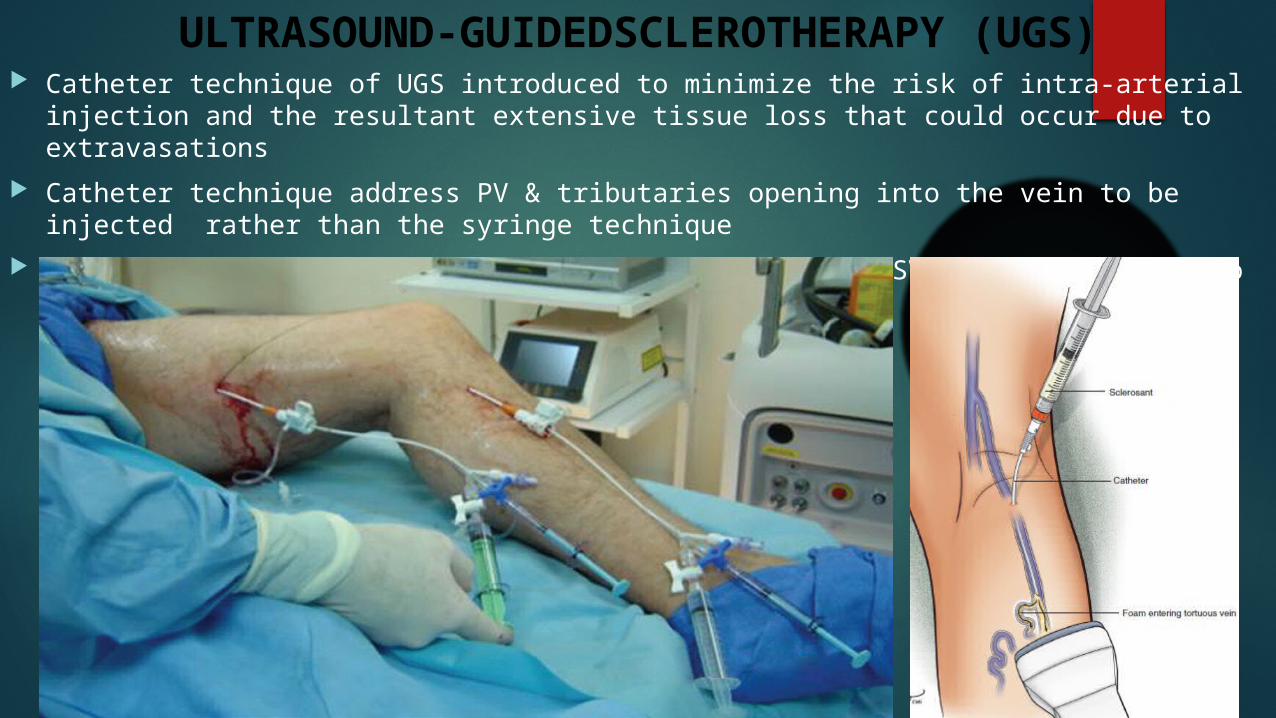
ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS) Catheter technique of UGS introduced to minimize the risk of intra-arterial injection and
the resultant extensive tissue loss that could occur due to extravasations
Catheter technique address PV & tributaries opening into the vein to be injected rather than the syringe technique
20-gauge 44-mm cannula for cannulation of he GSV or SSV 6 to 8 cm distal to the SFJ and SPJ

ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS) Efficacy of procedure verified by U/S including vasospasm, no compressibility along the
entire length of the treated vein, and absence of any blood flow in the vein
External Compression: most commonly used compression following treatment is the application of Class II (25- to 35 mmHg) graduated compression stockings. stockings are worn during the day for 2 to 3 weeks. The stocking may be removed each day for showering, without any undue adverse effects.
Internal Compression:
about 5 to 10 ml of normal saline is injected
via a 25g 1 1/2 inch needle at each
cross-sectional segment of the vein guided by U/S
Technique used routinely for vein greater than 3mm
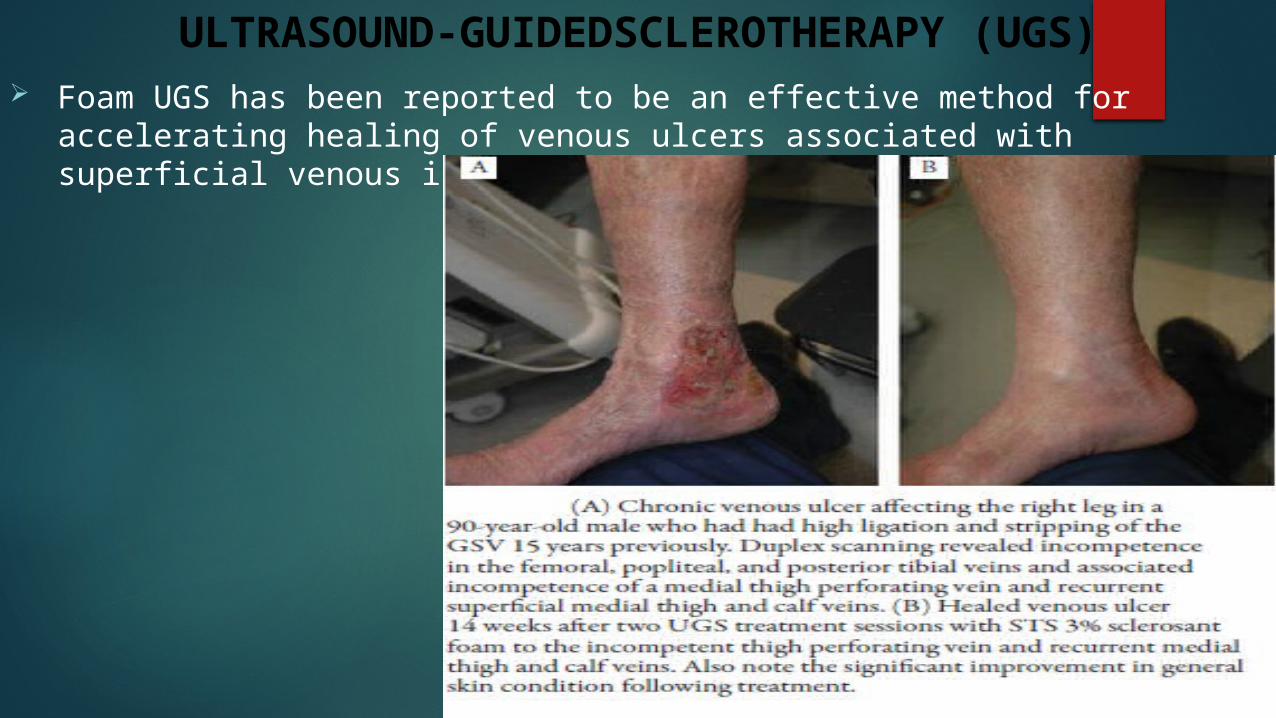
ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS) Foam UGS has been reported to be an effective method for accelerating
healing of venous ulcers associated with superficial venous incompetence
ULTRASOUND-GUIDEDSCLEROTHERAPY (UGS) Minor Complications:
phlebitis, pigmentation, edema, pain & Visual disturbances Major Complications:
1. DVT, pulmonary embolus, and severe allergic reaction. the incidence of major adverse effects were all less than 0.1%.
2. The most common serious adverse effect is anaphylactoid reactions to the sclerosant STS, The incidence of anaphylactoid reaction in 2,686 treatment sessions was 0.15%. This reaction appears to be concentration- and volume-dependent
Contraindications:Tamoxifen (DCI) has demonstrated a potential to induce superficial venous thrombosis during sclerotherapy; therefore, injections must be postponed to the end of chemotherapy.
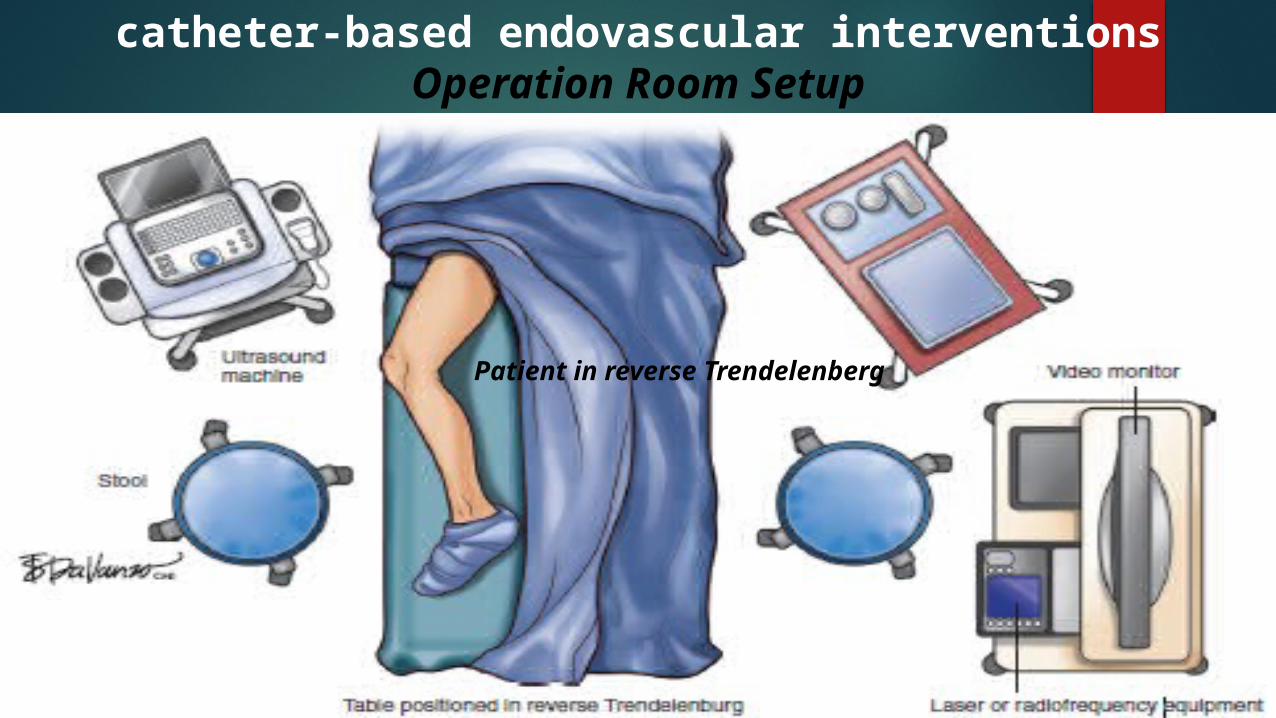
catheter-based endovascular interventionsOperation Room Setup
Patient in reverse Trendelenberg
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
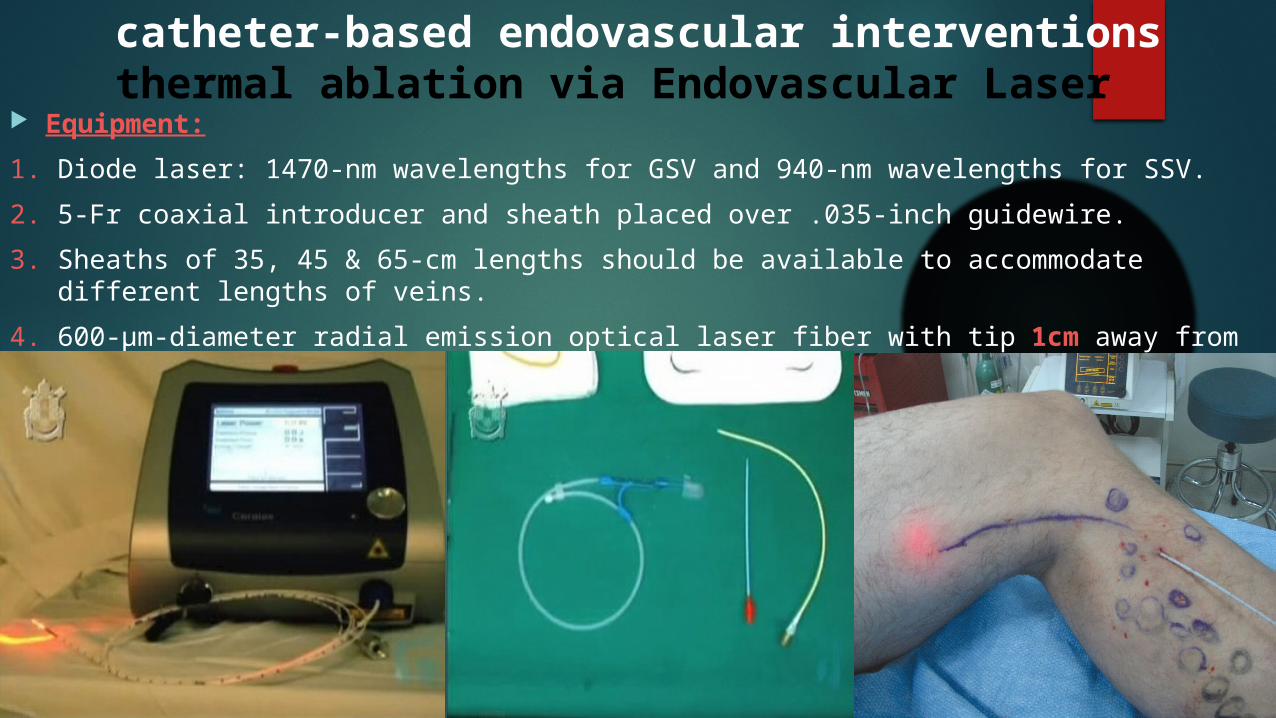
Equipment:
1. Diode laser: 1470-nm wavelengths for GSV and 940-nm wavelengths for SSV.
2. 5-Fr coaxial introducer and sheath placed over .035-inch guidewire.
3. Sheaths of 35, 45 & 65-cm lengths should be available to accommodate different lengths of veins.
4. 600-μm-diameter radial emission optical laser fiber with tip 1cm away from CFV
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
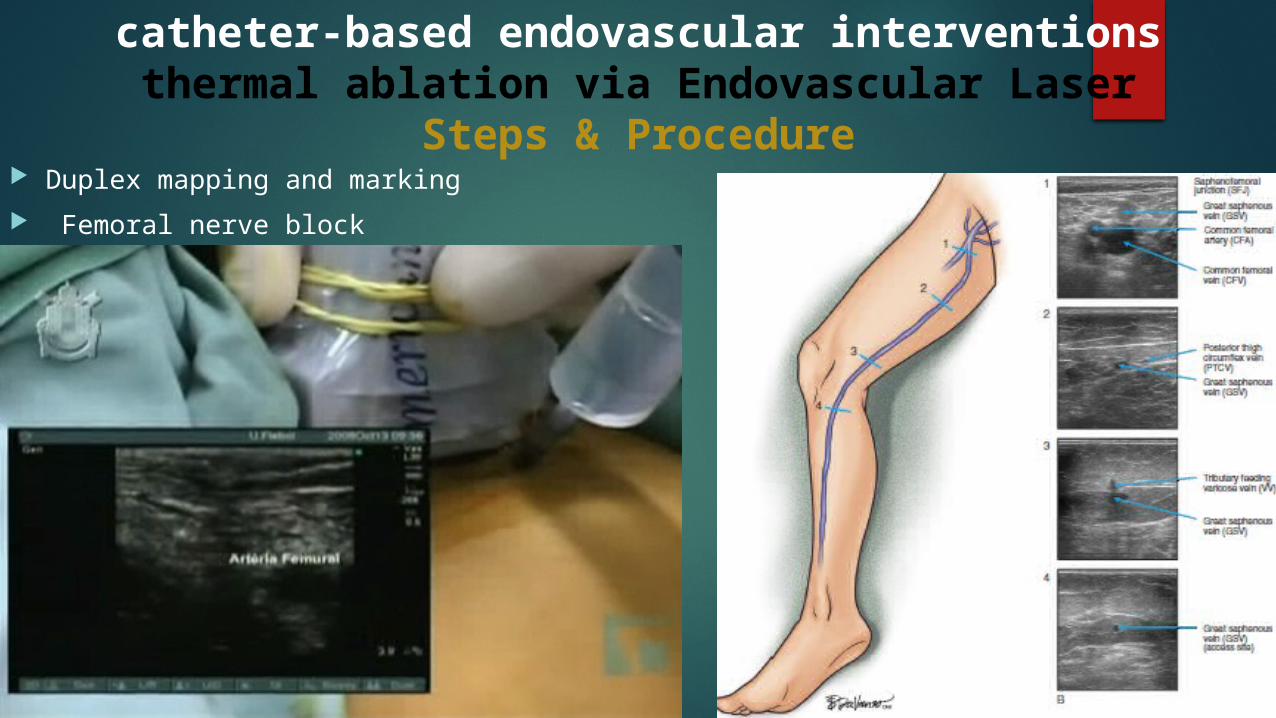
Steps & Procedure Duplex mapping and marking
Femoral nerve block
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
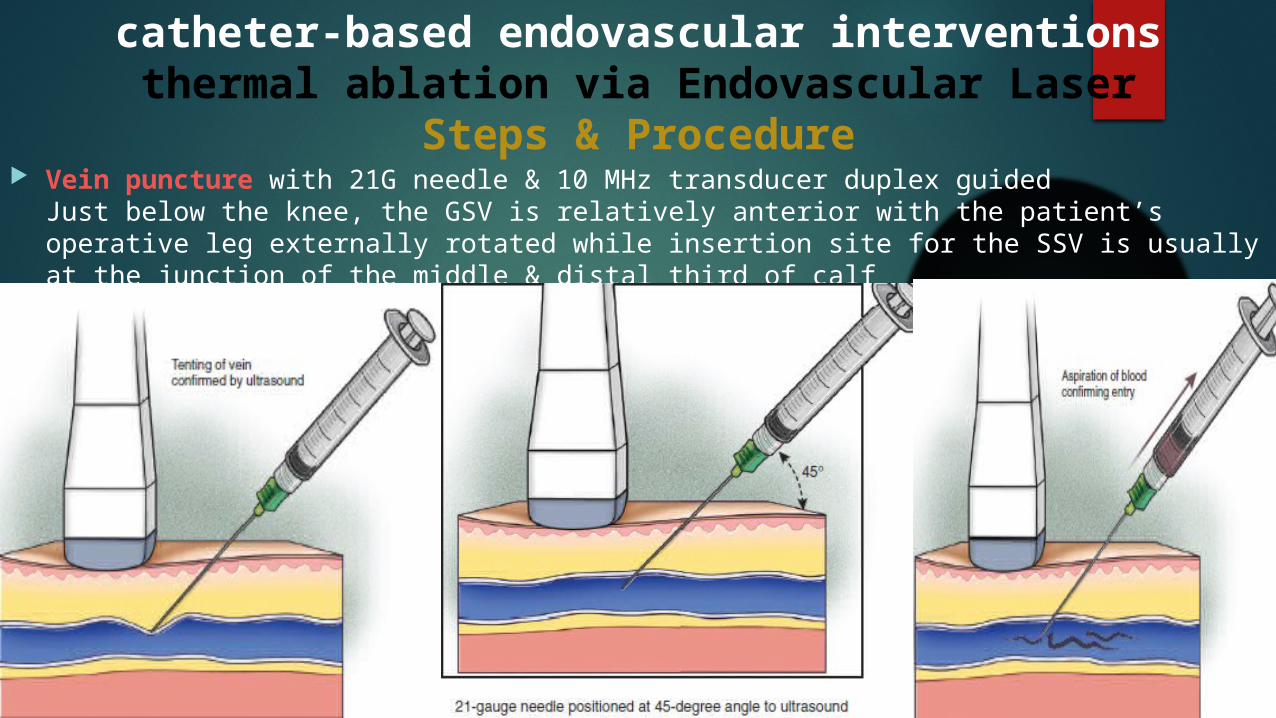
Steps & Procedure Vein puncture with 21G needle & 10 MHz transducer duplex guided
Just below the knee, the GSV is relatively anterior with the patient’s operative leg externally rotated while insertion site for the SSV is usually at the junction of the middle & distal third of calf
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
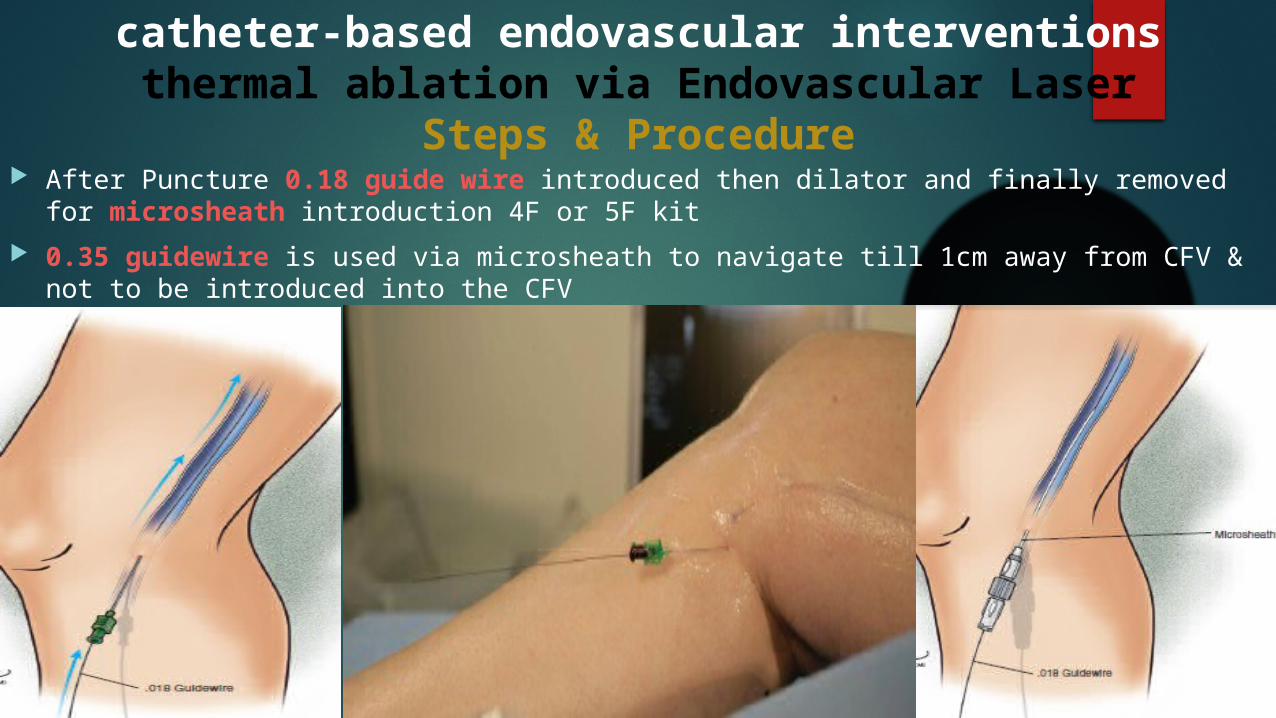
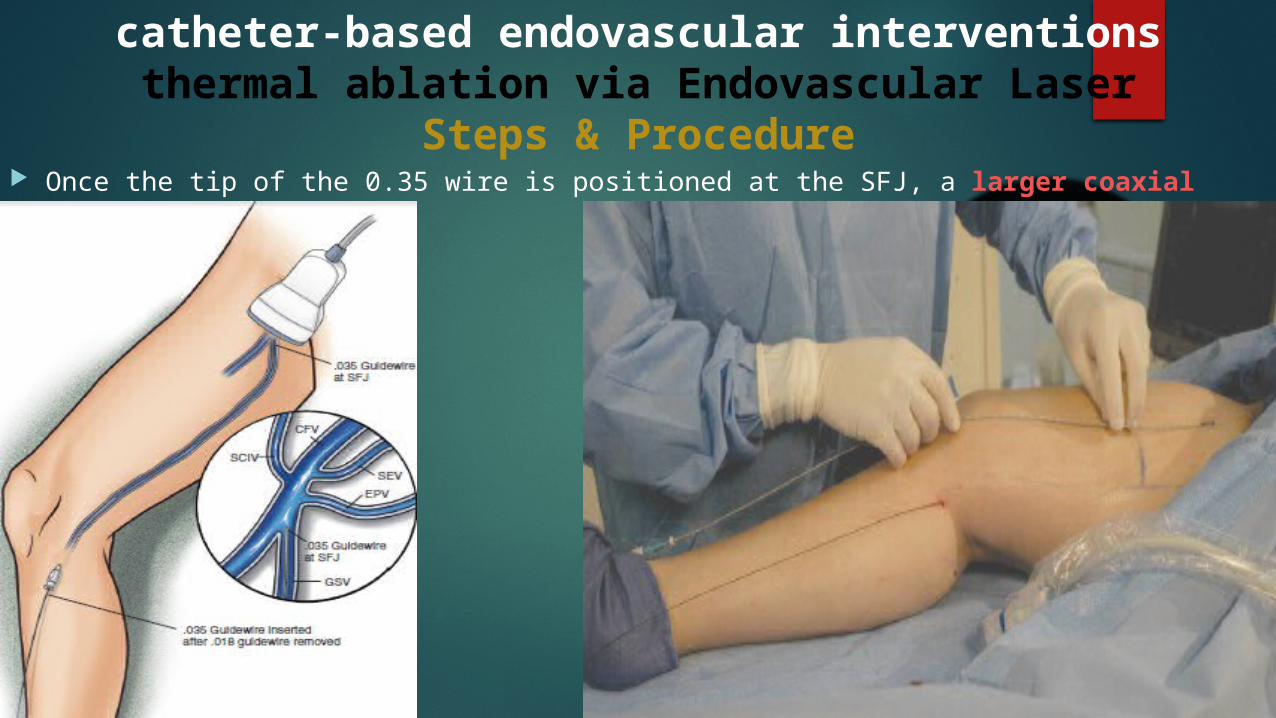
Steps & Procedure After Puncture 0.18 guide wire introduced then dilator and finally removed for
microsheath introduction 4F or 5F kit
0.35 guidewire is used via microsheath to navigate till 1cm away from CFV & not to be introduced into the CFV
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
Steps & Procedure Once the tip of the 0.35 wire is positioned at the SFJ, a larger coaxial sheath is placed
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
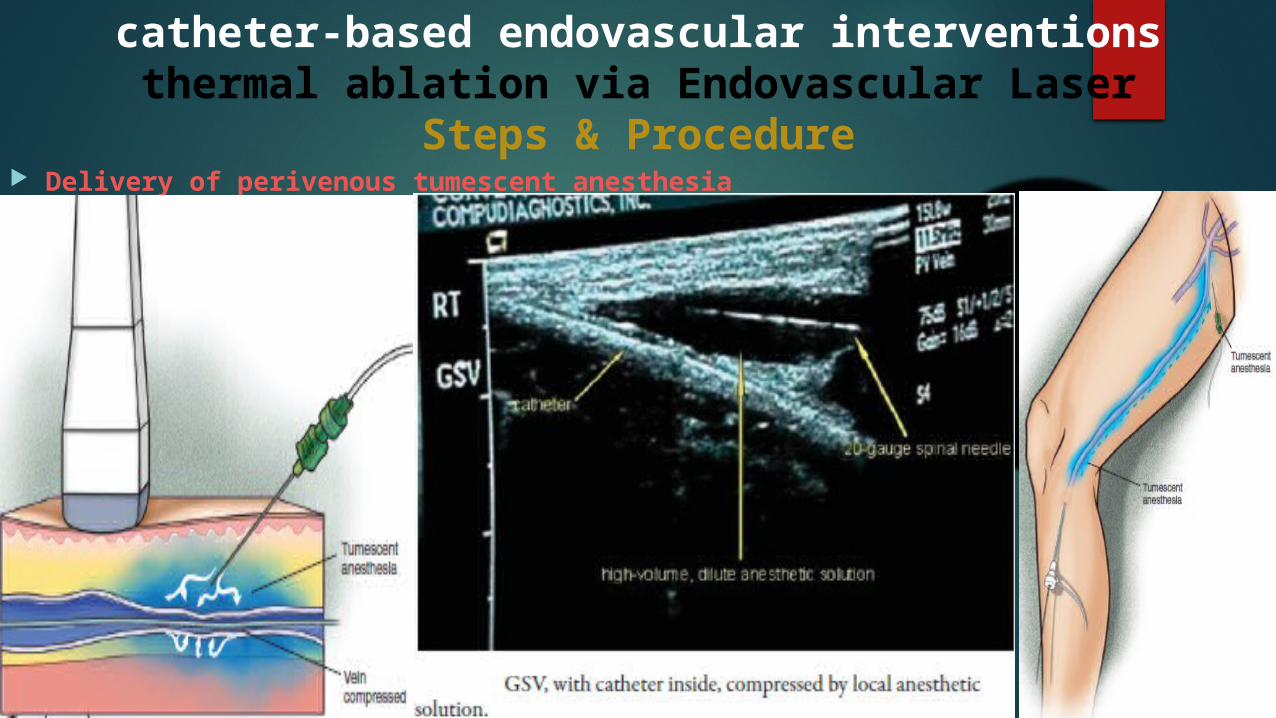
Steps & Procedure Delivery of perivenous tumescent anesthesia
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
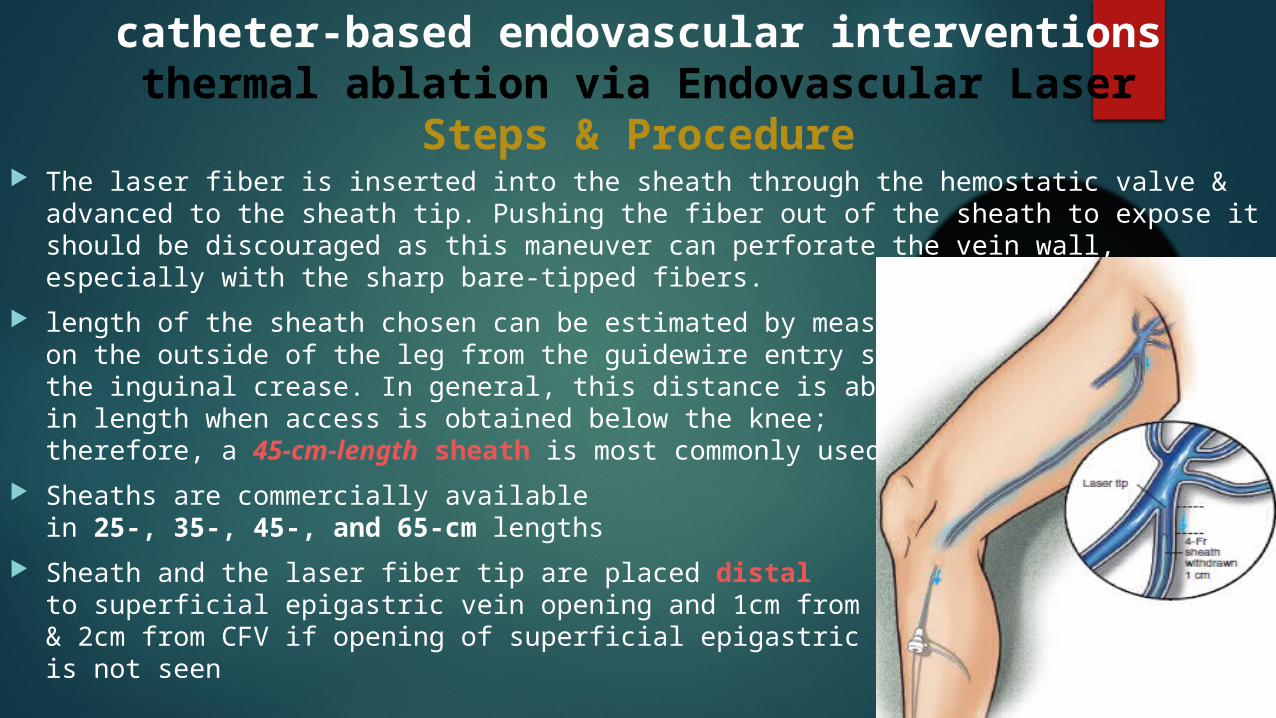
Steps & Procedure The laser fiber is inserted into the sheath through the hemostatic valve & advanced to the
sheath tip. Pushing the fiber out of the sheath to expose it should be discouraged as this maneuver can perforate the vein wall, especially with the sharp bare-tipped fibers.
length of the sheath chosen can be estimated by measuring on the outside of the leg from the guidewire entry site to the inguinal crease. In general, this distance is about 40 cmin length when access is obtained below the knee; therefore, a 45-cm-length sheath is most commonly used
Sheaths are commercially available in 25-, 35-, 45-, and 65-cm lengths
Sheath and the laser fiber tip are placed distal to superficial epigastric vein opening and 1cm from CFV& 2cm from CFV if opening of superficial epigastric vein is not seen
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
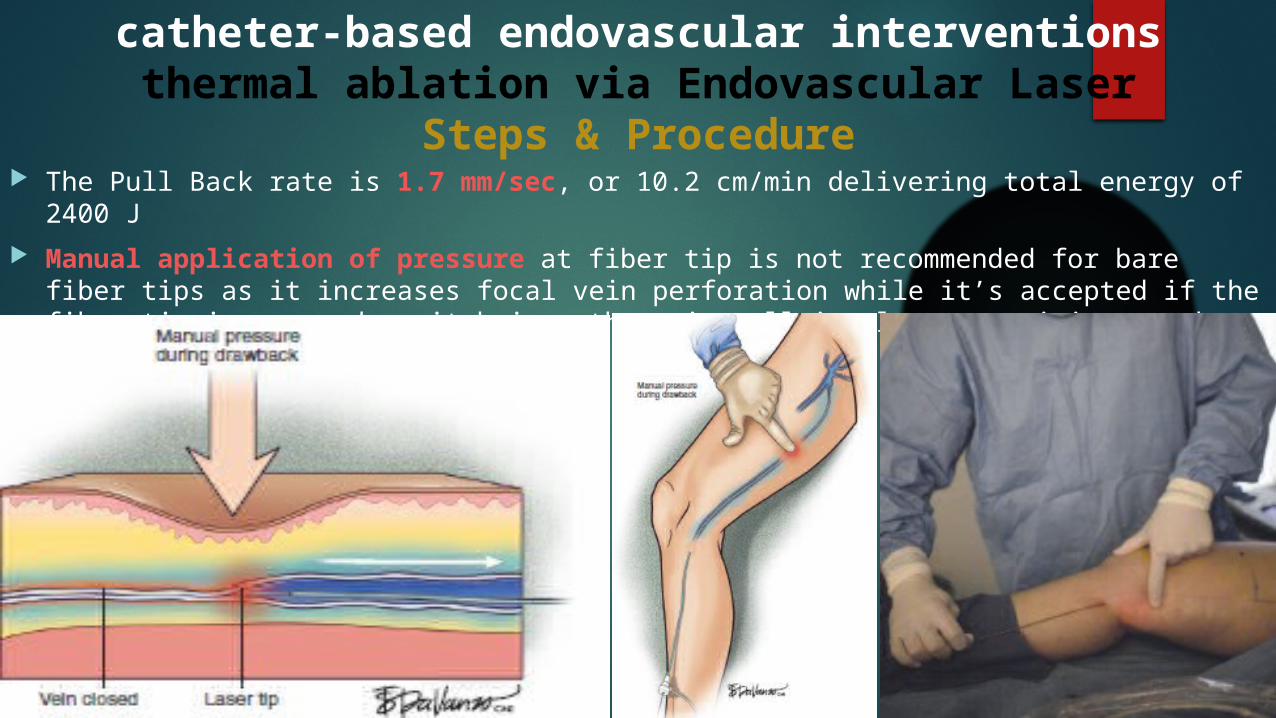
Steps & Procedure The Pull Back rate is 1.7 mm/sec, or 10.2 cm/min delivering total energy of 2400 J
Manual application of pressure at fiber tip is not recommended for bare fiber tips as it increases focal vein perforation while it’s accepted if the fiber tip is covered as it brings the vein wall in closer proximity to the energy source.
catheter-based endovascular interventionsthermal ablation via Endovascular Laser
Steps & Procedure Compression bandage:
amount of pressure should decrease as one proceeds from foot to groin padding of lateral fibular head is a must to avoid injury of peroneal nervesthree-layer bandage for 48 hours post procedure
catheter-based endovascular interventionsthermal ablation via Direct Radiofrequency
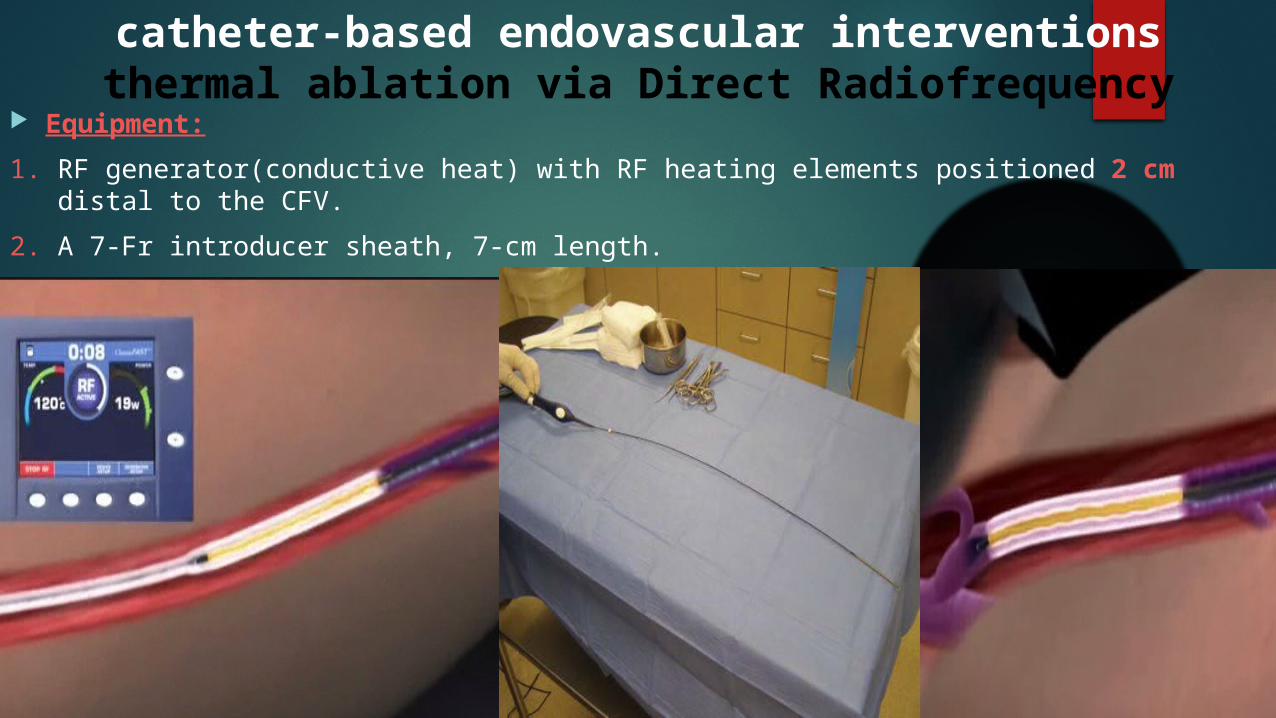
Equipment:
1. RF generator(conductive heat) with RF heating elements positioned 2 cm distal to the CFV.
2. A 7-Fr introducer sheath, 7-cm length.
3. A .025-inch guidewire.
catheter-based endovascular interventions thermal ablation via Direct Radiofrequency
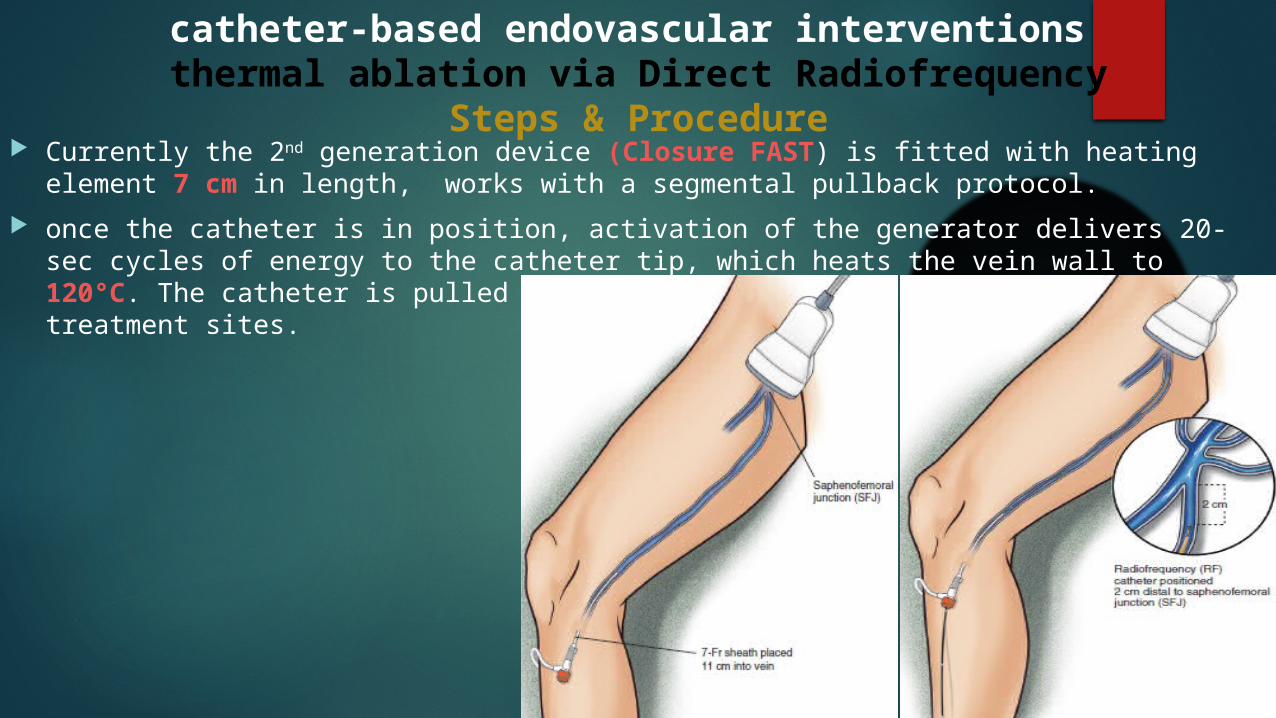
Steps & Procedure Currently the 2nd generation device (Closure FAST) is fitted with heating element 7 cm in
length, works with a segmental pullback protocol.
once the catheter is in position, activation of the generator delivers 20-sec cycles of energy to the catheter tip, which heats the vein wall to 120°C. The catheter is pulled back in segments of 6.5 cm to overlap the treatment sites.
catheter-based endovascular interventions thermal ablation via Direct Radiofrequency
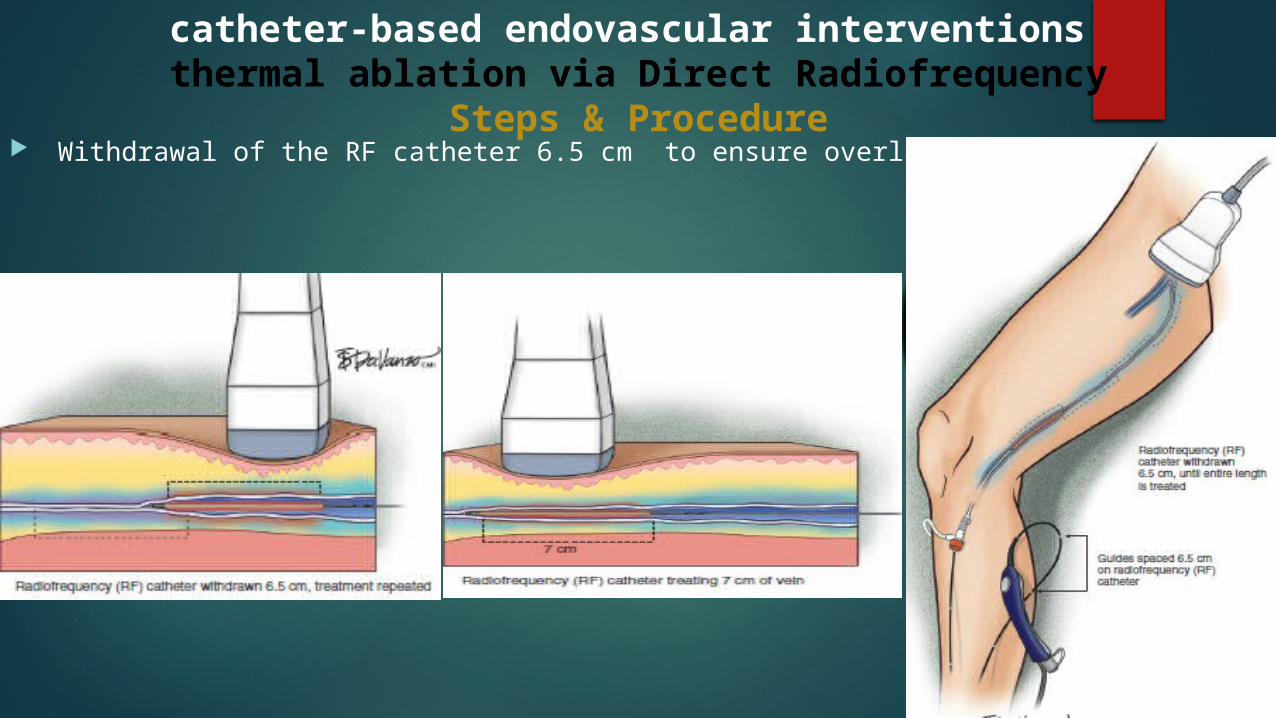
Steps & Procedure Withdrawal of the RF catheter 6.5 cm to ensure overlapping
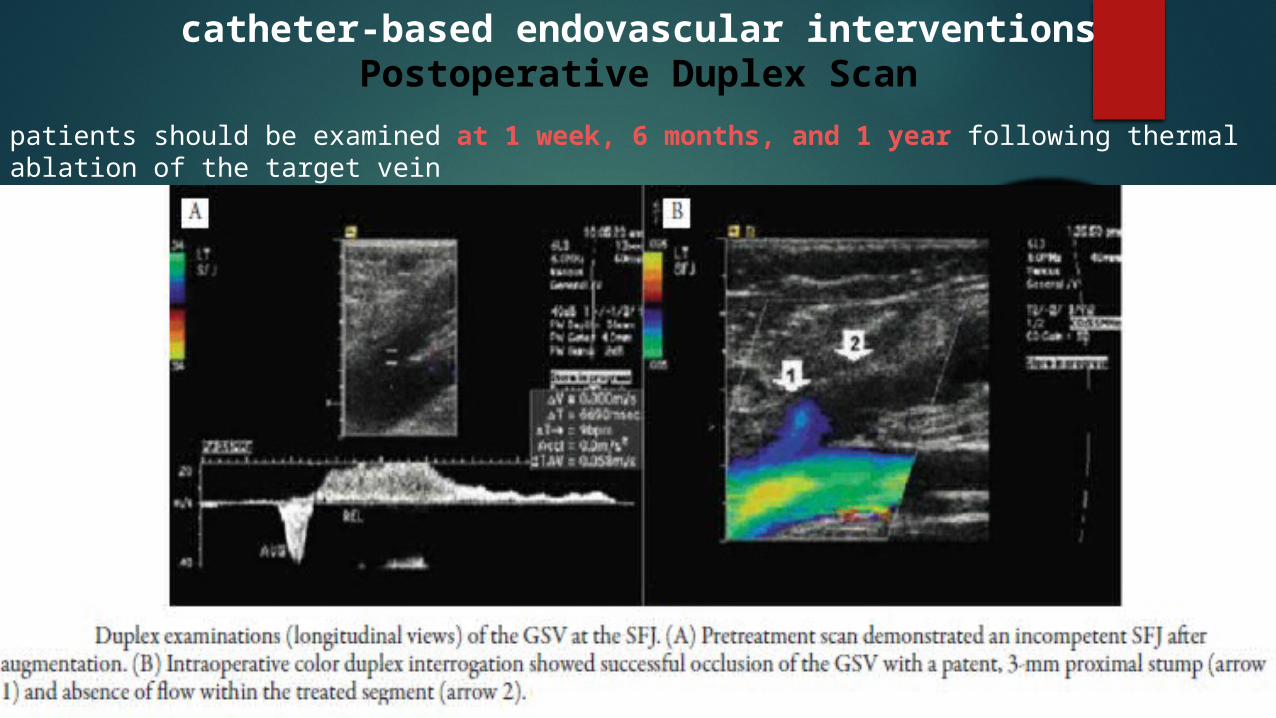
catheter-based endovascular interventionsPostoperative Duplex Scan
patients should be examined at 1 week, 6 months, and 1 year following thermal ablation of the target vein
catheter-based endovascular interventionsThermal Ablation
POSTOPERATIVE ADVERSE EFFECTS:
1. Bruising minimal & of less than 2 weeks duration
2. Paresthesia transient and distal surgeon related
3. Skin burn & Infection less than 0.1%
4. Superficial thrombophlebitis less than 5%
5. Deep vein thrombosis less than 1% mostly calf vein thrombosis
Pitfalls:
1. Distal portions of the GSV or SSV vein may be treated with endovenous thermal ablation yet they require efficacy in the delivery of ultrasound-guided local anesthetic as there is increased risk of paresthesia from damage to the saphenous or sural nerve
2. SSV will deepen its course as it approaches its union with the popliteal vein. It will appear as a 45-degree bend of 2 cm in length. It’s mandatory to leave this 2-cm-length angled segment untreated to avoid C.P.N or P.T.N damage with resultant foot drop