Embed Size (px)
Citation preview

VARICOSE VEINS
VIDULA SHEVADE
GROUP 603

VARICOSE VEINS
Definition:
Varicose veins are veins that have become distended over time. Long, tortuous and dilated veins of the superficial varicose system due to the pooling of blood in the lower extremities.

LEG VEIN ANATOMY Legs are made of network of
veins that carry blood to heart. The venous system is comprised
of – 1 Superficial veins long saphenous vein short saphenous vein

LEG VEIN ANATOMY2 Deep veins femoral vein Popliteal vein Peroneal vein Anterior tibial vein Posterior tibial vein3 perforating veins 90% of blood is returned by deep
veins and not by superficial veins.

PERFORATING VEINS Direct perforating veins :
These directly connect superficial veins with deep veins

PERFORATING VEINS In thigh : Adductor canal perforator
connects long saphenous with femoral vein in lower part of adductor canal. (hunterian’s perforator)
In the lower thigh on medial aspect Long SV connect femoral vein via DODD’s Perforator
Below knee : Perforator connects long SV or
post-Arch vein with posterior tibial vein knows as BOYD’S Perforator.

PERFORATING VEINS In leg : 1.Lateral perforator is presented at the junction of mid & lower third of leg .It connect SSV with peroneal vein. 2. Medially there are three perforator
which connect posterior arch vein with posterior tibial vein , know as COCKETT’S Perforator

PERFORATING VEINS Upper medial perforator lies
at the junction of middle and lower third of leg.
Middle medial perforator lies 4Inch above the medial malleolus .
Lower medial perforator lies posterio-inferior to the medial malleolus .


PERFORATING VEINS Indirect perforating veins: These consist of small
superficial veins which penetrate the deep fascia to connect with vessel in muscle and in turn end in Deep vein.

LEG VEIN ANATOMY Blood is drained from superficial
to deep veins of legs through perforating veins .
And through deep veins it is carried to heart.
Back flow of blood is impossible. But due to defect in valve of
blood flows in opposite direction .

LEG VEIN ANATOMY

VENOUS VALVES The venous valves are abundant in the
distal lower extremity and number of valves decreases proximally, with no valves in superior and inferior vena cava
Delicate structures Prevent reverse flow in the veins Ensure that the blood is pumped from
the superficial to the deep system and back towards the heart when the patient is walking

ETIOLOGY PRIMARY VARICOSE VEINS Defect in saphanofemoral valve Defect in saphanopoplitial valve Defect in valve of perforators

SECONDARY
Anything that increases intra-abdominal pressure
Or raises pressure in superfical or deep veins
Pregnancy Obesity Abdominal or pelvic mass Old age Long standing Thrombosis of leg veins

CONGENITAL CAUSES Arteriovenous fistulas

CLINICAL FEATURES Heaviness in the legs Night time cramps Dragging pain, postural discomfort Oedema, itching Discolouration Ulceration


CAUSES OF PAIN Anoxia Hyperviscosity or red cells Chronic venous hypertension Platelet aggregation Capillary functional disorder Altered cuteneous microcirculation

COMPLICATION Hemorrhage Pigmentation/ eczema Periostitis Venous ulcer Lipodermatosclerosis DVT Tromboplebitis

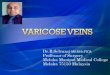
ECZEMA

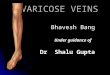
VENOUS ULCER

STAGES C0 no visible or palpable signs of venous
disease C1 telangectacia or reticular veins C2 varicose veins (without symptoms) C3 edema C4a skin changes due to venous disorders:
pigmentation, eczema C4b skin changes due to venous
disorders: lipodermatosclerosis C5 as C4 but with healed ulcers C6 skin changes with active ulcers (venous
insufficiency ulceration)

INVESTIGATION Venography Venous doppler Trendelenburg test Tourniquet test Cough impulse test Perthe test

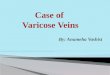
TRENDELENBURG TEST

TOURNIQUET TEST 3 tourniquets are tied. 1st at thigh 2nd at below knee 3rd above knee Now patient is asked to stand and
appearance of varicosity is looked for,within 30 sec in each segment
If the veins above the tourniquet fill up ,it indicates incompetence of communicating veins above tourniquet.

TOURNIQUET TEST If veins below tourniquet fill up
rapidly ,it indicates communicating veins below tourniquet are incompetent.

COUGH IMPULSE TEST Patient is asked to elevate the
limb . Then patient is asked to cough
forcibly. The impulse is felt on long
saphenous vein. This indicates the incompetent
of sapheno-femoral valve.

PERTHE TEST A tourniquet is tied around the
upper thigh. Then patient is asked to walk. If veins get dilated ,it indicates
the presence of incompetence.

CONSERVATIVE MANAGEMENT Elastic crepe bandage – stockings
Elevation of limbs
Graded compression
Excercise
Avoidance of prolonged standing

CONSERVATIVE MANAGEMENT Compression methods
Reduce ambulatory venous pressure
Improve cutaneous micro circulation

SCLEROTHERAPY Injection of sclerosant (ethanolamine
oleate) into an varicose vein causes sclerosis.
Leading to complete obliteration of vein.

SURGICAL MANAGEMENTINDICATION LSV /SSV incompetency . Perforating vein incompetency.
CONTRAINDICATION DVT Pregnancy Thrombophlebitis Peripheral vascular disease

STEPS OF SURGERY After anesthesia proper position
is given. The whole table is tilted head
down to an angle of about 10 degree. (trendelenberg position)

STEPS OF SURGERY Incisions :1. Hockey stick incision2. Oblique incision Incision is kept at groin at Saphenous opening 3-4 cm below and lateral to pubic tubercle.

STEPS OF SURGERY

STEPS OF SURGERY Then stripper is passed down the
saphenous vein and directed downward by finger .
Vein is tied with stripper and then stripper is slowly and steadily pulled out through lower wound

STEPS OF SURGERY

NEW SURGICAL TECHNIQUES Vein valve tranplantation