Embed Size (px)
DESCRIPTION
varicose vein treatment ,diagnosis
Citation preview



EpifascialSubcutaneous veins
IntrafascialSuperficial veins
SubfascialDeep veins
Three Anatomical Areas:
Three fully interacting systems: superficial, deep, perforators

Venous Disease
Divided into Superficial and Deep System
Deep System•Named for by associated arteries•Found running along the arteries•Predictable anatomy•Causes most of the Morbidity
1. DVT 200,000 cases/year in USA2. PE 50,000 caser/year3. Severe Leg Swelling4. Ulcerations
•Little Surgical interventions (IVC Filter)•Medical Management
• Anticoagulation• Thrombolytic therapy
•Systemic vs. Catheter directed• Elevation and Compression

Venous Disease
Superficial System• Varicose Veins• Spider Veins• Venous Malformation (birth marks and others)• Venous Reflux• Leg Swelling• Venous Ulceration

The collecting system of veins.
The conduits for blood to travel from superficial to the deep veins.
The channel through which blood is pumped out of the legs.
Contraction of leg muscles pumps blood through one-way valves up and out of the legs.

Superficial Venous System

Formed by union of dorsal digital vein of great toe & dorsal venous arch
Ascends ant: to medial malleolus, post: to medial condyle of femur.
Prox: it traverses saphenous opening in fascia to enter femoral vein.
Along its course, a variable number of named perforating veins may connect to deep system i.e. femoral, posterior tibial, gastrocnemius, & soleal veins.
Great Saphenous Vein

Formed by union of dorsal digital vein
of 5th digit & distal venous arch.
Runs post: to lateral malleolus, lateral to calcaneal tendon.
Runs superiorly medial to fibula and penetrates deep fascia of popliteal fossa, ascends b/w heads of gastrocnemius muscle to join popliteal vein.

Deep veins accompany the arteries. Usually paired and run with named arteries inside a vascular
sheath, this allows arterial pulsation to force blood proximally.
Popliteal vein joins femoral vein in popliteal fossa. Femoral vein is joined by deep vein of thigh . Femoral vein passes deep to inguinal ligament to become
external iliac vein.

These veins transverse deep fascia of lower extremity. Valves are located just distal to penetration of deep fascia. A number of named perforators are found at thigh, knee &
leg. Cockett perforators b/w ankle & knee are special group of
perforating veins. Rather than directly connecting sup: to deep venous
systems they connect subfascial deep system with post: arch vein which then empties into GSV.

Perforators
• Connect deep and superficial systems
• Flow normally from superficial to deep
• Common GSV perforators:- Hunterian (midthigh)- Dodd’s (above knee)- Boyd’s (below knee)- Cockett (distal leg)

Named perforators along the greater saphenous distributionNamed perforators along the greater saphenous distribution

Physiology
• Arteries deliver blood to tissue• Veins return blood to the hart• Hart is the arterial pump• What pumps the venous blood back to the heart?
• Venous pressure is about 25mmHg at the foot• Pressure needed 80mmHg to return blood
– Two unique features of veins accomplish this• Most important one-way Venous Valves• Easily compressible by surrounding muscle (calf
pump)

Calf Muscle Pump
Just like the in heart we have diastole and systole
This is why stretching your legs or walking improves circulation

Foot and calf muscles act to squeeze blood out of deep veins.
One way valve allow only upward and inward flow.
During muscle relaxation blood is drawn inward thru perforating veins.

Muscle Pump
• Contractions propel blood toward heart
• Relaxation draws blood from
- superficial veins- lower deep veins

Thoracoabdominal Pump
• Inspiration decreases intrathoracic pressure promoting venous return
• Expiration reverses the process
• Findings easily seen in US

Valves
• Maintain unidirectional flow- Extremity to heart- Superficial to deep
• GSV and SSV with terminal and preterminal valves
• Terminal (sentinel or first) valve with firm thickened white cusps different from the rest of the valves

Valve leaflets allow unidirectional flow upward or inward.
Dilation of vein wall prevents apposition of valve leaflets,resulting in reflux.
Valvular fibrosis,destruction, or agenesis results in reflux.

Normal venous flow in the Leg
Normal Flow • Superficial veins drain into the deep veins•From the foot up to the heart
Superficial vein disease always starts with abnormal valves and interruption to normal flow called venous reflux

Abnormal flow = Venous Reflux
Damaged Valves
1. Blood flows to the skin
2. Blood is pushed distally and proximally
3. Close loop recirculation
4. Blood is retained in the leg• Increased volume of blood (heaviness
Fatigue)
• Increased venous pressure• Veins Dilate (varicose veins)

Pathophysiology> 90% LEVI
A. Normal
Incompetent Valve ProgressionIncompetent Valve Progression
B. Leaky Valve Syndrome -Valves become stretched -Allow back flow of Blood
C. Superficial Valvular Reflux-Vein becomes engorged-Increasing pressure-Thinning walls-Weaken muscle support-Can enlarge vessel diameters greater than 10mm

Symptoms of venous reflux
• Leg Fatigue• Leg Heaviness• Itching and pain along veins• Varicose Veins• Spider veins (not always 2nd to reflux)• Leg swelling( think DVT 1st)
• Skin Discoloration (lipo dermatosclerosis)
• Venous ulceration

Varicose veins
• Dilated tortuous superficial veins - either main trunk (long or short sapehnous) or tributaries
distinct from• spider veins/telangiectasia
“What are they?”“What are they?”

Long tortuous & dilated veins of superficial varicose system.
Varicose veins are bulging veins that are larger than spider veins i.e. typically 3 mm or more in diameter.
Force of gravity,pressure of body weight & task of carrying blood from bottom of body up to heart make legs primary location for varicose veins.
May also occur else where i.e. Abdominal Wall,Anus,Vulva, Oesophagus.

Visible, palpable veins in the subcutaneous skin greater than 3 mm

Subcutaneous Veins
• When abnormal: - Varicose (> 3mm) - Reticular (1- 3
mm) - Telangiectasia
(spider)

Spider Veins
Etiology: Multifactorial
– Venous Hypertension associated with varicose veins
– Congenital: vascular nevi, neonatal hemangiomatosis, others..
– Collage Vascular Disease: lupus,
– Hormonal factors: pregnancy, estrogen therapy, topical steroids
– Trauma: contusion, incisions
– Infections

Spider Veins
The proper term is Telangiectasia
•These are non raised dilated veins located in the Dermis (deep layer of the skin)
•Single layer endothelium, minimal muscle
•Can be Red or Blue in color depending on the origin
•Do not cause major medical complications
•Appears earlier than varicose veins (4% of teenagers , and 13 % in 18 to 20 year olds
•More common in females
•Reticular Veins are lager feeding veins

Also called spider veins, hyphen webs, or thread veins.
Dilated intradermal venules greater than 1 mm in diameter.

Also called blue veins, subdermal varices or venulectasias.
Visible, dilated bluish subdermal, nonpalpable veins 1-3 mm.

Varicose Veins
•Incidence Increases with age
•Females to male 3 to 1
•50% of the population will affected in their life time

Etiology
• Pregnancy• Pelvic obstruction• Chronic straining• Prolonged standing• Prolonged sitting

Etiology
• Wearing constricting clothing • Obesity• Hormones• Heredity risk?
– Both parents = 80%– 50/50 chance if one parent– 20% chance if neither parent

Valvular insufficiency of the superficial veins, most commonly at the saphenofemoral junction.
Mainly caused by deep vein thrombosis (DVT) that leads to chronic deep venous obstruction or valvular insufficiency.
Catheter-associated DVTs are also included. Pregnancy-induced and progesterone-induced venous valve
weakness. Trauma.
This includes any venous malformations.i.eKlippel-Trenaunay variants,avalvulia etc.

Pathways leading to varicose veins and other clinical manifestations of venous hypertension.

Aging causes wear and tear on valves in veins that help regulate blood flow, that wear can cause valves to malfunction.
Women are more likely than men to develop condition. Hormonal changes during pregnancy or menopause may be
factor. Female hormones tend to relax vein walls. Taking hormone replacement therapy or birth control pills may
increase risk.

• If other family members had varicose veins,there's greater chance you will too.
Being overweight puts added pressure in veins.
Prolonged immobile standing impairs venous return.
Pregnancy,Abdominal/pelvic mass,Ascites,constipation etc inc: risk.

Varicose veins
“Why did I get them?”“Why did I get them?”
chronic inflammation lysosymal enzymes
– MMP collagen elastin? cause and effect
• micro AV fistulae

Varicose veins
Primary
• 27% US adults
“Secondary”
• DVT/obstruction• Pelvic mass
• Cross groin varicosities

Varicose Veins
• Appearance (Quality of Life)• Ache or pain• Itching• Swelling• Skin changes
– lipodermatosclerosis– eczema– ulceration
“Do they cause this pain, itching, burning ... ?”“Do they cause this pain, itching, burning ... ?”

Symptoms of Varicose Veins
• Pain: aching, throbbing, tingling, sharp• Cramps, heaviness, tiredness of legs• “Restless” legs at night• Itching, dermatitis, hyperpigmentation, skin
ulceration, bleeding, blood clots• All increase with dependency, resolve with leg
elevation or compression

A careful inspection & documentation of the site of varicosities is extremely important.
Look along distribution of Long saphenous vein i.e. Medial side along length of leg.
Next look along distribution of Short Saphenous vein i.e. Below knee, posterior & lateral aspects of leg.

Superficial Venous Insufficiency
• Abnormal veins- telangiectasia (spider)- reticular- Non-saphenous VV- Saphenous VV
• Abnormal skin

Superficial Venous Insufficiency
• Abnormal veins- telangiectasia (spider)- reticular- Non-saphenous VV- Saphenous VV
• Abnormal skin

Superficial Venous Insufficiency
• Abnormal veins- telangiectasia (spider)- reticular- Non-saphenous VV- Saphenous VV
• Abnormal skin

Superficial Venous Insufficiency
• Abnormal veins- telangiectasia (spider)- reticular- Non-saphenous VV- Saphenous VV
• Abnormal skin

Superficial Venous Insufficiency
• Abnormal veins• Abnormal skin
- eczema- edema- corona phlebectatica- lipodermatosclerosis- ulceration


Venous Stasis Ulcers
• Differential Diagnosis1. Venous ulcerations 50% on non healing ulcers
2. Arterial ulcers in about 10%
3. Malignancy : basal and squamous cell, lymphoma
4. Infections: HIV, fungal
5. Collagen vascular disorders: Lupus ec.
6. Lymphatic obstruction
• Affects over 1 million people in the US• 100,000 are disabled from this• More common in elderly population

Venous Stasis Ulcers
• Etiology1. Venous Hypertension
• Venous reflux• DVT• Varicose veins
2. Edema3. Biological factors
• Leakage of proteins impedes diffusion O22
• Aggregation of white cells – Block capillary flow– Release on inflammatory proteins

Varicose veins
• Progression• Skin changes ulceration• superficial thrombophlebitis• bleeding (trauma)• NO increased risk of DVT
“Are they dangerous?What complications might I get?”
“Are they dangerous?What complications might I get?”

Varicosities can lead to major complications due to poor circulation thru affected limb.
Extremely painful ulcers may form on skin particularly near ankles.
Pigmentations & skin changes ie.brownish darkening of skin resulting from extravasated blood that causes lipodermatosclerosis.
Development of carcinoma or sarcoma in longstanding venous ulcers.
Blood clotting within affected veins termed sup:thrombophlebitis that can extend into deep veins becoming more serious problem.
Acute fat necrosis can occur, esp: at ankle of overweight pats with varicose veins.

Varicose veins
• Clinical• Hand-held doppler (CWD)• Duplex
– recurrent– suspected deep venous
disease– evidence of SV disease
“What tests do I need to have done?”“What tests do I need to have done?”

Varicose veins
• Clinical assessment
• Distribution of varicosities
• Trendelenburg test
• Tourniquet test
• Perthés test
Reliable (>90%) if clinical shows LSV only but if ?SSV <50%.

Varicose Veins
Trendelenburg test– Lie patient down– identify SFJ*– apply pressure (tourniquet)– stand up
LSV

Trendelenburg

Trendelenburg

Varicose Veins
Trendelenburg test– Lie patient down– identify SFJ*– apply pressure (tourniquet)– stand up
• If veins do not fill– SFI confirmed
• IF veins do fill– perforators± SFI
LSV

Varicose Veins
Tourniquet test– Lie patient down– apply three tourniquets– stand up– release serially

Modified Trendelenberg

Modified Trendelenberg

Modified Trendelenberg

Modified Trendelenberg

Varicose Veins
Perthés test– apply tourniquet below knee– stand up– tip toe manoeuvres– if veins fill– perforators incompetent
normal
abnormal

Diagnosis of venous disease
• Physical exam• Appearance• Trendelenburg test• Palpation• Hand Doppler
• Duplex Examination• R/O DVT• Size of veins• Map out superficial veins• Locate the site of reflux• Reflux 0.5 sec in GSV and 1 sec in
deep system• Find refluxing perforators

This is physical exam: technique to localise valves that are incompetent
Lie patient down & raise leg attempting to drain varicosities Using either tourniquet or fingers put pressure over SFJ to
occlude it & ask patient to stand If varicosities don’t refill indicates SFJ incompetence & if do
refill then leaky valve is lower down Now try and locate incompetent perforators Place tourniquet aprox: over area of each perforator i.e.mid
thigh,sapheno popliteal,calf perforators If varicosities don’t refill that perforator is incompetent & if
varicosities do refill continue down leg

Evaluation of Vein Patients
• H & P– Coagulopathy– Thrombophlebitis or DVT– PAD– Results of previous treatment
• Blood flow tests– Most tests non-invasive– Hand-held Doppler– Duplex ultrasound
• Patient selection

Patterns of Reflux1. Truncal or saphenous related
reflux- GSV: 4/6 of VV- SSV: 1/6 of VV
2. Non-truncal reflux: 1/6 of VV- Pudendal, perforators- LSVS, Giacomini

This is also physical exam: technique in which tourniquet is placed over prox: part of leg to compress any sup: varicose veins while leaving deep veins unaffected.
Pat walks to activate calf-muscle pump which normally causes varicose veins to be emptied.
If obstruction of deep system exists then activation of calf-muscle pump causes paradoxical congestion of sup:venous system and engorgement of varicose veins resulting in positive test.
To verify pat is then placed supine & leg is then elevated (Linton test).
If varices distal to tourniquet fail to drain after a few seconds again deep venous obstruction must be considered.

Doppler transducer is positioned along axis of vein with probe at angle of 45° to skin.
When distal vein is compressed audible forward flow exists .
If valves are competent no audible backward flow is heard with release of compression.
If valves are incompetent an audible backflow exists.
These compression-decompression maneuvers are repeated while gradually ascending limb to level at which reflux can no longer be appreciated .

Duplex US with color-flow imaging sometimes called triplex ultrasound.
This is special type of 2-dimensional ultrasound that uses Doppler-flow information to add color for blood flow in image.
Vessels in blood are colored red for flow in one direction and blue for flow in other with graduated color scale to reflect speed of flow.
Venous valvular reflux is defined as regurgitant flow with Valsalva that lasts great than 2 seconds.

Venous Duplex
• R/O DVT
• Scan deep system in cross section, look for total compression of the vein in B mode
• Examine from the femoral vein to the below the pop
• Check flow characteristics with Doppler
– Sharp up stroke with calf compression
– Small or No flow with relaxation
• R/O DVI
• This must be done with patient upright
• Reversal of flow of > 1 sec with Valsalva or after calf compression

Duplex Anatomy
• Locate GSV Junction(FSJ)• Look for Mickey's hat
Normal venous flow Look at valve
Venous flow is opposite the artery

Scan of Common Femoral Vein
•Look for filling defect
•Look for compressibility
•Filling defects
•Echogenicity of defect
• Fresh
• Old
Femoral vein scan.avi

Venous Duplex• Examine superficial system with patient upright
• Start with the GSV at the groin and follow to below knee
• Take cross section diameter measurements• Doppler in longitudinal for reflux > 0.5 sec significant• Look for mid Thigh perforators and look for reflux• Draw map of GSV and other superficial tributaries
– Examine the Small Saphenous• Look for size and reflux• Find connection to deep system• Look for the vein of Giacomini ( superior extension of SSV to
the GSV)

Anatomy of Great Saphenous
• Femoral junction has multiple branches• Runs on medial side of leg down to
ankle• Found in a facial sheet• Perforators connect it to deep system

Anatomy of Great Saphenous
From Jose Almeida, MD, IVC talk

Anatomy of Great Saphenous
From Jose Almeida, MD, IVC talk

Duplex Of Saphenous Proximal
Reflux at the Saphenous Femoral JunctionLook at reversal of flow
Locate Terminal valves
Epigastric vein
Femoral Vein
Epigastric Vein
Fem Vein
Saphenous

Duplex Mid Thigh

Duplex Ultrasonography
• Replaced plethysmography and venography
- 7-10MHz linear transducer- Exam sitting and standing - Superficial and deep
systems evaluated- Physiologic reflux: < 0.5
sec- Pathologic reflux: > 0.5
sec

This is a physiologic test,using plethysmography.
VRT is time necessary for lower leg to become infused with blood after calf-muscle pump has emptied lower leg.
In healthy subjects VRT is greater than 120 seconds In pats with significant venous insufficiency VRT is abnormally
fast at 20-40 seconds.
VRT of less than 20 seconds is markedly abnormal & is nearly always symptomatic.
If VRT is less than 10 seconds venous ulcerations are likely.

Most sensitive & most specific test to find causes of anatomic obstruction.
MRV is particularly useful b/c unsuspected nonvascular causes for leg pain and edema may often be seen on scan image when clinical presentation erroneously suggests venous insufficiency or venous obstruction.
This is expensive test used only as adjuvant when doubt still exists.

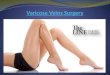
Treatment of Varicose Veins
– Conservative management• Exercise• Leg elevation• Compression stocking
– Surgical treatment• Standard Ligation and stripping• Phlebectomies
– Minimally invasive procedures (Currently accepted standard)
• Laser Ablation• Radio Frequency ablation• Sclerotherapy

Elevating legs often provides temporary symptomatic relief.
Wearing of graduated compression stockings with pressure of 30–40 mmHg has been shown to correct swelling, nutritional exchange & improve microcirculation in affected legs.
Caution should be exercised in patients with concurrent arterial disease.
They are offered in different levels of compression.
They are constructed using elastic fibers or rubber which help compress limb, aiding in circulation.


It is commonly performed non-surgical treatment.
Often used for spider veins & varicose veins that persist or recur after vein stripping.
Sodium tetradecyl sulphate etc is inj: in veins to make them shrink.
Sclerotherapy can also be performed using foamed sclerosants under ultrasound guidance to treat larger varicose veins including GSV & SSV.
In U/S guided sclerotherapy u/s is used to visualize underlying vein so surgeon can deliver and monitor injection.
Microsclerotherapy is used to treat spider veins & other very small varicose veins.

Sclerotherapy
• Cumulate vein with needle• Inject Sclerosing Solution
– Sotradecol (Sodium tetradecyl sulfate)– Pilodocanol– Hyper tonic Saline– Foam (Mix STS with air and make bubbles)
• Intravenous injection causes intima inflammation and thrombus formation

Sclerotherapy Use
• Neovascularization• Perforators• Clean up after Phlebectomies• Spider veins• Reticular veins• GSV: can closure the, but has high recurrence rate

Sclerotherapy results

Less Invasive Options

ClosureTM Procedure
A Minimally Invasive Alternative to Vein Stripping Surgery

ClosureTM Procedure

Closure Procedure Method
• Local, regional, or general anesthesia• Access vein• Insert catheter into the vein and advance closure
catheter tip to SFJ using US• Compress saphenous vein and displace blood away
from catheter electrodes

Pre/Post

Pre/Post

Pre/Post

Varicose veins
Long saphenous
• Groin exploration
– saphenofemoral ligation
• Stripping (to knee)
Short saphenous
• ligation of SSPV
Both
• multiple avulsions
“What does the operation consist of ?”
“What does the operation consist of ?”
SSV
LSV

Treatment of primary varicose veins by endovenous obliteration with the VNUS closure system: results of a prospective multicentre study
RFA saphenous vein obliteration improves symptoms of varicose veins. Reflux-free rates in treated veins remain constant over 3 yr f/u.
Eur J Vasc Endovasc Surg. 2005 Apr;29(4):433-9.

Standard Surgical Treatment
• Saphenous vein ligation• Saphenous vein stripping +/- ligation• Flush SFJ ligation, stripping thigh portion of
GSV with excision of tributaries and stab phlebectomies of VV
• SEPS (subfascial endoscopic perforator surgery)

Surgical ligation and Stripping
• Standard treatment for a century
• General anesthesia• Pain• Long recovery• Some complications• Good cosmetic results

Surgical Complications
• Wound Infection• Hematoma/severe bruising• Scarring, Keloid scars • DVT• Recurrence• injury to sural or saphenous nerve. • Hard tender lumps can sometimes
form along the line of removed vein which usually disappears after few weeks.

GSV Saphenectomy
Surgical removal of GSV have evolved from large open incisions to less invasive stripping.
Stripping consists of removal of all or part of saphenous vein main trunk
Different devices are used in stripping i.e Mayo stripper, Babcock device, Keller device etc.
Perforation-invagination (PIN) stripper is mainly used now a days.
Technique of PIN stripping begins with 2-3cm incision made at groin.

Femoral vein and SFJ are exposed with dissection & all tributaries of SFJ must be identified and flush-ligated to minimize incidence of reflux recurrence.
Vessel is then inverted into itself tearing away from each tributary & perforator as stripper is pulled downward thru leg & out thru incision in upper calf.
Long epinephrine-soaked gauze or ligature may be secured to stripper before invagination allowing hemostatic packing to be pulled into place after stripping is complete.


SSV Saphenectomy
Removal of SSV is complicated by variable local anatomy and risk of injury to popliteal vein & peroneal nerve
Saphenopopliteal junction must be located by duplex exam: before beginning dissection.
After ligation and division of junction stripping instrument is passed downward into distal calf where it is brought out thru a small incision (2-4 mm).
Stripper is secured to proximal end of vein which is invaginated into itself as it is pulled downward from knee to ankle and withdrawn from below.

Varicose Veins
• Recurrent/residual varicosities (22% by 6 years)– inadequate primary surgery– avulsion (LA)– sclerotherapy
• Compression stockings
“Will I be cured - can they come back? ”

It is extremely useful for treatment of residual vein clusters after saphenectomy & for removal of nontruncal tributaries when saphenous vein is competent.
Microincision is made over vessel phlebectomy hook is introduced & vein is delivered thru incision.
With traction, as long a segment as possible is pulled out of body until
vein breaks or cannot be pulled any further.
Another microincision is made and process is begun again and repeated along entire length of vein to be extracted.
Pat can go home same day after procedure is done.

Vein Ablation
• Laser Ablation (EVLA or EVLT)• Uses light to heat the vein
• Radio Frequency (VNUS Procedure)• Uses radio frequency to heat the vein
• Office based procedure• Done under local anesthesia• One needle puncture at the level of the
knee• Takes about 1 hour• Patient resumes normal activity same day

Vein Ablation Steps

EVLA Results
Images from http://venacure-evlt.com/

EVLA Results
Images from http://venacure-evlt.com/

EVLA Results
Images from http://venacure-evlt.com/

Laser fiber produces endoluminal heat that destroys vascular endothelium.
Seldinger technique is used to advance long catheter along entire length of truncal varicosity to be ablated.
Under U/S guidance tumescent solution with local anesthetic is inj: around entire length of vessel.
Firm pressure is applied to collapse vein around laser fiber & laser is fired generating heat leading to intraluminal steam bubbles,irreversible endothelial damage & thrombosis.
This process is repeated along entire course of vessel

RF thermal energy is delivered directly to vessel wall causing protein denaturation, collagenous contraction & immediate closure of vessel.
Metal fingers at tip of RF catheter are deployed until they make contact with vessel endothelium.
RF energy is delivered both in and around vessel to be treated.
Thermal sensors record temp: within vessel & deliver just enough energy to ensure endothelial ablation.
RF catheter is withdrawn a short distance & process is repeated all along length of vein to be treated

Endovascular occlusion of Saphenous veins using VNUS ClosureTM Catheter

Treatment of Small Vein disease
• Female• Heredity• Pregnancy• Steroid or estrogens• Red or blue in color• Close to surface and not raised

Common Symptoms
• Localized pain - similar to a bruise• Burning sensation• Aching• Often no symptoms. Treatment cosmetic only• Symptoms worsened by warm weather and/or by
menstrual cycle

Treatment Options
• Conservative – use of support hose to control symptoms
• Injection Sclerotherapy• Laser or light source therapy

Modern Sclerosants
• Detergents• Hypertonic and ionic solutions• Cellular toxins

Detergents
• Most commonly used – protein denaturation• Sodium morrhuate, sotradecol, polidocanol• Liquid or Foam

Polidocanol (0.5%)
Advantages• Injection is
Painless• Extravasation
No Necrosis
Disadvantages
• Pigmentation Intermediate

Sclerotherapy - Results
• Excellent for small veins: reticular, telangiectasias
• High recanalization rates for larger veins• GSV: > 50% recurrent reflux by US, which is
likely the prelude for recurrence of VV

Before and After

Sclerotherapy-Complications
• Pigmentation
• Matting

Sclerotherapy-Complications
Ulceration

Sclerotherapy vs. Surgery• Prospective 10 year study (121 96)• VV and superficial incompetence• Group A: Sclerotherapy (39)• Group B: Ligation + Sclerotherapy (40)• Group C: Ligation only (42)• No incompetence at SFJ in surgical groups• Sclerotherapy with 20-44% reflux• Sclerotherapy cheaper, surgery superior
Belcaro G, et al. Angiology 2000; 51:529-534.

Sclerosing Foam
• Orbach(1944): the air block technique
• Displaces blood• Induces more spasm• Tiny bubbles covered
by tensio-active liquid• Treat larger veins

1ml of 3% STS injected in a vein dilutes with 10ml of blood
Final drug concentration: 0.3%
1ml of 1% Foam STS injected in the same vein displaces blood
Final drug concentration: 1%

Sclerosing Foam
• Less volume • More potent• Morbidity appears
similar to liquid sclerosants
• Being used clinically since 1997, results in GSV better than liquid ~ 20-30% recanalization

Procedure• Several injections per visit with small gauge needles• Injected areas become reddened and “bee sting”
wheals occur for several hours• Moderately uncomfortable• Several treatments• Compressive bandaging after treatment• Appearance often “worse before better”

Patient Selection• Better results with injection of spider veins
and small varicose veins• Some patients require combination of surgery
for large veins followed by sclero for smaller veins
• Large varicose veins when injected may re-open soon after treatment
• Higher risk of complications with sclerotherapy of large varicose veins

Contraindications
• Pregnancy• Inability to walk• Allergy to sclerosant

Post Sclerotherapy Instructions• Avoid vigorous impact activities for 3 days• Compliance with use of compression garment• Avoid prolonged sun exposure for several weeks• Follow up visits essential for best results

Long Term Results
• 80-90% clearing of treated area• Improvement of symptoms• Cosmetic improvement• Variable rate of recurrence

SclerotherapyBefore After

SclerotherapyBefore After

SclerotherapyBefore After

10 Week Interval

Mechanism of Action• Beam is directed to and heats a target vessel• Blood in the vein coagulates, vessel is destroyed• Minimal effect on surrounding skin and tissue
Laser or Light Source Therapy

Procedure
• Avoid sun exposure for 2 months prior to treatment• Protective eye gear is worn by the patient and
practitioner• Cooling gel is applied to the skin before treatment

Procedure
• Multiple pulsed light wavelengths directed at the vein with variable strength of laser energy
• Moderate discomfort during treatment similar to “snap of a rubber band”
• Multiple treatments usually necessary

Risks
• Crusting or blistering of the skin• Loss of pigmentation of skin “white dots”• Increase in pigmentation “dark streaks”• Transient redness / swelling of skin• Most pigmentation changes resolve with time

Increase in Pigmentation “Dark Streaks”

Laser Treatment
• Advantages– Non- invasive ( no needles)– “State of the art” - most current therapy
• Disadvantages– Costly– Uneven results– Not amenable to all skin types– Not applicable to all types of veins

Post Treatment Instructions
• No vigorous exercise for 3 days• Continuous support hose for 1 week• Antibacterial ointment to treated areas for 7 days• Avoid sun exposure until healed, 4-6 weeks

Patient Selection
• Best results on small spider veins of the face or legs• Better results with fair skin types• No suntanned skin • Poor results on varicose veins