Embed Size (px)
Citation preview

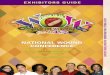
Wound Care This article discusses the management of chronic wounds. This topic is naturally diverse and far-reaching. Wound care in general and in terms of specific etiologies is considered. The images below depict a sacral pressure ulcer.
Image of advanced sacral pressure ulcer shows the effects of pressure, shearing, and moisture.
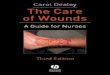
Sacral pressure ulcer before and after flap closure.
Epidemiology
Frequency
Pressure ulcers occur in approximately 9% of hospitalized patients, usually during the first 2 weeks of hospitalization. A study found that even with the use of a pressure-reducing bed and early nutritional support, 3% of patients in a surgical intensive care unit who were employed in the study developedpressure ulcers.[2] The annual risk of pressure ulceration in patients with neurologic impairment is 5-8%, with a lifetime risk of approximately 85% and a mortality rate of 8%.
The prevalence of pressure ulcers among patients residing in long-term care facilities has been reported as 2.3-28% and has been an increasingly common reason for litigation.[3, 4, 5, 6, 7] The presence of a pressure ulcer increases a nurse's workload by 50% for the patient and adds approximately $20,000 to the hospital bill. The treatment of pressure ulcers in the United States is estimated to cost more than $1 billion annually.
Venous ulcers make up 70% of chronic lower extremity ulcers.[8] The incidence of venous ulcers in the United States is approximately 600,000 cases annually. The recurrence rate is up to 90%.
According to the National Institute of Diabetes and Digestive and Kidney Diseases, an estimated 18 million Americans (6.3% of the population) are known to have diabetes,
1

and millions more are considered to be at risk. Of those at risk, diabetes is undiagnosed in 5.2 million. Diabetic foot lesions are responsible for more hospitalizations than any other complication of diabetes. Among patients with diabetes, 15% will develop a foot ulcer, and 12-24% of those with a foot ulcer will require amputation. Indeed, diabetes is the leading cause of nontraumatic lower-extremity amputations in the United States, accounting for 60% of these amputations.
Every year approximately 5% of persons with diabetes develop foot ulcers, and 1% require amputation.[9] Diabetic peripheral neuropathy confers the greatest risk of foot ulceration; microvascular disease and suboptimal glycemic control contribute. Even with successful treatment resulting in ulcer healing, the recurrence rate in that patient population is 66%, and the amputation rate rises to 12%.[10]
Etiology
In general, factors that adversely affect wound healing can be remembered by using the mnemonic device DIDN'T HEAL, as follows:
D = Diabetes: The long-term effects of diabetes impair wound healing by diminishing sensation and arterial inflow. In addition, even acute loss of diabetic control can affect wound healing by causing diminished cardiac output, poor peripheral perfusion, and impaired polymorphonuclear leukocyte phagocytosis.
I = Infection: Infection potentiates collagen lysis. Bacterial contamination is a necessary condition but is not sufficient for wound infection. A susceptible host and wound environment are also required. Foreign bodies (including sutures) potentiate wound infection.
D = Drugs: Steroids and antimetabolites impede proliferation of fibroblasts and collagen synthesis.
N = Nutritional problems: Protein-calorie malnutrition and deficiencies of vitamins A, C, and zinc impair normal wound-healing mechanisms.
T = Tissue necrosis, resulting from local or systemic ischemia or radiation injury, impairs wound healing. Wounds in characteristically well-perfused areas, such the face and neck, may heal surprisingly well despite unfavorable circumstances. Conversely, even a minor wound involving the foot, which has a borderline blood supply, may mark the onset of a long-term, nonhealing ulcer. Hypoxia and excessive tension on the wound edges also interfere with wound healing because of local oxygen deficits. See, for example, the pressure ulcers shown in the image below.
2

Pressure ulcers of the lateral aspect of the right foot.
H = Hypoxia: Inadequate tissue oxygenation due to local vasoconstriction resulting from sympathetic overactivity may occur because of blood volume deficit, unrelieved pain, or hypothermia, especially involving the distal extent of the extremities.
E = Excessive tension on wound edges: This leads to local tissue ischemia and necrosis.
A = Another wound: Competition between several healing areas for the substrates required for wound healing impairs wound healing at all sites.
L = Low temperature: The relatively low tissue temperature in the distal aspects of the upper and lower extremities (a reduction of 1-1.5°C [2-3°F] from normal core body temperature) is responsible for slower healing of wounds at these sites.
Specific etiologies
Arterial insufficiency
See Infrainguinal Occlusive Disease.
Venous insufficiency
Patients with varicose veins or nonfunctional venous valves after deep vein thrombosis develop ambulatory venous hypertension, that is, distal venous pressure remains elevated despite ambulation. This constant venous hypertension seems to cause white cell and fibrin buildup, which impairs capillary blood flow or traps growth factors. Macromolecules pass into the dermis and eventually cause the hemosiderin deposition and brawny induration in the distal leg (gaiter area) characteristic of chronic venous insufficiency.
Lymphedema
Although not typically a cause of ulceration, extremity ulcers may fail to heal because of untreated lymphedema. Nocturnal leg elevation and elastic wraps or support hose are appropriate adjuncts to the treatment of recalcitrant wounds in edematous extremities. For advanced and nonresponsivelymphedema, complex decongestive physiotherapy is a useful treatment option.
Neuropathy
Sensory neuropathy involving the feet may lead to unrecognized episodes of trauma caused by ill-fitting shoes. This is compounded by motor neuropathy causing intrinsic muscle weakness and spaying of the foot on weight bearing. The result is a convex foot with a rocker-bottom appearance. Multiple fractures go unnoticed, until bone and joint deformities become marked. This is termed a Charcot foot (ie, neuropathic osteoarthropathy) and is observed most commonly in people with diabetes mellitus, affecting approximately 2% of persons with diabetes.
Pressure (decubitus) ulcers
3

Pressure (decubitus) ulcers occur because of prolonged ischemia-producing external pressure, usually to a soft tissue region overlying a bony prominence. Tissue ischemia results when external pressure exceeds capillary closing pressure (ie, 25-32 mm Hg in healthy individuals), the minimum pressure that causes collapse of the capillary when applied to a capillary bed.
Shearing forces, exposure to constant moisture, and heat buildup also are major contributing factors. For example, the stratum corneum, the outer layer of skin, becomes 25 times more fragile at a relative humidity of 100% than at a relative humidity of 25% and becomes 4 times more fragile at 95°F (35°C) than at 86°F (30°C).
Neoplasms
Neoplasms strongly suggest malignancy in any chronic nonhealing wound, particularly if the wound appears to have occurred spontaneously.[11]
Basal cell carcinoma appears smooth, pearly, and elevated above the skin surface, as illustrated in the image below, whereas squamous cell cancer is often somewhat erythematous and scaly and almost always occurs on sun-exposed areas. Particularly pertinent in wound care is the so-called Marjolin ulcer, a squamous cell carcinoma originating in a chronic wound, such as a burn scar or sinus tract.[12] This implies that even a wound that is decades old is not necessarily benign. Patients with Kaposi sarcoma typically present with multifocal violaceous lower extremity lesions. Patients with cutaneous lymphoma present with a single nodule or a group of papules from one to several centimeters in diameter, and these almost always occurs above the waist.
Basal cell cancer manifesting as a chronic leg ulcer.
Perform a biopsy of every wound suggestive of neoplasm, but remember that biopsy findings are diagnostic only if an adequate representative specimen is obtained.
Radiation damage
The adverse effects of prolonged or excessive electromagnetic radiation vary with the wavelength. Wavelengths of electromagnetic radiation are as follows:
Gamma rays - Less than 0.01 nm X-rays - 0.01-10 nm Ultraviolet C - 10-280 nm Ultraviolet B - 280-320 nm
4

Ultraviolet A - 320-400 nm Visible light - 400-760 nm Infrared - 760 nm to 1 mm Microwave - 1 mm to 30 cm Radio waves - Centimeters to meters
Gamma radiation and x-ray exposure cause a zone of stasis, in which local blood supply is impaired by coagulative necrosis due to thrombotic occlusion of smaller arteries. Gamma and x-ray radiation also spawn ionized oxygen that adversely affects DNA. The long-term result is inhibition of regeneration of skin cells from dividing basal cells. This may cause recalcitrant painful skin ulcers. The surrounding skin is atrophic, with atrophy of hair follicles and a paucity subcutaneous fat.
Ultraviolet radiation exposure, particularly ultraviolet B, causes sunburn initially and subsequently conveys a continuing risk of skin malignancy (eg,basal cell carcinoma, squamous cell carcinoma, melanoma).
Excessive exposure to infrared radiation, which induces repeated or persistent skin hyperthermia of 43-47°C, may cause erythema ab igne. Patients with this skin condition present with telangiectasia, erythematous patches, and hyperpigmentation.
Atheroembolism syndrome
Patchy areas of ischemia involving the feet, especially in the presence of palpable pedal pulses, suggest the possibility of atheroembolism of plaque fragments from ulcerated, although nonocclusive, proximal atherosclerotic plaques or from thrombi lining the wall of an infrarenal aortic aneurysm.
Pyoderma gangrenosum
Pyoderma gangrenosum usually starts as a small painful papule or nodule, which is often erroneously presumed to be the result of an insect bite. The lesion enlarges, becomes ulcerated, and develops overhanging, violaceous borders, as shown in the image below.
Chronic ulcer of medial aspect of right leg due to pyoderma gangrenosum.
The histologic findings often are nonspecific. Associated underlying systemic problems, which occur in one half of patients with pyoderma gangrenosum, are often the best clues to the diagnosis. Examples of such systemic diseases include various arthritides, inflammatory bowel disease, hepatitis, myeloproliferative disorders, myeloma, primary
5

biliary cirrhosis, systemic lupus erythematosus, and Sjögren syndrome. An important clue is a paradoxical response in which debridement exacerbates the wound, particularly near the areas debrided. When myofascial and osseous tissues become involved, the only choice may be surgical debridement to try to save the extremity.[13, 14]
Sickle cell
Patients with sickle cell–associated leg ulcers typically present with painful small ulcers that start as crusting nodules in the distal one third of the leg, often near the malleoli. The surrounding skin demonstrates absence of hair follicles, hyperpigmentation, and atrophy of subcutaneous fat. Radiograph findings may reveal periosteal thickening of underlying bone; true osteomyelitis is rare. Sickle cell ulcers are more common in males than in females and occur predominantly in persons aged 10-50 years. Patients with sickle cell anemia can also develop leg ulcers because of other etiologies; the physical examination should exclude arterial and venous insufficiency.
Calciphylaxis
Calciphylaxis is an unusual and often fatal syndrome of cutaneous necrosis that tends to develop in patients with chronic renal failure, particularly those with diabetes. The average time of onset is 3 years after the start of dialysis. The female-to-male ratio is 3:1. The initial finding of calciphylaxis may be that of livedo reticularis, followed by painful erythematous areas of thickening of the skin and subcutaneous tissues. The most common site is the thigh, though the condition may also occur in the legs or the upper extremities.[15, 16]
Panniculitis signaling the onset of calciphylaxis may be precipitated by trauma, such as the site of an injection. Proximal painful myopathy, muscle weakness, and elevated serum creatine kinase (CK) levels may occur. Laboratory testing may demonstrate a high serum phosphate level and an elevated parathyroid hormone level. Skin biopsy reveals calcification of the arterial media and luminal stricture of small-to-medium blood vessels in the subcutaneous fat. Muscle biopsy shows patchy necrosis and atrophy.[17]
Necrobiosis lipoidica
Necrobiosis lipoidica usually involves the anterior tibial areas, though it can also occur in the face, arms, and chest. Patients present with well-circumscribed, shiny, reddish-brown, oval, painless nodules or papules that have a thick shiny surface. Over several months or a year, the lesions may gradually expand and develop a waxy yellow color. Trauma may lead to infected ulcerations, and involvement of adjacent cutaneous nerves may precipitate considerable pain. Necrobiosis lipoidica is more common in women and in persons with diabetes than in others, but it may also occur in persons without diabetes and before the diagnosis of diabetes.[18] Long-standing necrobiosis lipoidica may harbor a squamous cell carcinoma.
Vasculitic wounds
Vasculitic wounds tend to occur throughout the lower legs as multiple, small, painful, erythematous nodules. Scars resulting from previous vasculitic lesions may be a useful clue. Any of the disparate systemic manifestations of the diseases of cellular immunity
6

associated with atypical skin lesions, including unexplained fevers, jaw claudication, malaise, Raynaud phenomenon, myalgias, neurologic abnormalities, and craniofacial pain syndromes, suggest the possibility of vasculitis. These lesions are rare.
The differential diagnosis of wounds with these features includes other uncommon problems, such as anticoagulant-induced skin necrosis, atheroembolism syndrome (ie, trash foot), and Buerger disease. Leukocytoclastic vasculitides represent a disparate group of acquired connective tissue problems; patients present with palpable purpuric skin lesions, petechiae, and ecchymoses, usually involving the lower extremities. These syndromes include Wegener granulomatosis, Sjögren syndrome, cryoglobulinemia, systemic lupus erythematosus, rheumatoid arthritis, dermatomyositis, and hepatitis B. The common factor among these syndromes is a hypersensitivity angiitis.[19]
Skin biopsy demonstrates cuffing of the dermal microcirculation by granulocytes, which are found in diverse stages of viability, including complete cellular disintegration (ie, nuclear dust). The various disorders in this group are differentiated by clinical and serologic criteria. The presence of asymptomatic palpable purpura without thrombocytopenia suggests a drug adverse effect, such as those caused by iodides, penicillin, aspirin, chlorothiazides, oxytetracycline, isoniazid, or benzoic acid.
Anticoagulant-induced skin necrosis
Anticoagulant-induced skin necrosis is an unusual complication of anticoagulant therapy.[20] It may occur with heparin or warfarin, though it is more common with warfarin. Warfarin-induced skin necrosis manifests as painful hemorrhagic skin lesions, usually in an area having abundant adipose tissue, such as the thighs, abdomen, or breasts. The female-to-male ratio is 4:1.
This complication is often attributable to hereditary coagulation abnormalities. Warfarin (Coumadin) depletes vitamin K–dependent coagulation factors, such as protein C. Therefore, during the first several days of warfarin therapy, a period of transient hypercoagulability may occur, particularly in patients with hereditary coagulation abnormalities, such as protein C deficiency or protein S deficiency, antithrombin 3 deficiency, or activated protein C resistance.[20]
Actinomycosis
Actinomyces israelii is a fastidious anaerobic bacterium that is relatively common and usually nonpathogenic. In rare individuals, particularly hosts who are immunocompromised, the bacterium can become pathogenic and cause chronic, draining, painless skin ulcers and sinuses, usually in the head and neck. False-negative tissue cultures are common because the organism is often difficult to culture in vitro. However, microscopic examination of wound exudates may demonstrate characteristic sulfur granules. Actinomycosis is responsive to penicillin but requires long-term therapy.
Yaws
Yaws is a treponematosis caused by Treponema pertenue, which is endemic in humid regions near the equator. Approximately 3-4 weeks after exposure, a pruritic sore that resembles a raspberry (the mother yaw) develops at the site where the spirochete
7

enters the skin. This lesion eventually opens to form an ulcer. Scratching spreads the organism and results in multiple tubercles and ulcerations elsewhere, including the hands, feet, and genitals. These ulcers may have a caseous crust. Results of serologic testing for syphilis may be positive.
Treatment is with a single large dose of penicillin. Untreated yaws can erode to bone and joints and can become deforming and crippling.
The lesions of pinta, caused by Treponema carateum, are similar to those of yaws, but, unlike yaws, no ulceration is present. Pinta typically begins as a papule on the dorsum of the foot or leg. The papule enlarges and becomes a pruritic plaque, which changes from a copper to gray to bluish color over time. Regional lymphadenopathy may occur. Pinta is also responsive to penicillin.
Mucormycosis
Mucormycosis is an acute and sometimes rapidly progressive, even fatal, fungal infection that may occur in patients who are immunocompromised, especially following a burn. The primary lesions are plaques, ulcerations and abscesses, or painful ecchymotic nodules, which may ulcerate and then become necrotic and form eschars. The diagnosis is confirmed by demonstrating fungal elements of the black discharge in KOH preparations and by culturing on standard laboratory media.
Cutaneous anthrax
Cutaneous anthrax results from skin exposure to Bacillus anthracis, a gram-positive bacillus. Cutaneous anthrax evolves from a pruritic papule to an ulcerated wound in 1 or 2 days and then into a black eschar over the next week or so. Associated regional lymphadenopathy may be present. Findings on special stains and cultures of the wound exudate are diagnostic.
Anthrax is transmissible from specimens; therefore, so laboratory personnel should be warned in the event of clinical suspicion of this disease. Of course, appropriate public health authorities must be notified.
Pathophysiology
The phases of normal wound healing can be described as follows:
Hemostatic or inflammatory phase
This phase starts immediately and lasts 2-5 days. Tissue damage releases chemical mediators called cytokines (eg, transforming growth factor [TGF]-beta [interleukin-1beta]), which initiate a complex interrelated process that causes hemostasis and begins the healing process. Platelets aggregate to stem bleeding. They also release serotonin and other vasoconstrictors and activate the coagulation cascade. The result is conversion of fibrinogen into fibrin, which stabilizes the platelet plug. At that point, prostaglandins and activated complement cause vasodilation and increase capillary permeability. This allows plasma to leak into the tissue surrounding the wounded area. This is the inflammatory exudate.
8

Monocytes and neutrophils are attracted to the site of injury. Neutrophils trap and kill bacteria immediately, while monocytes become activated macrophages, which produce growth factors and cytokines and scavenge nonviable tissue and bacteria. Angiogenic growth factors stimulate neovascularization of the wound bed.
Proliferative phase
This phase lasts from 2 days to 3 weeks. Macrophages recruit fibroblasts. These cells create a network of collagen fibers. When adequate oxygen and vitamin C are present, granulation tissue forms. Oxygen is incorporated by 2 amino acids, proline and lysine, which are both required for collagen chain synthesis. Vitamin C is required for the hydroxylation of proline to hydroxyproline, an amino acid found in collagen.
During granulation, fibroblasts create a collagen bed to fill the defect and grow new capillaries. During contraction, myofibroblasts pull the wound edges closer together to decrease the size of the wound. During epithelialization, new epithelium migrates from the intact epidermis around the wound and can grow up to 3 cm over the granulation tissue. This process requires a moist surface.
Remodeling phase
This phase lasts from 3 weeks to 2 years.[21] An organized form of collagen gradually replaces the immature, soft, gelatinous collagen. The effect is to increase the tensile strength of the healed wound, but it is less than 80% as strong as the original tissue.
Types of wound healing
First intention, also termed primary healing, is the healing that occurs when a clean laceration or a surgical incision is closed primarily with sutures, Steri-Strips, or skin adhesive.
Second intention, also termed secondary healing, is the healing that occurs when a wound is left open to heal by granulation, contraction, and epithelialization.
Delayed primary closure is a combination of the other 2 types of wound healing. It is often intentionally applied to lacerations that are not considered clean enough for primary closure. The wound is left open for 5-10 days; then, it is sutured closed to decrease the risk of wound infection.
Indications
All chronic wounds require assessment.[22] Many heal with topical wound care; some require surgical intervention. The details vary widely with the nature of the wound. This article provides information regarding wound care in general and specific wound etiologies in particular.
9

Relevant Anatomy
Life is a constant battle against entropy (i.e., disorder). The skin provides the primary barrier between the human protoplasm and the entropy of the external environment. Histologically, the skin is divided into the epidermis and the dermis.
The epidermis consists of 5 histologic strata. From superficial to deep these layers are the (1) stratum corneum, (2) stratum lucidum, (3) stratum granulosum, (4) stratum spinosum, and (5) stratum germinativum. The keratinocyte, the preponderant epidermal cell, is generated in the stratum germinativum and eventually desquamates (sloughs) when it reaches the stratum corneum.
The dermis underlies the epidermis. A dermal vascular network functions in thermoregulation and provides metabolic support for the avascular epidermis. Fibroblasts synthesize supportive and structural polymers, including ground substance, collagen, and elastin.
Skin appendages include sebaceous glands, hair follicles, and sweat glands.
Laboratory Studies
Tests that sometimes are useful in identifying underlying factors that can slow wound healing include the following:
CBC to assess for leukocytosis, anemia, and thrombocytopenia Analysis of the patient's basic metabolic profile to look for renal insufficiency and
electrolyte abnormalities Determination of serum protein, albumin, prealbumin, and transferrin levels to assess
the patient's nutritional status Coagulation studies to evaluate for coagulation abnormalities, especially if deep
wound excision is required Tissue cultures of wound to determine appropriate antibiotic therapy
Laboratory studies that may play a role in evaluating specific wound etiologies include vascular laboratory studies (eg, plethysmography, pulse-volume recordings [PVRs]) to check the hemodynamic significance of arterial occlusive disease.
Imaging Studies
Imaging studies that may play a role in evaluating certain wound etiologies. Plain radiography, CT, and MRI may help in looking for underlying osseous
abnormalities, proximity of the wound to hardware, or foreign bodies. Vascular ultrasonography may be indicated to evaluate for aneurysmal disease or
deep venous occlusion. Bone scanning may be needed to look for possible osteomyelitis. Technetium-99m–
labeled WBC scanning (Ceretec) has high specificity and sensitivity for osteomyelitis. However, it requires 24 hours for completion and it lacks anatomic detail.
10

Diagnostic Procedures
Perform a biopsy of every suspicious wound, but remember that biopsy results are diagnostic only if an adequate representative specimen is obtained.
Medical Therapy
General treatment of nonhealing wounds can be described as follows:
See Treatment of specific types of wounds.
Assess the entire patient
Successful treatment of difficult wounds requires assessment of the entire patient and not just the wound. Systemic problems often impair wound healing; conversely, nonhealing wounds may herald systemic pathology.
Consider the negative effects of endocrine diseases (eg, diabetes, hypothyroidism), hematologic conditions (eg, anemia, polycythemia, myeloproliferative disorders), cardiopulmonary problems (eg, chronic obstructive pulmonary disease, congestive heart failure), GI problems that cause malnutrition and vitamin deficiencies, obesity, and peripheral vascular pathology (eg, atherosclerotic disease, chronic venous insufficiency, lymphedema).
Characterize the wound
Assess the following: (1) size and depth of involvement and the extent of undermining; (2) the appearance of the wound surface, that is, necrotic or viable; (3) amount and characteristics of wound exudate; and (4) status of the periwound tissues (eg, pigmented, scarred, atrophic, cellulitic).
Ensure adequate oxygenation
The usual reason for inadequate tissue oxygenation is local vasoconstriction as a result of sympathetic overactivity. This may occur because of blood volume deficit, unrelieved pain, or hypothermia, especially involving the distal extent of the extremities.
Ensure adequate nutrition
Adequate nutrition is an often-overlooked requirement for normal wound healing.[23] Address protein-calorie malnutrition and deficiencies of vitamins and minerals.
Inadequate protein-calorie nutrition, even after just a few days of starvation, can impair normal wound-healing mechanisms. For healthy adults, daily nutritional requirements are approximately 1.25-1.5 g of protein per kilogram of body weight and 30-35 calories/kg. Increase these requirements for those with sizable wounds.
11

Suspect malnutrition in patients with chronic illnesses, inadequate societal support, multisystemic trauma, or GI or neurologic problems that may impair oral intake. Protein deficiency occurs in approximately 25% of all hospitalized patients.
Chronic malnutrition can be diagnosed by using anthropometric data to compare actual and ideal body weights and by observing low serum albumin levels. Serum prealbumin is sensitive for relatively acute malnutrition because its half-life is 2-3 days (vs 21 d for albumin). A serum prealbumin level of less than 7 g/dL suggests severe protein-calorie malnutrition.
Vitamin and mineral deficiencies also require correction. Vitamin A deficiency reduces fibronectin on the wound surface, reducing cell chemotaxis, adhesion, and tissue repair. Vitamin C is required for the hydroxylation of proline and subsequent collagen synthesis.
Vitamin E, a fat-soluble antioxidant, accumulates in cell membranes, where it protects polyunsaturated fatty acids from oxidation by free radicals, stabilizes lysosomes, and inhibits collagen synthesis. Vitamin E inhibits prostaglandin synthesis by interfering with phospholipase-A2 activity and is therefore anti-inflammatory. Vitamin E supplementation may decrease scar formation.
Zinc is a component of approximately 200 enzymes in the human body, including DNA polymerase, which is required for cell proliferation, and superoxide dismutase, which scavenges superoxide radicals produced by leukocytes during debridement.
Treat infection
Issues to consider are wound infection versus colonization and osteomyelitis.[24]
A positive wound culture does not confirm a wound infection. Opportunistic microorganisms may colonize any wound. Wound exudate, which is naturally bactericidal, inhibits the spread of surface contamination from becoming a deep wound infection. However, when wound ischemia or systemic immune compromise supervenes, pathogenic microorganisms propagate until an excessive concentration of bacteria in the wound precludes healing. This heralds a true wound infection. Multidrug resistant organisms are becoming increasingly common.
Foul-smelling drainage, a spontaneously bleeding wound bed, flimsy friable tissue, increased levels of wound exudate, increasing pain, surrounding cellulitis, crepitus, necrosis, fasciitis, and regional lymphadenopathy characterize the infected wound. Fever, chills, malaise, leukocytosis, and an elevated erythrocyte sedimentation rate are common systemic manifestations of wound infection.
Wound infection requires surgical debridement and appropriate systemic antibiotic therapy. Topical antiseptics are usually avoided because they interfere with wound healing because of cytotoxicity to healing cells.
Proving the absence of osteomyelitis is often as onerous as establishing its presence. Although osteomyelitis may be associated with fevers, malaise, chronic fatigue, and
12

limited range of motion of the affected extremity, patients often present with only a nonhealing wound or a chronic draining sinus tract overlying a bone or joint.
Plain radiographs, CT scans, radionuclide bone scans, and MRIs have a role in the workup of osteomyelitis. All too often, even a comprehensive imaging evaluation is nondiagnostic. Therefore, negative findings on radiologic workup should not deter the clinician from performing curettage of suspicious bone underlying a chronic draining wound.
Osteomyelitis is treated with surgical curettage and appropriate systemic antibiotics. Provide a wound bed that is conducive to wound healing.
Surgically debride nonvitalized tissue and with appropriate irrigation. Significant amounts of nonviable and fibropurulent tissue must be removed surgically.
Initial aggressive debridement in the operating room with the patient under local anesthesia with sedation or under regional or general anesthesia is often wise. Subsequent debridement in an outpatient setting can be performed by using topical lidocaine gel or spray anesthesia and by gentle excision using iris scissors and forceps or by scraping using a curette.
Dressing changes require clean but not necessarily sterile technique.
Remove foreign bodies
Be attentive to the possibility of foreign bodies, which may prevent healing of traumatic wounds, including road debris and retained fragments of dressing materials or suture material.
Irrigate
Gently irrigate the wound with a physiologic saline solution. If cost is a major consideration, the patient can prepare a saline solution at home by using 1 gallon of distilled water and 8 teaspoons of table salt. The solution is boiled and then cooled to room temperature before use.
If surface exudate is present, consider irrigation under pressure. An irrigation pressure of approximately 8 psi can be achieved with saline forced through a 19-gauge angiocatheter with a 35-mL syringe. Pat the wound surface with soft moist gauze; do not disrupt viable granulation tissue.
Whirlpool treatment is reserved for large and infected wounds.
Provide a moist (not wet) wound bed
After debridement, apply a moist saline dressing, an isotonic sodium chloride gel (eg, Normlgel [Scott Health Care], IntraSite gel), or a hydroactive paste (eg, DuoDerm [ConvaTec]). Optimal wound coverage requires wet-to-damp dressings, which support autolytic debridement, absorb exudate, and protect surrounding normal skin.
13

A polyvinyl film dressing (eg, OpSite [Smith & Nephew], Tegaderm [3M]), which is semipermeable to oxygen and moisture and impermeable to bacteria, is a good choice for wounds that are neither dry nor highly exudative.
For dry wounds, hydrocolloid dressings, such as DuoDerm or IntraSite hydrocolloid, are impermeable to oxygen, moisture, and bacteria. They maintain a moist environment, and they support autolytic debridement. They are a good choice for relatively desiccated wounds.
For exudative wounds, absorptive dressings, such as calcium alginates (eg, Kaltostat [Calgon Vestal], Curasorb [Kendall]) and hydrofiber dressings (eg, Aquacel and Aquacel-AG [Convatec]), are highly absorptive and are appropriate for exudative wounds. Alginates are available in rope form, which is useful for packing deep wounds.
For very exudative wounds, impregnated gauze dressings, such as Mesalt (Scott), are useful. Twice-daily dressing changes may be needed.
For infected wounds, use silver sulfadiazine (Silvadene) if the patient is not allergic to sulfa drugs. If the patient is allergic to sulfa, bacitracin-zinc ointment is a good alternative. An ionic-silver hydrofiber dressing (Aquacel-AG) is also a good choice.[25, 26, 27,
28, 29]
Bandaging a challenging anatomic area (eg, around a heel ulcer) requires a highly conformable dressing, such as an extra-thin hydrocolloid. Securing a dressing in a highly moist challenging site (eg, around a sacrococcygeal ulcer) requires a conformable and highly adherent dressing, such as a wafer hydrocolloid.
Hydrogel sheets and nonadhesive forms are useful for securing a wound dressing when the surrounding skin is fragile.
Table 1. Characteristics and Uses of Wound-Dressing Materials
Category Examples Description Applications
Alginate AlgiSite, Comfeel, Curasorb, Kaltogel, Kaltostat, Sorbsan, Tegagel
Alginate dressings are made of seaweed extract contains guluronic and mannuronic acids that provide tensile strength and calcium and sodium alginates, which confer an absorptive capacity. Some can leave fibers in the wound if they are not thoroughly irrigated. These dressings are secured with secondary coverage.
These dressings are highly absorbent and useful for wounds have copious exudate. Alginate rope is particularly useful to pack exudative wound cavities or sinus tracts.
Hydrofiber Aquacel, An absorptive textile fiber pad, Hydrofiber absorbent
14

Aquacel-Ag, Versiva
hydrofiber is also available as a ribbon for packing of deep wounds. This material is covered with a secondary dressing. The hydrofiber combines with wound exudate to produce a hydrophilic gel. Aquacel-Ag contains 1.2% ionic silver that has strong antimicrobial properties against many organisms, including methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci.
dressings used for exudative wounds.
Debriding agents
Hypergel (hypertonic saline gel), Santyl (collagenase), Accuzyme (papain urea)
Various products provide some chemical or enzymatic debridement.
Debriding agents are useful for necrotic wounds as an adjunct to surgical debridement.
Foam LYOfoam, Spyrosorb, Allevyn
Polyurethane foam has absorptive capacity.
These dressings are useful for cleaning granulating wounds with minimal exudate.
Hydrocolloid CombiDERM, Comfeel, DuoDerm CGF Extra Thin, Granuflex, Tegasorb
Hydrocolloid dressings are made of microgranular suspension of natural or synthetic polymers, such as gelatin or pectin, in an adhesive matrix. The granules change from a semihydrated state to a gel as the wound exudate is absorbed.
Hydrocolloid dressings are useful for dry necrotic wounds, wounds with minimal exudate and for clean granulating wounds.
Hydrogel Aquasorb, DuoDerm, Intrasite Gel, Granugel, Normlgel, Nu-
Hydrogel dressings are water-based or glycerin-based semipermeable hydrophilic polymers; cooling properties may decrease wound pain. These gels can lose or absorb
These dressings are useful for dry, sloughy, necrotic wounds (eschar).
15

Gel, Purilon Gel, KY Jelly
water depending upon the state of hydration of the wound. They are secured with secondary covering.
Low-adherence dressing
Mepore, Skintact, Release
Low-adherence dressings are made of various materials designed to remove easily without damaging underlying skin.
These dressings are useful for acute minor wounds, such as skin tears, or as a final dressing for chronic wounds that have nearly healed.
Transparent film
OpSite, Skintact, Release, Tegaderm, Bioclusive
Transparent films are highly conformable acrylic adhesive films with no absorptive capacity and little hydrating ability. They may be vapor permeable or perforated.
These dressings are useful for clean, dry wounds with minimal exudate. They also are used to secure an underlying absorptive material, to protect high-friction areas and areas that are difficult to bandage (eg, heels) and to secure intravenous catheters.
Consider other topical agents
Topically applied platelet-derived growth factors have a modestly beneficial effect in promoting wound healing. Becaplermin gel 0.01% (Regranex), recombinant human platelet-derived growth factor (PDGF) that is produced through genetic engineering, is approved by the US Food and Drug Administration (FDA) to promote healing of diabetic foot ulcers. Regranex is contraindicated in persons with known skin cancers at the site of application. Freeze-dried, platelet-rich plasma showed promise in an animal study.[30]
Collagen comprises a significant fraction of the necrotic soft tissues in chronic wounds. The enzyme collagenase, which is derived form fermentation of Clostridium histolyticum, helps remove nonviable tissue from the surface of wounds. However, collagenase is not a substitute for an initial surgical excision of a grossly necrotic wound.
16

Other topical agents that have been used for wound treatment are sugar, antacids, and vitamin A&D ointment.
Avoid cytotoxic agents, such as hydrogen peroxide, povidone iodine, acetic acid, and Dakin solution (sodium hypochlorite).
Consider compression therapy
Consider the advisability of compression therapy. Compression is appropriate for ulcers caused or exacerbated by extremity edema. Compression may have to be avoided entirely in the presence of significant arterial inflow compromise.
Use support hose or elastic wraps with approximately 40-60 mm Hg of pressure in the absence of arterial disease and 20-30 mm Hg in the presence or suspicion of mild arterial insufficiency.
Manage pain
Manage wound pain by moistening dressings before removal. Consider using 2% topical lidocaine gel during wound care. (Anecdotal reports describe the use of topical morphine and diamorphine-infused gel for palliation of pressure ulcer pain in patients who are terminally ill,[31] but this use is not FDA approved.)
Treatment of specific types of wounds can be described as follows:
See General treatment of nonhealing wounds.
Pressure ulcers
Treatment of decubitus ulcers requires prolonged surgical and nursing care.[32, 33, 34,
35] During the extended period of treatment required, the patient remains at risk for the development of new pressure ulcers at other sites.[36, 37, 38] Treatment, particularly indications for support surfaces, is based on appropriate staging of the pressure ulcer.[39,
40]
Milne et al reported the outcome of a long-term acute care hospital's program to reduce the incidence of pressure ulcers.[41] The facility used a failure mode and effects analysis to determine where improvements in care were most needed. The hospital determined that its ulcer prevalence rates, which were believed to be above average, were associated with such problems as "a lack of 1) wound care professionals, 2) methods to consistently document prevention and wound data, and 3) an interdisciplinary wound care team approach." After the hospital addressed these issues, it saw the incidence of facility-acquired pressure ulcers drop from 41% (the baseline figure) to an average of 4.2%, over a 12-month period.
Table 2. Staging Pressure Ulcers
17

Stage Definition AppearanceAppropriate topical treatment
Average healing time (d)
I Nonblanchable erythema of intact skin
Pink skin that does not resolve when pressure is relieved; discoloration; warmth; induration
DuoDerm q2-3d 14
II Partial-thickness skin loss involving epidermis and/or dermis
Cracking, blistering, shallow crater, abrasion
Cleanse with saline; DuoDerm/Tegaderm dressing
45
III Full-thickness skin loss into subcutaneous fatty tissues or fascia
Distinct ulcer margin; deep crater (in general, 2.075 mm or deeper [the thickness of a nickel])
Debride; irrigate with saline; apply DuoDerm/Tegaderm
90
IV Full-thickness skin loss with extensive tissue involvement of underlying tissues
Extensive necrosis; damage to underlying supporting structures, such as muscle, bone, tendon, or joint capsule
Surgically debride; irrigate with saline (possibly under pressure); apply advanced topical dressings; consider antibiotics
120
*When the overlying skin is necrotic, the staging cannot be accurate until debridement is performed.
Pressure ulcers often require the following steps:
Debridement: The ulcer often requires surgical excision, usually down to underlying bone. In the absence of erythema, edema, fluctuance, or drainage, clean dry eschar does not need to be debrided surgically but may be softened and allowed to separate using dressings (eg, colloids, hydrogels) that provide a moist environment to encourage autolysis.
18

Topical wound care: Weeks or months of daily dressing changes are required before the wound begins granulating and appears clean enough for myocutaneous flap closure.
Treatment of infection: Debridement is a clean, not sterile, procedure. Frequent debridements maintain superficial colonization at acceptable levels. Swab cultures are often meaningless because they reflect only surface colonization of local infection, which does not require antibiotic treatment. In general, systemic antibiotics are not useful unless signs of progressive infection, such as bacteremia, septicemia, progressive cellulitis, or intractable osteomyelitis, are present.
Control of chronic wound contamination: Chronic wound contamination because of fecal incontinence can be a vexing problem in typical bedridden patients, who tend to develop sacral and ischial pressure ulcers. These types of ulcers are depicted in the images below. Initial treatment is dietary management. Foods that thicken the stool include applesauce, bananas, boiled milk, bread, cheese, creamy peanut butter, grits, oat bran, oatmeal, pasta, pretzels, rice, tapioca, and yogurt. In rare cases, fecal diversion by means of colostomy is required.
Image of advanced sacral pressure ulcer shows the effects of pressure, shearing, and moisture.
Sacral pressure ulcer before and after flap closure.
Sacral ulcer.
19

Positioning: Patients with pressure ulcers or those at risk for a pressure ulcer should be turned in bed every 2 hours. Patients who are immobile should not be positioned directly on the trochanters; foam wedges and pillows are useful to pad pressure points, to prevent direct contact between bony prominences, and to raise their heels off the bed surface. Pressure ulcers can also be induced by shear forces if patients slide down the bed; therefore, try to use the lowest degree of elevation of the head of the bed that the patient's medical conditions allow.
Use of support surfaces
Support surfaces are further discussed as follows:
Federal regulations (Medicare Bulletin 405) dictate that patients with bedsores or those who are at risk for bedsores must be placed on an appropriate support surface.
Federally mandated standards of care dictate what support surfaces are allowable and provide for both civil and criminal penalties for health care entities that fail to comply.
Proper prevention and management of pressure ulcers in health care facilities is mandated by federal regulations (Ch IV § 483.25 (c)(1)&(2), 10/1/95), which state, "Based on the comprehensive assessment of a resident, the facility must ensure that (1) a resident who enters the facility without pressure sores does not develop pressure sores unless the individual's clinical condition demonstrates that they were unavoidable, and (2) a resident having pressure sores receives necessary treatment and services to promote healing, prevent infection and prevent new sores from developing."
A class I support surface is a simple pressure pad device that is required as follows:o For patients who cannot independently change their body position to effectively
alleviate pressureo For patients who have any stage of pressure ulcer on the trunk or pelvis, plus
impaired nutritional status, fecal or urinary incontinence, altered sensory perception, or compromised circulatory status
A class II support surface is a pressure-relieving device that reduces pressure over bony prominences to less than 32 mm Hg and that does so for a sustained period. A class II support surface is required as follows:
o For patients who have multiple pressure ulcers on the trunk or pelvis that has not improved despite a comprehensive treatment, including a class I support surface for a stage II, III, or IV pressure ulcer for at least 1 month
o For patients who have large or multiple stage III or IV pressure ulcers on the trunk or pelvis
o For patients who have had a myocutaneous flap or skin graft procedure for a pressure ulcer on the trunk or pelvis within the past 60 days and have been on a class II or III support surface immediately before a recent discharge from a hospital or nursing facility within the past 30 days
A class III support surface is an advanced pressure-relieving device. A class III support surface, that is, an air-fluidized bed, may be used only for failure of a comprehensive conservative treatment plan after 30 days. (Note that an air-fluidized bed is contraindicated for any patient with associated severe pulmonary compromise because the absence of firm back support makes coughing ineffective, and the dry air
20

thickens pulmonary secretions.) Such a conservative treatment program includes the following:
o Education of the patient and the caregiver. A patient information page regarding pressure ulcers is available.[34]
o Assessment by a licensed health care practitioner, at least weeklyo Appropriate turning and positioningo Use of a class II support surfaceo Appropriate wound careo Appropriate management of incontinenceo Appropriate nutritional management
Table 3. Support Surfaces
Class Type Principle Examples
I Simple Pressure-relieving pad or mat 3- to 5-inch foam mattress, gel overlay, egg-crate mattress
II Advanced Powered air* overlay for mattress with low air loss feature; nonpowered advanced pressure-reducing mattress replacement or powered air* floatation bed with or without low air loss feature
Roho dry floatation mattress system, Pegasus Renaissance mattress
III Air fluidized
Floatation by filtered air* flow pumped through porcelain beads
Clinitron bed
*Long-term use of powered air devices is relatively contraindicated for patients with chronic obstructive lung disease, such as chronic bronchitis, emphysema, and asthma.
Additional protection is described as follows:
Proper off-loading for ischial ulcers: Sacral ulcers usually result from prolonged supine bed rest or from shearing forces, particularly because of the patient sliding down the bed when the head is elevated. On the other hand, ischial ulcers often result from prolonged sitting either in the head-up position in the bed or in a wheelchair. Hence, off-loading for ischial ulcer prevention and treatment requires support surfaces for sitting as well as mattress support surfaces. Sitting time must also be limited.
Heel protection: Pressure ulcers involving the heel regions commonly occur in patients who are bedridden, even if they are immobilized for just a few days, such as after hip surgery. A heel pressure ulcer is illustrated in the image below. Prevention and
21

treatment of heel pressure ulcers requires off-loading. Off-loading devices are usually selected based on availability and include the following:
Heel pressure ulcer.
o Booties are simple pressure pads that surround the heel with polyester fibers, iconized fibers, or foam material.
o Boots are made from a firm outer shell lined with pressure-relief padding. They can also provide positioning capability to help treat contractures and foot drop.
o Pillows made from polyester and sheepskin fleece or special rubber or plastic interpose a conformable soft overlay between the heel and the mattress.
o Suspension devices isolate the heel and transfer the weight to the lower leg. These devices also have positioning capabilities that are useful in treating contractures and foot drop.
o Inflatable devices made from plastic sheets surround the heel and adjacent tissues.
Venous ulcers
Treatment of venous ulcers includes compression therapy, providing a moist wound environment and debridement of necrotic tissue.[42, 43] Most venous ulcers heal with these measures alone. Some require split-thickness skin grafting or application of bioengineered skin (eg, Apligraf, Dermagraft).[44]Pentoxifylline (Trental) and horse chestnut seed (available in supermarkets and health food specialty stores) have been shown to expedite healing of venous stasis ulcers. In some cases, compression therapy is inadequate to maintain healing of venous ulcers, and surgical vein stripping or ligation of venous perforators may be helpful.
A study of 98 limbs with active chronic venous ulcers revealed that all but one had venous reflux; the study also suggested that most of these patients would benefit from surgical or endovascular intervention.[45] Other studies suggested a more modest level of benefit from corrective venous surgery.[46]
22

Table 4. Compression Bandages for Venous Ulcers*
Type Description Examples
Single layer Single-layer simple tubular woven nylon/elastic bandages may be imprinted with rectangles that stretch to squares when appropriate wrapping tension (30-40 mm Hg) is applied.
ACE bandage, Comperm (Conco Medical), Setopress (Seton Healthcare Group)
Three layer The layers include a padding absorption layer, a compression bandage layer, and a cohesive compression bandage. Bandages may be left in place for up to 1 week depending on wound exudate.
Dyna-Flex (Johnson & Johnson)
Four layer The layers include a nonwoven wound contact layer that is permeable to wound exudate and 4 overlying bandages. Bandages may be left in place for up to 1 week depending on exudate volume.
Profore (Smith & Nephew)
Impregnated wrap
The porous flexible occlusive dressing is composed of stretchable gauze and a nonhardening zinc oxide paste.
Unna boot (ConvaTec)
*Compression wraps are contraindicated in severe arterial compromise. Some of these products are contraindicated in patients who are allergic to latex.
Diabetic foot ulcers
The treatment of diabetic foot ulcers requires the following: (1) appropriate therapeutic footwear, (2) daily saline or similar dressings to provide a moist wound environment, (3) debridement when necessary, (4) antibiotic therapy if osteomyelitis is present, (5) optimal control of blood glucose, and (6) evaluation and correction of peripheral arterial insufficiency.[47, 48, 49, 50, 51]See also Diabetic Ulcers.
Wound coverage with cultured human cells or heterogeneic dressings and/or grafts, application of recombinant growth factors, negative pressure wound therapy, and hyperbaric oxygen treatments may also be beneficial.[17, 52, 53, 54]
Lymphedema
Although lymphedema is not typically a cause of ulceration, ulcers on the extremities may fail to heal because of untreated lymphedema. Nocturnal leg elevation and elastic wraps or support hose are appropriate adjuncts to the treatment of the recalcitrant
23

wound in an edematous extremity. For advanced and nonresponsive lymphedema, complex decongestive physiotherapy is a useful treatment option.
Surgical Therapy
Methods are available to expedite healing of the clean wound. After a wound is in a steady clean state, a decision must be made about allowing it to heal by natural processes or expediting healing with a surgical procedure. Clinical experience and observation of the healing progress in the individual case dictate the appropriate treatment. Surgical options include skin grafting, application of bioengineered skin substitutes, and use of flap closures.[55]
Skin grafting: Autologous skin grafting is the criterion standard for viable coverage of partial-thickness wounds. The graft can be harvested with the patient under local anesthesia in an outpatient procedure. Meshing the graft allows wider coverage and promotes drainage of serum and blood.
Cadaveric allografting: A cadaveric skin allograft is a useful covering for relatively deep wounds after surgical excision when the wound bed does not appear appropriate for application of an autologous skin graft. The allograft is only a temporary solution.
Application of bioengineered skin substitutes[50, 56, 57]
o Apligraf (Organogenesis; Novartis) is a bilayered skin substitute produced by combining bovine collagen and living cells derived from tissue-cultured human infant foreskins. One study of diabetic foot ulcers demonstrated 12-week healing rates of 39% for patients who received only standard wound care versus 56% for those who were treated by application of an Apligraf after a period of standard wound care.
o Dermagraft (Smith & Nephew, Inc) is human fibroblast-derived dermal substitute manufactured by seeding dermal fibroblasts onto a 3-dimensional bioabsorbable scaffold. It has been marketed for use in the treatment of diabetic foot ulcers, venous ulcers, and pressure sores. A clinical trial showed improved healing rates in diabetic foot ulcers.
o Oasis (Healthpoint, Ltd), a relatively new product, is a xenogeneic acellular collagen matrix derived from porcine small intestinal submucosa in such a way that an extracellular matrix and natural growth factors remain intact. This provides a scaffold for inducing wound healing.[58] Do not use this in patients with allergies to porcine materials.
o Cultured epithelial autograft (Epicel; Genzyme Tissue Repair, Cambridge, Mass) is an epidermal replacement that is grown in a tissue culture from a skin biopsy taken from the recipient and is cocultured with mouse cells. Preparation of the graft requires about 2 weeks of culture time.
Use of flap closures: Delayed primary closure of a chronic wound, as shown below, requires well-vascularized clean tissues and tension-free apposition. This usually requires undermining and mobilization of adjacent tissue planes by creating skin flaps or myocutaneous flaps.[59]
24

Image of advanced sacral pressure ulcer shows the effects of pressure, shearing, and moisture.
Sacral pressure ulcer before and after flap closure.
Complications
Complications of nonhealing wounds include the following:
Amyloidosis - See Amyloidosis, Macular. Bacteremia - See Shock, Septic. Cellulitis Endocarditis Heterotopic bone formation Maggot infestation Meningitis Osteomyelitis Perineal-urethral fistula Pseudoaneurysm - See Peripheral Vascular Injuries. Septic arthritis Sinus tract or abscess Squamous Cell Carcinoma
Outcome and Prognosis
The prognosis for healing of chronic wounds varies with the etiology of the wound and the general health status of the patient.
Future and Controversies
The aging of the population and continued advances in biotechnology drive the wound care industry, estimated at $10 billion globally. Besides the always-improving synthetic dressing materials, newer technologies in wound treatment include the xenogeneic tissue scaffold, bilayered human dermal substitutes, recombinant growth factors,
25

endoscopic subfascial ligation of venous perforators, and endovascular arterial repair techniques. The use of hyperbaric oxygen therapy and electrical stimulation remain controversial.
26