Embed Size (px)
Citation preview

T x plasma g ndii

Outlines• Taxonomy• Prevalence • Clinical importance• Morphology• Life cycle• Prevention of infection• Diagnosis• Treatment

Taxonomy
Ctenodactylus gondi
Phylum: Apicomplixa Class: SporozoaDefinitive host: catsIntermediate host: almost any mammal Prevalence: one third of the world populationDisease: toxoplasmosis



• Acute disease in adults:• the majority are asymptomatic
or unrecognized.
Clinical Importance

• Immunocompromised Patients:
• Most frequently results from reactivation of latent infection
• it can cause serious pathology including: hepatitis, pneumonia, blindness, myocarditis• the central nervous system is primarily involved
with diffuse encephalopathy, meningoencephalitis or cerebral mass lesions. Toxoplasma encephalitis has been reported as a life-threatening among patients with AIDS.
Clinical Importance

• Congenital Toxoplasmosis:• Total maternal-fetal transmission is about 30% throughout all of
gestation, but varies from 6% at 13 weeks to 72% at 36 weeks• If the fetus is exposed during the first trimester, death nearly
always occurs as a result of CNS damage.• Infection during the second trimester may result in hydrocephaly,
blindness, or other nervous system damage.• Later infection may result in blindness or mild CNS defects.• However, women who are exposed to this parasite before
pregnancy do not transmit the infection to the fetus.
Clinical Importance


- Ocular disease (toxoplasmic retinochoroiditis)
• the most common sequelae of congenital toxoplasmosis
• up to 2% of adults newly infected with T. gondii develop ocular lesions
Clinical Importance

Morphology
Tachyzoites, trophozoites,or endozoites
orCystozoite

MorphologyTachyzoites
orCystozoite
oocystSporulatedoocyst
Bradyzoites within
tissue cyst
Tachyzoites

Tachyzoites vs bradyzoites
Tachyzoites rapidly dividing stage seen in body fluids in early,
acute infection directly destroy cells,
particularly parenchymal and reticuloendothelial cells
Bradyzoites slowly dividing stage contained in cysts in muscle
and brain tissue and in the eye Released from ruptured tissue
cysts cause local inflammation with blockage of blood vessels and necrosis


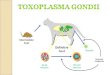
Life cycle
sexual asexual
• Intestinal (enteroepithelial) phases
• occurs in cats only (wild as well as domesticated cats)
• produces "oocysts."
• Extraintestinal phases• occurs in all infected
animals (including cats)• produces "tachyzoites"
and,eventually,"bradyzites“ or "zoitocysts."


Prevention measures Action situation
Wash hands carefully after stroking a catWear gloves when changing cat litterChange litter frequently and wash the tray with hot water (> 60° C)Avoid litter in the kitchen
Cat contact
Cook the meat well-done or stewAvoid microwave cooking for meatAvoid raw vegetables at restaurantsAvoid raw shellfishAvoid raw goat milk
Meals
Wash vegetables, fruits and herbs thoroughly, especially if they grow close to the groundWash hands, knives, any containers and table thoroughly after meat manipulation or cutting
Preparation of meals
Prefer mineral water to tap water WaterWash hands thoroughly and brush nails after any outdoor activities in contact with soilWear gloves for gardeningAvoid ingestion of water during recreation activities in lakes or rivers
Gardening or outdoor activities
Prevention of Toxoplasma infection

control
• It is difficult to control toxoplasmosis because of wide range of animal reservoirs.
• Currently, there is no effective vaccine available for humans.
• A genetically engineered vaccine is under development for use in cats.


Microscopy
• Tachyzoites and tissue cysts can be detected• Specimens: blood, sputum, bone marrow aspirate, cerebrospinal
fluid (CSF), aminiotic fluid, and biopsy material from lymphnode, spleen, and brain.
Smear made from above specimens is stained by: Giemsa, PAS, or Gomori methanamine silver (GMS) stain
Tachyzoites or cyst can also be demonstrated effectively by fluroscent conjugated antibody technique in tissue biopsy or impression smear.
Presence of only tissue cysts does not differentiate between active and chronic infection.
The presence of cysts in placenta or tissues of newborn establishes congenital toxoplasma infection.

SerodiagnosisAntibody detectionDiagnosis of acute infection with T. gondii can be made by detection of the simultaneous presence of IgM and IgG antibodies. Tests for detecting IgG antibody include:o Enzyme-linked immunosorbent assay (ELISA)o Indirect fluorescent antibody test (IFAT)o Latex agglutination testo Sabin-Feldman dye test. Positive IgG can be detected as early as 2–3 weeks after infection. Peak level of antibody is observed in blood 4–8 weeks after infection. Positive IgM antibody titer indicates an early primary infection. The serum IgM
titer can be measured by:o sandwich IgM ELISAo IgM immunosorbent assay (IgM-ISAGA). Both assays are equally specific and sensitive. Negative IgM titer and positive IgG titer indicate distant infection. Sandwich IgA-ELISA test is used for detecting congenital infection in newborns.

SerodiagnosisAntigen detection
Detection of antigen by ELISA indicates recent Toxoplasma infection.In AIDS and other immunocompromised
patients, antigen detection is very useful.Detection of antigen in amniotic fluid is helpful to
diagnose congenital toxoplasmosis.

Molecular Methods
• DNA hybridization techniques and polymerase chain reaction (PCR) are increasingly used to detect Toxoplasma from different tissues and body fluids.
B1 gene of T. gondii can be detected by PCR of the amniotic fluid in case of congenital toxoplasmosis

Imaging
• Magnetic resonance imaging (MRI) and computed tomography (CT) scan are used to diagnose toxoplasmosis with central nervous system involvement.
Ultrasonography (USG) of the fetus in utero at 20–24 weeks of pregnancy is useful for diagnosis of congenital toxoplasmosis.

Animal Inoculation• Toxoplasma can be isolated
by inoculating body fluids, blood, or tissue specimens by intraperitoneal inoculation in mice or in tissue culture. • Mice should be examined for
Toxoplasma in their peritoneal exudate after 7–10 days of inoculation.

Skin test of Frenkel• Diluted toxoplasmin is injected intradermally and
delayed positive reaction appears after 48 hours. • This test is not very reliable for diagnosis

Treatment Congenital Toxoplasmosis:• Oral pyrimethamine (1 mg/kg) daily and sulfadiazine (100 mg/ kg) with folinic acid for 1
year. Systemic corticostoriod may be added to reduce chorioretinitis.
Immunocompetent Patientswho have only lymphadenopathy, do not require specific therapy unless they have persistent, severe symptoms.• Patients with ocular toxoplasmosis are treated for 1 month with pyrimethamine plus
either sulfadiazine or clindamycin
Immunocompromised PatientsAIDS patients who are seropositive for T. gondii and have a CD4+ Tlymphocytecount below <100/μL, should receive primary prophylaxis against toxoplasma encephalitis. Trimethoprimsulfamethoxazole is the drug of choice. If trimethoprimsulfamethoxazole
cannot be tolerated by patients, dapsonepyrimethamine is the recommended alternative drug of choice.
Prophylaxis against toxoplasma encephalitis should be discontionued in patients who have responded to antiretroviral therapy (ART) and whose CD4+ T lymphocyte count has been above 200/μL for 3 months.

References
MEDICAL AND CLINICAL LABORATORY PROFESSIONALS- John W. Ridley, Ph.D.
DIAGNOSING MEDICAL PARASITES- A Public Health Officers Guide to Assisting Laboratory and Medical Officers
MICROBIOLOGY DEMYSTIFIED- TOM BETSY, D.C.JIM KEOGH Lippincott’s Illustrated Reviews: Microbiology Third Edition Chapter 14 Toxoplasmosis: A Widespread Zoonosis Diversely
Affecting Humans and Animals-Florence Robert-Gangneux, Dominique Aubert and Isabelle Villena
Paniker’s Textbook of Medical Parasitology-SEVEnth EDition

THANK YOU






![Research Article Toxoplasma gondii Pave the Road for Dementia?downloads.hindawi.com/journals/jpr/2020/8859857.pdf · including Toxoplasma gondii (T. gondii) [6], Herpes simplex virus-1](https://img.pdfslide.us/doc/110x75/5f9376ed91220772b35c9b7d/research-article-toxoplasma-gondii-pave-the-road-for-dementia-including-toxoplasma.jpg)



![Primerdesign Ltd TM Toxoplasma gondii - Home : genesig · Toxoplasma gondii is a species of parasitic protozoa in the genus Toxoplasma.[1] The definitivehostofT.gondiiisthecat,buttheparasitecanbecarriedbythevastmajorityof](https://img.pdfslide.us/doc/110x75/5cc21bb288c993ed078d60da/primerdesign-ltd-tm-toxoplasma-gondii-home-toxoplasma-gondii-is-a-species.jpg)





![Toxoplasma gondii - PCRmax · Toxoplasma gondii is a species of parasitic protozoa in the genus Toxoplasma.[1] The definitive host of T. gondii is the cat, but the parasite can be](https://img.pdfslide.us/doc/110x75/5cc21bb288c993ed078d60e8/toxoplasma-gondii-toxoplasma-gondii-is-a-species-of-parasitic-protozoa-in.jpg)