Embed Size (px)
DESCRIPTION
Jan. 4th, 2012
Citation preview

The diseases of the knee jointThe diseases of the knee joint

Anatomy of the knee Anatomy of the knee
Joints: there are two joints in the Joints: there are two joints in the knee: knee: – Patellofemoral joint Patellofemoral joint – Tibiofemoral joint (the joint that is Tibiofemoral joint (the joint that is
usually referred to as 'the knee joint')usually referred to as 'the knee joint')

Anatomy of the kneeAnatomy of the knee
Patella: the patellar tendon (also Patella: the patellar tendon (also called patellar ligament) passes called patellar ligament) passes anteriorly to the patella. anteriorly to the patella.

Ligaments: stability to the Ligaments: stability to the tibiofemoral joint is provided by tibiofemoral joint is provided by various ligaments:various ligaments:
Anatomy of the kneeAnatomy of the knee

Anatomy of the kneeAnatomy of the knee
Anterior cruciate ligament (ACL) - Anterior cruciate ligament (ACL) - controls rotational movement and controls rotational movement and prevents forward movement of the prevents forward movement of the tibia in relation to the femur. Runs tibia in relation to the femur. Runs between attachments on the front between attachments on the front (hence anterior cruciate) of the tibial (hence anterior cruciate) of the tibial plateau and the posterolateral aspect plateau and the posterolateral aspect of the intercondylar notch of the of the intercondylar notch of the femur femur

Anatomy of the kneeAnatomy of the knee
Posterior cruciate ligament (PCL) - Posterior cruciate ligament (PCL) - prevents forward sliding of the femur prevents forward sliding of the femur in relation to the tibial plateau. Runs in relation to the tibial plateau. Runs between attachments on the between attachments on the posterior part (hence posterior posterior part (hence posterior cruciate) of the tibial plateau and the cruciate) of the tibial plateau and the medial aspect of the intercondylar medial aspect of the intercondylar notch of the femur. notch of the femur.

Anatomy of the kneeAnatomy of the knee
Medial collateral ligament - prevents Medial collateral ligament - prevents lateral movement of the tibia on the lateral movement of the tibia on the femur when valgus (away from the femur when valgus (away from the midline) stress is placed on the knee. midline) stress is placed on the knee. Runs between medial epicondyle of Runs between medial epicondyle of the femur and the anteromedial the femur and the anteromedial aspect of the tibia. Also has a deep aspect of the tibia. Also has a deep attachment to the medial meniscus attachment to the medial meniscus

Anatomy of the kneeAnatomy of the knee
Lateral collateral ligament - prevents Lateral collateral ligament - prevents medial movement of the tibia on the medial movement of the tibia on the femur when varus (towards the femur when varus (towards the midline) stress is placed on the knee. midline) stress is placed on the knee. Runs between lateral epicondyle of Runs between lateral epicondyle of the femur and head of the fibula. the femur and head of the fibula.

Menisci: the medial and lateral Menisci: the medial and lateral menisci are located within the knee menisci are located within the knee joint, attached to the tibial plateau. joint, attached to the tibial plateau. They help to protect the articular They help to protect the articular surfaces by absorbing some of the surfaces by absorbing some of the forces transmitted through the knee. forces transmitted through the knee. They also help to stabilise and They also help to stabilise and lubricate the knee. lubricate the knee.
Anatomy of the kneeAnatomy of the knee

Anatomy of the kneeAnatomy of the knee

Anatomy of the kneeAnatomy of the knee

History History
Was onset of pain gradual or acute? Was onset of pain gradual or acute? OA comes on over years; ACL injuries OA comes on over years; ACL injuries cause immediate pain.cause immediate pain.
If acute, was there trauma? If acute, was there trauma?

HistoryHistory
If there was trauma, what exactly If there was trauma, what exactly happened? If injury occurred in sport happened? If injury occurred in sport or an accident get a precise history or an accident get a precise history of the mechanism. Was there a direct of the mechanism. Was there a direct blow causing vulgus or varus stress? blow causing vulgus or varus stress? Was there a twisting motion? Was there a twisting motion?

HistoryHistory
Figure 2Figure 2
Figure 3Figure 3
Figure 1Figure 1
Figure 5Figure 5

HistoryHistoryWas there any sound? A 'popping' or Was there any sound? A 'popping' or 'snapping' sound may suggest rupture of a 'snapping' sound may suggest rupture of a ligament. ligament.
Did the knee swell immediately, gradually, Did the knee swell immediately, gradually, or not at all? Rapid swelling (0-2 hours) or not at all? Rapid swelling (0-2 hours) suggests suggests haemarthrosishaemarthrosis which may be due which may be due to e.g. ACL or PCL rupture, patellar to e.g. ACL or PCL rupture, patellar dislocation. Gradual swelling (6-24 hours) dislocation. Gradual swelling (6-24 hours) suggests an effusion which may be due to suggests an effusion which may be due to meniscal injury. meniscal injury.

HistoryHistory

HistoryHistory
What was the degree of pain and What was the degree of pain and disability at the time of injury? How disability at the time of injury? How does this compare to the current does this compare to the current situation? situation?
Does the knee lock or click? Suggests Does the knee lock or click? Suggests a loose body and may be due to a loose body and may be due to meniscal injury. meniscal injury.

HistoryHistory
Does the knee give way? Suggests Does the knee give way? Suggests instability (e.g. ACL injury) or muscle instability (e.g. ACL injury) or muscle weakness. weakness.
Does the patient have a previous Does the patient have a previous history of knee injury? history of knee injury?
What are the patient's past medical What are the patient's past medical history, occupation and level of history, occupation and level of exercise? exercise?

SymptomsSymptoms
pain: causes of knee pain could be pain: causes of knee pain could be due to:due to:– Inflammatory.Inflammatory.– Degenerative.Degenerative.– Mechanical.Mechanical.– Trauma. In which the mechanism is Trauma. In which the mechanism is
useful.useful.

SymptomsSymptoms
Stiffness. Due to trauma or arthritis.Stiffness. Due to trauma or arthritis.
Locking. Differs from stiffness in Locking. Differs from stiffness in which the knee suddenly cannot which the knee suddenly cannot straightened fully, although flexion is straightened fully, although flexion is still possible like in torn meniscus. still possible like in torn meniscus.
Deformity like knock knee and bow Deformity like knock knee and bow leg.leg.

SymptomsSymptoms
Swelling which could be localized or Swelling which could be localized or diffused, it may appear suddenly like diffused, it may appear suddenly like in haemoarthrosis or after few hours in haemoarthrosis or after few hours like in torn meniscus.like in torn meniscus.
Giving way due to mechanical Giving way due to mechanical disorder or as a result of muscle disorder or as a result of muscle weakness.weakness.
Limp due to pain or instability. Limp due to pain or instability.

Signs Signs
Look Look
Valgus or varus deformity.Valgus or varus deformity.
Wasting.Wasting.
Swelling and lump.Swelling and lump.

Signs Signs

Signs Signs

Signs Signs

signssigns

SignsSignsFeel Feel Temperature.Temperature.intra-articular fluid in which can be tested intra-articular fluid in which can be tested by:by:– Cross-fluctuation test can test large amount Cross-fluctuation test can test large amount
of fluid.of fluid.– The patellar tap test can test moderate The patellar tap test can test moderate
amount of fluid.amount of fluid.– The bulge test can test small amount of fluid.The bulge test can test small amount of fluid.– The patellar hollow test can test very small The patellar hollow test can test very small
amount of fluid.amount of fluid.

SignsSigns


signssigns
Tenderness over soft tissue and Tenderness over soft tissue and bony outlines.bony outlines.
Synovial thickening.Synovial thickening.

Signs Signs
Move Move
Flexion and extension normally the Flexion and extension normally the range 0 - 150°. Hyperextension range 0 - 150°. Hyperextension should be recorded as minus degree.should be recorded as minus degree.
Rotation normally the knees can be Rotation normally the knees can be rotated internally and externally for rotated internally and externally for 10° if the hip and knee are 90° 10° if the hip and knee are 90° flexed. flexed.

Signs Signs

Tests for stabilityTests for stability
In testing for stability it is essential to In testing for stability it is essential to compare the normal with the compare the normal with the abnormal knee. abnormal knee.

Tests for stabilityTests for stabilityACL and PCL

Tests for stabilityTests for stability
The medial and lateral collateralThe medial and lateral collateral ligaments (MCL and LCL)ligaments (MCL and LCL)
are tested by stressing the knee into are tested by stressing the knee into valgus and varus: this is best done valgus and varus: this is best done by tucking the patient’s foot under by tucking the patient’s foot under your arm and holding the extended your arm and holding the extended knee firmly with one hand on each knee firmly with one hand on each side of the joint; the leg is then side of the joint; the leg is then angulated alternatively towards angulated alternatively towards abduction and adduction. This is abduction and adduction. This is called called valgus and varus stress tests.valgus and varus stress tests.

Tests for stabilityTests for stability
The test is performed at full The test is performed at full extension and again at 30 degrees extension and again at 30 degrees of flexion. Sideways movement in of flexion. Sideways movement in full extension is always abnormal: it full extension is always abnormal: it may be due to either may be due to either
1.1. Torn or stretched ligament.Torn or stretched ligament.
2.2. Loss of articular cartilage or bone. Loss of articular cartilage or bone.

Valgus stress test for MCL
Note Direction Of Forces
Leg flexed at 30°

Tests for stabilityTests for stabilityVarus Stress test for LCL
Note direction of forces

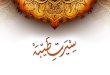
Tests for stabilityTests for stabilityThe cruciate ligamentsThe cruciate ligaments
are tested by examining for abnormal gliding are tested by examining for abnormal gliding movements in the antero-posterior plane. movements in the antero-posterior plane. With both knees flexed 90 degrees and the With both knees flexed 90 degrees and the feet resting on the couch, the upper tibia is feet resting on the couch, the upper tibia is inspected from the side; if its upper end has inspected from the side; if its upper end has dropped back, or can be gently pushed dropped back, or can be gently pushed back, this indicates a tear of the back, this indicates a tear of the posterior posterior cruciate ligament (the 'sag sign'). cruciate ligament (the 'sag sign').

Sagging Sign

Tests for stabilityTests for stability
With the knee in the same position, With the knee in the same position, the foot is anchored by the examiner the foot is anchored by the examiner sitting on it (provided this is not sitting on it (provided this is not painful): then, using both hands, the painful): then, using both hands, the upper end of the tibia is grasped upper end of the tibia is grasped firmly and rocked backwards and firmly and rocked backwards and frontward to see if there is any frontward to see if there is any antero-posterior glide (antero-posterior glide (the drawer the drawer testtest) )

Tests for stabilityTests for stability
an excessive posterior movement an excessive posterior movement ((a positive posterior drawer signa positive posterior drawer sign) ) signifies signifies posterior cruciate laxity posterior cruciate laxity

PCL exam
Posterior drawer test Posterior drawer test
(VC*):(VC*):
excessive backward
movement of the tibia in
relation to the femur.

Tests for stabilityTests for stability
Excessive anterior movement Excessive anterior movement
((a positive anterior drawer signa positive anterior drawer sign) ) denotes denotes anterior cruciate laxity anterior cruciate laxity

ACL examAnterior drawer Anterior drawer testtest:Excessive forward movement of the tibia on the femur

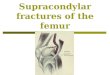
ACLACLLachman test-Lachman test- is more sensitive but this is more sensitive but this is difficult if the patient has big thighs (or is difficult if the patient has big thighs (or the examiner has small hands). The the examiner has small hands). The patient’s knee is flexed 30 degrees; with patient’s knee is flexed 30 degrees; with one hand grasping the lower thigh and the one hand grasping the lower thigh and the other the upper part of the leg, the joint other the upper part of the leg, the joint surfaces are shifted backwards and surfaces are shifted backwards and forwards upon each other. If the knee is forwards upon each other. If the knee is stable, there should be no gliding. stable, there should be no gliding.

ACL and PCL -Lachman Test
Note direction of forces
Grade the motion based on the amount of anterior translation.
Normal laxity is 0
Grade 1: Less than 0.5 cm of translation
Grade 2: 0.5-1.0 cm of translation
Grade 3: 1.0-1.5 cm of translation
Also assess the end point. Is it soft or firm?
Bend the knee to about 30 degrees. Then, stabilize the femur with one hand. Place the other hand behind the proximal tibia at the level of the joint line and then pull forward.

ACL exam
LachmanLachman’’ss test test (VC*)(VC*):The most sensitive test for ACL rupture

McMurray’s testMcMurray’s test
This is the classic test for a torn meniscus and is This is the classic test for a torn meniscus and is based on the fact that the loose tag can based on the fact that the loose tag can sometimes be trapped between the articular sometimes be trapped between the articular surfaces and then induced to snap free with a surfaces and then induced to snap free with a palpable and audible click. The knee is flexed as palpable and audible click. The knee is flexed as far as possible; one hand steadies the joint and far as possible; one hand steadies the joint and the other rotates the leg medially and laterally the other rotates the leg medially and laterally while the knee is slowly extended. The test is while the knee is slowly extended. The test is repeated several times with the knee stressed in repeated several times with the knee stressed in valgus or varus feeling and listening for the click.valgus or varus feeling and listening for the click.

Meniscus Testing
• McMurray’s Test• 3 passes with knee in
neutral, IR, and ER• Valgus stress applied
as knee extended• Varus stress applied
as knee is flexed• (+)= pain at jointline or
clicking/popping felt at jointline

Meniscus Testing
• Apley’s Compression Test
• Box 6-19, p. 232
• Knee flexed with axial loading of tibia into femur while tibia is rotated
• (+)= pain or popping at jointline

The patellofemoral jointThe patellofemoral jointThe patellofemoral joint is examined separately: The patellofemoral joint is examined separately: The size, shape and position of the patella are The size, shape and position of the patella are noted. The bone is felt first on its anterior surface noted. The bone is felt first on its anterior surface and then along is edges and at the attachments and then along is edges and at the attachments of the quadriceps tendon and the patellar of the quadriceps tendon and the patellar ligament. Much of the posterior surface is ligament. Much of the posterior surface is accessible to palpation if the patella is pushed accessible to palpation if the patella is pushed first to one side and then to the other: tenderness first to one side and then to the other: tenderness suggests synovial irritation or articular cartilage suggests synovial irritation or articular cartilage softening moving the patella up and down while softening moving the patella up and down while pressing it lightly against the femur (the friction pressing it lightly against the femur (the friction test') causes painful grating if the central portion test') causes painful grating if the central portion of the articular cartilage is damaged. of the articular cartilage is damaged.

KNEE SPECIAL TESTSKNEE SPECIAL TESTSApprehension TestApprehension Test
(Assessment for Patella Subluxation or Dislocation)
1. Athlete is sitting with the affected leg extended (straight).
2. Place thumbs along medial or lateral edge of patella.
3. Gently move patella in opposite direction.
(+) = athlete voices apprehension to you doing test OR pain on
movement

Do not forgot to examine the Do not forgot to examine the patient in prone position patient in prone position
These signs might be found:These signs might be found:
1.1. Bulging capsule (midline swelling).Bulging capsule (midline swelling).
2.2. Semi membranous bursa ( above Semi membranous bursa ( above joint line).joint line).
3.3. Baker’s cyst (below joint line).Baker’s cyst (below joint line).

Tests to be done from posterior Tests to be done from posterior aspect are:aspect are:
1.1. Apley’s testApley’s test
2.2. Lachman's test can be readily, Lachman's test can be readily, performed with the patient prone performed with the patient prone

ImagingImaging
Antero-posterior, lateral and Antero-posterior, lateral and sometimes patello-femoral (or sometimes patello-femoral (or skyline) and intercondylar or tunnel skyline) and intercondylar or tunnel views are needed. The antero-views are needed. The antero-posterior view should be taken with posterior view should be taken with the patient standing. Stress films in the patient standing. Stress films in valgus and varus are essential for valgus and varus are essential for diagnosing collateral ligament tears. diagnosing collateral ligament tears. Loose bodies also can e detected.Loose bodies also can e detected.

ImagingImaging
Arthrography and MRI are useful in Arthrography and MRI are useful in doubtful Meniscal or ligament doubtful Meniscal or ligament injuries.injuries.
Radioisotope Scans may show Radioisotope Scans may show increased activity in the sub articular increased activity in the sub articular bone which indicates early sign of bone which indicates early sign of osteoarthritis.osteoarthritis.

ArthroscopyArthroscopy
Arthroscopy is useful:Arthroscopy is useful: (1) To establish or refine the accuracy of diagnosis.(1) To establish or refine the accuracy of diagnosis. (2) To help in deciding whether to operate, or to (2) To help in deciding whether to operate, or to
plan the operative approach with more precision.plan the operative approach with more precision. (3) To record the progress of a knee disorder. (3) To record the progress of a knee disorder. (4) To perform certain operative procedures. (4) To perform certain operative procedures.