Embed Size (px)
Citation preview

Chapter 20Respiratory
System
Alveolar Duct

Respiration
1. Movement of air into and out of the lungs (Ventilation or Breathing)
2. Exchange of O2 and CO2 between the lungs and the blood
3. Transport of these gases
4. Exchange of O2 and CO2 between the blood and the tissues

Functions of the Respiratory System
1. Gas exchange
2. Regulation of blood pH
3. Voice production
4. Olfaction
5. Protection

Anatomy of the Respiratory System
• The respiratory system consist of the upper and lower respiratory tract
– Upper respiratory tract: external nose, nasal cavity, pharynx, and associated structures
– Lower respiratory tract: larynx, trachea, the bronchi, and lungs

Fig. 20.1


Nose
• Consist of the external nose and the nasal cavity– External nose
• only visible structure
– Nasal cavity• Nares or Nostrils – external openings• Choanae – openings to pharynx• Vestibule – anterior portion of nasal cavity• Hard palate – separates the nasal cavity from the oral cavity• Nasal septum – divides nose into right and left parts• Conchae – boney ridges in the nasal cavity• Meatus – Passageway beneath each conchae

Nose
– Provides an airway for respiration– Moistens and warms the entering air– Filters inspired air and cleans it of foreign
matter– Serves as a resonating chamber for speech– Houses the olfactory receptors

The Pharynx
• Connects the nasal cavity and mouth to the larynx and esophagus inferiorly
• Common passageway for air, food, and drink• Commonly called the throat• There are 3 regions:
– Nasopharynx: air only• posterior to the choanae and superior to the soft palate
– soft palate separates the nasopharynx from the oropharynx
– Oropharynx: air and food• soft palate to the epiglottis
– Laryngopharynx: primarily food and drink• epiglottis to the esophagus

Fig. 20.2

Larynx (Voice Box)
• Anterior part of the throat, from the base of the tongue to the trachea
• The three functions of the larynx are:1. To provide an airway
2. To act as a switching mechanism to route air and food into the proper channels
• Epiglottis: elastic cartilage that covers the laryngeal inlet during swallowing
• Closure of the vestibular and vocal folds
3. To function in voice production

Fig. 20.3

Vocal Cords
• Two pairs of ligaments• False vocal cords (vestibular folds)
– Superior mucosal folds – Have no part in sound production
• True vocal cords (vocal folds)– Inferior mucosal folds composed of elastic fibers – The medial opening between them is the glottis– They vibrate to produce sound as air rushes up from
the lungs– Laryngitis: Inflammation of the vocal folds

Fig. 20.4

Sound Production
• Sound: Vibration of the vocal folds as air moves past them
• Loudness: depends on the amplitude of the vibration, which is determined by the force at which the air rushes across the vocal cords
• Pitch: determined by the length and tension of the vocal cords, which changes the frequency of the vibrations
• Sound is “shaped” into language by action of the tongue, lips, teeth, and other structures
• The pharynx resonates, amplifies, and enhances sound quality

Trachea
• Descends from the larynx through the neck to the fifth thoracic vertebra
• Composed of dense regular connective tissue and smooth muscle reinforced with 15-20 C-shaped rings of hyaline cartilage, which protect the trachea and keep the airway open
• The mucous membrane lining the trachea is made up of goblet cells and pseudostratified ciliated columnar epithelium– Goblet cells produce mucus
• It ends by dividing into the two primary bronchi

Main Bronchi
• The right and left bronchi are formed by the division of the trachea
• Right primary bronchus is wider, shorter and more vertical than the left– Common site for an inhaled object to become lodged
• By the time that incoming air reaches the bronchi, it is warmed, cleansed and saturated with water vapor

Lungs
• Principal organs of respiration
• Base rest on diaphragm and the apex extends superiorly to ~2.5 cm above the clavicle
• Right lung has 3 lobes, while the left has only 2 lobes

The Tracheobronchial Tree
• Once inside the lungs each main bronchus– Subdivides into lobar (secondary) bronchi– Then segmental (tertiary) bronchi – Finally giving rise to the bronchioles, which
subdivide many times to give rise to the terminal bronchioles
• ~16 generations of branching from the trachea to the terminal bronchioles

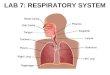
The Tracheobronchial Tree• Terminal bronchioles divide into respiratory
bronchioles, which have a few attached alveoli– Alveoli – small air filled chambers where gas
exchange between the air and blood takes place• Respiratory bronchioles lead to alveolar ducts,
then to terminal clusters of alveolar sacs composed of alveoli
• Approximately 300 million alveoli– Account for most of the lungs’ volume – Provide tremendous surface area for gas exchange
• ~7 generations of branching occur from the terminal bronchioles to the alveolar ducts

Fig. 20.5

Fig. 20.6

Fig. 20.7

The Tracheobronchial Tree
• As air passageways become smaller, structural changes occur – Cartilage support structures decrease– Amount of smooth muscle increases– Epithelium types change
• Terminal bronchioles are mostly smooth muscle with no cartilage, which allows the bronchioles to alter their diameter when a change in air flow is needed (i.e. during exercise)

Alveoli
• Alveolar walls:– Are a single layer of type I pneumocytes
• Squamous epithelial cells• Compose 90% of the alveolar surface• Permit gas exchange by simple diffusion
– Type II pneumocytes• Round or cube-shaped secretory cells that
produce surfactant• Surfactant reduces surface tension, which makes it
easier for the alveoli to expand

Respiratory Membrane
• Where gas exchange between air and blood occurs
• It is very thin to facilitate the diffusion of gases• Consists of:
1. Thin layer of fluid lining the alveolus
2. Alveolar epithelium
3. Basement membrane of the alveolar epithelium
4. A thin interstitial space
5. Basement membrane of the capillary endothelium
6. The capillary endothelium

Fig. 20.8

Pleura• Thin, double-layered serous membranes• Parietal pleura
– Covers the thoracic wall, diaphragm, and mediastinum
• Visceral pleura– Covers the external lung surface
• Pleural cavity– Negative pressure space between the parietal and visceral
pleura
• Pleural Fluid– Fills the pleural cavity– Made by the pleural membranes– Serves as a lubricant– Holds the pleural membranes together

Fig. 20.9


Blood Supply to Lungs
• Lungs are perfused by two circulations: pulmonary and bronchial
• Pulmonary circulation– Pulmonary arteries: supply deoxygenated systemic blood to be
oxygenated• Ultimately feed into the pulmonary capillary network surrounding the
alveoli
– Pulmonary veins: carry oxygenated blood from lungs back to the heart
• Bronchial circulation– Bronchial arteries: provide systemic oxygenated blood to the
lung tissue• Supply all lung tissue except the alveoli
– Bronchial veins: carry the deoxygenated blood back to the heart

• Inspiration: movement of air into the lungs– Muscles involved are the diaphragm and those that elevate the
ribs and sternum– As the diaphragm and other muscles of inspiration contract and
the rib cage rises and thoracic volume increases
• Expiration: movement of air out of the lungs– Muscles actively involved are those that depress the ribs and
sternum (usually only with forceful expiration)– Largely a passive process– Muscles of inspiration relax, the rib cage descends due to gravity
and the thoracic cavity volume decreases
• Pressure changes in the thoracic cavity change air pressure in the lungs, which in turn causes ventilation– largest change in thoracic volume is due to the diaphragm
Ventilation

Fig. 20.10

Pressure Changes and Airflow• Physical Principles Influencing Pulmonary Ventilation
1. Air flows from areas of higher to lower pressure– If pressure is higher at one end of a tube (P1) than at the other
(P2), air will flow down its pressure gradient
2. Changes in volume result in changes in pressure– As volume increases in a closed container the pressure
decreases or as volume decreases pressure increases– This inverse relationship is known as Boyle’s law
3. Changes in tube diameter result in changes in resistance– Poiseuille’s law: resistance (R) to airflow is proportional to the
diameter (d) of a tube raised to the fourth power (d4)
F =P1 – P2
RF=Airflow(mm/min)


Alveoli Airflow
Fig. 20.11

Alveoli Airflow
Fig. 20.11

Fig. 20.11


Lung Recoil
• Tendency for an expanded lung to decrease in size due to
1. Elastic fibers in the connective tissue
2. Surface tension
• Two factors keep lungs from collapsing1. Surfactant
2. Pleural Pressures

Surfactant
• Surface acting agent
• Mixture of lipoprotein molecules
• Acts in reducing surface tension in the alveoli– Attraction of water molecules to each other
• Surfactant reduces the surface tension in alveoli by 10-fold

Pleural Pressure
• Pressure in the pleural cavity– When pleural pressure is less than alveolar
pressure alveoli expand
• Subatmospheric pleural pressure is caused by– Removal of fluid from the pleural cavity– Lung recoil

Measurement of Lung Function
• Measurements can be used to – Diagnose disease– Track progress of disease– Track recovery from disease
• Measurements include– Lung compliance– Pulmonary volumes and capacities– Minute ventilation– Alveolar ventilation

Lung Compliance• Measurement of the ease with which the lungs
and thorax expand• Volume increases for each unit of pressure
change in alveolar pressure– Liters (volume of air)/Centimeter of H2O (pressure)
• In a normal person = 0.13 L/cm H2O– Higher than normal compliance = less resistance to
lung and thorax expansion• Emphysema
– Lower than normal compliance = more resistance to lung and thorax expansion
• Pulmonary fibrosis, infant respiratory distress syndrome, pulmonary edema, asthma, bronchitis, and lung cancer

Pulmonary Function Tests
• Spirometry is the process of measuring volumes of air that move into and out of the respiratory system
• Spirometer – a device used to measure these pulmonary volumes
• The following factors can cause variations in Pulmonary Volumes and Capacities
• Sex• Age • Body Size • Physical Condition

Pulmonary Volumes
• Tidal volume (TV)– volume of air inspired or expired with each breath (approximately
500 ml at rest)
• Inspiratory reserve volume (IRV)– amount of air that can be inspired forcefully after inspiration of
the tidal volume (approximately 3000 ml at rest)
• Expiratory reserve volume (ERV)– amount of air that can be forcefully expired after expiration of the
tidal volume (approximately 1100 ml at rest)
• Residual volume (RV)– volume of air still remaining in the respiratory passages and
lungs after the most forceful expiration (approximately 1200 ml)

Pulmonary Capacities• Sum of two or more pulmonary volumes• Inspiratory capacity (IC = IRV + TV)
– Amount of air that a person can inspire maximally after a normal expiration (approximately 3500mL at rest )
• Functional residual capacity (FRC = ERV + RV)– Amount of air remaining in the lungs after a normal expiration
(approximately 2300mL at rest )
• Vital capacity (VC = IRV + TV + ERV)– Maximum volume of air that a person can expel from the
respiratory tract after a maximum inspiration (approximately 4600mL at rest )
• Total lung capacity (TLC = IRV + ERV + TV + RV)– Sum of all lung volumes (approximately 5800 ml at rest)

Fig. 20.12

Pulmonary Function Tests
• Forced expiratory vital capacity– individual inspires maximally and then exhales
maximally as rapidly as possible– volume of air expired at the end of the test is the
person’s forced expiratory vital capacity
• Forced expiratory volume in 1 second (FEV1)– amount of air expired during the first second of the
test
– decreased FEV1 can be caused by airway obstruction, asthma, emphysema, tumors, pulmonary fibrosis, silicosis, kyphosis, and scoliosis

Minute Ventilation• Minute Ventilation
– equals tidal volume (~500mls) times respiratory rate (~12 breaths/min.)
– Average ~ 6 L/min– Only measures movement of air into and out of the lungs, not
amount of air available for gas exchange
• Dead space– Areas of the respiratory system where gas exchange does
not take place– Includes the nasal cavity, pharynx, larynx, trachea, bronchi,
bronchioles, and terminal bronchioles (~150 mLs)– Nonfunctional alveoli can also contribute, but are rare in
healthy individuals

Alveolar Ventilation
• Alveolar ventilation (VA)– volume of air available for gas exchange
• Slow, deep breathing increases AVR and rapid, shallow breathing decreases AVR
VA = ƒ X (VT – VD)
(mLs/min)(frequency, breaths/min)
(Tidal Volume – Dead Space)
(mLs/respiration)


Gas Exchange in the Tissues
1. In the tissues, CO2 diffuses into the plasma and into RBC. Some of the CO2 remains in the plasma
2. In RBC, CO2 reacts with H2O to form carbonic acid (H2CO3) in a reaction catalyzed by the enzyme carbonic anhydrase (CA)
3. H2CO3 dissociates to form bicarbonate ions (HCO3
-) and hydrogen ions (H+)
4. In the chloride shift, as HCO3-
diffuses out of the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) into them
5. Oxygen (O2) is released from hemoglobin (Hb). O2 diffuses out of RBCs and plasma into the tissues
6. H+ combine with Hb, which promotes the release of O2 from Hb (Bohr effect)
7. CO2 combines with Hb. Hb that has released O2 readily combines with CO2 (Haldane effect)

Gas Exchange in the Tissues
1. In the tissues, CO2 diffuses into the plasma and into RBC. Some of the CO2 remains in the plasma
2. In RBC, CO2 reacts with H2O to form carbonic acid (H2CO3) in a reaction catalyzed by the enzyme carbonic anhydrase (CA)
3. H2CO3 dissociates to form bicarbonate ions (HCO3
-) and hydrogen ions (H+)
4. In the chloride shift, as HCO3-
diffuses out of the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) into them
5. Oxygen (O2) is released from hemoglobin (Hb). O2 diffuses out of RBCs and plasma into the tissues
6. H+ combine with Hb, which promotes the release of O2 from Hb (Bohr effect)
7. CO2 combines with Hb. Hb that has released O2 readily combines with CO2 (Haldane effect)

Gas Exchange in the Tissues
1. In the tissues, CO2 diffuses into the plasma and into RBC. Some of the CO2 remains in the plasma
2. In RBC, CO2 reacts with H2O to form carbonic acid (H2CO3) in a reaction catalyzed by the enzyme carbonic anhydrase (CA)
3. H2CO3 dissociates to form bicarbonate ions (HCO3
-) and hydrogen ions (H+)
4. In the chloride shift, as HCO3-
diffuses out of the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) into them
5. Oxygen (O2) is released from hemoglobin (Hb). O2 diffuses out of RBCs and plasma into the tissues
6. H+ combine with Hb, which promotes the release of O2 from Hb (Bohr effect)
7. CO2 combines with Hb. Hb that has released O2 readily combines with CO2 (Haldane effect)

Gas Exchange in the Tissues
1. In the tissues, CO2 diffuses into the plasma and into RBC. Some of the CO2 remains in the plasma
2. In RBC, CO2 reacts with H2O to form carbonic acid (H2CO3) in a reaction catalyzed by the enzyme carbonic anhydrase (CA)
3. H2CO3 dissociates to form bicarbonate ions (HCO3
-) and hydrogen ions (H+)
4. In the chloride shift, as HCO3-
diffuses out of the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) into them
5. Oxygen (O2) is released from hemoglobin (Hb). O2 diffuses out of RBCs and plasma into the tissues
6. H+ combine with Hb, which promotes the release of O2 from Hb (Bohr effect)
7. CO2 combines with Hb. Hb that has released O2 readily combines with CO2 (Haldane effect)

Gas Exchange in the Tissues
1. In the tissues, CO2 diffuses into the plasma and into RBC. Some of the CO2 remains in the plasma
2. In RBC, CO2 reacts with H2O to form carbonic acid (H2CO3) in a reaction catalyzed by the enzyme carbonic anhydrase (CA)
3. H2CO3 dissociates to form bicarbonate ions (HCO3
-) and hydrogen ions (H+)
4. In the chloride shift, as HCO3-
diffuses out of the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) into them
5. Oxygen (O2) is released from hemoglobin (Hb). O2 diffuses out of RBCs and plasma into the tissues
6. H+ combine with Hb, which promotes the release of O2 from Hb (Bohr effect)
7. CO2 combines with Hb. Hb that has released O2 readily combines with CO2 (Haldane effect)

Gas Exchange in the Tissues
1. In the tissues, CO2 diffuses into the plasma and into RBC. Some of the CO2 remains in the plasma
2. In RBC, CO2 reacts with H2O to form carbonic acid (H2CO3) in a reaction catalyzed by the enzyme carbonic anhydrase (CA)
3. H2CO3 dissociates to form bicarbonate ions (HCO3
-) and hydrogen ions (H+)
4. In the chloride shift, as HCO3-
diffuses out of the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) into them
5. Oxygen (O2) is released from hemoglobin (Hb). O2 diffuses out of RBCs and plasma into the tissues
6. H+ combine with Hb, which promotes the release of O2 from Hb (Bohr effect)
7. CO2 combines with Hb. Hb that has released O2 readily combines with CO2 (Haldane effect)

Gas Exchange in the Tissues
1. In the tissues, CO2 diffuses into the plasma and into RBC. Some of the CO2 remains in the plasma
2. In RBC, CO2 reacts with H2O to form carbonic acid (H2CO3) in a reaction catalyzed by the enzyme carbonic anhydrase (CA).
3. H2CO3 dissociates to form bicarbonate ions (HCO3
-) and hydrogen ions (H+).
4. In the chloride shift, as HCO3- diffuse
out of the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) into them.
5. Oxygen (O2) is released from hemoglobin (Hb). O2 diffuses out of RBCs and plasma into the tissues
6. H+ combine with Hb, which promotes the release of O2 from Hb (Bohr effect)
7. CO2 combines with Hb. Hb that has released O2 readily combines with CO2 (Haldane effect)

Gas Exchange in the Tissues
1. In the tissues, CO2 diffuses into the plasma and into RBC. Some of the CO2 remains in the plasma
2. In RBC, CO2 reacts with H2O to form carbonic acid (H2CO3) in a reaction catalyzed by the enzyme carbonic anhydrase (CA)
3. H2CO3 dissociates to form bicarbonate ions (HCO3
-) and hydrogen ions (H+)
4. In the chloride shift, as HCO3-
diffuses out of the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) into them
5. Oxygen (O2) is released from hemoglobin (Hb). O2 diffuses out of RBCs and plasma into the tissues
6. H+ combine with Hb, which promotes the release of O2 from Hb (Bohr effect)
7. CO2 combines with Hb. Hb that has released O2 readily combines with CO2 (Haldane effect)

Gas Exchange in the Lungs
1. In the lungs, CO2 diffuses from the RBCs and plasma into the alveoli
2. Carbonic anhydrase (CA) catalyzes the formation of CO2 and H2O from carbonic acid (H2CO3)
3. Bicarbonate ions (HCO3-) and H+
combine to replace H2CO3
4. In the chloride shift, as HCO3- diffuse
into the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) out of them
5. Oxygen diffuses into the plasma and into RBCs. Some of the O2 remains in the plasma. O2 binds to Hb
6. H+ are released from Hb, which promotes the uptake of O2 by Hb (Bohr effect)
7. CO2 is released from Hb. Hb that is bound to O2 readily releases CO2 (Haldane effect)

Gas Exchange in the Lungs
1. In the lungs, CO2 diffuses from the RBCs and plasma into the alveoli
2. Carbonic anhydrase (CA) catalyzes the formation of CO2 and H2O from carbonic acid (H2CO3)
3. Bicarbonate ions (HCO3-) and H+
combine to replace H2CO3
4. In the chloride shift, as HCO3- diffuse
into the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) out of them
5. Oxygen diffuses into the plasma and into RBCs. Some of the O2 remains in the plasma. O2 binds to Hb
6. H+ are released from Hb, which promotes the uptake of O2 by Hb (Bohr effect)
7. CO2 is released from Hb. Hb that is bound to O2 readily releases CO2 (Haldane effect)

Gas Exchange in the Lungs
1. In the lungs, CO2 diffuses from the RBCs and plasma into the alveoli
2. Carbonic anhydrase (CA) catalyzes the formation of CO2 and H2O from carbonic acid (H2CO3)
3. Bicarbonate ions (HCO3-) and H+
combine to replace H2CO3
4. In the chloride shift, as HCO3- diffuse
into the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) out of them
5. Oxygen diffuses into the plasma and into RBCs. Some of the O2 remains in the plasma. O2 binds to Hb
6. H+ are released from Hb, which promotes the uptake of O2 by Hb (Bohr effect)
7. CO2 is released from Hb. Hb that is bound to O2 readily releases CO2 (Haldane effect)

Gas Exchange in the Lungs
1. In the lungs, CO2 diffuses from the RBCs and plasma into the alveoli
2. Carbonic anhydrase (CA) catalyzes the formation of CO2 and H2O from carbonic acid (H2CO3)
3. Bicarbonate ions (HCO3-) and H+
combine to replace H2CO3
4. In the chloride shift, as HCO3- diffuse
into the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) out of them
5. Oxygen diffuses into the plasma and into RBCs. Some of the O2 remains in the plasma. O2 binds to Hb
6. H+ are released from Hb, which promotes the uptake of O2 by Hb (Bohr effect)
7. CO2 is released from Hb. Hb that is bound to O2 readily releases CO2 (Haldane effect)

Gas Exchange in the Lungs
1. In the lungs, CO2 diffuses from the RBCs and plasma into the alveoli
2. Carbonic anhydrase (CA) catalyzes the formation of CO2 and H2O from carbonic acid (H2CO3)
3. Bicarbonate ions (HCO3-) and H+
combine to replace H2CO3
4. In the chloride shift, as HCO3- diffuse
into the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) out of them
5. Oxygen diffuses into the plasma and into RBCs. Some of the O2 remains in the plasma. O2 binds to Hb
6. H+ are released from Hb, which promotes the uptake of O2 by Hb (Bohr effect)
7. CO2 is released from Hb. Hb that is bound to O2 readily releases CO2 (Haldane effect)

Gas Exchange in the Lungs
1. In the lungs, CO2 diffuses from the RBCs and plasma into the alveoli
2. Carbonic anhydrase (CA) catalyzes the formation of CO2 and H2O from carbonic acid (H2CO3)
3. Bicarbonate ions (HCO3-) and H+
combine to replace H2CO3
4. In the chloride shift, as HCO3- diffuse
into the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) out of them
5. Oxygen diffuses into the plasma and into RBCs. Some of the O2 remains in the plasma. O2 binds to Hb
6. H+ are released from Hb, which promotes the uptake of O2 by Hb (Bohr effect)
7. CO2 is released from Hb. Hb that is bound to O2 readily releases CO2 (Haldane effect)

Gas Exchange in the Lungs
1. In the lungs, CO2 diffuses from the RBCs and plasma into the alveoli
2. Carbonic anhydrase (CA) catalyzes the formation of CO2 and H2O from carbonic acid (H2CO3)
3. Bicarbonate ions (HCO3-) and H+
combine to replace H2CO3
4. In the chloride shift, as HCO3- diffuse
into the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) out of them
5. Oxygen diffuses into the plasma and into RBCs. Some of the O2 remains in the plasma. O2 binds to Hb
6. H+ are released from Hb, which promotes the uptake of O2 by Hb (Bohr effect)
7. CO2 is released from Hb. Hb that is bound to O2 readily releases CO2 (Haldane effect)

Gas Exchange in the Lungs
1. In the lungs, CO2 diffuses from the RBCs and plasma into the alveoli
2. Carbonic anhydrase (CA) catalyzes the formation of CO2 and H2O from carbonic acid (H2CO3)
3. Bicarbonate ions (HCO3-) and H+
combine to replace H2CO3
4. In the chloride shift, as HCO3- diffuse
into the RBC, electrical neutrality is maintained by the diffusion of chloride ions (Cl-) out of them
5. Oxygen diffuses into the plasma and into RBCs. Some of the O2 remains in the plasma. O2 binds to Hb
6. H+ are released from Hb, which promotes the uptake of O2 by Hb (Bohr effect)
7. CO2 is released from Hb. Hb that is bound to O2 readily releases CO2 (Haldane effect)


![Respiratory system roadmap.pptx [Repaired] - Loginanatomical-sciences.health.wits.ac.za/roadmaps/Respiratory system... · DIVISION OF THE RESPIRATORY SYSTEM CONDUCTING PORTION Nasal](https://img.pdfslide.us/doc/110x75/5a78c3d87f8b9ae6228c9db0/respiratory-system-repaired-loginanatomical-scienceshealthwitsaczaroadmapsrespiratory.jpg)


















![Anatomy and Physiology Respiratory System [Tab 2] Respiratory System](https://img.pdfslide.us/doc/110x75/56649ebd5503460f94bc631f/anatomy-and-physiology-respiratory-system-tab-2-respiratory-system.jpg)