Embed Size (px)
Citation preview
Dept of periodontics
Periodontal flaps
Presented by, S.SHIFAYA NASRIN SHIJI MARGARETD.SAPNAD.SARANYA
CRRI
Definition
“A periodontal flap is a section of gingiva and/or mucosa surgically separated from the underlying tissues to provide visibility and access to the bone and root surface.
INDICATIONS:
•Irregular bony contours
•Pockets on teeth in which a complete removal of
root irritants is not clinically possible
•Grade II or III furcation involvement
•Root resection / hemisection
•Persistent inflammation in areas with moderate
to deep pockets.
CONTRAINDICATIONS
• Uncontrolled medical conditions such as‐unstable angina‐uncontrolled diabetes‐uncontrolled hypertension‐myocardial infarction / stroke within 6
months •Poor plaque control•High caries rate
Bone exposure after flap reflection
•Full thickness (mucoperiosteal)
•Partial thickness (mucosal)
Placement of the flap after surgery
•Non displaced flaps
•Displaced flaps
Management of the papilla
•Conventional flaps
•Papilla preservation flaps
Classification of flaps
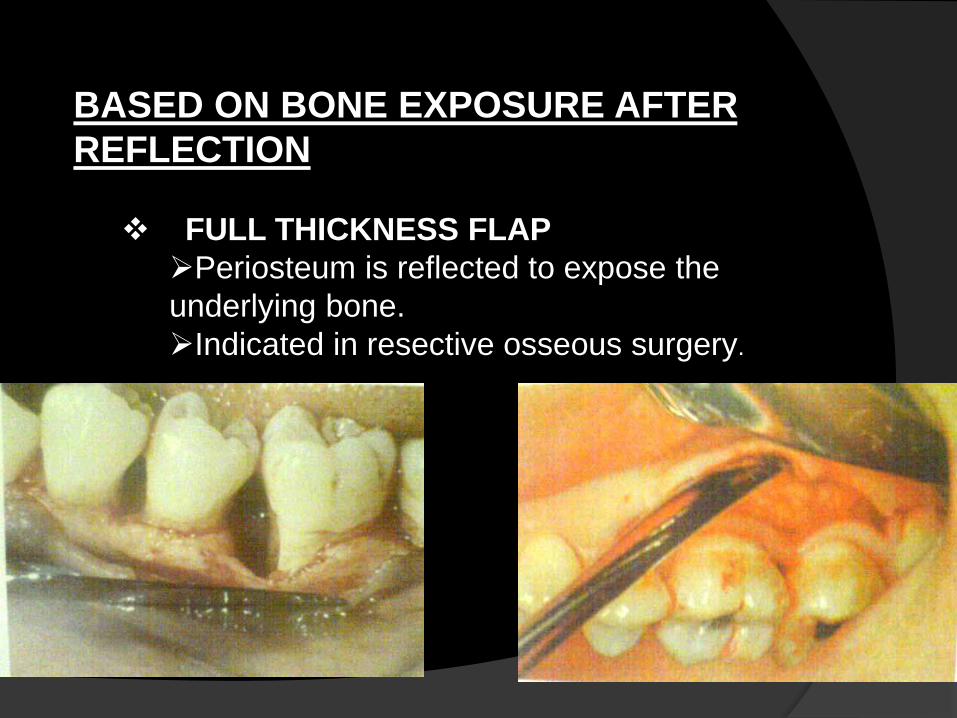
BASED ON BONE EXPOSURE AFTER
REFLECTION
FULL THICKNESS FLAP
Periosteum is reflected to expose the
underlying bone.
Indicated in resective osseous surgery.
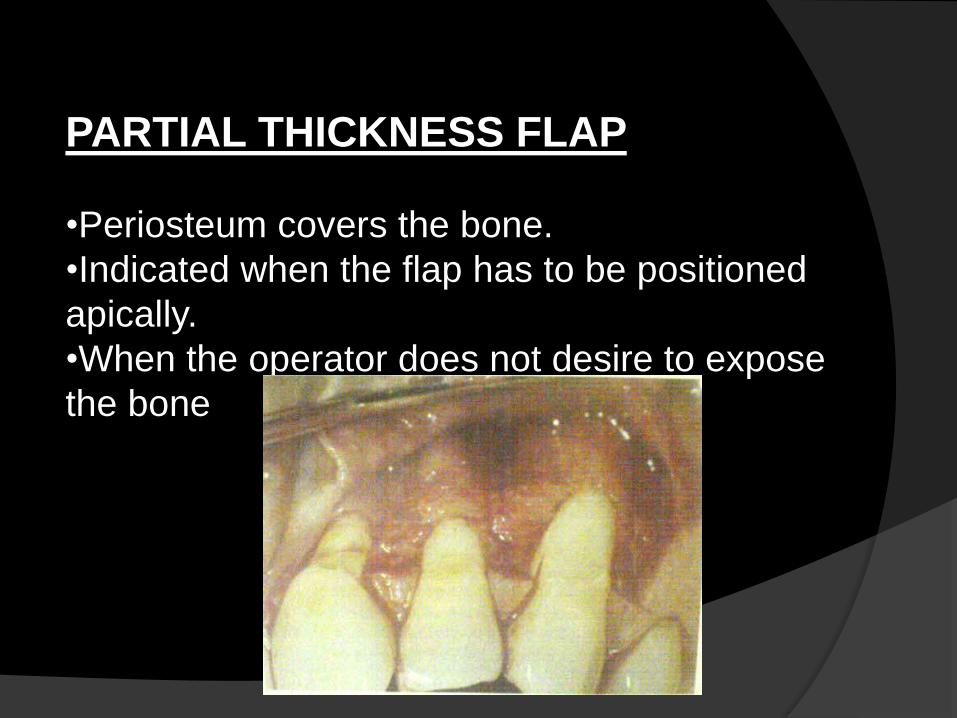
PARTIAL THICKNESS FLAP
•Periosteum covers the bone.
•Indicated when the flap has to be positioned
apically.
•When the operator does not desire to expose
the bone

BASED ON FLAP PLACEMENT AFTER SURGERY•Non displaced flaps:
When the flap is returned and sutured in
its original position.
•Displaced flaps:
When the flap is placed apically,
coronally or laterally to their original
position
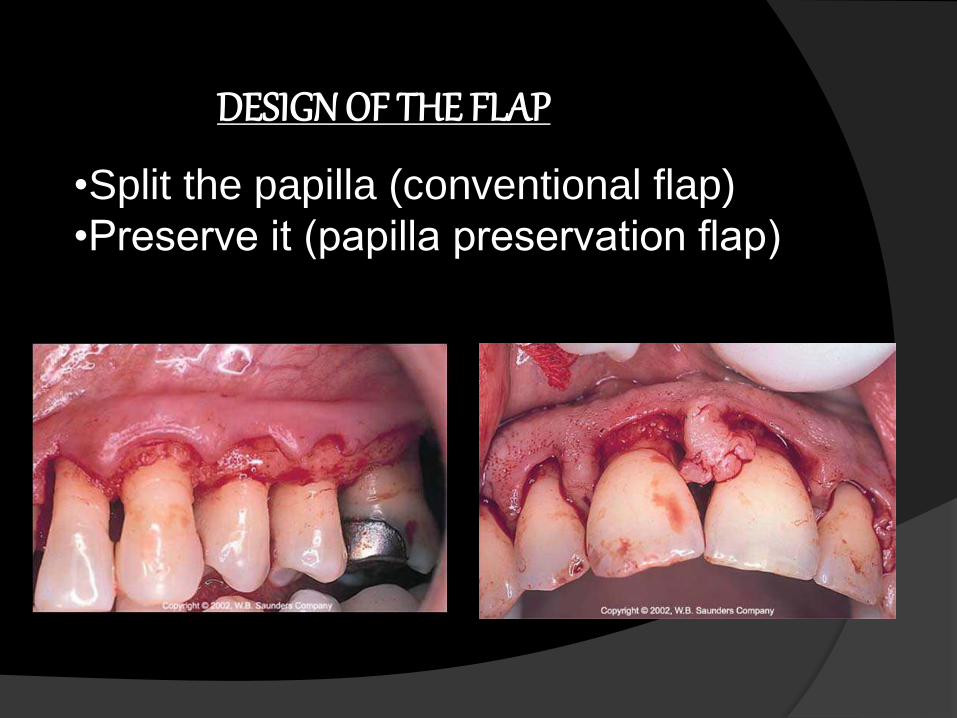
DESIGN OF THE FLAP
•Split the papilla (conventional flap)
•Preserve it (papilla preservation flap)
MODIFIED WIDMAN
FLAP
THE ORIGINAL ‘WIDMAN’ FLAP: In 1918, Leonard Wildman published the
detailed description of this procedure for pocket
elimination
In 1965, Morris revived this technique and called
it as “unrepositioned mucoperiosteal flap”
The flap was elevated to expose 2-3 mm of the
alveolar bone.
The soft tissue collar incorporating the pocket
epithelium and connective tissue was removed,
the exposed root surface scaled and the bone
recontoured to re-establish a 'physiologic'
alveolar form.
The flap margins were placed at the level of
the bony crest to achieve optimal pocket
reduction.
MODIFIED WIDMAN FLAP:
Presented by Ramfjord and Nissle in 1974
Exposing the root surfaces for meticulous
instrumentation and for removal of the pocket
Lining.
INDICATIONS:
Effective with pocket depths of 5-7 mm
CONTRAINDICATIONS:
This technique is difficult incase of very thin
and narrow attached gingiva ,because a narrow
band of attached gingiva does
not permit the initial scalloped incision
ADVANTAGE:
Root cleaning done
with direct vision.
Healing by primary
intention.
Minimal crestal bone
resorption.
Lack of post operative
discomfort.
DISADVANTAGE:
Requires high degree of technical skill
Interproximal flap require exact
placement.
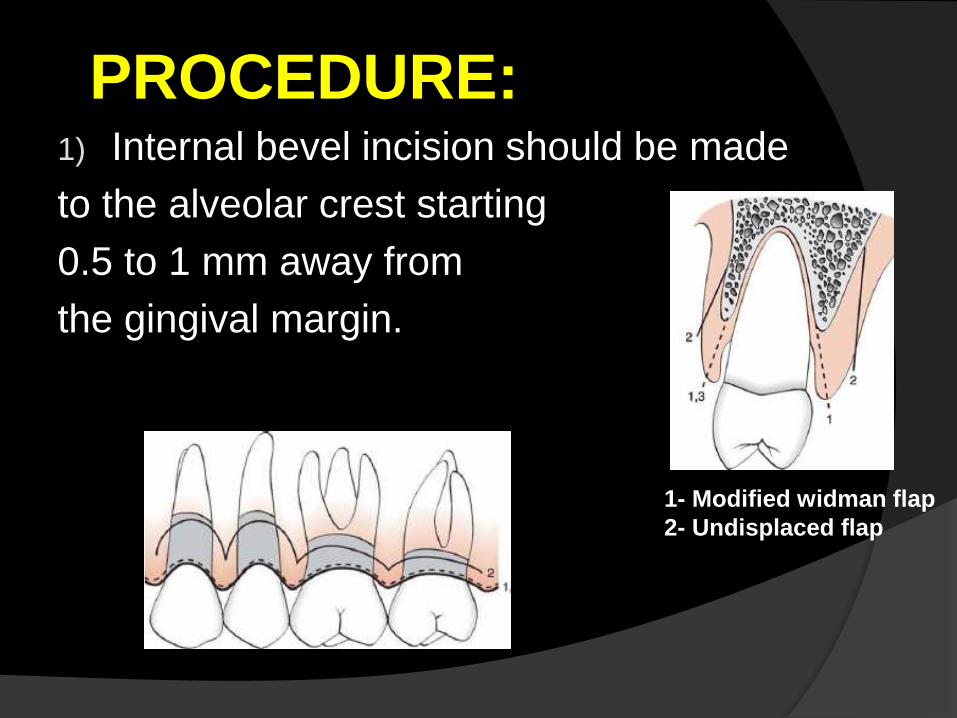
1) Internal bevel incision should be made
to the alveolar crest starting
0.5 to 1 mm away from
the gingival margin.
PROCEDURE:
1- Modified widman flap
2- Undisplaced flap
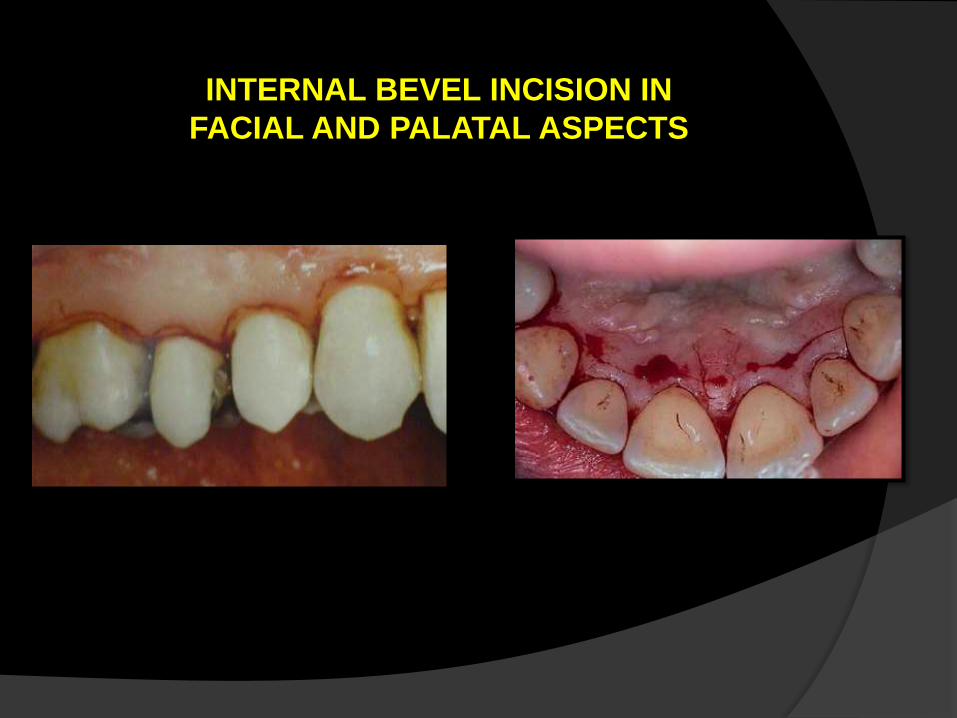
INTERNAL BEVEL INCISION IN
FACIAL AND PALATAL ASPECTS
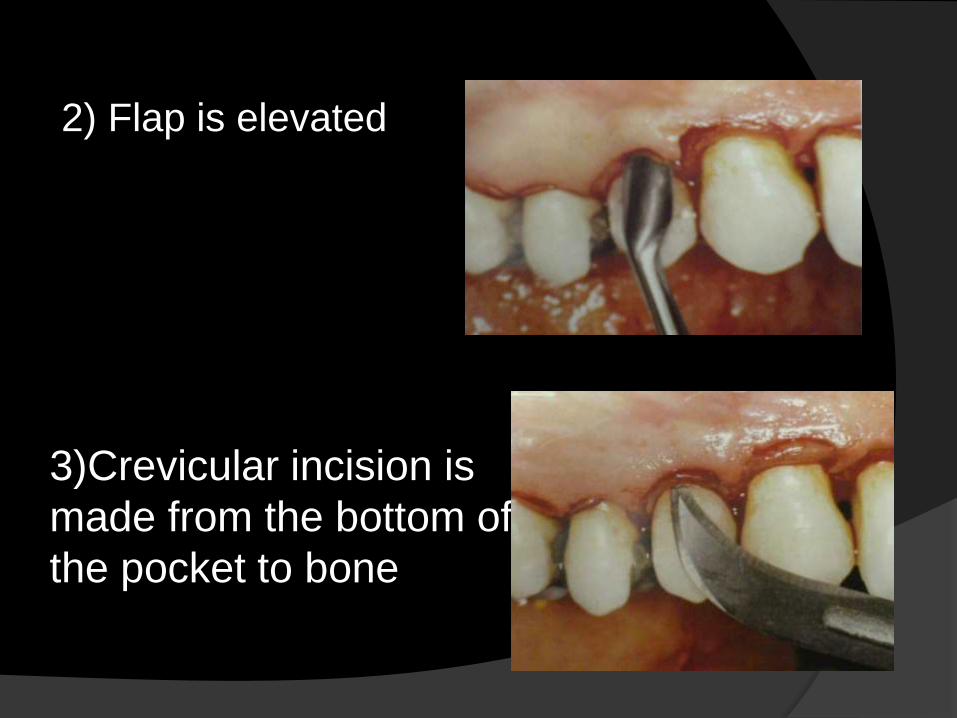
2) Flap is elevated
3)Crevicular incision is
made from the bottom of
the pocket to bone
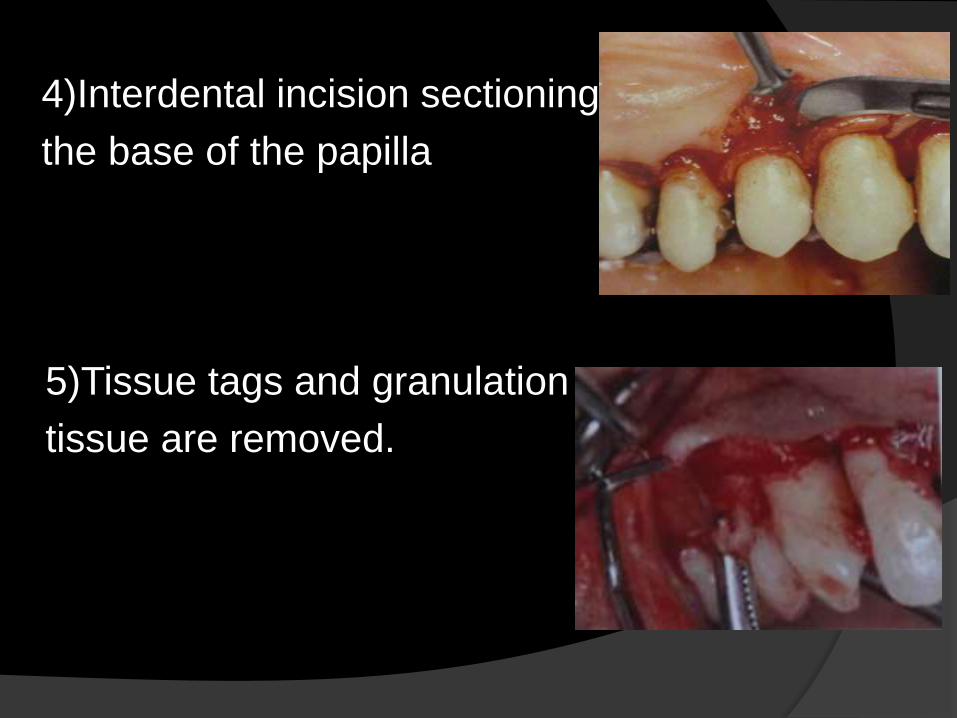
4)Interdental incision sectioning
the base of the papilla
5)Tissue tags and granulation
tissue are removed.
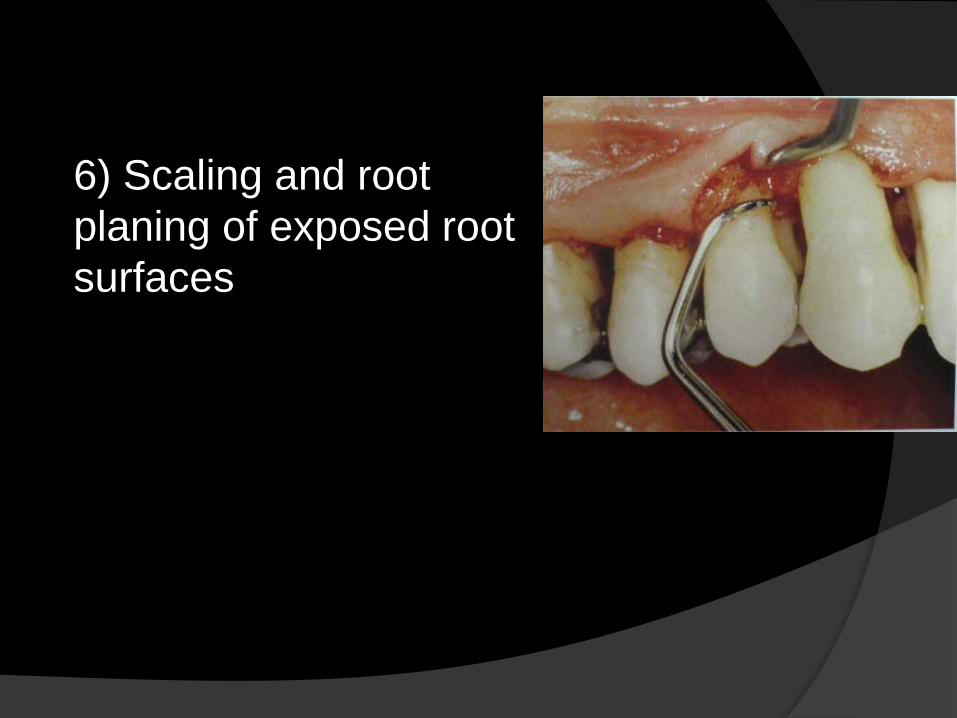
6) Scaling and root
planing of exposed root
surfaces
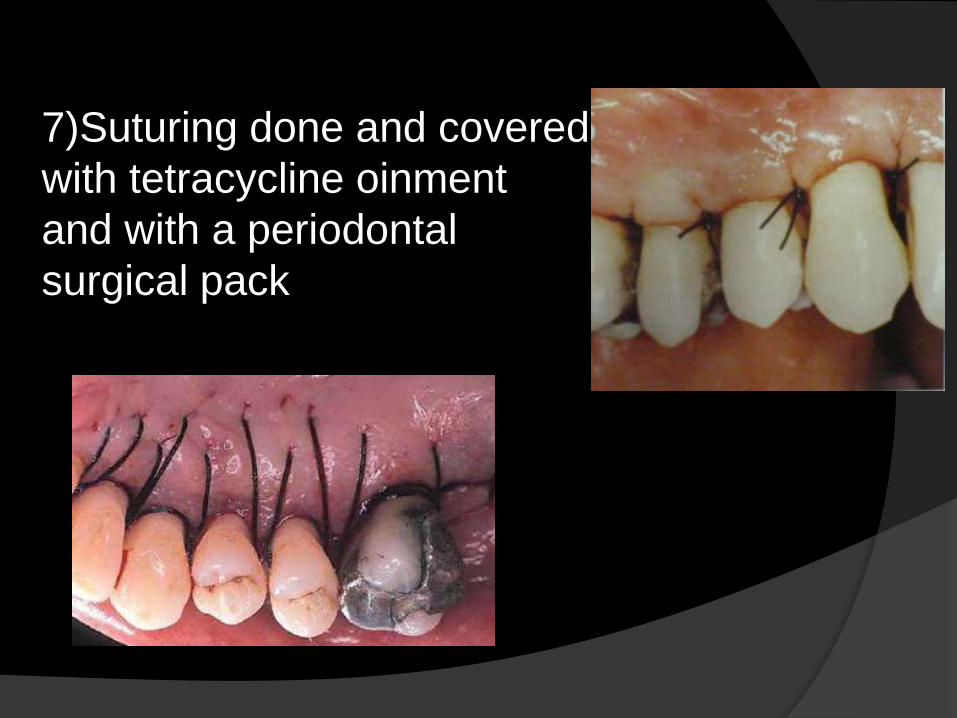
7)Suturing done and covered
with tetracycline oinment
and with a periodontal
surgical pack

Post operative results
UNDISPLACED FLAP Unrepositioned flap improves accessibility for
instrumentation ,but it also removes the pocket
wall there by reducing or eliminating the pocket.
It differs from the modified Widman flap in
that the soft tissue pocket wall is removed with
the initial incision; thus it considered an
“internal bevel gingivectomy”.
INDICATION:
Used for palatal tissue surgery
ADVANTAGE:
Flap is positioned and sutured in its
original position
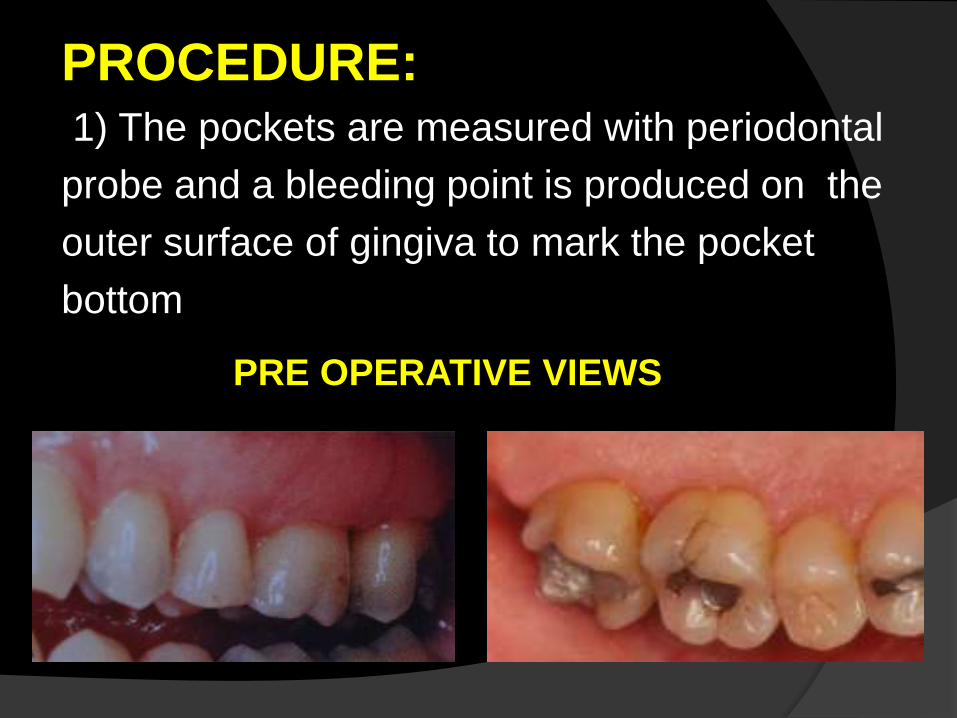
PROCEDURE:1) The pockets are measured with periodontal
probe and a bleeding point is produced on the
outer surface of gingiva to mark the pocket
bottom
PRE OPERATIVE VIEWS
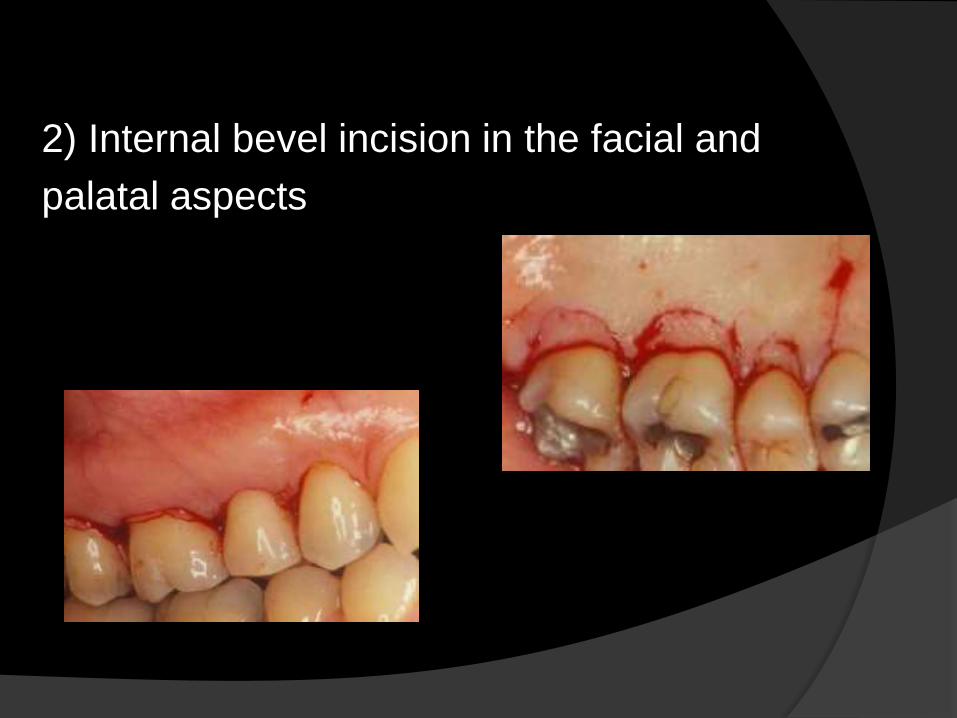
2) Internal bevel incision in the facial and
palatal aspects

3)Crevicular incision is made and Flap is
elevated
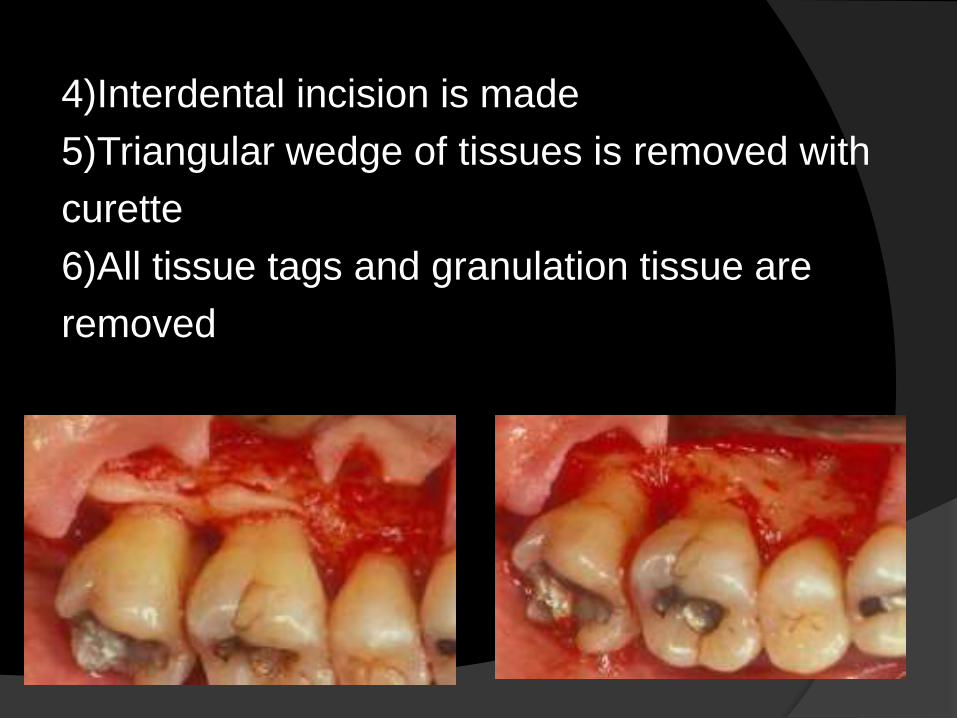
4)Interdental incision is made
5)Triangular wedge of tissues is removed with
curette
6)All tissue tags and granulation tissue are
removed

7)After the scaling and root planing the flap
edge should rest on the root bone junction.
8)Flaps have been placed in their original site
and Sutured.

Post operative results
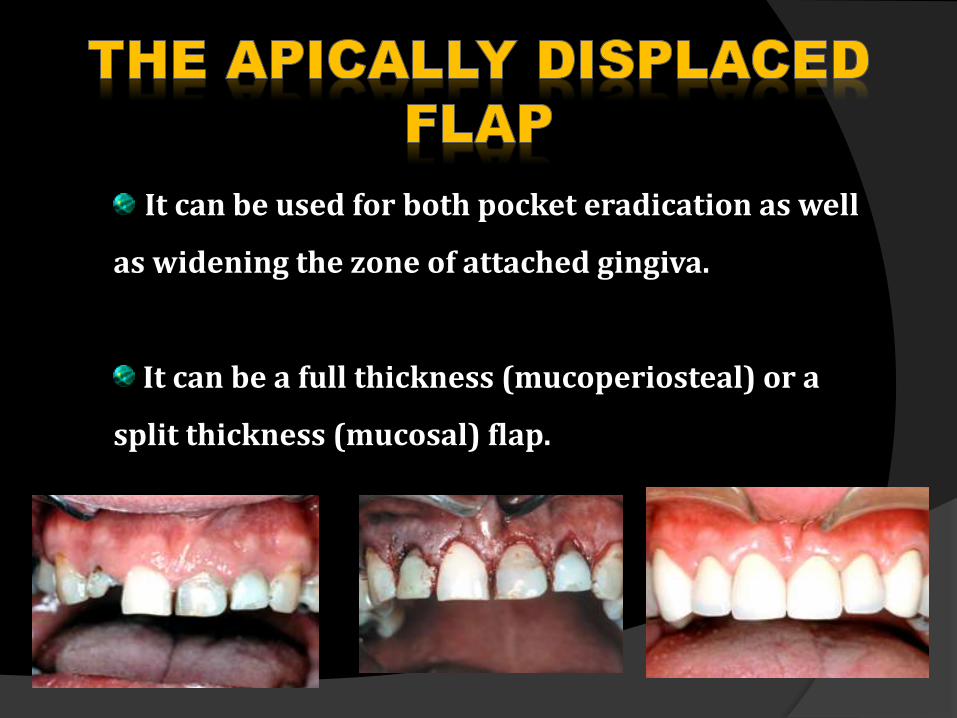
It can be used for both pocket eradication as well
as widening the zone of attached gingiva.
It can be a full thickness (mucoperiosteal) or a
split thickness (mucosal) flap.
INDICATIONS:
pocket eradication
increasing the width of attached gingiva
Used in cases of surgery on the buccal surfaces
of upper and lower jaws and
Lingual surfaces of lower jaw
CONTRAINDICATIONS:
Periodontal pockets in severe periodontal disease.
Periodontal pockets in areas where esthetics is critical.
Deep intrabony defects.
Patient at high risk for caries.
Severe hypersensitivity.
Tooth with marked mobility and severe attachment loss.
Palatal aspect of maxillary teeth, this is due to lack of
alveolar mucosa on palatal aspect
Tooth with extremely unfavorable clinical crown / Root
ratio.
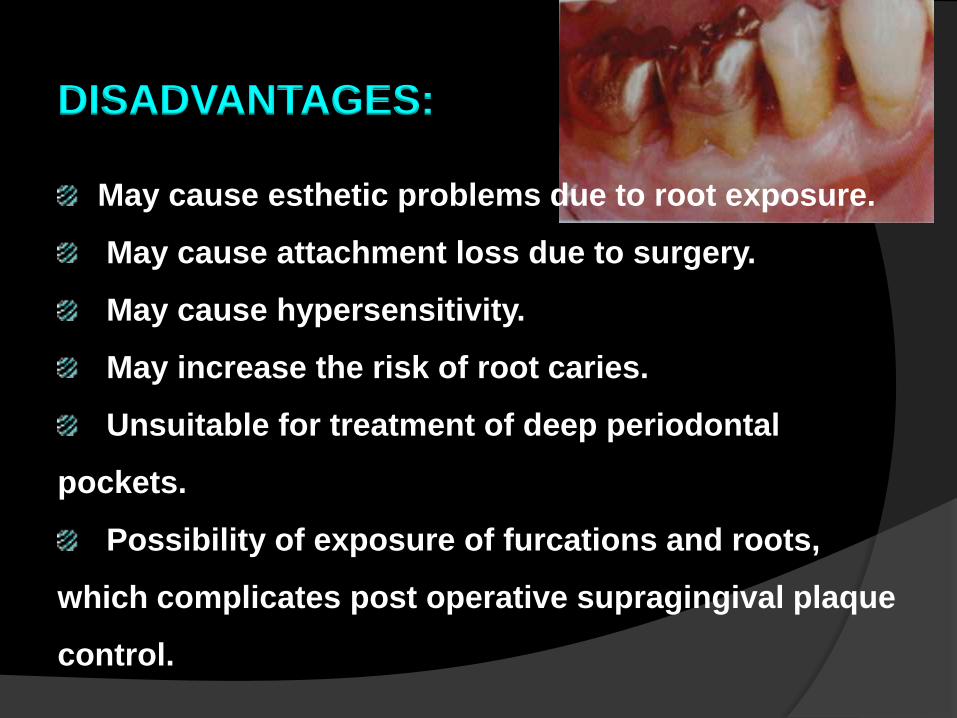
DISADVANTAGES:
May cause esthetic problems due to root exposure.
May cause attachment loss due to surgery.
May cause hypersensitivity.
May increase the risk of root caries.
Unsuitable for treatment of deep periodontal
pockets.
Possibility of exposure of furcations and roots,
which complicates post operative supragingival plaque
control.
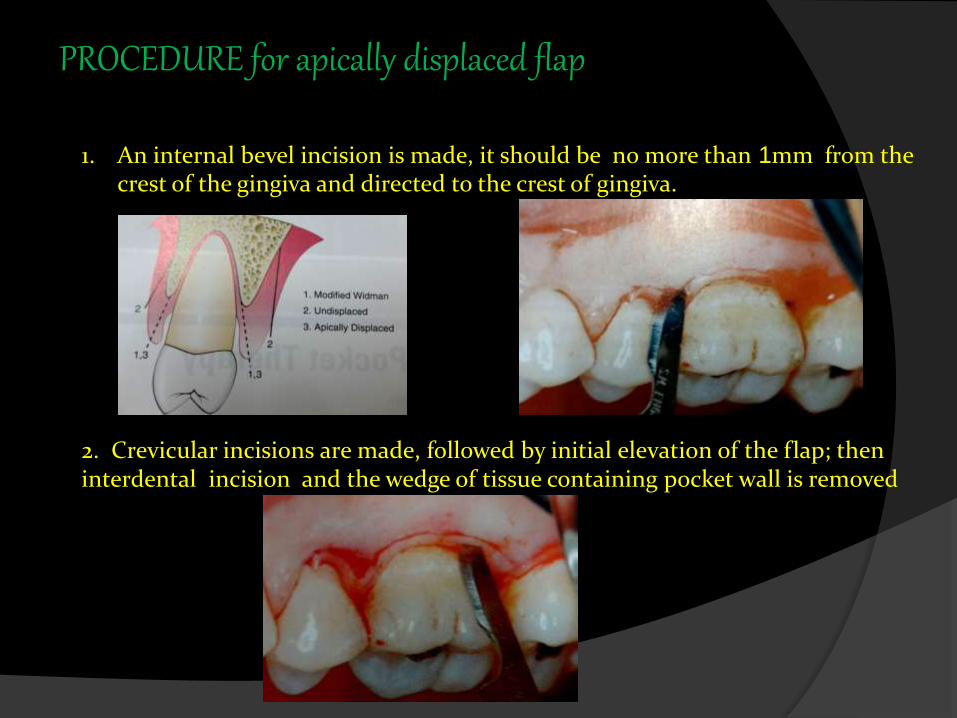
PROCEDURE for apically displaced flap
1. An internal bevel incision is made, it should be no more than 1mm from the crest of the gingiva and directed to the crest of gingiva.
2. Crevicular incisions are made, followed by initial elevation of the flap; then interdental incision and the wedge of tissue containing pocket wall is removed
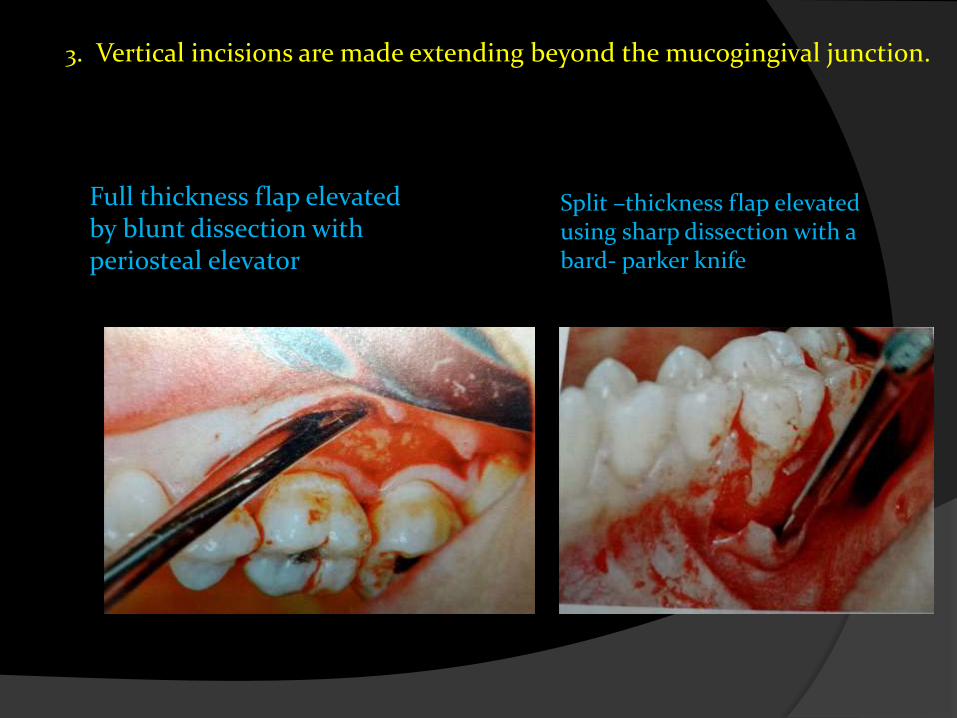
3. Vertical incisions are made extending beyond the mucogingival junction.
Full thickness flap elevated by blunt dissection with periosteal elevator
Split –thickness flap elevated using sharp dissection with a bard- parker knife

4.After debridement of the areas
5.Sutures in place

PRE TREATMENT-
POST TREATMENT
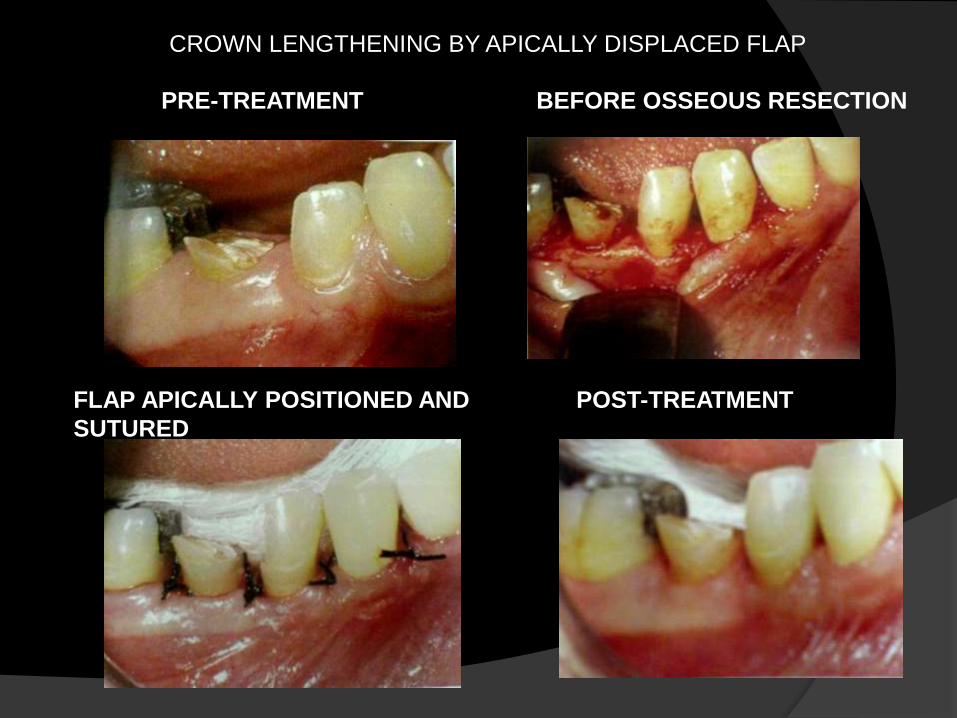
PRE-TREATMENT BEFORE OSSEOUS RESECTION
FLAP APICALLY POSITIONED AND
SUTURED
POST-TREATMENT
CROWN LENGTHENING BY APICALLY DISPLACED FLAP
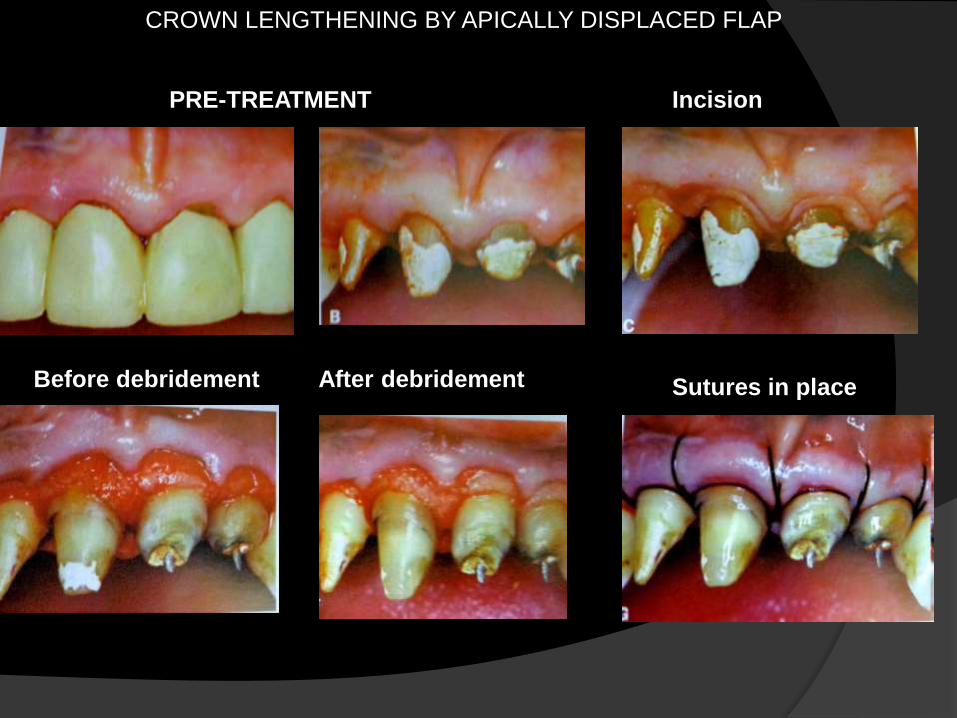
CROWN LENGTHENING BY APICALLY DISPLACED FLAP
PRE-TREATMENT
Before debridement After debridement
Incision
Sutures in place
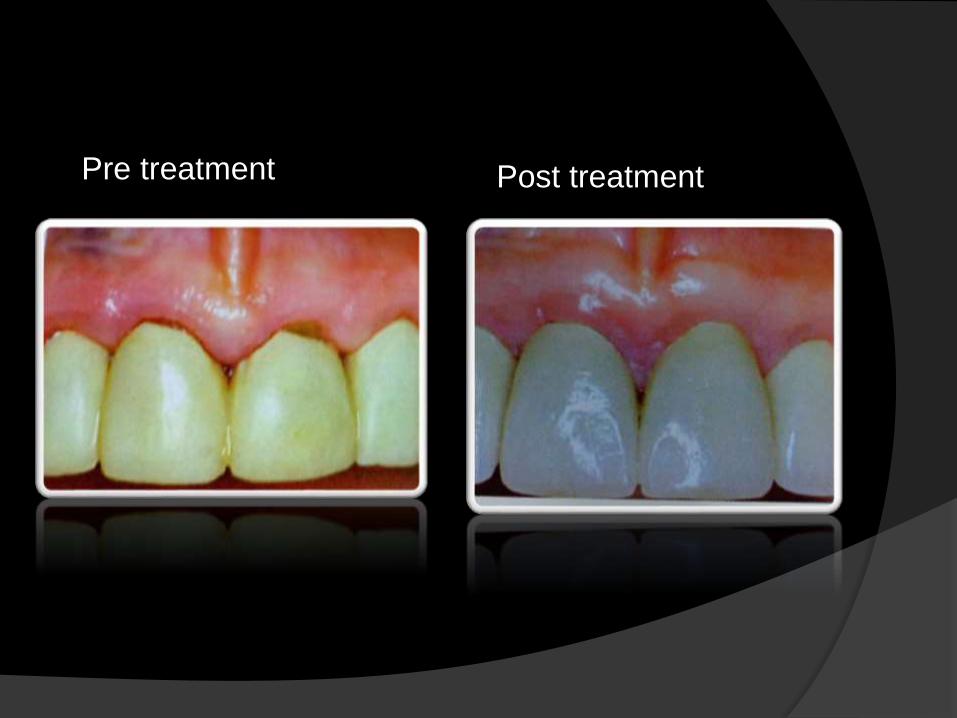
Pre treatment Post treatment
FLAPS FOR REGENERATIVE SURGERY
Two flap designs are available for
regenerative surgery:
1. The papilla preservation flap&
2. The conventional flap with only crevicular incisions.
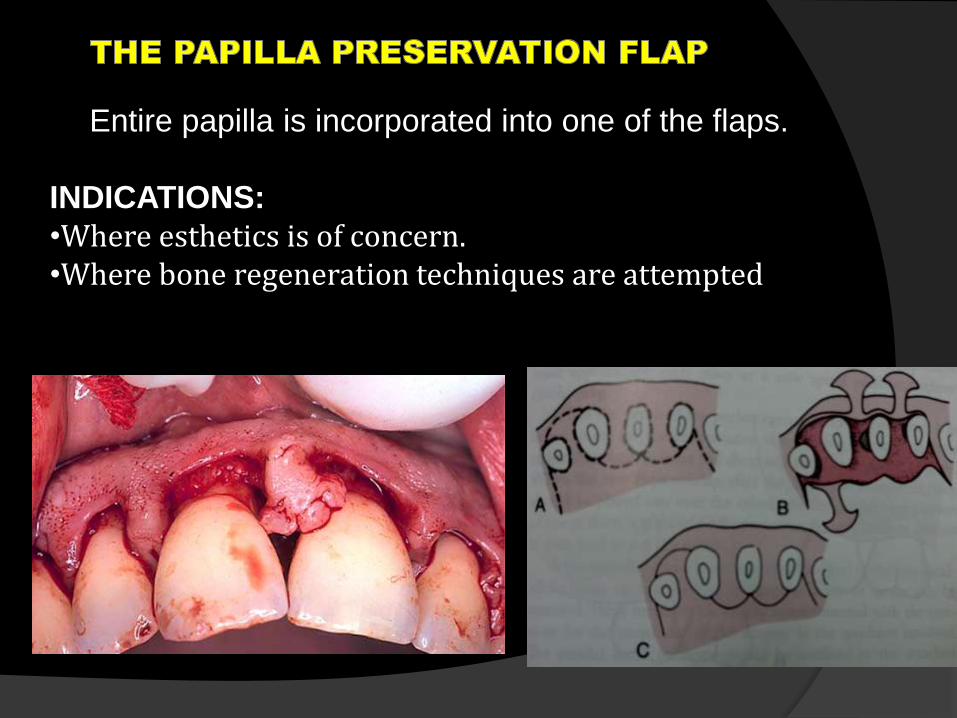
Entire papilla is incorporated into one of the flaps.
INDICATIONS:
•Where esthetics is of concern.•Where bone regeneration techniques are attempted
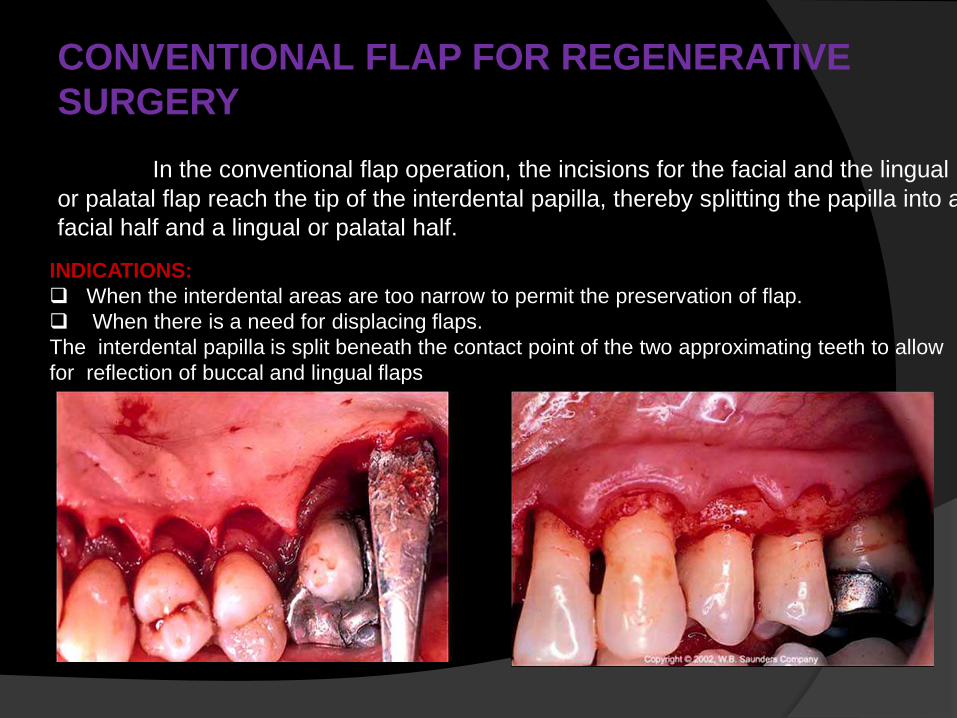
CONVENTIONAL FLAP FOR REGENERATIVE
SURGERY
In the conventional flap operation, the incisions for the facial and the lingual
or palatal flap reach the tip of the interdental papilla, thereby splitting the papilla into a
facial half and a lingual or palatal half.
INDICATIONS:
When the interdental areas are too narrow to permit the preservation of flap.
When there is a need for displacing flaps.
The interdental papilla is split beneath the contact point of the two approximating teeth to allow
for reflection of buccal and lingual flaps
DISTAL MOLAR
SURGERY
Treatment of periodontal pockets on the
distal surface of terminal molars is often
complicated by the presence of bulbous
fibrous tissue over the maxillary
tuberosity or prominent retromolar pads
in the mandible.
Operations for this purpose were
described by Robinson and Braden
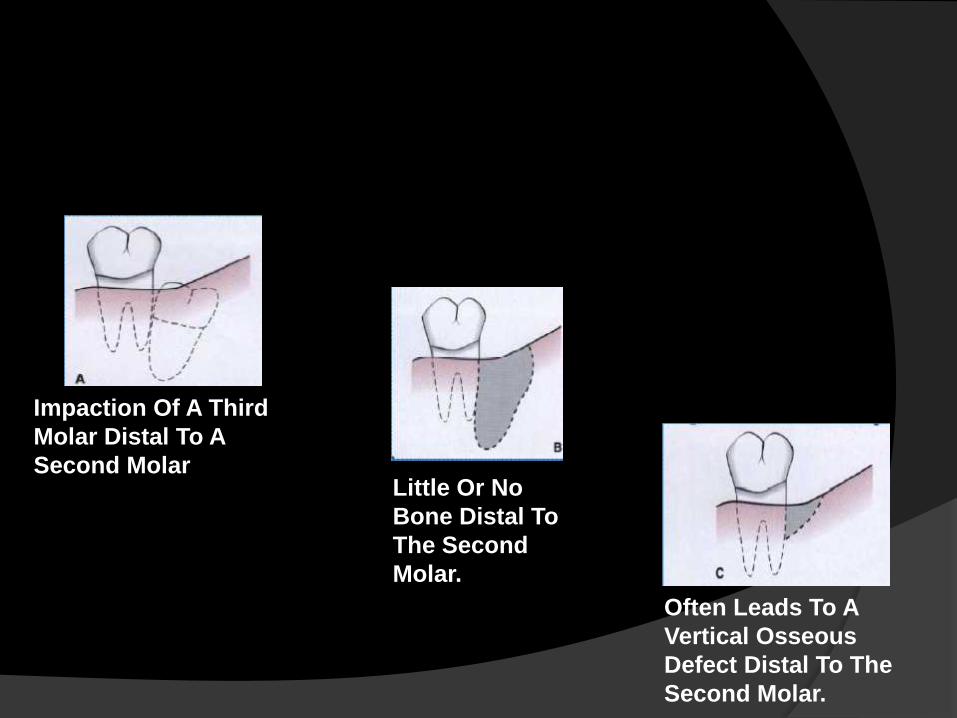
Impaction Of A Third
Molar Distal To A
Second MolarLittle Or No
Bone Distal To
The Second
Molar.
Often Leads To A
Vertical Osseous
Defect Distal To The
Second Molar.
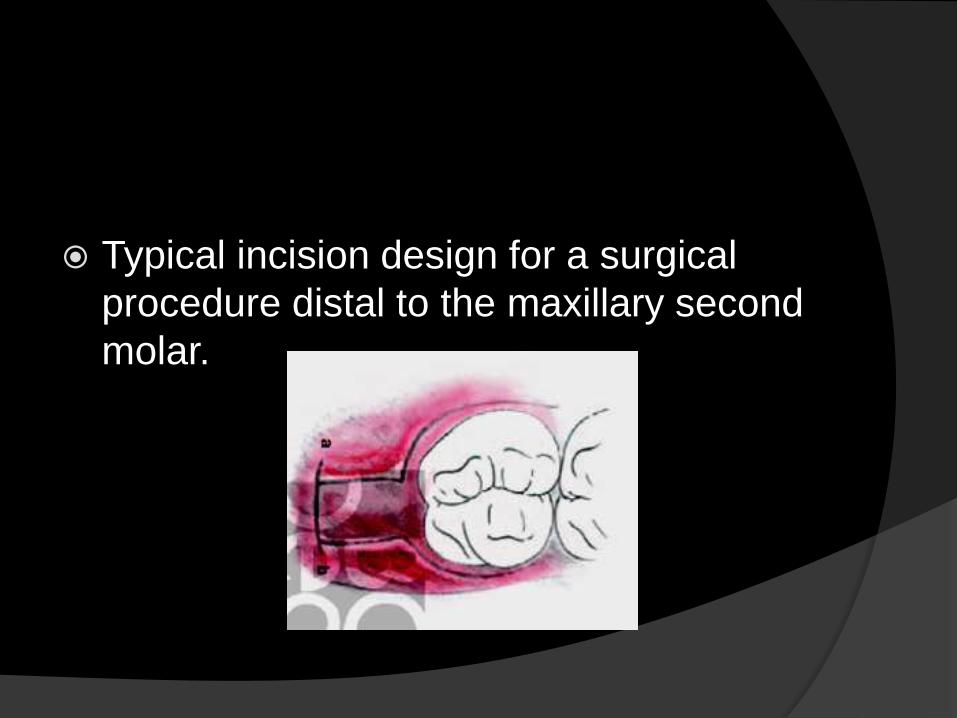
Typical incision design for a surgical
procedure distal to the maxillary second
molar.
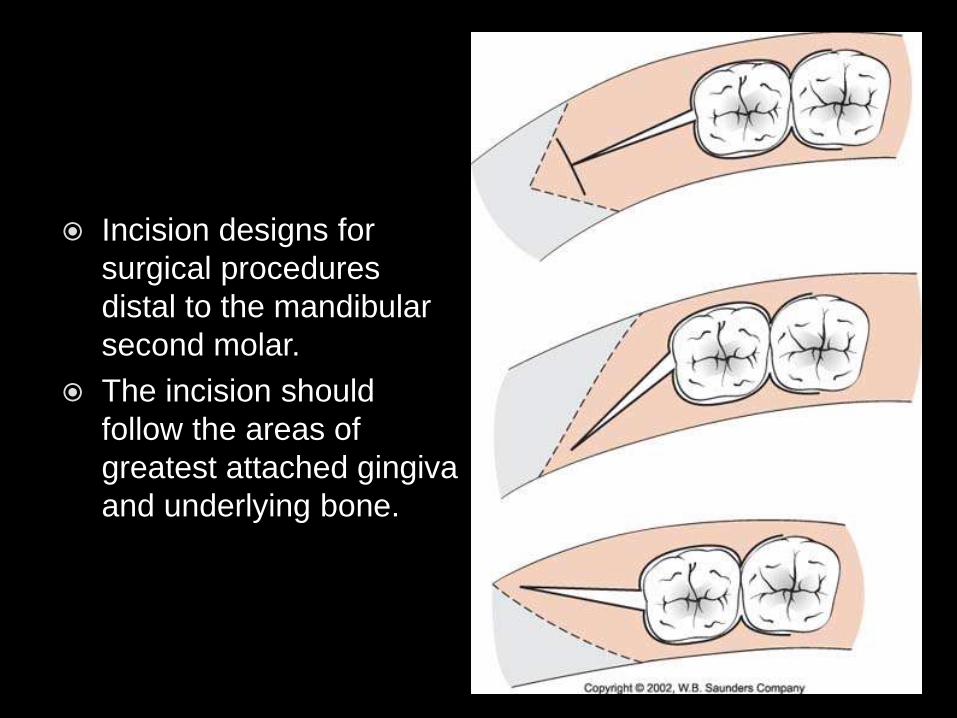
Incision designs for
surgical procedures
distal to the mandibular
second molar.
The incision should
follow the areas of
greatest attached gingiva
and underlying bone.
Distal wedge
Triangular
Square , parallel or H-design
Linear or pedicle
The size, shape ,thickness and access
of the tuberosity or retromolar area
determine treatment procedures
ADVANTAGES
Maintainence of attached tissue
Access to treatment of both the distal
furcation and underlying osseous
irregularities
Closure by mature thin tissue
Greater opening and access when done
in conjunction with other flap procedures
limitation
Accessability or anatomy(ascending
ramus and external oblique ridge)
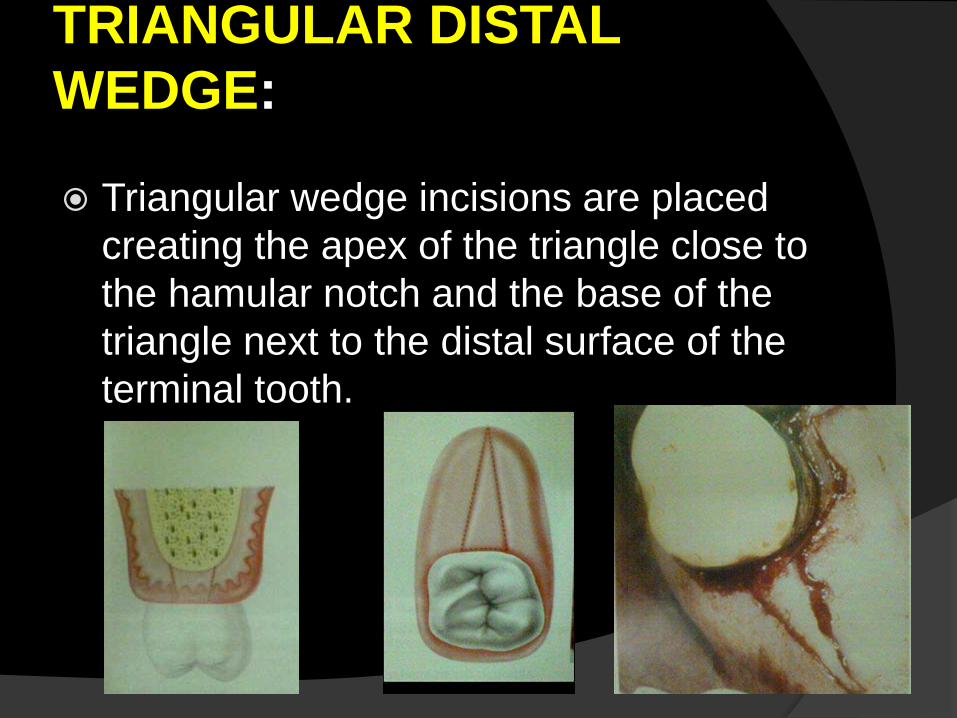
TRIANGULAR DISTAL
WEDGE:
Triangular wedge incisions are placed
creating the apex of the triangle close to
the hamular notch and the base of the
triangle next to the distal surface of the
terminal tooth.
Instrument used
no.12 or no.15 scalpel blade
scalers ,hoes , or knives
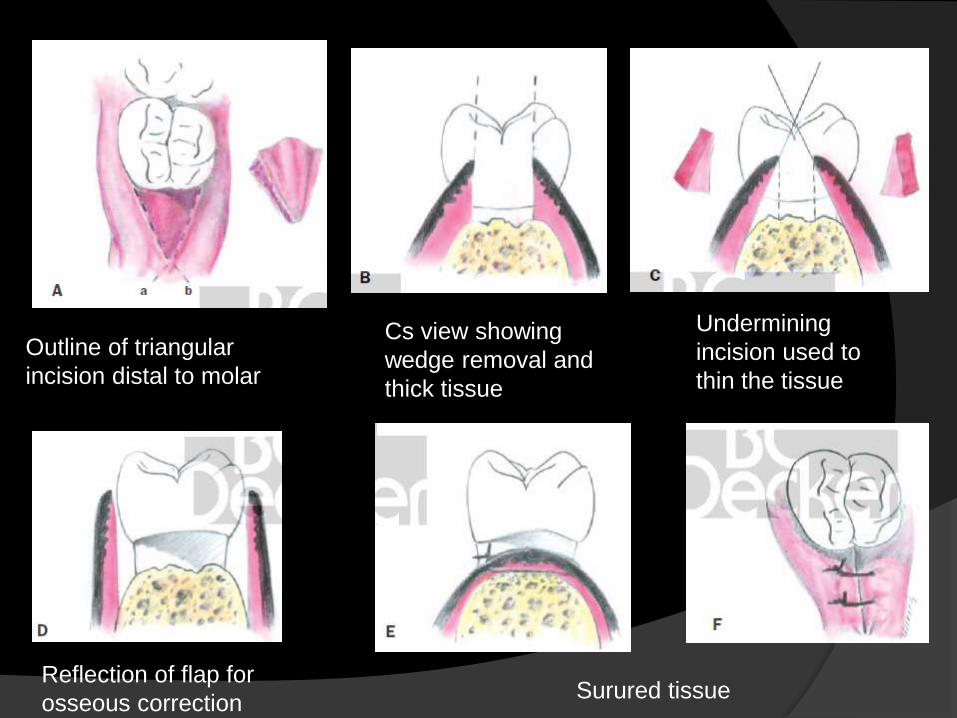
Outline of triangular
incision distal to molar
Cs view showing
wedge removal and
thick tissue
Undermining
incision used to
thin the tissue
Reflection of flap for
osseous correctionSurured tissue
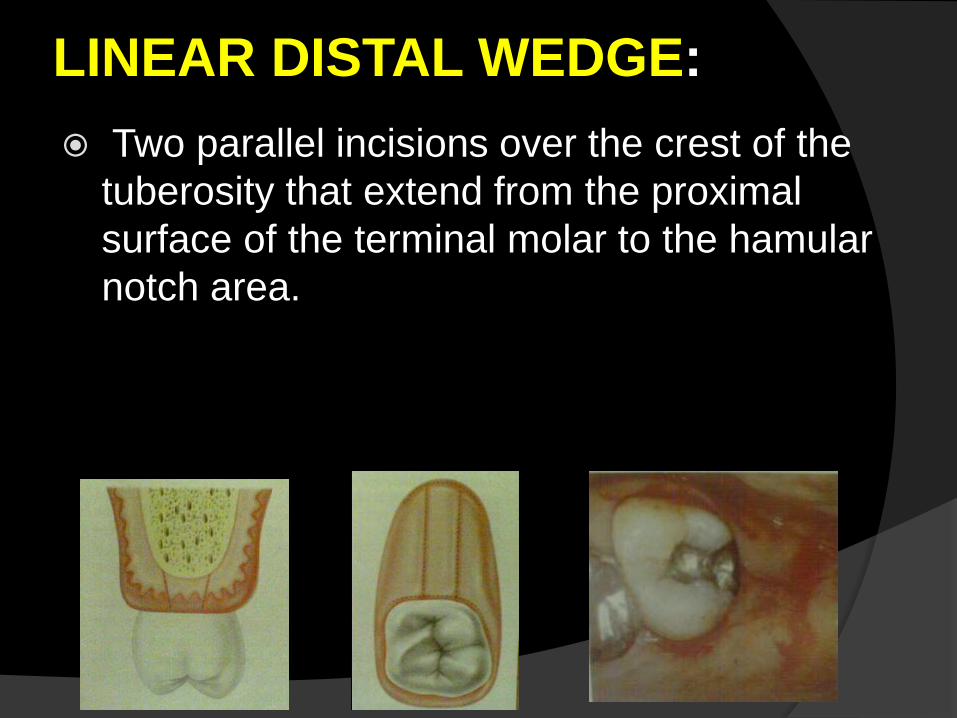
LINEAR DISTAL WEDGE:
Two parallel incisions over the crest of the
tuberosity that extend from the proximal
surface of the terminal molar to the hamular
notch area.
Instruments used
no.15 blade
Periosteal elevators
Kirkland or orban knives
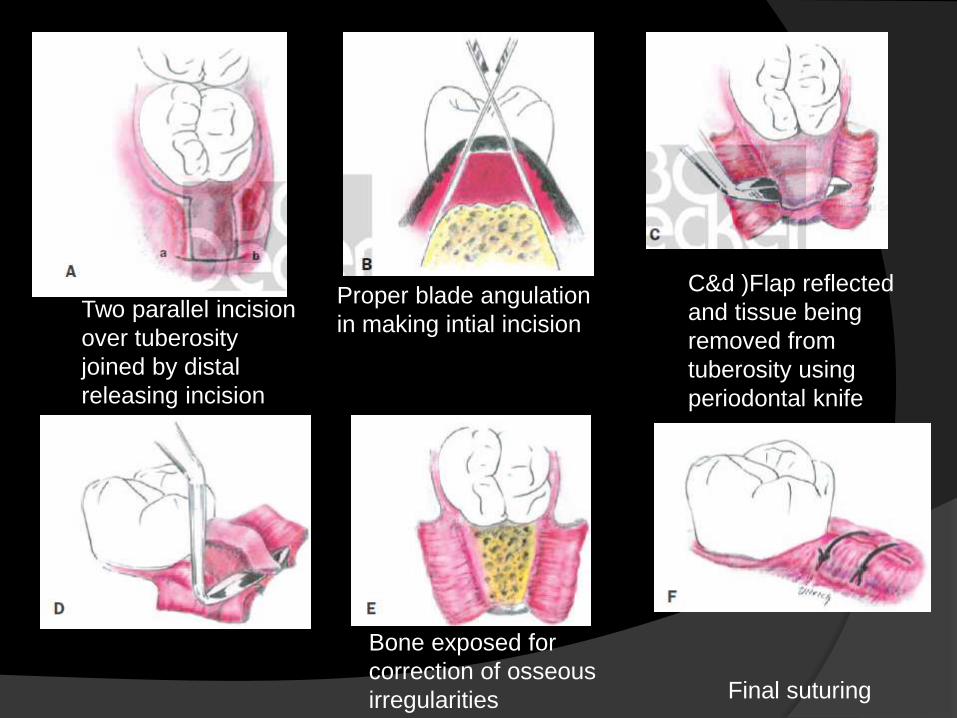
Two parallel incision
over tuberosity
joined by distal
releasing incision
Proper blade angulation
in making intial incision
C&d )Flap reflected
and tissue being
removed from
tuberosity using
periodontal knife
Bone exposed for
correction of osseous
irregularities Final suturing
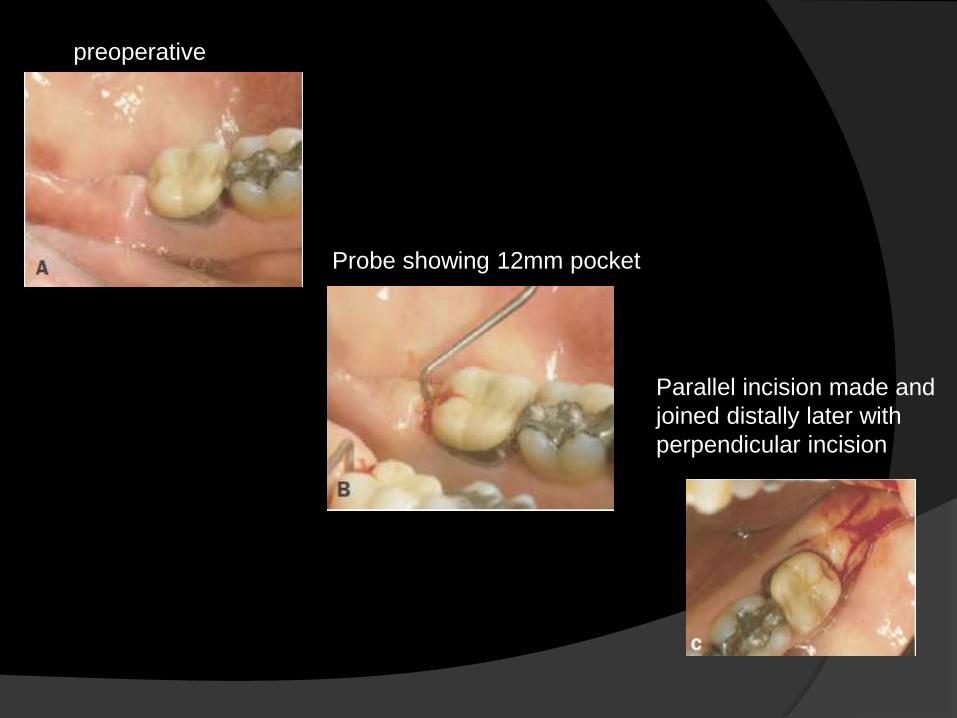
preoperative
Probe showing 12mm pocket
Parallel incision made and
joined distally later with
perpendicular incision
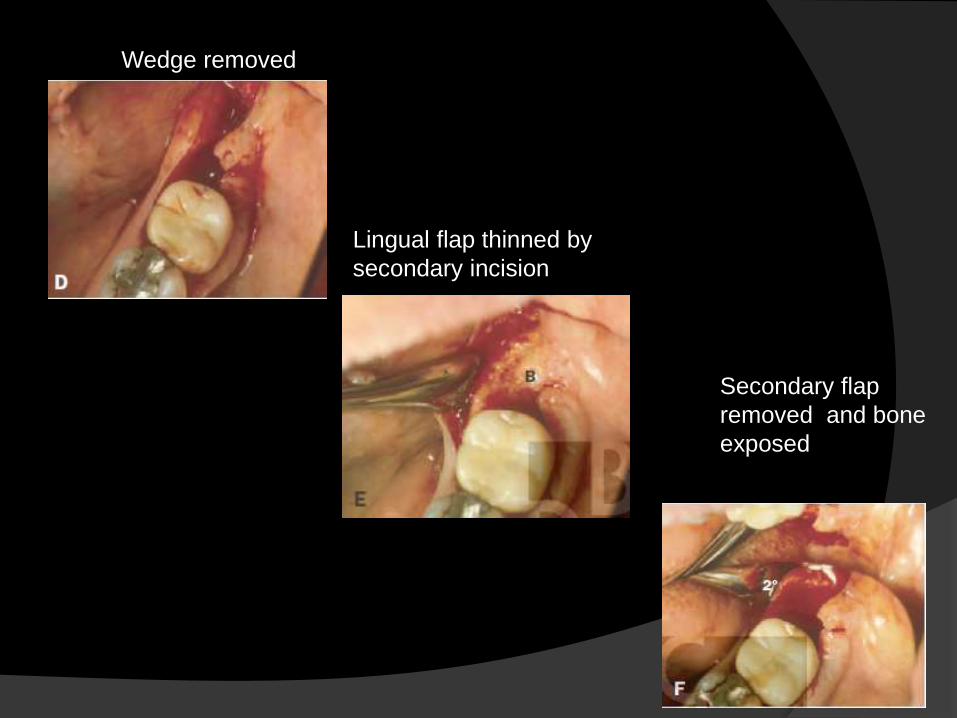
Wedge removed
Lingual flap thinned by
secondary incision
Secondary flap
removed and bone
exposed
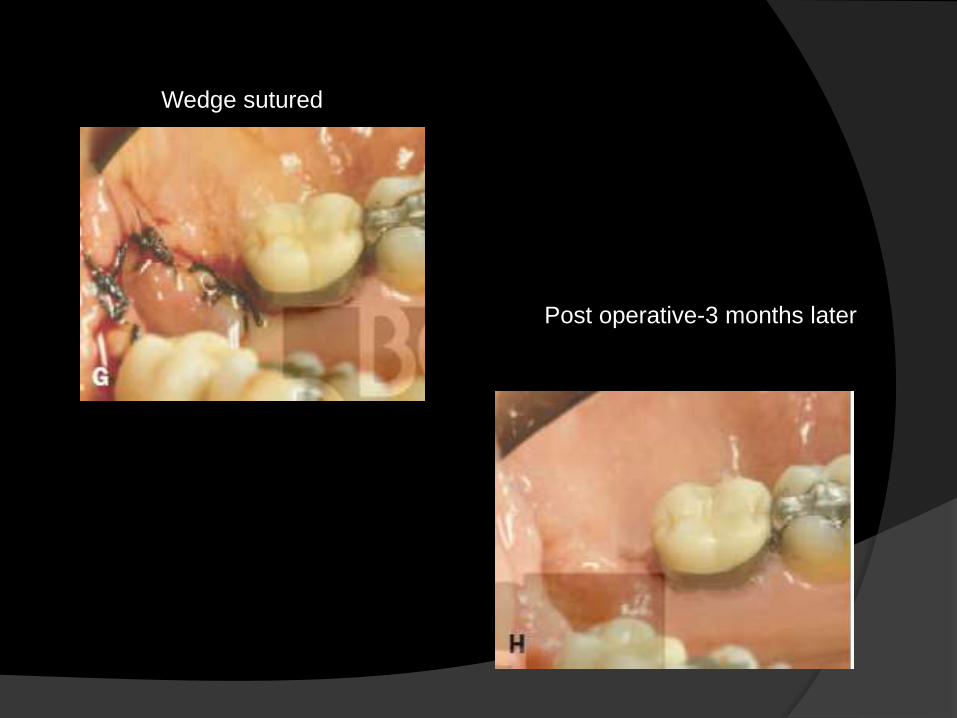
Wedge sutured
Post operative-3 months later
PERIODONTAL PACKS
Periodontal dressing or periodontal
packs is a productive materials applied
over the wound created by periodontal
surgical procedure
minimize postoperative infection and
hemorrhage
Facilitates healing
Protects against pain
Retention of packs Mechanically by interlocking in interdental
spaces and joining the facial and lingual portion
of the pack
Antibacterial properties
Improved healing and patient comfort –
incorporating antibiotics
Bacitracin, oxytetracycline , neomycin
nitrofurazone(hypersensitivity)
Instructions for patients after
surgery
1. The pack should remain in place until it
is removed in the office at the next
appointment
2. For the first three hours after the
operation avoid hot foods to permit the
pack to harden
3. Do not smoke
4. Do not brush over the pack
Postoperative complication
Persistent bleeding after surgery – pack
removed , bleeding stopped with
pressure ,electro surgery ,
electrocautery
Sensitivity to percussion-
Swelling- soft painless swelling in the
cheek , lymphadenopathy
Feeling of weakness
Removal of periodontal
pack After 1 week
Inserting a surgical hoe along the
margin and exert gentle lateral pressure
Pieces of pack- removed with scalers
Entire area rinsed with peroxide to
remove superficial debris
Findings at pack removal
Epithelialized but bleed readily when
touched
Pockets should not be probed
HEALING AFTER FLAP
SURGERY
Immediately after suturing (0 to 24
hours),established by a blood clot, which
consists of a fibrin reticulum with many
polymorph nuclear leukocytes, erythrocytes,
debris of injured cells, and capillaries at the
edge of the wound.
One to 3 days after flap surgery, the space
between the flap and the tooth or bone is
thinner, and epithelial cells migrate over the
border of the flap
One week after surgery‐The blood clot is
replaced by granulation tissue derived from
the gingival connective tissue, the bone
marrow, and the periodontal ligament.
Two weeks after surgery , collagen fibers
begin to appear parallel to the tooth
surface. Union of the flap to the tooth is
still weak, owing to the presence of
immature collagen fibers, although the
clinical aspect may be almost normal.
One month after surgery, a fully
epithelialized gingival crevice with a
well‐defined epithelial attachment is
present. There is a beginning functional
arrangement of the supra crestal fibers
conclusion
The entire surgical procedure should be planned in every detail before intervention is begun. This include type of flap ,exact location ,type of incisions , management of underlying bone and final closure of flap and suture
Although some details may be modified during actual performance of the procedure detailed planning allows for a better clinical result.
Reference
Atlas of cosmetic and reconstructive
periodontal surgery- EDWARDS
COHEN 3rd edition
Carranza’s Clinical periodontology –
NEWMANN , TAKEI ,CARRANZA- 9th
edition