Embed Size (px)
Citation preview
243
A Review of Longitudinal Studies ThatCompared Periodontal TherapiesWayne B. Kaldahl, * Kenneth L. Kalkwarf, t and Kashinath D. Patil*
THERE HAVE BEEN NUMEROUS longitudinal periodontal studies that have compared theeffects of two or more therapies on various clinical parameters. These studies are reviewed and their results are compiled. Both surgical and non-surgical therapy producedimprovement in periodontal health. Surgical therapy tended to create greater short-termprobing depth reduction than non-surgical therapy; however, the advantage was lost insome studies over time. In shallow probing depths, surgery produced a greater loss ofprobing attachment than non-surgical therapy. In deeper probing sites, the short-termresults comparing mean probing attachment change following non-surgical and surgicaltherapy were mixed. In most studies, no long-term differences in mean probing attachment level change were present between non-surgical and surgical therapy. There wereno differences between surgical and non-surgical therapy in any of the gingival inflammatory indices. J Periodontal 1993; 64:243-253.
Key Words: Follow-up studies; periodontal diseases/surgery; periodontal diseases/therapy.
Longitudinal studies have documented not only the immediate, but also the long-term clinical results following several types of periodontal therapy. Treatment methods havebeen compared by their therapeutic effects on the clinicalparameters traditionally utilized in periodontal evaluation.These parameters have included probing depth, probing attachment level, gingival recession, inflammatory indices(gingival index, Ramfjordperiodontal index, bleedinguponprobing, presence of suppuration), plaque accumulation,tooth mobility, andmolarfurcation involvement. Moststudieshave attempted to collect initial clinical measurements in astandardized method. The therapies to be evaluated havethen been performed with subsequent supportive care ofvarying duration. Clinical data collection has occurred atvarying periods post-therapy and during maintenance. Thispaper reviews the longitudinal studies that have comparedtwo or more therapeutic approaches within their experimental design. For the sake of simplification, the studiesare often identified by their geographic location. Also acompilation of the studies grouped by their reported therapeutic effects on each clinical parameter is included.
REVIEWRamfjord and coworkersI were the first to prospectivelycompare and report the longitudinal clinical results follow-
"Department of Periodontics, University of Nebraska Medical Center,College of Dentistry, Lincoln, NE.
'University of Texas Health Science Center, Dental School, San Antonio,TX.
*Universityof Nebraska Medical Center, College of Medicine, Omaha, NE.
ing various periodontal therapy modalities on a large groupof patients over an extended period of time. Their workbegan to focus the profession on the long-term rather thanthe short-term results of treatment. Two groups of patientswere initially treated in their first study. One group receivedgingival curettage and the other received pocket eliminationsurgery (gingivectomy or flap with osseous resectional surgery). After 2 years, the study format changed to a splitmouth design, with two or more therapies performed indifferent regions of each subject's mouth. This approachreduced the biological variability inherent in other studydesigns. Most subsequent investigators have followed thissplit mouth format.
Michigan StudiesThe Michigan Study I reported data from a subset of patients and compared the response following gingival curettage to that following pocket elimination surgery.P Later,the Michigan Study II reported data from patients treatedin a split mouthdesignwith gingival curettage, pocketelimination surgery, and modified Widman surgery.3 This second report included some of the patients treated in theMichigan Study I. The final report of the Michigan StudyII included 72 patientswho had completed5 years of maintenance care and 43 patients who had completed 8 years."Periodontal sites were grouped for analyses according toseverity of periodontal involvement as defined by the initialprobing depth. The results of therapy related to tooth typeswere also reported." The therapeutic impact of initial nonsurgical instrumentation (Phase 1 therapy) on the clinical
244 A REVIEW OF LONGITUDINAL PERIODONTAL THERAPY STUDIESJ Periodontol
April 1993
parameters was not separatedfrom that of the surgical phaseof therapy in Michigan Studies I and II.
The Michigan Study III used a split mouth design tocompare root planing, gingival curettage, modified Widman surgery, and pocket elimination or reduction surgery.Initial therapy was performed and its effect on the clinicalparameters was analyzed prior to the initiation of the surgical and maintenance phases." The first paper from theMichigan Study III reported results from 90 patients whohad completed 2 years of maintenance care,? Subsequentpapers documented results from 72 patients following completion of 5 years of maintenance.S?
Swedish StudiesA group of longitudinal studies from Sweden comparedseveral types of periodontal therapy. The Sweden Study Icompared apically positioned flap with osseous resection,apically positioned flap without osseous resection, Widmanflap with osseous resection, Widman flap without osseousresection, and gingivectomy. Five parallel groups of 10patients each received one of the therapeutic modalities.Clinical sites around single rooted teeth and the mesial aspects of mandibular molars were evaluated. The surgicalphasewas followed by frequent maintenance therapy. Sweden Study I first reported results 2 years post-therapy'? witha subsequent report following 6 years of maintenance care.11
A similar parallel study was conducted with each of fivepatients receiving one of the above therapies and a 24month follow-up. No professional maintenance therapywasprovided. 12
The Sweden Study II included 15 patients who receivedroot planing alone and root planing with modified Widmansurgery in a split mouth design. The first papers from Sweden Study II reported results 2 years post-therapy,13,14 witha subsequent paper reporting the results from 11 patientswho completed 5 years of maintenance."
The Sweden Study III involved 15 patients who receivedroot planing, modified Widman surgery, and modifiedKirkland flap surgery in a split mouth design. The caseswere observed for one year. The role of granulation tissuein the healing response was determined by leaving it intactat some surgical sites.'?
The Sweden Studies IV and V compared root planing,gingivectomy, apically positioned flap, apically positionedflap with bone recontouring, modified Widman, and modified Widman with bone recontouring in a split mouth design. Clinical results were reported following a duration of6 months. The first paper included results from 16 patients," and the second reported findings from 39 patients. 18
Washington StudyThe Washington Study compared apically positioned flapsurgery with and without osseous recontouring in a splitmouth design. The first report from this study includedresults from 12 patients after 6 months of follow-up.19 Asubsequent paper included findings from eight patients after
5 years of maintenance. i" The Washington Studywent intogreat detail to define the osseous resection surgical technique used, since questions had been raised regarding theactual osseous surgical techniques performed in prior studies.
Minnesota StudyThe Minnesota Study compared root planing and modifiedWidman surgery in a split mouth design on 17 patients.The first results were reported 4 years following the completion of periodontal therapy,21 with a subsequent reportof 10 patients following 61/ 2 years of maintenance care."The clinical differences between the responses of molarandnonmolar teeth from the same study were also publishedfollowing 61/ 2 years of maintenance."
Denmark StudyThe DenmarkStudy compared root planing, modified Widman surgery, and reverse bevel apically positioned flapsurgery in 17 patients utilizing a split mouth design;" Molarswere not included in the evaluation. The initial paper fromthis study discussed results 6 months after therapy.24 Afollow-up paper reported on 16 patients completing 5 yearsof maintenance."
Lorna Linda StudySeveral therapeutic studies have been reported from theLorna Linda group. Two studies compared therapies performed on designated isolated defects in a split mouth design. The first study compared results 6 months followingflap surgery with and without partial osseous resection of26 defects in 16 patients. Citric acid root treatment wasutilized in conjunction with both procedures." The secondstudy compared the results following root planing to thosefollowing flap surgery with citric acid root treatment in 50defects from 14 patients. Results were reported 6 months"and 5 years following therapy.28
Three other studies from Loma Linda assessed findingsfrom patients who initially performed only plaque controlfor varying periods (i.e., 1 to 8 months) and subsequentlyreceived root planing. These studies involved 7 to 16 patients each, included no molars, and were 13 to 24 monthsin duration. The effects of plaque control alone and thesubsequent root planing were compared. P>"
Arizona StudyThe Arizona Study was undertaken in a private practicesetting in part to dispel concerns regarding the relevance oflongitudinal studies to a private practice situation. Sixteenpatients were treated with initial therapy followed by rootplaning, modified Widman surgery, and flap with osseousresectional surgery in a split mouth design. Clinical resultswere reported following one year of maintenance."
Nebraska StudyThe Nebraska Study compared coronal scaling (nosubgingival instrumentation), root planing, modified
. I
i
Volume 64Number 4
Widman surgery, and flap with osseous resectional surgery performed in a split mouth design. Vertical and horizontal probing attachment level changes in the furcationregion of molars were also evaluated. Results were initially reported following 2 years of maintenance care on75 patients. P v"
Other StudiesThree studies of short duration were published in the late1970s comparing various types of therapy. Zarner" compared gingival curettage, replaced flap surgery, apicallypositioned flap with osseous resectional surgery, and initial therapy alone. Thirty-nine patients were treated in asplit mouth design and then followed for 4 months. Waite"?compared root planing and gingivectomy in a split mouthstudy involving 28 patients followed for 48 weeks. Aeschlimann et al.40 compared apically positioned flap surgery with and without osseous recontouring in a splitmouth design involving 10 patients treated and followedfor 4 months.
Payot et al.41 compared root planing, modified Widmansurgery, flap with "smoothed bone and odontoplasty," andno treatment in 38 lower molar furcations from 16 patients.Some patients had two therapies on individual molars whileothers had one therapy. Results were reported for up to 1year follow-up.
Schroer et al.42 compared root planing in 12 facial ClassII molar furcations and open flap debridement in 13 similarfurcations that involved 15 patients. Surgical therapy wasperformed after 4 months of initial therapy and followedby a 12-month maintenance period.
Two short-termstudies compared only plaque control andplaque control coupled with root planing in split mouthdesigns. One involved 12 patients followed for 25 weekspost-therapy with six of the patients receiving tetracyclinetherapy.43.44 In addition to the usual periodontal clinicalparameters, microbiological assessment of the crevice andhistological evaluation of the gingiva were completed. Thesecond study evaluated data obtained from three designatedsites in each of 22 patients during a 2-month period." Siteswere shallow supra bony pockets and were evaluatedhistologically.
Most recent studies have grouped data according to theseverity of the initial probing depth (i.e., 1 to 3 rnm, 4 to6 mm, and ;::.7 mm) at each site. This approach capturesthe effects of therapy on comparable periodontal situationsand allows for more accurate therapeutic documentation.Therapies have been contrasted by comparing 1) the meanchanges of clinical parameters; 2) the frequency distributions of sites for a clinical parameter; or 3) the prevalenceof a parameter.
Numerous other studies have documented the successful effects of a particular periodontal therapy longitudinally but did not include comparison to other therapeuticapproaches. These studies have not been included in thisreview.
KALDAHL, KALII...VARF, PATIL 245
RESULTSThe following is a summary of studies grouped accordingto the effects compared for each clinical parameter. Presentation is grouped by short-term (:51 year post-therapy)or long-term (;::. 5 years post-therapy) results.
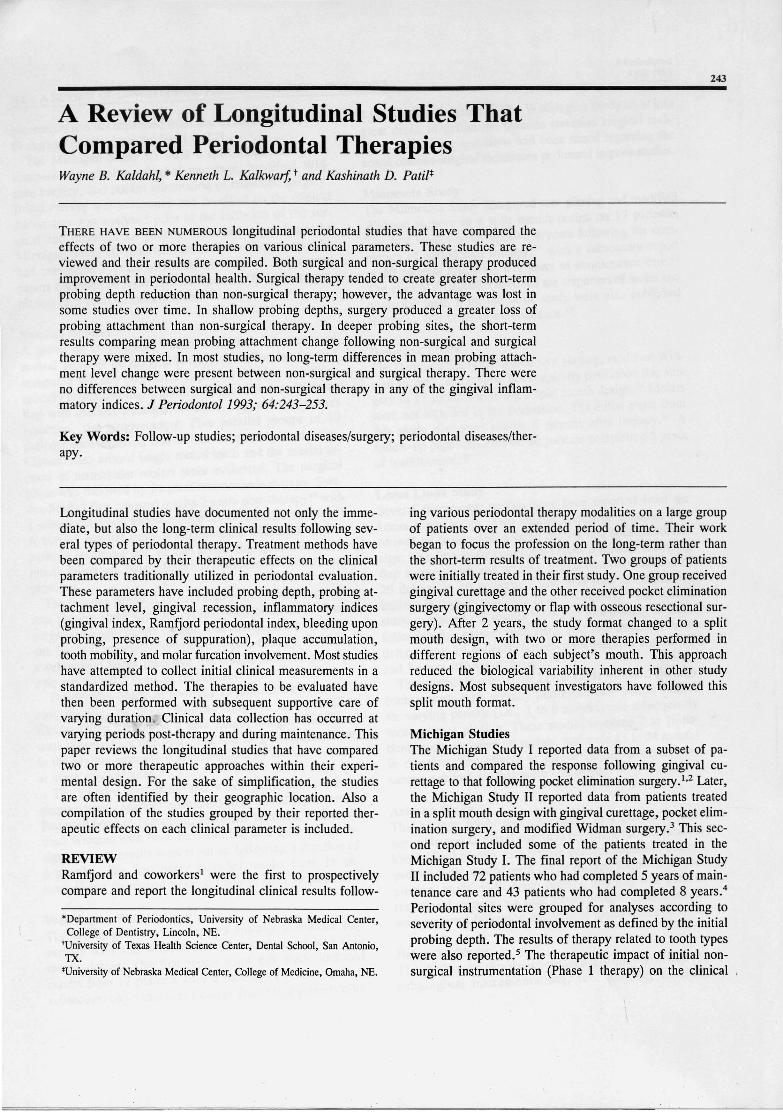
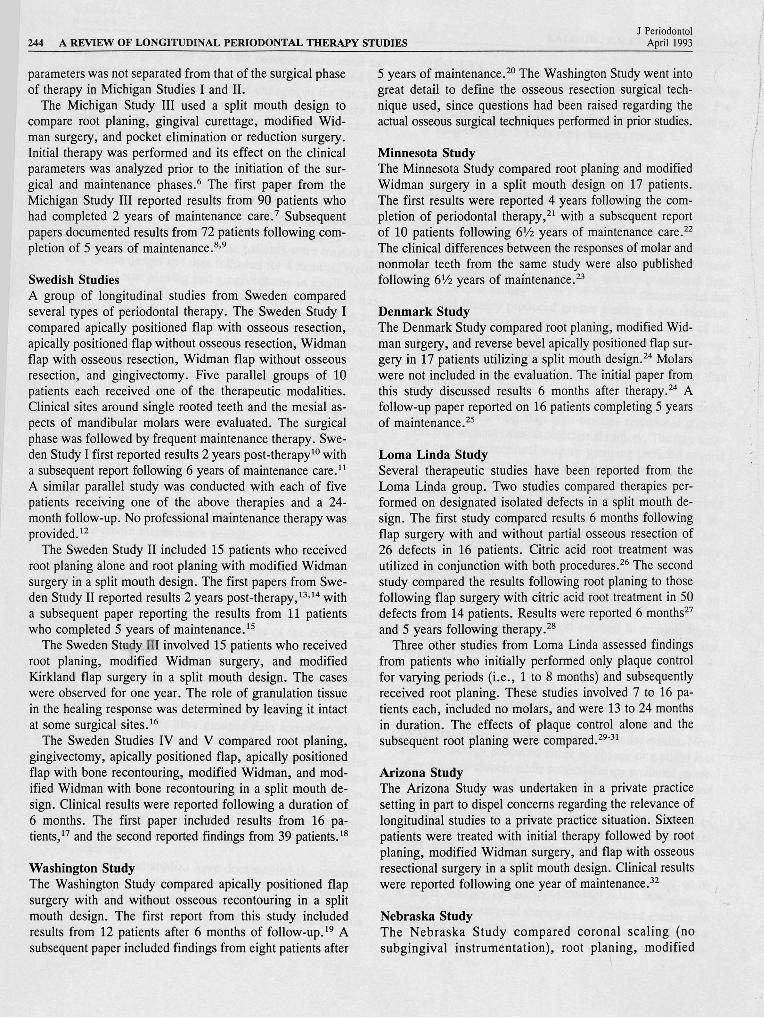
Probing DepthTable 1 summarizes the studies that compared non-surgicaland surgical therapies according to probingdepthreduction." Non-surgical therapy" usually consisted of root planingbut in some instances also included gingival curettagc'v-""Surgical therapy" included flap with or without osseousresection (i.e., modified Widman, flap with osseous resection, pocket elimination surgery, apically positioned flap,etc.). Several studies2,4,7,13,21 ,24,27,32,33,38,39demonstrated thatsurgical therapy produced greater probing depth reductionthan non-surgical therapy over the short-term. Some of theearly differences diminished during long-term follow-up;however, some studies2,4,8,22,28 showed that the surgicallytreated sites retained greater probing depth reduction thandid non-surgical sites.
Table 2 presents studies which compared probing depthreduction following flap with osseous resectional surgeryand flap without osseous resectional surgery. The flapwithout osseous resectional surgery grouping included severalclinical procedures (modified Widman surgery, flap curettage, apically positioned flaps, etc.). Some studies4,7, I0,17-19,32showed no differences during short-term follow-up, whileothers4,7,26,33,38,40 demonstrated that regions treated with osseous resection had greater reduction of probing depth. Onlyone study" reported a significant difference between therapygroups following 5 years.
All studies which compared the effects of plaque controlalone to the effects of root planing and plaque control onprobing depth reduction reported similar results. Plaquecontrol alone produced a slight decrease in probing depth,however, the addition of root planing resulted in much greaterreduction.29-31,33,43-45
Probing Attachment LevelThe effects of non-surgical and surgical therapy on probingattachment levels were comparedin shallow sites (:5 3 mm)by several studies. All studies reported similarresults. Nonsurgical therapy produced either no change or a slight lossof probing attachment while surgical therapy produced greaterloss. This was true for studies of shorr, 7,13,16-18,21,32 andlong duration.4,8,22
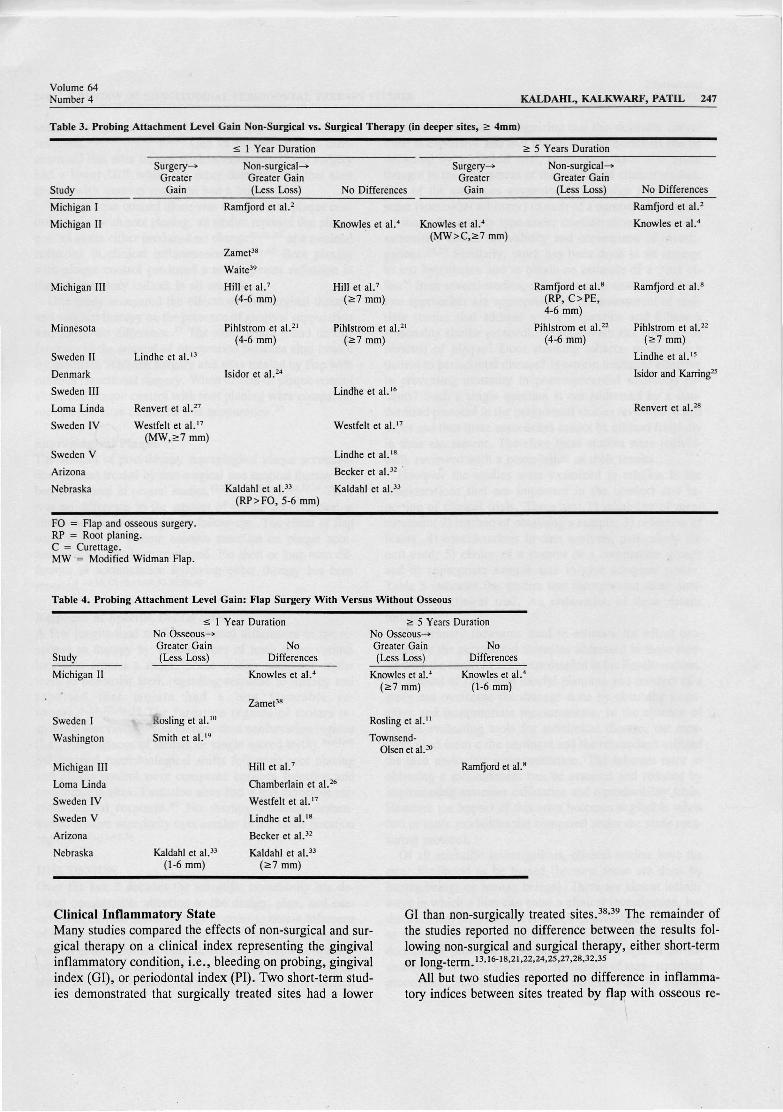
Table 3 presents the studies that compared the effects ofnon-surgical and surgical therapy on probing attachmentlevel gain in initially deeper sites (;::. 4 mm). A fewstudies13,17,27reported that surgeryproduced a greater probing attachment level gain during short-term follow-up, whilea larger number of studies2,4.7,16-18,21,24,32,33,38,39 demon-strated that non-surgical therapy either produced greater gainor that no differences could be discerned. In the studies thatshowed surgery producing greater gain, the surgical mo-
246 A REVIEW OF LONGITUDINAL PERIODONTAL THERAPY STUDIES
Table 1. Probing Depth Reduction: Non-Surgical Versus Surgical Therapy
~ 1 Year Duration <": 5 Years Duration
J PeriodontolApril 1993
Study
Michigan I
Michigan II
Michigan III
Minnesota
Sweden II
Denmark
Sweden III
Lorna Linda
Sweden IV
Sweden V
Arizona
Nebraska
Surgery-»Greater t
Ramfjord et al.2
Knowles et al." (1-6 rnrn)"
Zamet" (FO> RP,C)
Waite)9
Hill et al.7
Pihlstrom et a1.2' (<": 4 mm)
Lindhe et al. 1J
Isidor et al.24
Renvert et alY
Becker et al.)2
Kaldahl et al.J3
NoDifferences
Knowles et al." (<":7 mm)
Zamet' " (C = MW)
Pihlstrom et al.2I (1-3 mm)
Lindhe et al.16
Westfelt et al.!?
Lindhe et al.18
Surgery-»Greater t
Ramfjord et al.2
Knowles et al." (4-6 mm)
Ramfjord et al." (4-6 mm)
Pihistrom et al.22 (<":7 mm)
Renvert et al.28
NoDifferences
Knowles et al." (1-3, <": 7 mm)
Ramfjord et al." (1-3, <": 7 mm)
Pihistrom et al.22 (1-6 mm)
Lindhe et al."
Isidor and Karring >
* Special situations regarding certain therapies or severity categories.FO= Flap and osseous surgery.RP= Root planing.C = Curettage.MW= Modified Widman flaps.
Table 2. Probing Depth Reduction: Flap Surgery With Versus Without Osseous
StudyOsseous-»Greater t
~ 1 Year DurationNo
DifferencesOsseous-»Greater t
<": 5 Years DurationNo
Differences
Michigan II
Sweden I
Washington
Michigan III
Lorna Linda
Sweden IV
Sweden V
Arizona
Nebraska
Knowles et al." (1- 3 mm)
Zarnet"
Aeschlimann et al.40
Hill et al.? (1-6 mm)
Chamberlain et al.26
Kaldahl et al.))
Knowles et al." (> 4 mm)
Rosling et al.10
Smith et al.19
Hill et al.7 (<":7 mm)
Westfelt et al.!?
Lindhe et al. I'
Becker et al.32
Townsend-Olsen et al.20
Knowles et al.4
Rosling!'
Ramfjord et al.'
dality was a modified Widman flap or similar surgical approach. Long-term follow-up demonstrated that some of theprobing attachment gains were lost during the maintenanceperiod. Most long-term studies reported no differences between the results following non-surgical and surgicaltherapy.2.4.8 ,15, 22,25, 28
Studies that compared the effects of flap surgery withand without osseous resection on the probing attachmentlevel are presented in Table 4. Some studieslO, 19 ,33 reportedthat sites treatedwith flap surgerywithout osseous resectionhad more short-term probing attachment level gain thansites treated with osseous resection, while
others4,7, 17, 18,26,32,33,38 reported no difference. Two longterm studies'J -'" and the ~ 7 mm sites in a third study"demonstrated that flap surgery without osseous resectionproduced greater probing attachment level gain than flapsurgery with osseous resection.
Several studies, all of short duration, comparedtheeffectof plaque control alone to the effect of root planing andplaque control on probing attachment levels. All except onereported that either no differences existed between studygroups or root planing producedgreater probingattachmentgain.29,3 1,33,43-45 A mean loss of probing attachment occurred at sites treated by plaque control alone in one study."
Volume 64Number 4
Table 3. Probing Attachment Level Gain Non-Surgical vs. Surgical Therapy (in deeper sites, 2: 4mm)
KALDAHL, KAL KWARF , PATIL 247
Study
Michigan I
Michigan II
Michigan III
Minnesota
Sweden II
Denmark
Sweden III
Lorna Linda
Sweden IV
Sweden V
Arizona
Nebraska
$ 1 Year Duration
Surgery-» Non-surgical-« Surgery-»Greater Greater Gain Greater
Gain (Less Loss) No Differences Gain
Ramfjord et al.2
Knowles et al." Knowles et al.4
(MW>C,2:7 mm)
Zarnet-"
Waite"
Hill et al.7 Hill et at.'(4-6 mm) (2:7 mm)
Pihlstrom et al.2' PihIstrom et al.2'(4-6 mm) (2:7 mm)
Lindhe et al. 13
Isidor et al.24
Lindhe et al. i s
Renvert et al.27
Westfelt et al. '7 Westfelt et al."(MW,2:7 mm)
Lindhe et al. '"Becker el al.)2 '
Kaldahl et al.33 Kaldahl et al.33
(RP> FO, 5-6 mm)
2: 5 Years Duration
Non-surgical-»Greater Gain(Less Loss)
Ramfjord et al."(RP, C >PE,4-6 mm)
Pihlstrom et al.22(4-6 mm)
No Differences
Ramfjord et al.2
Knowles et al. "
Ramfjord et al."
Pihlstrom et al.22
(2:7 mm)
Lindhe et al. 15
Isidor and Karring"
Renvert et al.2"
FO = Flap and osseous surgery.RP = Root planing.C = Curettage.MW '= Modified Widman Flap.
Table 4. Probing Attachment Level Ga in: Flap Surgery With Versus Without Osseous
Study
$ 1 Year DurationNo Osseous-»Greater Gain No(Less Loss) Differences
2: 5 Years DurationNo Osseous-»Greater Gain No(Less Loss) Differences
Michigan II
Sweden I
Washington
Michigan III
Lorna Linda
Sweden IV
Sweden V
Arizona
Nebraska
Rosling et al.10
Smith et al. !"
Kaldahl et al.33
(1-6 mm)
Knowles et al.4
Zamet?"
Hill et al.7
Chamberlain et al.2.
Westfelt et al. ·7
Lindhe et al.!"
Becker et al.32
Kaldahl et al.33
(2:7 mm)
Knowles et al.'(2:7 mm)
Rosling et aI."
TownsendOlsen et aI.:D
Knowles et al."(1-6 mm)
Ramfjord et al."
Clinical Inflammatory StateMany studies compared the effects of non-surgical and surgical therapy on a clinical index representing the gingivalinflammatory condition, i.e. , bleeding on probing, gingivalindex (GI), or periodontal index (PI). Two short-term studies demonstrated that surgically treated sites had a lower
GI than non-surgically treated sites.38 ,39 The remainder ofthe studies reported no difference between the results following non-surgical and surgical therapy, either short-termor long_term. 13, 16-18,2 1,22,24 ,25 ,27 ,28,32,35
All but two studies reported no difference in inflammatory indices between sites treated by flap with osseous re-

248 A REVIEW OF LONGITUDINAL PERIODONTAL THERAPY STUDIESJ Periodontal
April 1993
sectional surgery and those treated by flap without osseousresection. IO,II,17,18,19,20,32,35 One of the two studies dem-onstrated that sites treated with osseous resectional surgeryhad a lower GI40 while the other demonstrated that sitestreated with osseous resection had a higher GI.38
When plaque control alone was compared to plaque control coupledwith root planing, all studiesreported that plaquecontrol alone either produced no change29,31 ,43 or a minimalreduction in clinical inflammation.30,35,44,45 Root planingwith plaque control produced a much greater reduction inthe inflammatory indices in all studies.
One study compared the effects of non-surgical therapyand surgical therapy on the presence of gingival suppurationand found no difference.?? The same study found no differences in the amount of suppuration between sites treatedby modified Widman surgery and sites treated by flap withosseous resectional surgery. When effects of plaque controlalone and plaque control with root planing were compared,root planed sites exhibited less suppuration.??
Supragingival PlaqueThe amount of post-therapy supragingival plaque accumulation in areas treated by non-surgical and surgical therapy hasbeen compared in several studies.13,16-18,21,22,24,25,32,37-39 Therewas no difference in the amount of plaque accumulation ateither short-term or long-term follow-ups. The effect of flapsurgery with or without osseous resection on plaque accumulation also has been compared. No short or long-term difference in accumulation following either therapy has beenreported. 10.11 ,1 7,18,1 9,20,32,37,38,40
Response at Specific Dental SitesA few longitudinal studies evaluated differences in the response to therapy by various types of teeth or by variouslocations around a tooth. Some studies compared molarteeth to nonmolar teeth regarding response to therapy andreported that molars had a less favorable response.5,13,23,36,46 The furcation regions of molars responded less favorably to therapy than nonfurcation regions(i.e., flat surfaces of molars or single rooted teeth).36,47,48Subgingival microbiological shifts following root planingand plaque control were compared between furcation andnonfurcation sites. Furcation sites had a less favorable microbiological response.f? No therapy modality demonstrated relativesuperiorityover another in the molar furcationregion,34,36,41,42,50
DISCUSSIONOver the last 2 decades the scientific community has devoted considerable attention to the design, plan, and execution of clinical investigations in order to obtain inferenceof maximum durability or credibility." Although many important guidelines have been developed to improve specifictypes of studies, it is well accepted that the best way toobtain durability is through a study type commonly referred
to as a clinical trial. Recognizing that this desirable instrument is expensive and that not all clinical questions can beanswered by a clinical trial, researchers have also giventhought to the assessment of the validity of clinical studies.One of the strategies suggested is to assign a numericalscore (somewhat arbitrary) to each of a number of desirableattributes for a study type under consideration, and use thesummative scores for validity and comparison of .investigations.52,53 Similarly, work has been done in an attemptto test hypotheses and to obtain an estimate of a " net effect" from several studies, called the meta-analysis.54 Thesetwo approaches are appropriate for the assessment of multiple studies that address a single question and follow areasonably similar protocol. Is mouthwash xxx effective inremoval of plaque? Does smoking tobacco predispose apatient to periodontal disease? Is aspirin treatment effectivein preventing mortality in post-myocardial infarction patients? Such a single question is not addressed by a standardized protocol in the periodontal studies reviewed in thispaper and thus these approaches cannot be utilized fruitfullyin their assessment. Therefore these studies were individually reviewed with a compilation of their results.
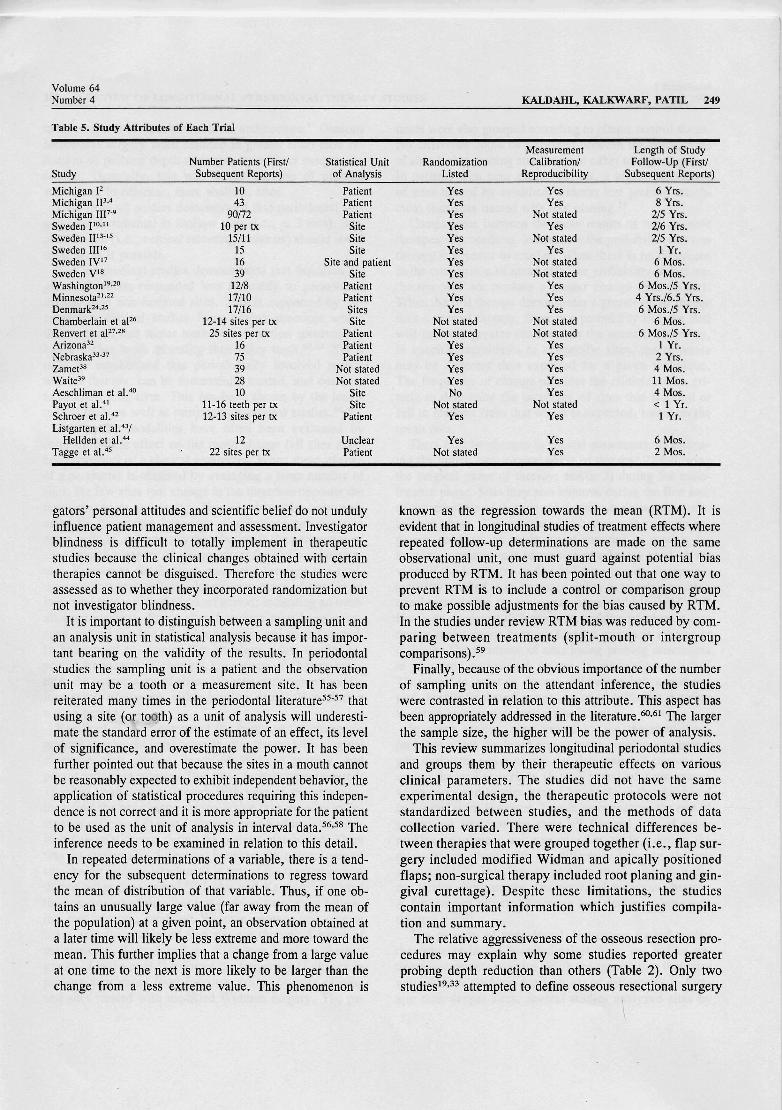
However the studies were examined in relation to theconsiderations that are important in the conduct and reporting of clinical trials. These are: 1) reliability of measurement; 2) method of obtaining a sample; 3) reduction ofbiases; 4) considerations in data analysis, particularly theunit used; 5) choice of a control or a comparison group;and 6) appropriate sample size to give adequate power.Table 5 indicates the studies that incorporated these attributes of a clinical trial. An elaboration of these detailsfollow.
The primary measures used to estimate the effect produced by the periodontal therapies addressed in these studieswere the clinical parameters detailed in the Results section.No amount of otherwise careful planning and conduct of astudy can overcome the damage done by obtaining insensitive and inappropriate measurements. In the absence ofprecise evaluating tools for subclinical disease, the measures used seem quite pertinent and the researchers utilizedthe then up-to-date instrumentation. The inherent error inobtaining a measurement can be assessed and reduced byimplementing examiner calibration and reproducibility trials.However the impact of this error becomes negligible whentwo or more modalities are compared under the same measuring protocol.
Of all scientific investigations, clinical studies have themost likelihood to be biased (because these are done byhuman beings on human beings). There are almost infiniteways in which a bias can enter a clinical investigation, butthere are two broad stages at which an investigator attemptsto control for bias. Obtaining the sampling units by randomization provides reasonable protection against an assemblybias and also legitimizes application of manystatisticalprocedures. Secondly, blindness ensures that the investi-
{
\
Volume 64Number 4 KALDAHL, KALKWARF, PATIL 249
Ta ble 5. Study Attribu tes of Each Trial
Measurement Length of StudyNumber Patients (First/ Statistical Unit Randomization Calibration/ Follow-Up (Firs t!
Study Subsequent Reports) of Analysis Listed Reproducibility Subsequent Reports)
Michigan F 10 Patient Yes Yes 6 Yrs.Michigan IP " 43 Patient Yes Yes 8 Yrs.Michigan IIF·9 90/72 Patient Yes Not stated 2/5 Yrs.Sweden 110• 11 10 per IX Site Yes Yes 2/6 Yrs.Sweden II13.ls 15/11 Site Yes Not stated 2/5 Yrs.Sweden III!6 15 Site Yes Yes 1 Yr.Sweden IV'7 16 Site and patient Yes Not stated 6 Mos.Sweden V' 8 39 Site Yes Not stated 6 Mos.Wasbington"-" 12/8 Patient Yes Yes 6 Mos./5 Yrs.Minnesota-I-" 17110 Patient Yes Yes 4 Yrs./6.5 Yrs.Denmark24.2s 17/16 Sites Yes Yes 6 Mos. /5 Yrs.Chamberl ain et aF6 12-14 sites per IX Site Not stated Not stated 6 Mos.Renvert et aF7.28 25 sites per IX Patient Not stated Not stated 6 Mos./5 Yrs.Arizona" 16 Patient Yes Yes 1 Yr.Nebraska'>" 75 Patient Yes Yes 2 Yrs.Zamet ?" 39 Not stated Yes Yes 4 Mos.Waite39 28 Not stated Yes Yes 11 Mos.Aeschliman et a!' 40 10 Site No Yes 4 Mos.Payot et a!.41 11-16 teeth per IX Site Not stated Not stated < 1 Yr.Schroer et a!.42 12-13 sites per IX Patient Yes Yes 1 Yr.Listgarten et a!' 43/
Hellden et a!' 44 12 Unclear Yes Yes 6 Mos.Tagge et a!' 4S 22 sites per IX Patient Not stated Yes 2 Mos.
gators' personal attitudes and scientific belief do not undulyinfluence patient management and assessment. Investigatorblindness is difficult to totally implement in therapeuticstudies because the clinical changes obtained with certaintherapies cannot be disguised. Therefore the studies wereassessed as to whether they incorporated randomization butnot investigator blindness.
It is important to distinguish between a sampling unit andan analysis unit in statistical analysis because it has important bearing on the validity of the results. In periodontalstudies the sampling unit is a patient and the observationunit may be a tooth or a measurement site. It has beenreiterated many times in the periodontal literature55.57 thatusing a site (or tooth) as a unit of analysis will underestimate the standard error of the estimate of an effect, its levelof significance, and overestimate the power. It has beenfurther pointed out that because the sites in a mouth cannotbe reasonably expected to exhibit independent behavior, theapplication of statistical procedures requiring this independence is not correct and it is more appropriate for the patientto be used as the unit of analysis in interval data. 56,58 Theinference needs to be examined in relation to this detail.
In repeated determinations of a variable, there is a tendency for the subsequent determinations to regress towardthe mean of distribution of that variable. Thus, if one obtains an unusually large value (far away from the mean ofthe population) at a given point, an observation obtained ata later time will likely be less extreme and more toward themean. This further implies that a change from a large valueat one time to the next is more likely to be larger than thechange from a less extreme value. This phenomenon is
known as the regression towards the mean (RTM) . It isevident that in longitudinal studies of treatment effects whererepeated follow-up determinations are made on the sameobservational unit, one must guard against potential biasproduced by RTM. It has been pointed out that one way toprevent RTM is to include a control or comparison groupto make possible adjustments for the bias caused by RTM.In the studies under review RTM bias was reduced by comparing between treatments (split-mouth or intergroupcomparisonsj."
Finally, because of the obvious importance of the numberof sampling units on the attendant inference, the studieswere contrasted in relation to this attribute. This aspect hasbeen appropriately addressed in the literature. 60 ,61 The largerthe sample size , the higher will be the power of analys is.
This review summarizes longitudinal periodontal studiesand groups them by their therapeutic effects on variousclinical parameters. The studies did not have the sameexperimental design, the therapeutic protocols were notstandardized between studies, and the methods of datacollection varied. There were technical differences between therapies that were grouped together (i.e., flap surgery included modified Widman and apically positionedflaps; non-surgical therapy included root planing and gin gival curettage). Despite these limitations, the studiescontain important information which justifies compilation and summary.
The relative aggressiveness of the osseous resection procedures may explain why some studies reported greaterprobing depth reduction than others (Table 2). Only twostudies19,33 attempted to define osseous resectional surgery
250 A REVIEW OF LONGITUDINAL PERIODONTAL THERAPY STUDIESJ Periodontol
April 1993
to the endpoint of " positive osseous architecture." Osseousresectional surgery often resulted in greater short-term reduction of probing depth than surgery without osseous resection. Generally, this was at the expense of probingattachment in adjacent, more shallow, sites.
Data from all studies demonstrated that periodontal surgery was detrimental in shallow sites (i.e., $ 3 mm). Surgical design (i.e., vertical releasing incisions) should avoidthese areas if possible.
The longitudinal studies demonstrated that furcation regions of molars responded less favorably to periodontaltherapy than non-furcated sites. This is supported by retrospective clinical studies from private practices whichdemonstrated that molar teeth with furcation involvementhad a higher tooth mortality than other teeth.62,63 Yet itmust be emphasized that periodontally involved molarswarrant therapy, can be successfully treated, and continueto function long-term. This has been shown by the longitudinal trials as well as retrospective clinical studies.64,65
Therapeutic modalities have often been evaluated bycomparing their effect on the mean change (all sites averaged together) of a clinical parameter. When mean changeof a parameter is obtained by averaging a large number ofsites, the few sites that change in the direction opposite themean change go undetected. Therapies have also been evaluated by comparing frequency distributions between twoexam periods. A frequency distribution is the percentage ofsites in each category of measurement for a clinical parameter. Frequency distributions compared between two evaluation points may reflect a larger percentage of sites in animprovedcategory at the second period; indicating an overall improvement. Some sites however may have worsened, moved to a less favorable categoryand go undetected.In an attempt to counter this situation a few studies reported frequency of change. Frequency of change separates the percentages of sites that have undergone specificincrements of change, either positive or negative, duringa time period.
Ramfjord et al.8,9 compared the frequency of change inprobingattachment level between sites treatedwith gingivalcurettage, root planing, modified Widman surgery, andpocket reduction surgery. Two time periods were reported:1) initial examination through fifth year of maintenance,including the net change during active therapy plus maintenance care; and 2) year 1 through year 5 of maintenance,including only change during the maintenance period. Therewas no appreciable difference between the percentages ofsites losing probing attachment in any of the therapy groupsduring either time period.P-? Isidor and Karring" reportedthe percentagesof sites that lost probing attachment following root planing, modified Widman surgery and reversebevel apically positioned flap surgery through 5 years ofmaintenance. They found no difference between therapygroups. Lindhe et al.15 reported the frequency of change inprobing attachment level for sites treated by root planingand sites treated with modified Widman surgery. The pa-
tients were also grouped according to plaque control status.No difference could be discerned between the percentagesof sites losing probingattachment in either treatmentgroup.In patients' with poor plaque control, a higher percentageof sites treated by modified Widman lost probing attachment than sites treated with root planing."
Comparisons between the mean results of two or moretherapeuticprocedures demonstrate the probability that onetherapy is superior to another. When there is no differencein the comparison of mean data, the probability is that onetherapy will not produce a greater change than another.When the first therapydemonstrates a greater mean changethan a second therapy, there is a probability that the firstwill create a greater change than the second. However,in specific individuals or at specific sites, the responsemay be different than expected for a given technique.The frequency of change provides the clinician with criteria to determine the incidence of sites that respond orfail to respond from that which is expected, based on themean data.
There may be changes in clinical parameters: 1) following the initial, non-surgical phase of therapy; 2) followingthe surgical phase of therapy; and/or 3) during the maintenance phase. Sites may also improve during the first and/or second phase of therapyand deteriorate during the maintenance phase. The question is whether a therapeutic approach produces an environment superior to another forlong-term maintenance of probing attachment level. A review of the long-term studies indicates that no therapeuticmodalityresulted in an increased ability to maintainprobingattachment during the maintenance period.4,8,11,15,20,22,25,28However, to depict differences in probing attachment lossduring maintenance between therapy groups is inherentlydifficult. The incidence of sites losing probing attachmentin untreated periodontal disease is relatively small.66,67
Therefore, in order to discern differences between therapies, longitudinal studies need to be of sufficient durationto detect enough sites losing attachment.
In some studies, sites treated by the therapeutic approaches which producedgreater mean probing attachmentgain during the active phasesalso demonstrated greater lossduring the earlier periods (1 to 2 years) of maintenancewhen compared to sites treated by therapies that producedless initial gain. However, later in maintenance, the rate ofsubsequent loss was the same.8,28 General loss of meanprobing attachment occurred in other studies during themaintenance phase with no difference between therapygroupS.4,8,15,25 This loss of probing attachment often didnot totally eliminate the gain produced by active therapy.A few studies reported no mean loss during maintenancetherapy.11,20,22
The severity of periodontal destruction varied withinthe subjects in the longitudinal studies, not unlike patients in a private practice. With the recognition that siteswith shallow probing depths respond differently to therapy than deeper sites, several studies analyzed sites by
Volume 64Number 4
grouping them according to their initial probing depth(i.e., 1 to 3 mm, 4 to 6 mm, ~ 7 mm). Usually a largernumber of sites were in the shallower categories. In studies that did not subdivide data by initial probing depth,the magnitude of response may have been affected by themore numerous shallow sites, therapy underestimating ordiluting the response actuallyoccurring in the deeper sites.In studies that did categorize by initial depth, the sameconcern applies to the deeper category (~ 7 mm). Is thetherapeutic effect observed in the more numerous 7 or 8mm sites diluting that of the fewer ~ 9 mm sites? Aquestion remains as to the most appropriate therapy fordeeper regions.
Therapeutic results and comparisons changed over timeas evidenced by comparing the short- and long-term datain the few long-term studies. More clinical studies monitoring long-term results are needed.
When all the results of the periodontal longitudinal studies are considered, the logical therapeutic approach for apatient with periodontitis is: 1) non-surgical periodontaltherapy; 2) evaluation afteradequate time for patient's plaquecontrol improvement and potential resolutionof the inflammatory response; 3) periodontal surgery to obtain access toremaining sites with an "active disease process" or to correct (regenerate) existing deep defects; and 4) supportiveperiodontal therapy (maintenance). This approach essentially agrees with the World Workshop observations.r" Itmust be recognized that some sites do not respond like theaverage. A clinical therapeutic procedure should be performed and reevaluated against an expected response. Aresponse that is less than expected requires evaluation ofother potential variables to determine the direction for future therapy.
SUMMARYThe following composite summary can be made of the longitudinal studies that have compared modes of periodontaltherapy:
1. Surgical and non-surgical periodontal therapy produced general improvement in the periodontal clinicalparameters.
2. Surgical therapy generally created greater short-termreduction of probingdepth. Long-term results were mixed,with somestudies reporting greater probing depth reductionfollowing surgery and others reporting no differences.
3. Effects of flap surgery with and without osseous resection on probingdepth showed mixed short-term results.Some studies reported thatosseous resection produced greaterprobing depth reduction while others showed no difference.One long-term study reported that osseous resection produced greater probing reduction while the others showedno difference.
4. Surgery produced a greater loss of probing attachmentin shallow sites, both short- and long-term. In sites withinitiallydeeper probing depths, short-term results were mixedwith a few studies reporting greater gain following surgery,
KALDAHL, KALKWARF, PATIL 251
others reporting greater gain following non-surgical therapy, and still others reporting no difference. Most longterm studies reported no difference in probing attachmentchange between non-surgical and surgical therapy.
5. When probing attachment levels following surgery withand without osseous resection were compared, either nodifference was found between therapies or flap surgerywithout osseous resection produced greater gain both shortand long-term.
6. There was no difference in the longitudinal maintenance of probing attachment level between sites treated nonsurgically and those treated surgically, with or without osseous resection.
7. There was no difference in inflammatory indices between sites treated with non-surgical therapy and any typeof surgical therapy.
8. There was no difference in post-treatment supragingival plaque accumulation between sites treated with anyof the therapeutic approaches reported.
9. When the effects of plaque control alone and plaquecontrol with root planing were compared, root planing produced a superior response in the clinical parameters.
AcknowledgmentsThe authors wish to thank PennyGardner, Dr. Robert Krejci,and Dr. Jeffrey Payne for help in the manuscript preparation.
REFERENCES1. Ramfjord S, Nissle R, Shick R, Cooper H. Subgingival curettage
versus surgical elimination of periodontal pockets. J Periodontol 1968;39:167-175 .
2. Ramfjord S, Knowles J, Nissle R, Shick R, Burgett F. Longitudinalstudy of periodontal therapy. J Periodontol 1973; 44:66-77.
3. Ramfjord S, Knowles J, Nissle R, Burgett F, Shick R. Results following three modalities of periodontal therapy. J Periodontol 1975;46:522- 526.
4. Knowles J, Burgett F, Nissle R, Shick R, Morrison E, Ramfjord S.Results of periodontal treatment related to pocket depth and attachment level. Eight years. J Periodontol1979; 50:225- 233.
5. Ramfjord S, Knowles J, Morrison E, Burgett F, Nissle R. Results ofperiodontal therapy related to tooth type. J Periodontol 1980; 51:270273.
6. Morrison E, Ramfjord S, Hill R. Short-term effects of initial nonsurgical periodontal treatment (hygiene phase). J Clin Periodontol1980; 7:199- 211.
7. Hill R, Ramfjord S, Morrison E, et al. Four types of periodontaltreatment compared over two years. J Periodontol1981; 42:655-662.
8. Ramfjord S, Caffesse R, Morrison E, et al. Four modalities of periodontal treatment compared over 5 years. J Clin Periodontol 1987;14:445-452.
9. Ramfjord S. Surgical periodontal pocket elimination: Still a justifiableobjective ? J Am Dent Assoc 1987; 114:37-40.
10. Rosling B, Nyman S, Lindhe J, Jern B. The healing potential of theperiodontal tissues following different techniques of periodontal surgery in plaque-free dentitions. A 2-year clinical study. J Clin Periodontol1976; 3:233-250.
11. Rosling B. Periodontally treated dentitions: Their maintenance andprognosis . Int Dent J 1983; 33:147-151.
12. Nyman S, Lindhe J, Rosling B. Periodontal surgery in plaque-infecteddentitions . J Clin PeriodontoI1977; 4:240-249.
13. Lindhe J, Westfelt E, Nyman S, Socransky S, Heijl L, Bratthall G.
)
252 A REVIEW OF LONGITUDINAL PERIODONTAL THERAPY STUDIES1 Periodontol
April 1993
Healing following surgical/nonsurgical treatment of periodontal disease. A clinical study. J Clin Periodontol 1982; 9:115-128.
14. Lindhe 1, Socransky S, Nyman S, Haffajee A, Westfelt E. " Criticalprobing depths" in periodontal therapy. J Clin Periodontol 1982;9:323-336.
15. Lindhe 1, Westfelt E, Nyman S, Socransky S, Haffajee A. Long-termeffect of surgical/nonsurgical treatment of periodontal disease . J ClinPeriodontol1984; 11:448-458.
16. Lindhe 1, Nyman S. Scaling and granulation tissue removal in periodontaltherapy. J Clin Periodontol1985; 12:374--388.
17. Westfelt E, Bragd L, Socransky S, Haffajee A, Nyman S, Lindhe 1.Improved periodontal conditions following therapy . J Clin Periodontol 1985; 12:283-293.
18. Lindhe 1, Socransky S, Nyman S, Westfelt E. Dimensional alterationsof the periodontal tissues following therapy. lnt J Periodontics Restorative Dent 1987; 7(2):9-21.
19. Smith D, Ammons W, van Belle G. A longitudinal study of periodontal status comparing osseous recontouring with flap curettage . I.Results after 6 months. J Periodontol1980; 51:367-375.
20. Townsend-Olsen C, Ammons W, van Belle G. A longitudin al studycomparing apically repositioned flaps with and without osseous surgery. lnt J Periodontics Restorative Dent 1985; 5(4) :11-33.
21. Pihlstrom B, Oritz-Campos C, McHugh R. Randomized four-yearstudy of periodontal therapy. J Periodontol 1981; 52:227-242.
22. Pihlstrom B, McHugh R, Oliphant T, Oritz-Campos C. Comparisonof surgical and nonsurgical treatment of periodontal disease. A reviewof current studies and additional results after 6'12 years. J Clin Periodontol1983; 10:524--541.
23. Pihlstrom B, Oliphant T, McHugh R. Molar and nonmolar teeth compared over 6'12 years following two methods of periodontal therapy. 'J Periodontol1984; 55:499-504.
24. Isidor F, Karring T, Attstrorn R. The effect of root planing as comparedto that of surgical treatment. J Clin Periodontol 1984; 11:669-Q81.
25. Isidor F, Karring T. Long-term effect of surgical and nonsurgicalperiodontal treatment. A 5-year clinical study. J Periodont Res 1986;21:462-472.
26. Chamberlain D, Garrell S, Renvert S, Egelberg1. Healing after treatmentof periodontal intraosseous defects. IV. Effect of a non-resective versusa partially resective approach. J Clin Periodontol 1985; 12:525-539.
27. Renvert S, Nilveus R, Egelberg 1. Healing after treatment of periodontal intraosseous defects . V. Effect of root planing versus flapsurgery. J Clin Periodontol 1985; 12:619-629.
28. Renvert S, Nilveus R, Dahlen G, Slots 1, Egelberg 1. 5-year followup of periodontal intraosseous defects treated by root planing or flapsurgery. J Clin Periodontol 1990; 17:356--363.
29. Badersten A, Nilveus R, Egelberg 1. Effect of non-surgical periodontal therapy. I. Moderately advanced periodontitis. J Clin Periodontol1981 ; 8:57-72.
30. Cercek 1, Kiger R, Garrell S, Egelberg 1. Relative effects of plaquecontrol and instrumentation on the clinical parameters on human periodontal disease. J Clin Periodontol 1983; 10:46--56.
31. Badersten A, Nilveus R, Egelberg 1. Effect of non-surgical periodontal therapy. II. Severely advanced periodontitis. J Clin Periodontol1984; 11:63-76.
32. Becker W, Becker B, Ochsenbein C, et al. A longitudinal studycomparing scaling, osseous surgery and modified Widman procedures. Results after one year. J Periodontol1988; 59:351-365.
33. Kaldahl W, Kalkwarf K, Patil K, DyerJ, Bates R. Evaluat ion of fourmodalities of periodontal therapy. Mean probing depth, probing attachmentlevel and recession. J Periodontol1988; 59:783-793 .
34. Kalkwarf K, Kaldahl W, Patil K. Evaluation of furcat ion region response to periodontal therapy. J Periodontol 1988; 59:794--803.
35. Kalkwarf K, Kaldahl W, Patil K, Molvar M. Evaluation of gingivalbleeding following four types of periodontal therapy. J Clin Periodontol1989; 16:601-608.
36. Kaldahl W, Kalkwarf K, Patil K, Molvar M. Responses of four toothand site groupings to periodontal therapy. J Periodontol 1990; 61:173179.
37. Kaldahl W, Kalkwarf K, Patil K, Molvar M. Evaluation of fourmodalitie s of periodontal therapy . Gingival suppuration and supragingival plaque. J Clin Periodontol 1990; 17:642-649.
38. Zamet 1. A comparative clinical study of three periodontol surgicaltechniques. J Clin Periodontol1975; 2:87-97.
39. Waite I. A comparison between conventional gingivectomy and a nonsurgical regime in the treatment of periodontitis. J Clin Periodontol1976; 3:173-185.
40. Aeschlimann C, Robinson P, Kaminski E. A short-term evaluationof periodontal surgery. J Periodont Res 1979;14:182-1 84.
41. Payot P, Bickel M, Cimasoni G. Longitudinal quantitative radiodensitomeric study of treated and untreated molar furcation involvements. J Clin Periodontol1987; 14:8-18 .
42. Schroer M, Kirk C, Wahl T, Hutchens L, Moriarty 1, BergenholtzB. Closed versus open debridement of facial grade II molar furcations.J Clin Periodontol1991; 18:323-329.
43. Listgarten M, Lindhe 1, Hellden L. Effect of tetracycline and/or scaling on human periodontal disease. Clinical , microbiological and histological observations. J Clin Periodontol1978; 5:246--271.
44. Hellden L, Listgarten M, Lindhe 1. The effect of tetracycline and/orscaling on human periodontal disease. J Clin Periodontol1 979; 6:222230.
45. Tagge D, O'leary T, EI-Kafrawy A. The clinical and histologicalresponse of periodontal pockets to root planing and hygiene. J Periodontol1975; 46:527-533 .
46. Yokota M, Kubo K, Matsuyama K, Sueda T. Pocket depth reductionby tooth types and sites after initial treatment. Dent Jpn 1990; 27:127133.
47. Nordland P, Garrell S, Kiger R, Vanooteghem R, Hutchens L, Egelberg 1. The effect of plaque control and root debridement in molarteeth. J Clin Periodontol1987; 14:231-236 .
48. Loos B, Nylund K, Claffey N, Egelberg 1. Clinical effects of rootdebridem ent in molar and non-molar teeth. A 2 year follow-up. J ClinPeriodontol 1989; 16:498-504.
49. Loos B, Claffey N, Egelberg 1. Clinical and microbiological effectsof root debridement in periodontal furcation pockets. J Clin Periodontol 1988; 15:453-463.
50. Rosling B, Slots 1, Christersson L, Genco R. Clinical and microbiological effects of surgical and nonsurgical treatment of multi-rootedteeth in adult periodontit is. J Dent Res 1984; 63 (Spec. Issue):205(Abstr . 311).
51. Friedman LM, Furburg CD, Demets DL. Fundamentals of ClinicalTrials, 2nd ed. Littleton, MA: PSG Publishing Co; 1985.
52. Chalmers T, Smith H Jr, Blackburn B. A method of assessing thequality of a randomized control trial. Controlled Clin Trials 1981;2:31-49.
53. Antczak A, Tang 1, Chalmers T. Quality assessment of randomizedcontrol trials in dental research. II. Results: Periodontal research. JPeriodont Res 1986; 21:315-321.
54. Boissel 1, Blanchard 1, Panak E, Peyrieux 1, Sacks H. Considerationsfor the meta-analysis of randomized clinical trials. Summary of apanel discussion. Controlled Clin Trials 1989; 10:254--281.
55. Blomqvis t N. On the choice of computational unit in statistical analysis. J Clin Periodontol1985; 12:873-876.
56. Imrey PB. Considerations in the statistical analysis of clinical trialsin periodontitis. J Clin Periodontol1986; 13:517-528.
57. Fleiss 1L, Wallenstein S, Chilton NW, Goodson 1M. A re-examination of within-mouth correlations of allachment level and of changein allachmentlevel. J Clin Periodontol1988; 15:411-414.
58. DeRouen TA. Statistical Models for Assessing Risk of PeriodontalDisease . Risk Assessment in Dentistry In: Bader 10, ed. Chapel Hill:University of North Carolina Press; 1990:234--244.
Volume 64Number 4
59. Blomqvist N. On the bias caused by regression toward the mean instudying the relation between change and initial value . J Clin Periodontol 1986; 13:34-37.
60. Hujoel P, Moulton L. Evaluation of test statistics in split-mouth clinical trials. J Periodont Res 1988; 23:378-380.
61. Hujoel P, Baab D, DeRouen T. The power of tests to detect differences between periodontal treatments in published studies. J ClinPeriodontoI1992;19:784-789.
62. Hirschfeld L, Wasserman B. A long-term survey of tooth loss in 600treated periodontal patients. J Periodontol 1978; 49:225-237.
63. McFall W. Tooth loss in 100 treated patients with periodontal disease.J Periodontol 1982; 53:539-549.
64. Ross 1, Thompson R. A long-term study of root retention in thetreatment of maxillary molars with furcation involvement. J Periodontol 1978;49:238-244.
KALDAHL, KALKWARF, PATIL 253
65. Ross I, Thompson R. Furcation involvement in maxillary and mandibular molars. J Periodontol 1980; 51:45(}....454.
66. Haffajee A, Socransky S, Goodson J. Comparison of different analyses for detecting changes in attachment level. J Clin Periodontol1983; 10:298-310.
67. Lindhe J, Haffajee A, Socransky S. Progression of periodontal diseasein adult subjects in the absence of periodontal therapy. J Clin Periodontol1983; 1O:43~42.
68. The American Academy of Periodontology. Proceedings ofthe WorldWorkshop in Clinical Periodontics Chicago: The American Academyof Periodontology; 1989: 11113-11116.
Send reprint requests to: Dr. Wayne B. Kaldahl, UNMC College ofDentistry, 40th and Holdrege, Lincoln, NE 68583-0740.
Accepted for publication October 15, 1992.





























