Embed Size (px)
Citation preview

Never offer the devil (desire) a ride,He always want to be in the driving seat…!
-- BK

CPC 4.2.3 – 2013 – “yellow eyes”
• Fatigue / Anorexia..?• Nausea, Vomiting..?• Haematemesis… ?• Itching..? • Fever..?• Abdominal distension slow..?• Bleeding / Bruising..?• 10 stubbies/day /more..?• Many Tattoos..?• BMI – if low / High..?
2
Mr. T.D. 50 year old, presents to his GP. ‘My stomach appears big and my wife has noticed a yellow tinge in my eyes’.
CASE STUDY 1
Abd distension, fatigue, yellow discoloration of eyes for 1 week
Presenting Symptoms:
• Liver failure…• Liver failure…• Portal Hypertension• Obstructive jaundice.• Hepatitis.• Cirrhosis.• Vit-K deficiency.• Alcoholic hepatitis.• Viral Hepatitis (B/C)• Anorexia / Obesity –
steatosis.
• Differential Diagnosis: • Hepatitis: Alcoholic/Infective/Malignant/Drug/Toxins• Acute / Chronic? Primary/Secondary? • “HBV / HCV, CMV, Lepto, Dengue, Melioidosis.

Case2: Mr.GG, 48y, fatigue & yellow…
• Abdominal distension, fatigue, yellow sclera – 6 weeks.
• Hardware business, Alcohol 40units / wk.• Travel: Thailand, had tattoo / surgery /
transfusion.. * • PE: abdomen nil sig. mild RUQ
tenderness. No organomegaly.• Differential: Acute hepatitis.
– CMV, Lepto, Hep A,B,C..– Hepatitis - Alcohol– Chronic hepatitis.– Drugs, toxins,
3
AST = 1320 U/l ALT = 1780 U/lAlk. Phos. = 133 U/lGGT = 192 U/lHep B Serology Hep B sAg +ive Hep B sAb <10 Hep B cAb IgM +ive Hep B e Ag +ive Hep B eAb –ive

4
CPC 4.2.2 - 2010• George, 62 year old farmer from Tully, presents to
his GP with fatigue. His wife has asked him to consult you as his eyes look a bit yellow'.
• Fatigue: Progressing 2wk. Unable to get out. • nausea : no • vomiting/haematemesis : no • Anorexia, wt loss: yes thinks lost a bit of weight. • bowel habit : constipated, stool pale, no blood.• 2 x episodes fatigue last 2 years preceded by 2
weeks of fever. Lab: “liver not working so well'. then felt better and has not been to see GP since.
• Banana farmer from Greece - 26 years ago.

5
Laboratory Investigations:• FBC: Hb 13.8 g/dl, PCV 45%; WBC 7000/mm3, 70% N,
25% L; Platelets 200,000/mm3 • Blood film: Normocytic, normochromic cells • Bilirubin: Total serum Bilirubin = 98 μmol/l, (Direct 67)• Liver enzymes: • Aspartate amino transferase (AST) = 182 U/l • Alanine amino transferase (ALT) = 55 U/l • Alkaline Phosphatase = 190 U/I • Serum Protein: Total protein = 59 g/l, Albumin = 20 g/l, • Hepatitis B Surface Antigen (HbsAg): Positive Hep B sAg +ive
Hep B sAb <10Hep B cAb IgM +iveHep B e Ag +iveHep B eAb –ive

6
Differential Diagnosis:• Viral fever -?
– Yellow fever, Relapsing fever, Dengue, Ebola, – Leptospirosis (common in Tully) - ?
• Hepatitis – Acute / Chronic - ?• Chronic Hepatitis B – why chronic?• History & presentation in Hep. A & C ?• Other causes of Jaundice?• Alcoholic liver disease ?• Toxins, chemical, Reyes syndrome?• Hemolytic / Anemia - ?• Malignancy - ?

7
CPC23: HBS – Hepatitis & Cirrhosis
• Pathology Major CLI:– Acute & Chronic Liver injury.– Pathophysiology of Jaundice, Clinical & Pathological types. – Alcoholic Liver disease – Pathophysiology, types & complications.– Hepatitis – Causes, types, Pathology (Alcohol, viral, Drug) – Pathology of cirrhosis – Types, morphology & Clinical.
• Pathology Minor CLI:– Primary Biliary cirrhosis & Primary Sclerosing Cholangitis.– Wilson's disease, α1-Antitrypsin (AAT) deficiency.
– Hemosiderosis, Hemochromatosis, Wilson’s disease.– Liver tumours – adenoma, hyperplasia & cancer.– Cysts: Amoebic liver abscess & Hydatid disease of liver.– Congenital: Gilberts sy, Childhood cirrhosis– Dengue, Ebola virus, Reye’s sy,– Liver blood supply disorders: Budd-Chiari Sy.

"When you speak, speak the truth; perform when you promise; discharge your trust... Withhold your hands from striking, and from taking that which is unlawful and bad..."-- From Wings of Fire, book by Dr. APJ Abdul Kalam, Foremer President of India.

9
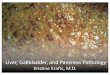
Pathology of Common Liver Disorders
Dr. Venkatesh M. Shashidhar.Assoc.Prof & Head of Pathology

10
• 1.5 kg, wedge shape• 4 lobes, Right, left,
(Caudate, Quadrate)• Double blood supply• Hepatic arteries• Portal – Venous blood
Normal

Normal Liver - InfantMuch larger, both lobes big, palpable below costal margin

12
CT Upper abdomen - Normal
Liver
Stomach
Spleen
Aorta
LungLung

13
Normal Liver – MicroscopyAcinus – showing zones 1, 2 & 3.
Portal Triad
Central Vein
Blood Flow

14
Structure of Liver LobulePortal Triad: Art, Vein, BD
Metab, synthesis, detoxification...
GIT Venous bl. HeartIVC
Liver failure in Cirrhosis…?

15
Acinus LobuleFunctional Anatomic
Zone 1 – Toxin damage. Zone 3 – Ischemic damage
Toxins Ischemia
Toxins
Ischemia

16
Liver Function Tests: Interpretation• Synthesis / Function.
– Total protein & albumin low, PT prolonged why? (vit K..)
• Hepatocyte Injury.– ALT, AST, LDH - high. – why?– Alk Phos – moderately increased. – why?
• Bile Duct Damage:– Alk Phos – increased – why?
• Other:– GGT – increased with alcohol use. – why?– Viral serology - – Auto-Antibody panel.
GGT ↑ Alcohol (centrilobular)
IgG ↑ Autoimmune hepatitis
IgM ↑ Primary biliary cirrhosis
IgA ↑ Alcoholic cirrhosis
AFP +ve Hep. Cell. Carcinoma
Anti-mitochondrial antibody
+ve Primary biliary cirrhosis
Anti-smooth muscle, & ANA
+ve Autoimmune hepatitis

17
• Overproduction (Hemolytic - Unconjugated)
• Impaired uptake (Hepatitis - mixed)
• Block in metabolism (Congenital)
• Impaired transport. (Hepatitis, toxins)
• Intrahepatic Obst. (Hepatitis)
• Extrahepatic Obst. (Obstructive - Congugated)
Jaundice Types:

18
Jaundice Clinical Types:
Stool Urine Ser. chem. Diagnosis
Dark Normal Un.Conj / ID Hemolysis.
Pale Dark Conj./D + ALP Cholestasis
Pale Dark ID+D ALT/AST Hepatitis.
Variable Variable Variable Cong. Syndr.

A wise man watches his faults more closely than his virtues; others reverse the order. --Napoleon Hill

20
Pathology of Viral Hepatitis
Dr. Venkatesh M. Shashidhar.Assoc.Prof & Head of Pathology

21
Viral Hepatitis: Introduction• Viral Hepatitis:
– Specific – Heptitis B, C, D (serum), A, E – Non-Specific - Many viruses CMV, EBV, etc.– Acute, Chronic (CPH, CAH), Fulminant.
• Specific viral hepatitis important cause of morbidity & mortality.
• Horizontal transmission – Blood.. Sex.• Vertical transmission – Mother to fetus.• Hepatitis Cirrhosis Hepatic Ca. (not in A/E)

22
Hepatitis A• 'faecal-oral' spread, Travel / exposure. • Relatively short incubation period (2-6wk)• Epidemics common, may be sporadic. • Direct cytopathic virus (immune in B & C)• No carrier state – prolonged immunity.• Usually mild illness, full recovery usual.• Rarely – severe or fulminant.• IgM Ab is diagnostic. (no IgG tests).

23
Viral Hepatitis A: Serology

24
History Hep B Virus:
• In 1965 - Dr. Blumberg who was studying haemophilia, found an antibody in two patients which reacted against an antigen from an Australian Aborigine. Later the antigen was found in patients with serum type hepatitis and was initially designated "Australia Antigen". Later proved to be hepatitis B virus surface antigen (HBsAg). Dr. Blumberg was awarded the Nobel Prize in 1976.

25
Hepatitis B• Spread by blood, Sex & birth (serum hepatitis..)
• Relatively long incubation period (4-26wk)• liver damage by antiviral immune reaction • Carrier & Chronic state exist.• Relatively serious infection – chronic • Complications: cirrhosis, carcinoma.• Diagnosis: Viral serology (HBs, HBc & HBe) IgM anti-HAV
antibodyAcute Hepatitis A
HBsAg Hepatitis B or carrier – exp./inf.
HBeAg Active hepatitis B infection
Anti-HCV antibody Hepatitis C virus exposure
HCV RNA Active hepatitis C infection

26
Viral Hepatitis B: Serology
Sequence of serologic markers for hepatitis B viral hepatitis demonstrating (A) acute infection with resolution and (B) progression to chronic infection.

27
Pathogenesis of Hepatitis A & B:

28
Pathogenesis:• Ingestion / inoculation• Replication - Viremia• Liver – major site replication.• Cellular immune response.• Apoptosis, necrosis of hepatocytes.• Inflammation - Hepatitis • Bridging Hepatocyte necrosis (Central vein,
portal triad)• Fibrosis – patchy/bridging• Cirrhosis – extensive fibrosis with loss of
archetecture & regenerating nodules.• Liver Failure, Coma, Carcinoma..

29
Pattern of Liver Damage
• Zonal – Toxin/Hypoxia• Bridging – Viral & severe• Interface – CAH, Immune• Apoptotic – Acute Viral

30
Clinical Viral Hepatitis: (A,B,C, D & E)
• Carrier state / Asymptomatic phase• Hepatic dysfunction:• Acute hepatitis – fever, icterus.• Chronic Hepatitis – non specific.
– Chronic Persistent Hepatitis (CPH)– Chronic Active Hepatitis (CAH)
• Fulminant hepatitis – massive necrosis• Cirrhosis – total fibrosis.• Hepatocellular Carcinoma

31
Viral Hepatitis: Microbiology
Virus Hep-A Hep-B Hep-C Hep-E
agent ssRNA dsDNA ssRNA ssRNA
Incubation 2-6 wk 4-26 wk 2-6 wk 4-6 wk
Transm. Faeco-oral Parenteral Parenteral Faeco-oral
Carrier None 5-10% Rare/None None
ChronicCirrhosis
NoneNone
4-10%1-3%
80%50%
NoneNone
Other Young Mild / fulminant, travel.
Long incubat. ~ 120d
SteatosisSevere.
Severe inPregnant

32
Acute viral Hepatitis: Swelling & Apoptotic cells.
• Diffuse Inflammation.• Necrosis & Apoptosis.• Liver enzymes raised.

33
Liver Biopsy – CPH:
Inflammation
• Portal Inflammation.• No Necrosis• Liver enzymes normal

34
Chronic Active Hepatitis(CAH):
• Portal & Diffuse Inflammation.• Necrosis & Apoptosis.• Liver enzymes abnormal.

35
Viral – Steatosis - Alcoholic
Microvesicular (viral) Macrovesicular (alcoholic)

36
Fulminant Hepatitis:• Hepatic failure with in 2-3 weeks.• Reactivation of chronic or acute hepatitis• Massive necrosis, shrinkage, wrinkled• Collapsed reticulin network• Only portal tracts visible• Little or massive inflammation – time• More than a week – regenerative activity• Complete recovery – or - cirrhosis.

37
Fulminant Hepatitis:

38
Clinical Spectrum of HBV inf:

Failure is a blessing when it pushes one out of a cushioned seat of self-satisfaction and forces him to do something useful.
--Napoleon Hill

Laboratory DiagnosisViral Hepatitis

41
Viral Hepatitis C: Serology

Hepatitis B – Lab result interpret

43
Learn from the mistakes of others. You can't live long enough to make them all yourself…!
61% of 5th year students exceeded ‘sensible’ limitsDrugs and alcohol were taken mainly for pleasure and were perceived as a normal part of life for many students… Capability of advising patients…?
http://www.lycaeum.org/research/researchpdfs/1996_webb_1.pdf

"The past, the present and the future are really one: they are
today!"-Harriet Beecher Stowe
The past has gone and future you cannot see. The present, when you can do something, that is the Gift (Present) with which you can make your future & past memorable.
- Sai Baba

45
Other Hepatitis

Drug Induced Zonal Hepatitis:
46
• Autopsy specimen in a case of acetaminophen (paracetamol / NSAID) overdose.
• Prominent hemorrhagic necrosis of the centrilobular zones of all liver lobules.
• greater activity of drug-metabolizing enzymes in the central zones.
• Other agents that produce such injury are carbon tetrachloride, toxins of the mushroom Amanita phalloides.
• Patients either die in acute hepatic failure or recover without sequelae.

Autoimmune Hepatitis:
47
• Clinical & pathology similar to Chronic hepatitis.
• Female predominance (70%)
• Elevated serum IgG • High titers of
autoantibodies.• Autoimmune diseases.

Reye Syndrome:
48
• Acute disease of children • Following a febrile illness,
commonly influenza or varicella infection with use of aspirin.
• Microvesicular steatosis, hepatic failure, and encephalopathy.
• Cerebral edema and fat accumulation in the brain.
• Pathogenesis remains unknown (Aspirin..)
• Uncommon.
Fat stain (oil-red o)

Toxemia of Pregnancy:
49
• Abnormal LFT in 3-5% of preg.• Acute Fatty Liver of Pregnancy• Intrahepatic Cholestasis of Preg.• Hypertension, proteinuria, edema
and coagulation abnormalities (pre-eclampsia) with convulsions & coma (eclampsia).
• HELLP syndrome (hemolysis, elevated liver enz. & low plt).
• Patchy hemorrhages over capsule, DIC
• Fibrin thrombi in portal vessels.• Hepatocellular necrosis.

Self Study: brief
• Primary Biliary cirrhosis & Primary Sclerosing Cholangitis (differences, Male, female, associated conditions etc).
• Wilson's disease & α1-Antitrypsin (AAT) deficiency.
• Hemosiderosis, Hemochromatosis – differences.• Liver tumours – adenoma, hyperplasia & cancer.• Cysts: Congenital, Amoebic & Hydatid.• Congenital: Gilberts sy, Childhood cirrhosis• Hepatitis in Dengue & Leptospirosis• Reye’s syndrome.• Budd-Chiari Syndrome.
50

51
Pathology of Cirrhosis

52
Normal
Cirrhosis
Cirrhosis End stage of many
diffuse liver damages. Resulting in scaring & regenerating nodules (liver failure due to loss of archetecture)
Nodular
Shrunken

53
Clinical Features - Pathogenesis• Hypoalbuminemia/edema • Hyperammonemia/CNS coma.• Hypoglycemia • Palmar erythema • Spider angiomas • Hypogonadism • Gynecomastia • Weight loss • Muscle wasting • Ascites • Splenomegaly • Esophageal varices • Hemorrhoids • Caput medusae-abdominal skin • Coagulopathy • Hepatic encephalopathy • Hepatorenal syndrome
• Decreased Albumin synthesis• Hepatorenal syndrome• Glycogen metabolism.• Excess Oestrogens• Excess Oestrogens• Excess Oestrogens• Excess Oestrogens• Decreased metabolism.• Decreased metabolism • Portal Hypertension• Portal Hypertension• Portal Hypertension• Portal Hypertension• Portal Hypertension• Coag factory synthesis.• Detoxification.• ? Renal ischemia

54
MRI Cirrhosis
Nodular
Shrunken

55
Liver Biopsy – Cirrhosis
Reg. nodule
Fibrous septa

56
Liver Biopsy – Cirrhosis
Reg. nodule
Fibrous septa

57
Liver Needle Biopsy – Cirrhosis:(Blue collagen stain)
Reg. nodule
Fibrous septa

58
Etiology of Cirrhosis• Alcoholic liver disease 60-70%• Viral hepatitis 10%• Biliary disease 5-10%• Primary hemochromatosis 5%• Cryptogenic cirrhosis 10-15%• Wilson’s, 1AT def rare

59
Pathogenesis:
• Hepatocyte injury leading to necrosis.– Alcohol, virus, drugs, toxins, genetic etc..
• Chronic inflammation - (hepatitis).
• Bridging fibrosis.• Regeneration of remaining hepatocytes
Proliferate as round nodules.• Loss of vascular arrangement results in
regenerating hepatocytes ineffective.

60
Cirrhosis – Portal hypertension
• Cirrhosis-obstruction
• Portal hypertension
• Splenomegaly• transudation -
Ascites

61
Clinical Features
Hepatic encephalopathy

62
Gynaecomastia in Cirrhosis
??
?
?

63
Palmar erythema & Spider nevi
? Pathogenesis

Primary Biliary Cirrhosis• Autoimmune.• Females 6:1.• Pruritis, jaundice,
hepatosplenomegaly (initial).• Intrahepatic Bile duct inflammation • Cholestasis (bile stained liver)
64

Neonatal cholestasis / Cirrhosis• Infections;
– CMV, Syphilis, Septicemia.
• Extrahepatic biliary atresia.• Drugs & Toxins
– Nutrition, drugs.
• α1-Antitrypsin deficiency– Protease inhibitor (inflam).– Mild hepatitis cirrhosis.
• Cystic fibrosis.• Idiopathic
– Indian child hood cirrhosis.
65

66
Normal / Cirrhosis Liver

67
Hepatocellular Carcinoma
Normal - Carcinoma

68
Hepatic Adenoma: rare
adenoma
adenoma

69
Nutmeg Liver:• Chronic Passive
Congestion – Heart failure.• Central zone (Zone-3) –
congestion and necrosis.• Hemorrhage – RBCs in
zone-3 - Mottled appearance (nutmeg).
• Symptoms similar to chronic hepatitis, Ascites, distended abdomen, ankle edema, Hepatic encephalopathy, confusion.

70
Liver Metastasis:• Multiple• Clear
demarcation• Hemorrhage /
Central necrosis (+/-)
• Microscopy depends on type.

71
Learn from the mistakes of others. You can't live long enough to make them all yourself…!
61% of 5th year students exceeded ‘sensible’ limitsDrugs and alcohol were taken mainly for pleasure and were perceived as a normal part of life for many students… Capability of advising patients…?
http://www.lycaeum.org/research/researchpdfs/1996_webb_1.pdf

Alcoholic Liver Disease

73
Incidence is increasing…!

74
Chronic Alcoholism:• Clinical Features:

75
Alcoholic Liver Injury:• Ethyl alcohol : Common cause of
acute/Chronic liver disease• Alcoholic Liver disease - Patterns
– Fatty change, – Acute hepatitis (Mallory Hyalin)– Chronic hepatitis with Portal fibrosis – Chronic Liver failure– Cirrhosis
• All reversible except cirrhosis stage.

76
Alcoholic Liver Injury: Pathogenesis
• Acetaldehyde – metabolite – hepatotoxic• Diversion of metabolism to alcohol • Fat storage – fatty change. Cell swelling..• Rupture Fat necrosis severe
inflammation fibrosis.• Alcohol stimulates collagen synthesis• Inflammation, Portal bridging fibrosis• Micronodular cirrhosis.

77
Alcoholic Liver Injury: Pathogenesis• Diversion of fat metabolism
to alcohol – fat storage.• Acetaldehyde – hepatotoxic
– denatures Proteins• Increased peripheral release
of fatty acids.• Alcohol stimulates collagen
synthesis• Mutant ALDH2 gene with low
activity enzyme is observed in Caucasians but is found in some 40% of Orientals (autosomal dominant).
Acetaldehyde

78
Alcoholic Liver Damage
Ito Cells

79
High Risk
Intermediate
Low Risk
Safe drinking…

80
Risk of Alcohol injury
1 Unit = 10ml = 8gm

81
Alcohol Toxicity:Liver Fatty change Toxicity
Acute hepatitis
Alcoholic cirrhosis
Nervous system Wernicke syndrome Thiamine deficiency
Korsakoff syndrome Toxicity and thiamine deficiency
Cerebellar degeneration Nutritional deficiency
Peripheral neuropathy Thiamine deficiency
Cardiovascular system Cardiomyopathy Toxicity
Hypertension Vasopressor
Gastrointestinal tract Gastritis Toxicity
Pancreatitis Toxicity
Skeletal muscle Rhabdomyolysis Toxicity
Reproductive system Testicular atrophy ?
Spontaneous abortion ?
Fetal alcohol syndrome Growth retardation Toxicity
Mental retardation, Birth defects.

82
Alcoholic Liver Damage

Alcoholic Hepatitis:
83
• Centrilobular necrosis. Ballooned degenerating hepatocytes (BC) Mallory bodies (MB) Many Neutrophils, few lymphocytes & Macrophages.
• The central vein(or terminal hepatic venule (THV), is encased in connective tissue (C) (central sclerosis). Fat-laden hepatocytes (F) are evident in the lobule. The portal tract displays moderate chronic inflammation.

84
Alcoholic Hepatits - Mallory's hyalin

85
Alcoholic hepatitis & Mallory Hyalin:

86
Alcoholic Fatty Liver

87
Alcoholic Fatty Liver

88
Alcoholic Fatty Liver

Diffuse fatty liver - un-enhanced CT.
Hamer O W et al. Radiographics 2006;26:1637-1653
©2006 by Radiological Society of North America
Normal

90
Alcoholic Fatty Liver - CT

91
Alcoholic Fatty Liver - CT

92
Alcoholic Fatty liver:

93
Alcoholic Fatty Liver - collagen stain

94
Alcoholic Cirrhosis:

95
Alcoholic Fatty Liver - collagen stain

96
Alcoholic Liver Injury: Complications
• Pancreatitis – Acute or Chronic. Due to ischemic damage to pancreas.
• Alcoholic hepatitis – similar to viral hepatitis.• Fulminant hepatitis• Alcoholic Cirrhosis – Micronodular.
Alcohol & Medical students
http://www.m-c-a.org.uk/about_us/about_mca

Miscellaneous Conditions
97

Primary Biliary Cirrhosis
• Autoimmune, Chronic, progressive • Destruction of intrahepatic bile ducts, portal
inflammation & scarring – cholestasis.• Leading to cirrhosis and liver failure.• Females common (6:1)• Insidious onset of Pruritis & cholestatic jaundice.• Markedly high ALP, +ve antimitochondrial Ab.• Histopathology: Portal inflammation, bile stasis,
bile plugs & lakes, Later stages cirrhosis – Firm fibrotic, nodular, greenish, Shrunken.

Macronodular Cirrhosis - PBC

PBC – Microscopy:

Cholestasis: Bile “plugs”, Bile “lakes”
Bile Plugs
Bile Lakes

Biliary Atresia in a 3m child.Dark bile stained liver tissue, cirrhosis & death before 2 years of age.

103
Hepatosplenic schistosomiasis:
• Schistosoma Mansoni / haematobium
• Granulomas in the liver.• Fibrotic reaction around egg • Pipe stem Portal Fibrosis• Cirrhosis, spleenomegaly,
ascitis.

104
Hepatosplenic schistosomiasis:
• Schistosoma Mansoni / haematobium
• Granulomas in the liver.• Fibrotic reaction around egg • Pipe stem Portal Fibrosis• Cirrhosis, spleenomegaly,
ascitis.

"It's not the will to win, but the will to prepare to win that makes the
difference."
- - Bear Bryant 1913-1983, Football Coach

106
CPC-2.2– Major Pathology CLI:• Pathology of Acute & Chronic Liver injury. • Hepatitis – Causes, Types, Pathophysiology, Gross &
Microscopic Pathology. Complications. • Common types: Viral (Specific & Non specific), Alcoholic
& Drug induced. • Pathophysiology of Jaundice, Clinical & Pathological
types. • Pathology of cirrhosis – Classification, morphology &
Complications. • Pathology of Alcoholic Liver disease – Pathophysiology,
types & complications.

107
CPC-2.2– Minor Pathology CLI:• Hemosiderosis & Hemochromatosis. • Pathogenesis of Hepatic coma, Liver failure. • Primary Biliary cirrhosis. • Hepatocellular carcinoma. • Liver cysts & tumours – adenoma, hyperplasia & cancer.• Amoebic liver abscess & Hydatid disease of liver.• Congenital liver disorders – enzyme disorders.

108
Clinical Case Study

109
Case # 2 - ? Diagnosis• 60yr Male, 8 month slowly developing weakness,
mild icterus. • PE: Mild Abdominal tenderness, No
organomegaly. Mild Scleral icterus.• Labs: ALT: 52 (N= 8-33 U/L)• AST: 58 (N= 4-36 U/L)• Alk Phos: 150 (N= 20-130 u/L)• Bilirubin 3.9 (N= 0.1-1.2 mg/dL) (direct 1.8)• T Protein 4.8 (N= 6.0-7.8 g/dL)• Albumin 2.5 (N= 3.2-4.5 g/dl)• PT = 16 sec (N= 11-14.7 sec )• Differential diagnosis?• What further investigations?

110
Diagnosis pathway:• Jaundice?
– Mild increase, Mixed (combined)
• Synthesis?– Total protein, albumin – Low & PT abnormal.
• Obstruction & Bilirubin Clearance ?– Alk Phos is up a bit – but not high – some obstruction.
• Hepatocyte Direct Injury:– ALT & AST are up a bit, but not dramatically.
• Discussion:– Chronic Mild compromise - chronic Active
hepatitis. (In CPH LFT will be normal)
ALT: 52
AST: 58
Alk Phos: 150
Bilirubin 3.9 (direct 1.8)

111
• 28y Male, 3 weeks after visiting east Timor, presents with malaise, fatigue, loss of appetite. Mild icterus. AST & ALT mild elevation. Total bil 3.9mg/dl (Direct 2.8). Which of the following would be positive?

112
Alcohol Metabolism:

113
Chronic Hepatitis:• Passive CPH• Limited Periportal inflammation. • Mild Periportal fibrosis• No hepatocyte Necrosis.• LFT normal or mild change.• Late cirrhosis
• Active CAH• Extensive Inflammation • More fibrosis.• Necrosis of hepatocytes.• LFT abnormal.• Early cirrhosis & other complication.

“Nearly all men can stand adversity, but if you want to test a man's character, give him power!”
— Abraham Lincoln