Embed Size (px)
Citation preview
Gastrointestinal Pathology
Jocelyn Myra R. Caja, MD
Emmanuel R. de la Fuente, MD
Lorna B. Lioanag, MD
REQUIRED READINGS:
1. Tracheo-esophageal fistula
2. Diverticulum
3. Hiatal hernia
4. Mallory-Weiss syndrome
5. Reflux esophagitis
6. Barrett esophagus
7. Peptic ulcer
8. Esophageal varices
9. Achalasia
10. Tumors (squamous and adenocarcinomas)
Required Readings
1. Anatomy of the stomach
2. Acute and chronic gastritis
3. Peptic ulcer disease
4. Malignancies of the stomach and duodenum
- carcinoma
- malignant lymphoma
Required Readings
1. Anatomy of the small and large intestines
2. Infectious disease (viral infections, cholera, bacillary dysentery, salmonella, entamoeba histolytica, tuberculosis)
3. Hirschprung’s disease
4. Idiopathic inflammatory bowel disease
5. Acute appendicitis
6. Intestinal obstructions (intussuception, volvulus, hernias and adhesions)
7. Diverticular disease
8. Polyps/adenomas
9. Malignancies (carcinoma, lymphoma)
10. Hemorrhoids
PART I
PATHOLOGY OF THE
ESOPHAGUS
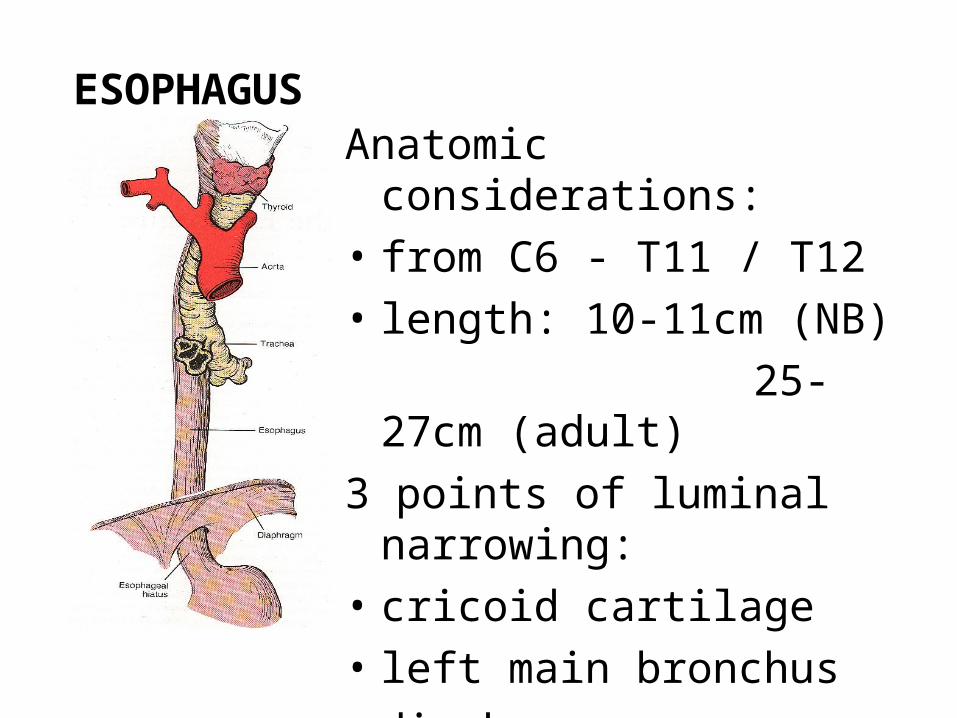
ESOPHAGUSAnatomic considerations:
• from C6 - T11 / T12
• length: 10-11cm (NB)
25-27cm (adult)
3 points of luminal narrowing:
• cricoid cartilage
• left main bronchus
• diaphragm
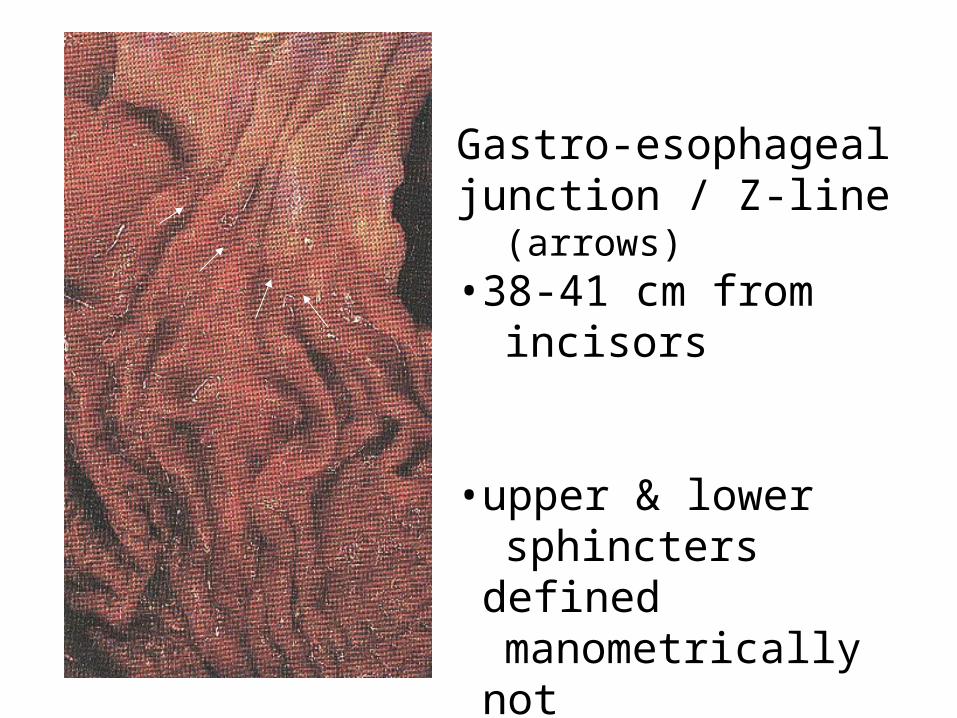
Gastro-esophagealjunction / Z-line (arrows)•38-41 cm from incisors
•upper & lower sphincters defined manometrically not morphologically
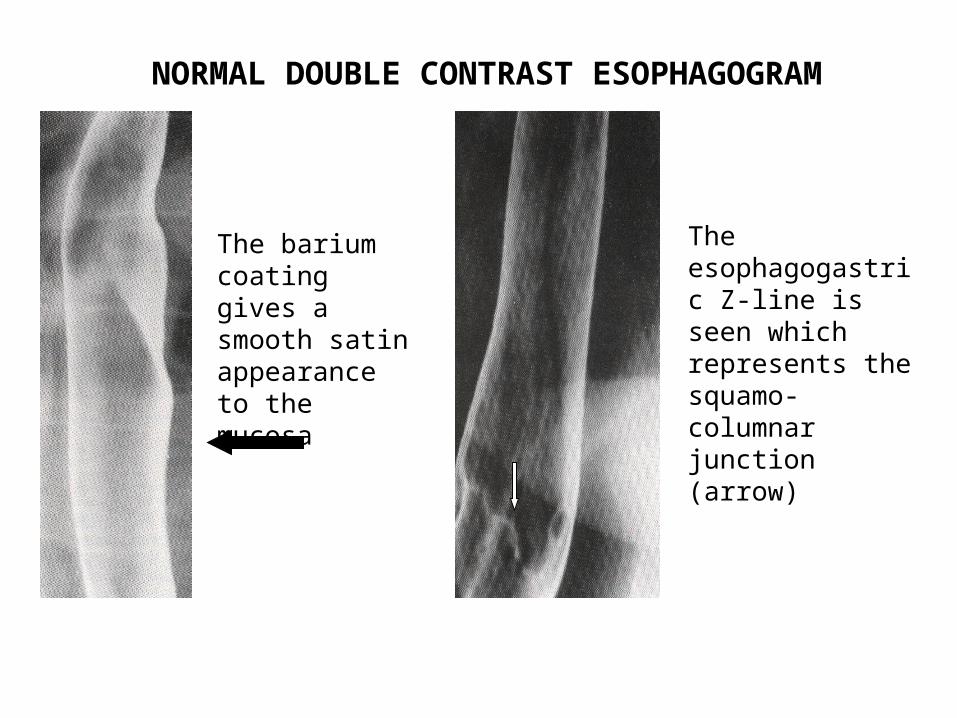
NORMAL DOUBLE CONTRAST ESOPHAGOGRAM
The barium coating gives a smooth satin appearance to the mucosa
The esophagogastric Z-line is seen which represents the squamo-columnar junction (arrow)
Histologic considerations:
3 muscle layers:– Inner circular– Middle oblique– Outer longitudinal - striated muscles
in the first 6-8 cm
* no serosa (allows easy spread of disease into mediastinum)
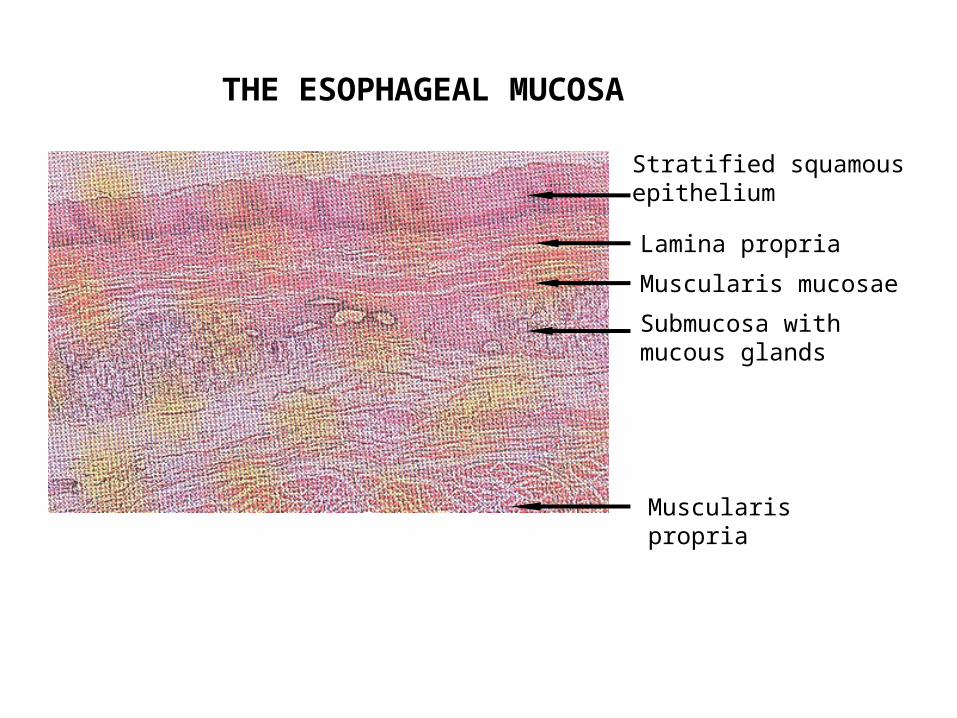
THE ESOPHAGEAL MUCOSA
Stratified squamous epithelium
Lamina propria
Muscularis mucosae
Submucosa with mucous glands
Muscularis propria
Congenital and Acquired Malformations:
• Tracheo-esophageal fistulas• Webs / Rings• Heterotopic tissue • Diverticula• Hiatal hernia• Mallory-Weiss tears• Varices
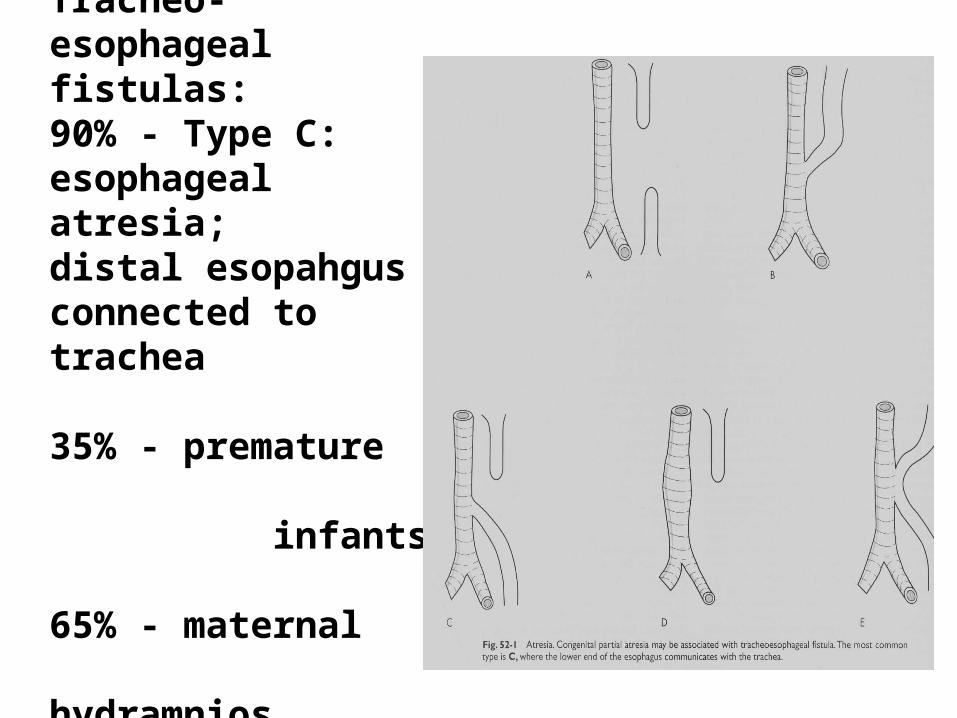
Tracheo-esophageal fistulas:90% - Type C: esophageal atresia; distal esopahgus connected to trachea
35% - premature infants
65% - maternal hydramnios
Hiatal hernia:
Saclike dilatation of
stomach present
above the diaphragm
* heartburns (10%); asymptomatic(50%)
*difficult to document grossly on autopsy
* no diagnostic microscopic findings
* incidence in peptic ulcer patients
* carcinoma is a rare complication
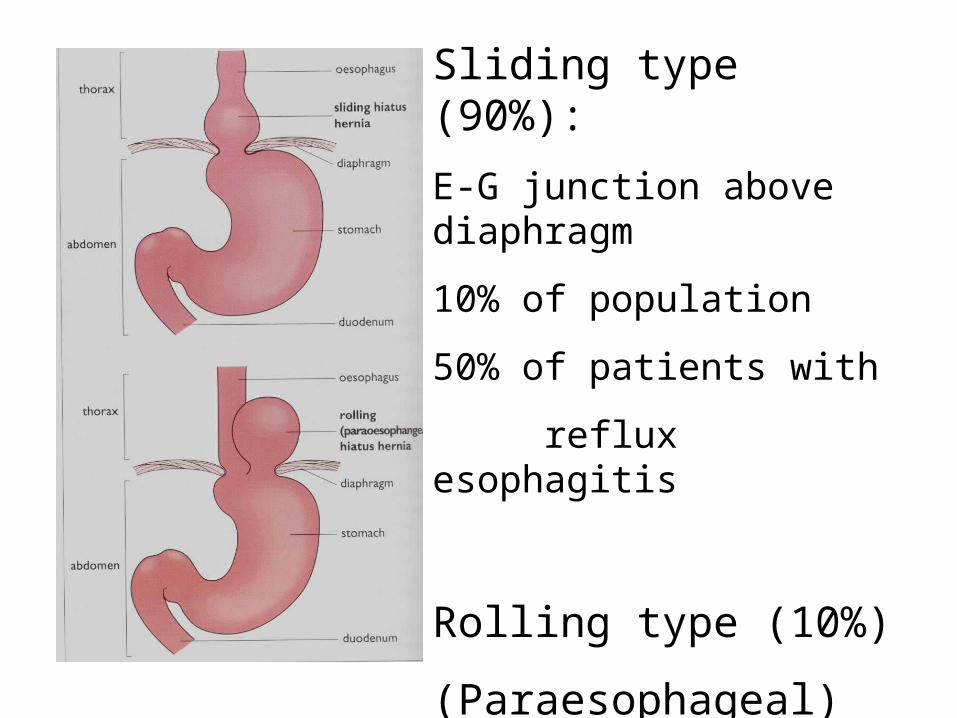
Sliding type (90%):
E-G junction above diaphragm
10% of population
50% of patients with
reflux esophagitis
Rolling type (10%)
(Paraesophageal)
E-G junction in normal location
Sliding type: 80-90%• congenitally short esophagus• esophageal scarring w/ traction on stomach• aggravated by swallowing• predisposes to reflux
Rolling (paraesophageal):10 -20 %• portion of cardia protrudes thru diaphragm
into thorax alongside esophagus• vulnerable to strangulation & infarction
ESOPHAGEAL DIVERTICULA
1. Outward protrusions of all, or portions, of the esophageal wall
2. May be acquired or congenital
3. Most common location of acquired is in the proximal portion due to uncoordinated actions of muscles of swallowing
4. May be due to traction due to pulling of esophageal wall by scar tissue; or pulsion due to congenital weakening of the muscular wall
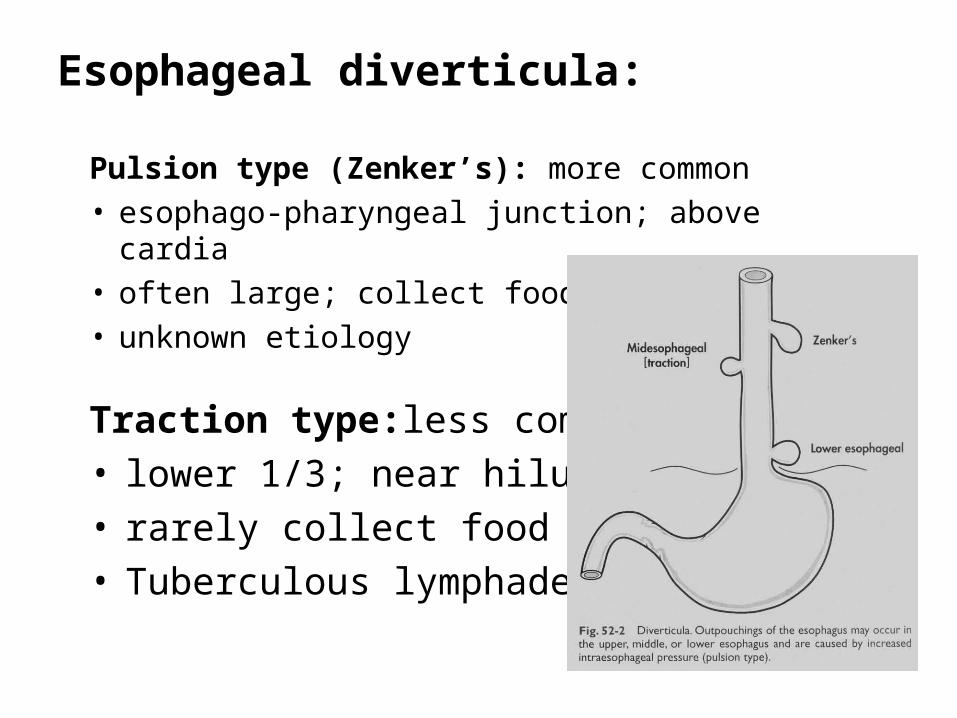
Esophageal diverticula:
Traction type:less common• lower 1/3; near hilum• rarely collect food• Tuberculous lymphadenitis
Pulsion type (Zenker’s): more common• esophago-pharyngeal junction; above cardia• often large; collect food• unknown etiology
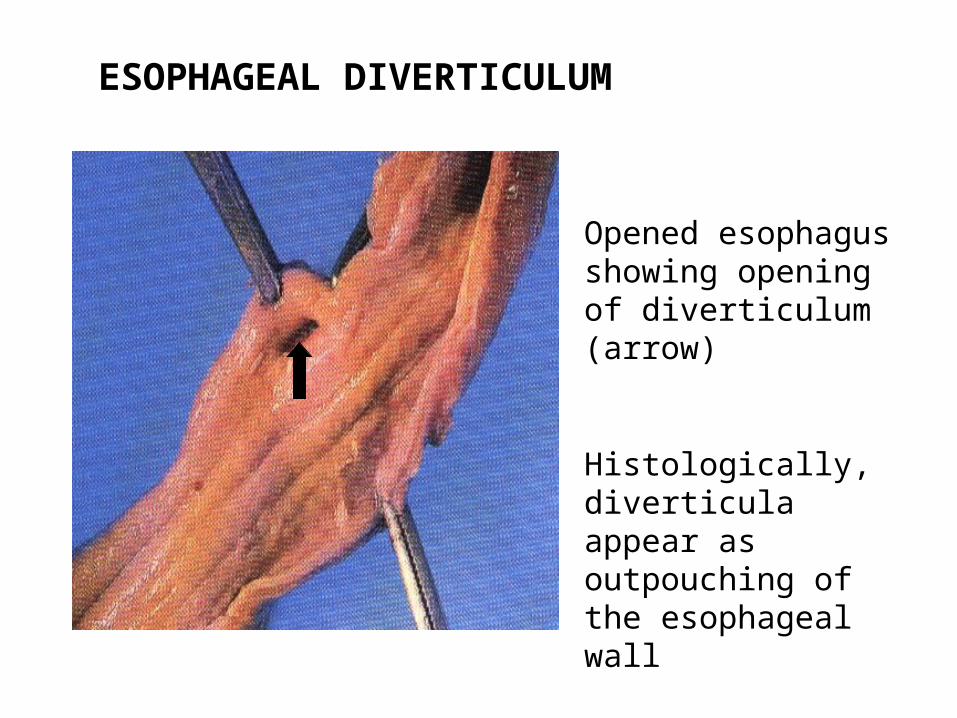
ESOPHAGEAL DIVERTICULUM
Opened esophagus showing opening of diverticulum (arrow)
Histologically, diverticula appear as outpouching of the esophageal wall
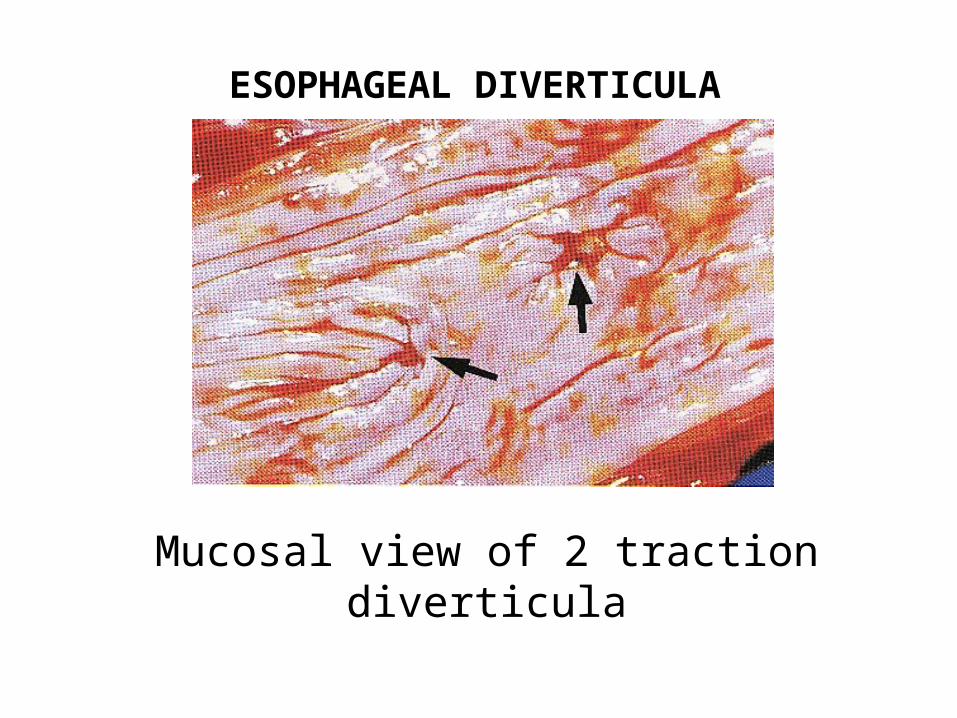
ESOPHAGEAL DIVERTICULA
Mucosal view of 2 traction diverticula
Mallory-Weiss tears:• linear lacerations oriented longitudinally
along the long axis of the esophagus
• usually occur at the G-E junction
• occur as consequence of chornic vomiting with severe counter peristalsis; most commonly in alcoholics
• may involve mucosa or even full thickness of the wall
• accounts for 5-10% of cases of massive hematemesis; may be fatal
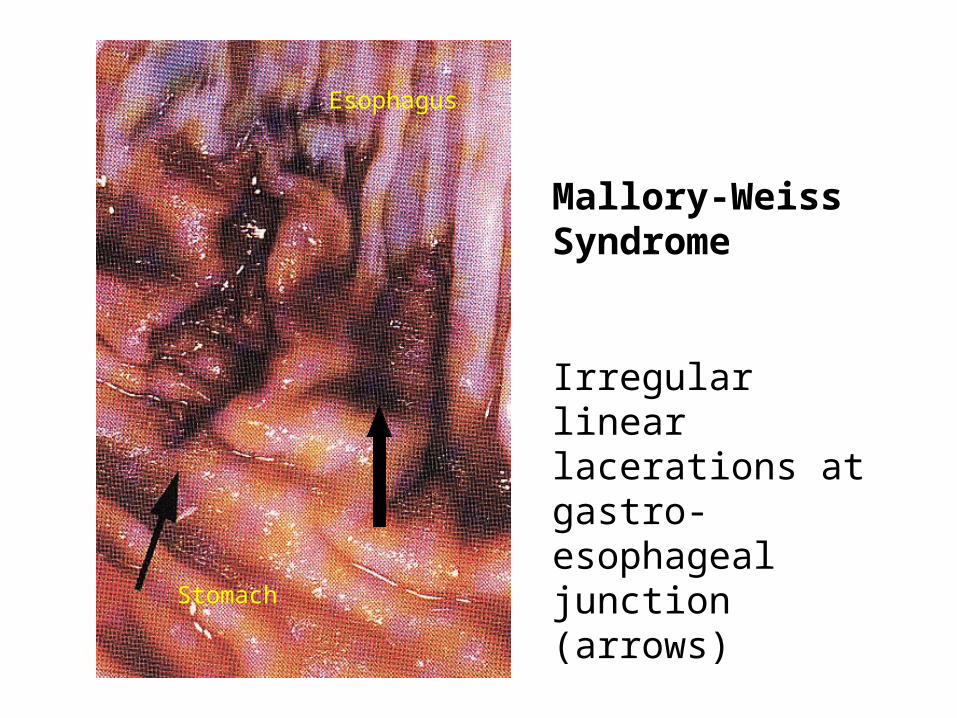
Mallory-Weiss Syndrome
Irregular linear lacerations at gastro-esophageal junction (arrows)
Stomach
Esophagus
Esophageal varices:
• dilated coronary veins in lower esophagus due to portal hypertension, usually in cirrhosis
• Portal hypertension causes the portal blood to be diverted thru the gastric coronary veins into the esophageal submucosal plexus veins.
• complication: massive hematemesis and rupture• 40% fatality rate; 50% of survivors rebleed• 40% of rebleeding cases eventually die
* varices commonly collapse postmortem
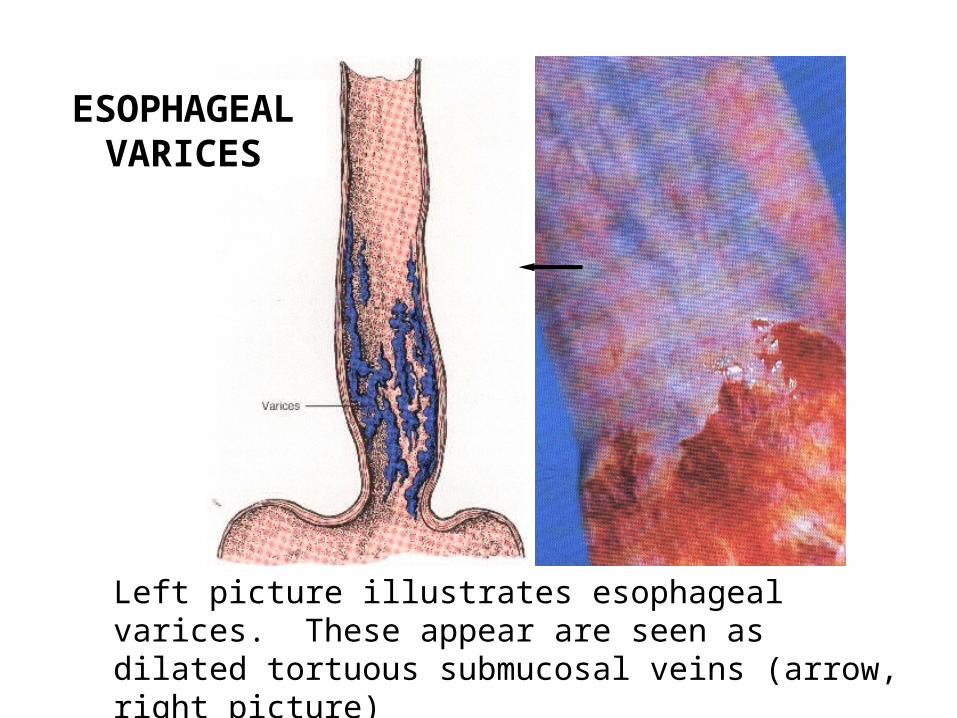
Left picture illustrates esophageal varices. These appear are seen as dilated tortuous submucosal veins (arrow, right picture)
ESOPHAGEAL VARICES
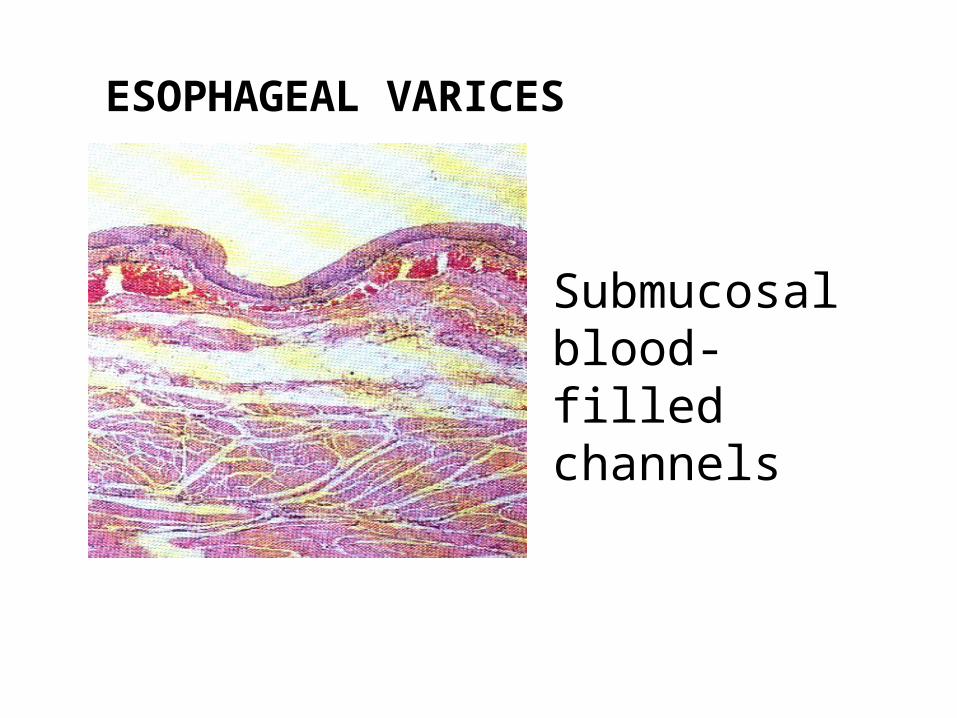
ESOPHAGEAL VARICES
Submucosal blood-filled channels
Esophageal dysmotility:• Achalasia
• Idiopathic Muscular Hypertrophy
• Progressive Systemic Sclerosis
• Plummer-Vinson Syndrome
• Leiomyomatosis
ACHALASIA
(Megaloesophagus)
1. Failure of relaxation of the smooth muscle fibers at the gastro-esophageal junction
2. May be due to: a) aperistalsis, b) partial or complete lower esophageal sphincter relaxation (LES), & c) increased resting LES pressure
3. Reduction of ganglion cells due to destruction
4. Progressive dysphagia is characteristic
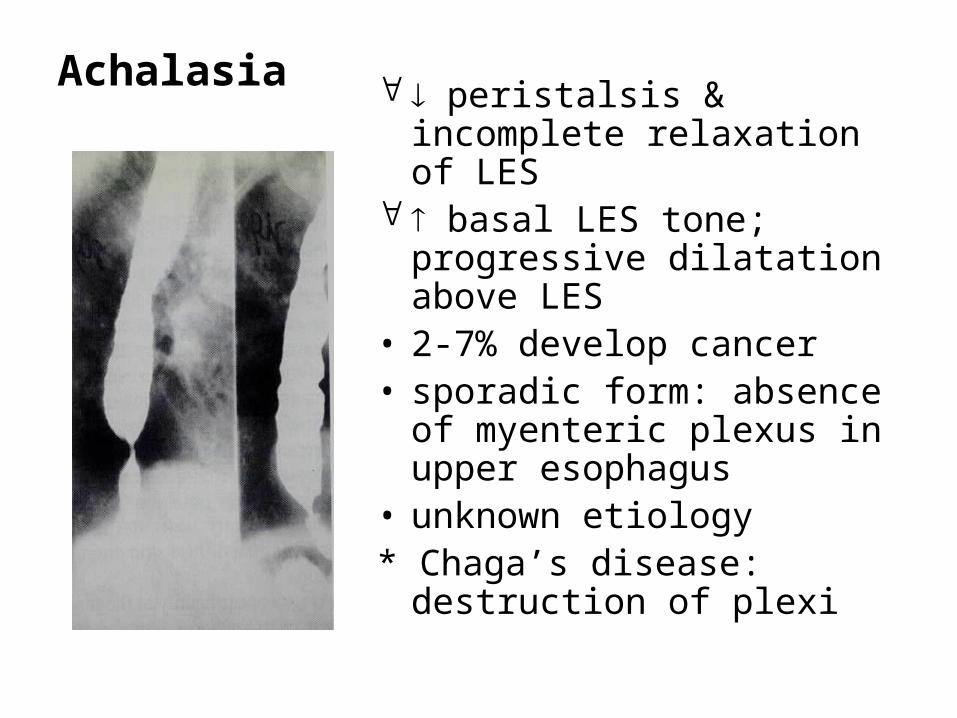
Achalasia peristalsis & incomplete relaxation of LES
basal LES tone; progressive dilatation above LES
• 2-7% develop cancer• sporadic form: absence of
myenteric plexus in upper esophagus
• unknown etiology* Chaga’s disease: destruction
of plexi
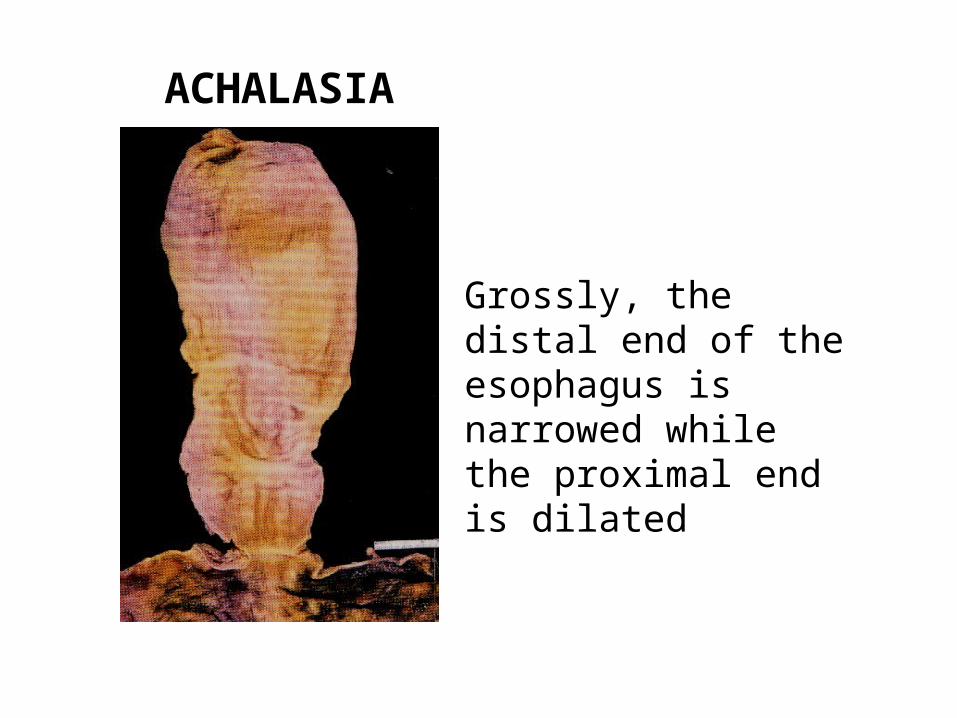
ACHALASIA
Grossly, the distal end of the esophagus is narrowed while the proximal end is dilated
Idiopathic Muscular Hypertrophy• primary abnormality of neural control
of distal esophageal musculature• results in spasm• predominantly affects inner circular
muscle layer
Progressive Systemic Sclerosis• vasculitis with muscle wall
degeneration• part of CREST syndrome
Plummer-Vinson Syndrome
• Atrophic glossitis, dysphagia• Hypochromic, microcytic anemia• Esophagitis in upper 1/3
* most common in middle-aged females
* risk of CA in upper 1/3 esophagus, oropharynx & tongue
* assoc. w/ esophageal webs
Esophagitis
• Reflux esophagitis
• Infectious (bacterial, viral, fungal)
• Chemically induced (corrosives)
• Iatrogenic (irradiation, instrumentation, Rx)
• others: Crohn’s disease
Pemphigus vulgaris
Uremia
Graft vs Host disease
Reflux esophagitis:
• recurrent or prolonged reflux
• elevated acidity & disordered motility
• basal hyperplasia > 15%; vascular pillae > 50% of mucosal height
• intraepthelial eosinophils
• assoc. w/ sliding hernia, ZE syndrome, scleroderma
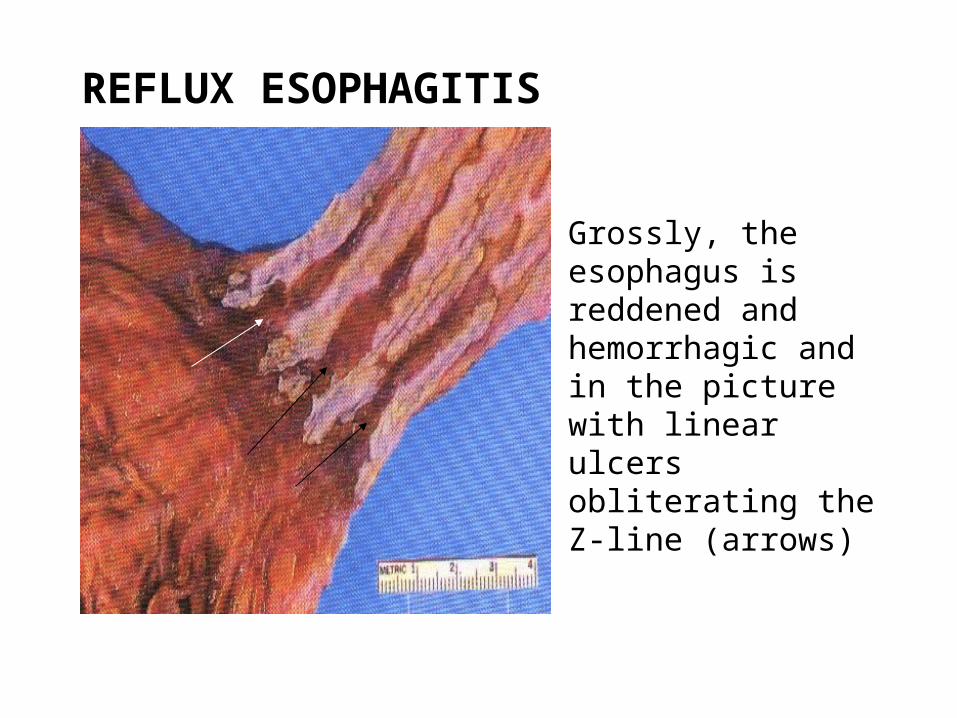
REFLUX ESOPHAGITIS
Grossly, the esophagus is reddened and hemorrhagic and in the picture with linear ulcers obliterating the Z-line (arrows)
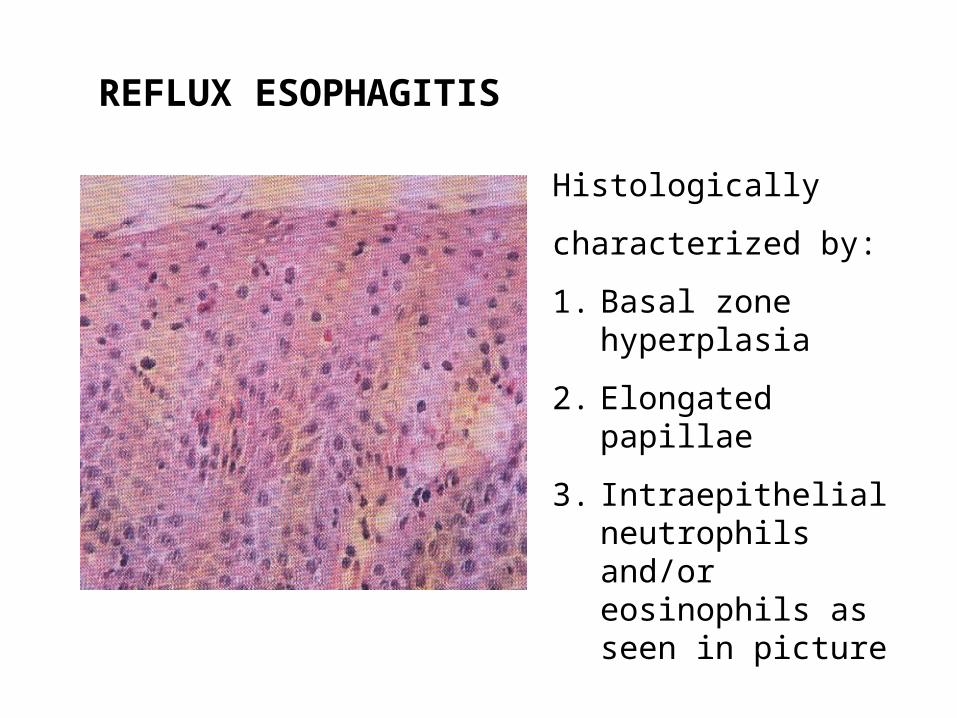
REFLUX ESOPHAGITIS
Histologically
characterized by:
1. Basal zone hyperplasia
2. Elongated papillae
3. Intraepithelial neutrophils and/or eosinophils as seen in picture
BARRETT’S ESOPHAGUS
1. A condition in which the stratified squamous epithelium of the esophagus is replaced by columnar epithelium
2. Usually involving the lower 3rd
3. Usually acquired as a complication of reflux esophagitis
4. Complication: development of glandular dysplasia and adenocarcinoma
BARRETT’S ESOPHAGUS
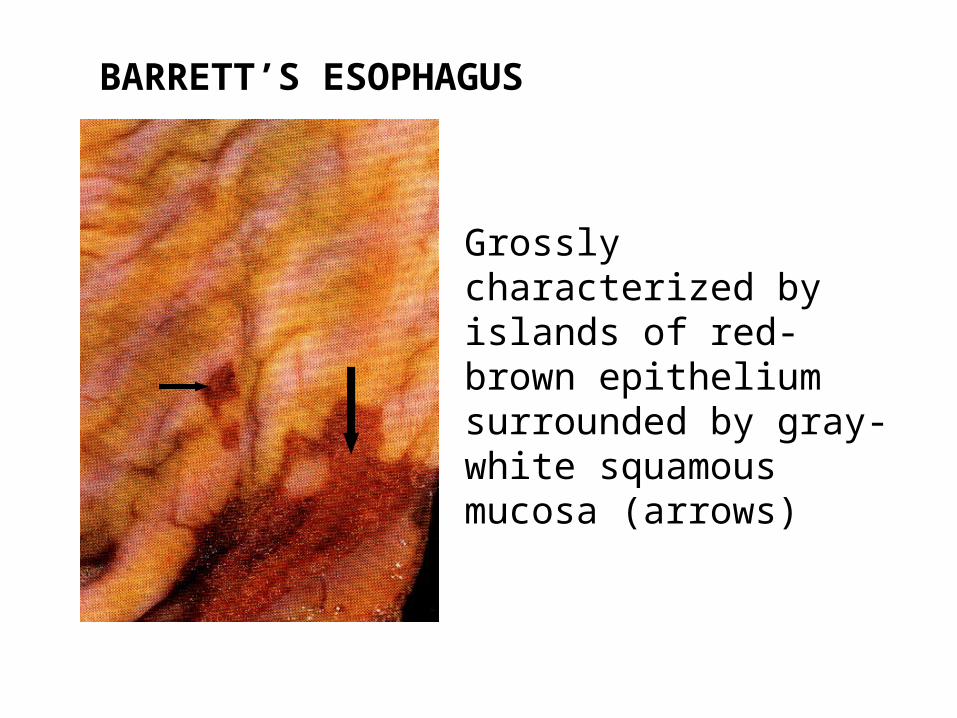
Grossly characterized by islands of red-brown epithelium surrounded by gray-white squamous mucosa (arrows)
BARRETT’S ESOPHAGUS
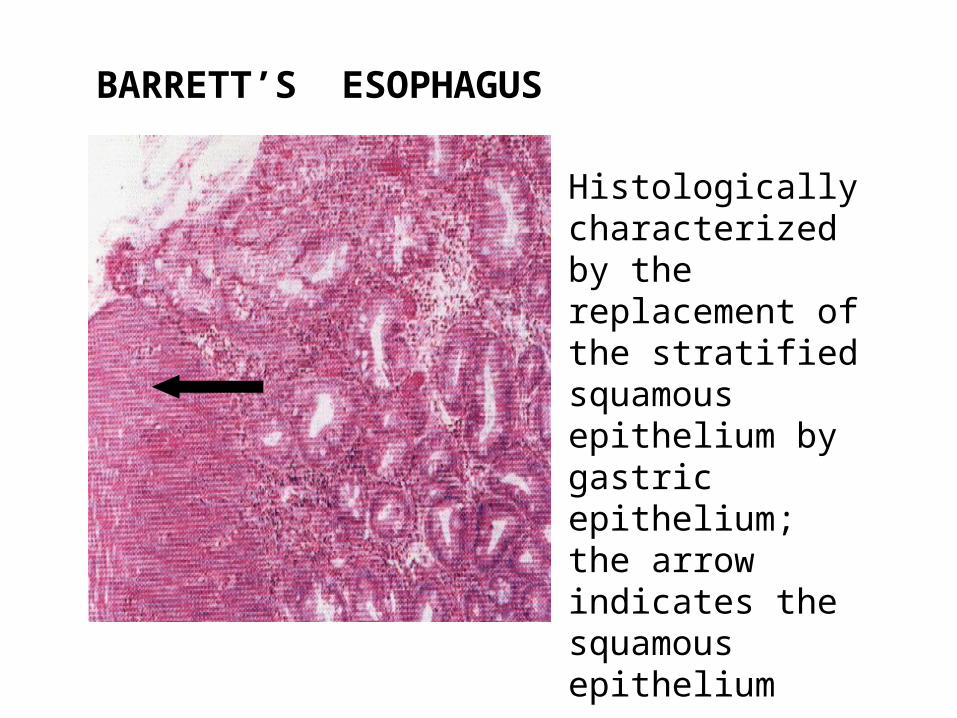
Histologically characterized by the replacement of the stratified squamous epithelium by gastric epithelium; the arrow indicates the squamous epithelium
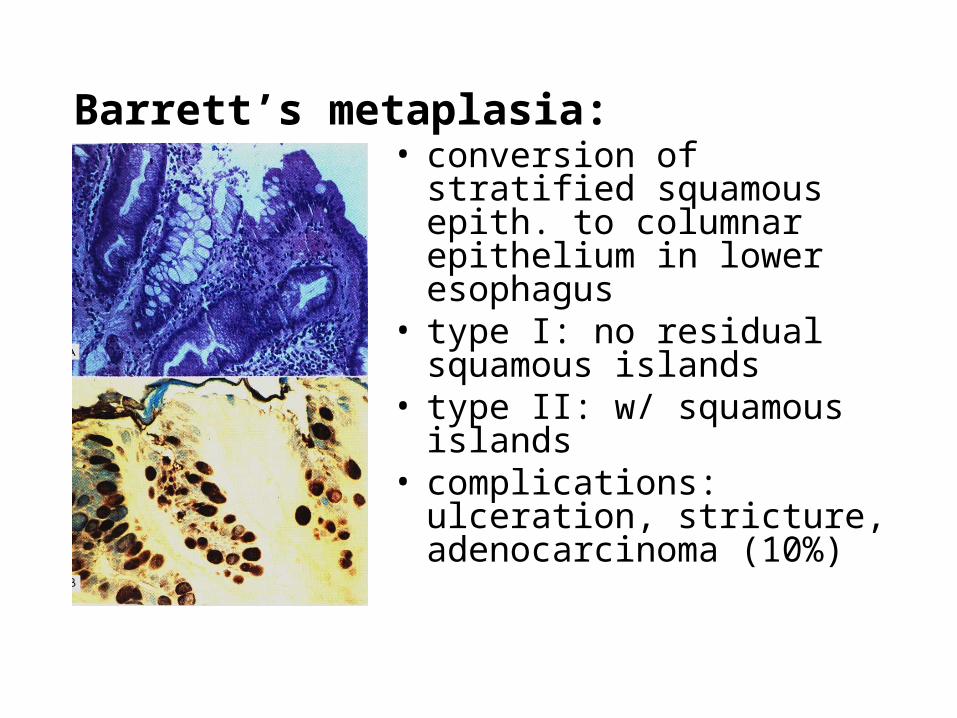
Barrett’s metaplasia:• conversion of stratified
squamous epith. to columnar epithelium in lower esophagus
• type I: no residual squamous islands
• type II: w/ squamous islands
• complications: ulceration, stricture, adenocarcinoma (10%)
Types of Barrett’s metaplasia:
• specialized type (intestinal or colonic)
incomplete = goblet & columnar cells
complete = purely intestinal type cells• cardiac/junctional type = entirely mucin
cells
3cm above GEJ (35cm from incisors)• atrophic fundal type = parietal & chief cells
Dysplasia in Barrett’s metaplasia:
• Low grade - hyperchromatic crowding nuclei• High grade* - glandular distortion & nuclear
hyperchromasia extends to upper portions of eputhelium
* if high grade dysplasia is seen in biopsy, there is 70% chance of carcinoma being present
Infectious esophagitis:
Bacterial
Viral: CMV- submucosal cells w/ inclusions
Herpes - epith. cells w/ ground glass nuclei
multinucleated giant cells
Fungal: Candida - white plaques
usually in middle & lower 1/3
Mucormycoses
Aspergillus
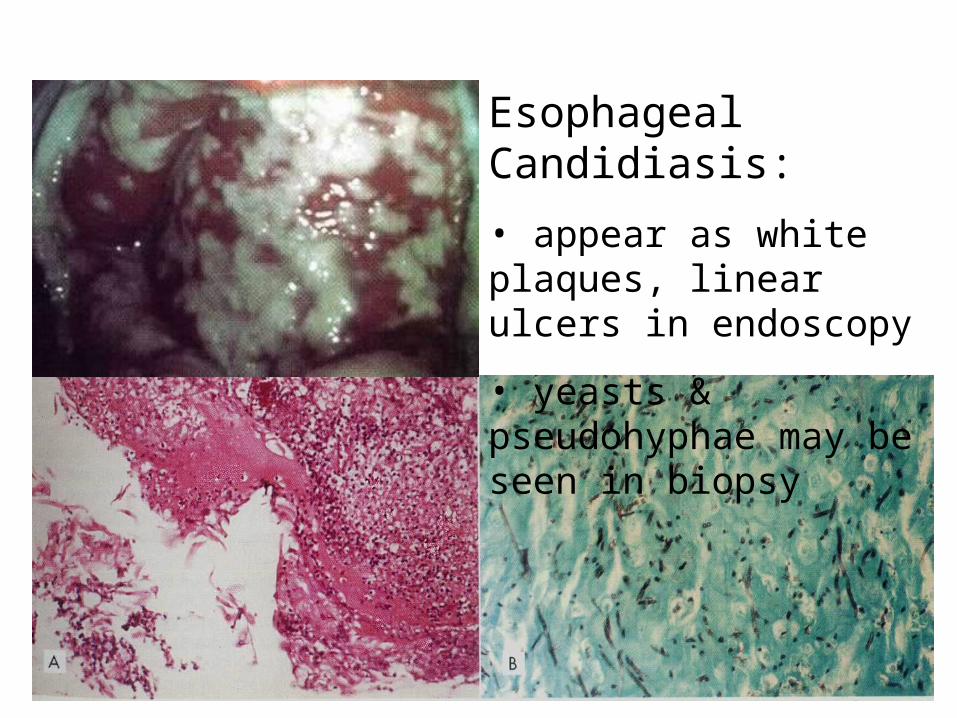
Esophageal Candidiasis:
• appear as white plaques, linear ulcers in endoscopy
• yeasts & pseudohyphae may be seen in biopsy
Benign Lesions:
Inflammatory polyps/fibrovascular polyps– submucosal proliferation of vascularized,
inflammed fibrous stroma w/ eosinophils
– 85% in upper 1/3
– usually pedunculated, solitary
– similar lesions in sstomach
• Squamous papilloma– lower esophagus; may be multiple
– men > 40 y/o
Benign Lesions:
• Adenoma– arises in Barrett’s esophagitis
• Gastrointestinal Stromal Tumors (GIST)– Leiomyoma
• Granular cell tumor
• Localized amyloidosis
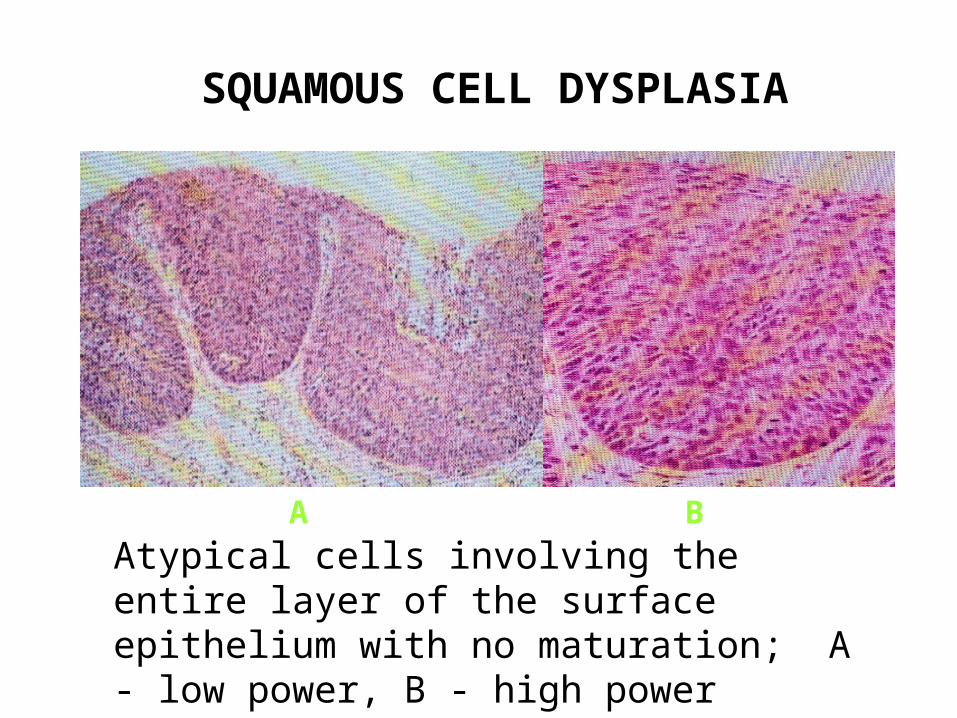
SQUAMOUS CELL DYSPLASIA
Atypical cells involving the entire layer of the surface epithelium with no maturation; A - low power, B - high power
A B
Esophageal Carcinoma
• > 50 y/o; male = female• Sx: dysphagia & emaciation• metastasizes and extends early (no serosa)• patients often die before widespread
metastases• associated with cigarette smoking & alcohol
use
SQUAMOUS CELL CARCINOMA
1. Most common type of malignancy
2. High-risk factors include tabacco use, smoking , alcohol intake
3. Associated with epithelial dysplasia
4. Genetic predisposition
5. Prognosis poor since tumor growth and spread to adjacent structures and lymph nodes are rapid
Squamous Cell Carcinoma of Esophagus:
• 80-85% of all esophageal carcinomas• 10% of all GIT cancers• more common in blacks and males• 12% upper; 56 % middle; 32% lower portion
Verrucous carcinoma:• exophytic growth with pushing margins• rare; slow growing, rarely metastasize
Adenocarcinoma:
• 5-10% of esophageal carcinomas;
2-8% of esophageal malignancies• male > female (5:1), 50y/o• middle or lower 1/3, often involve
gastroesophageal junction• most arise from Barrett’s esophagitis• gross: mass or nodular elevation
Histologic types of adenocarcinoma:
• Intestinal type - same in stomach & intestine
• Diffuse - diffuse infiltration by mucin-producing cells
• Adenosquamous - mixture of squamous cell & adenocarcinoma
*staging same as in SCC; most are at high stages when diagnosed
Esophageal CarcinomaGross: Ulcerative/Polypoid/Diffuse infiltrative
Squamous cell carcinoma• lower 1/3 > middle 1/3 >
upper 1/3 *• squamous cells in
sheets w/ keratinization & desmoplasia
* usually assoc. w/ Plummer-Vinson syndrome
Adenocarcinoma• lower 1/3 (90%)
• epithelial cells in glandular pattern
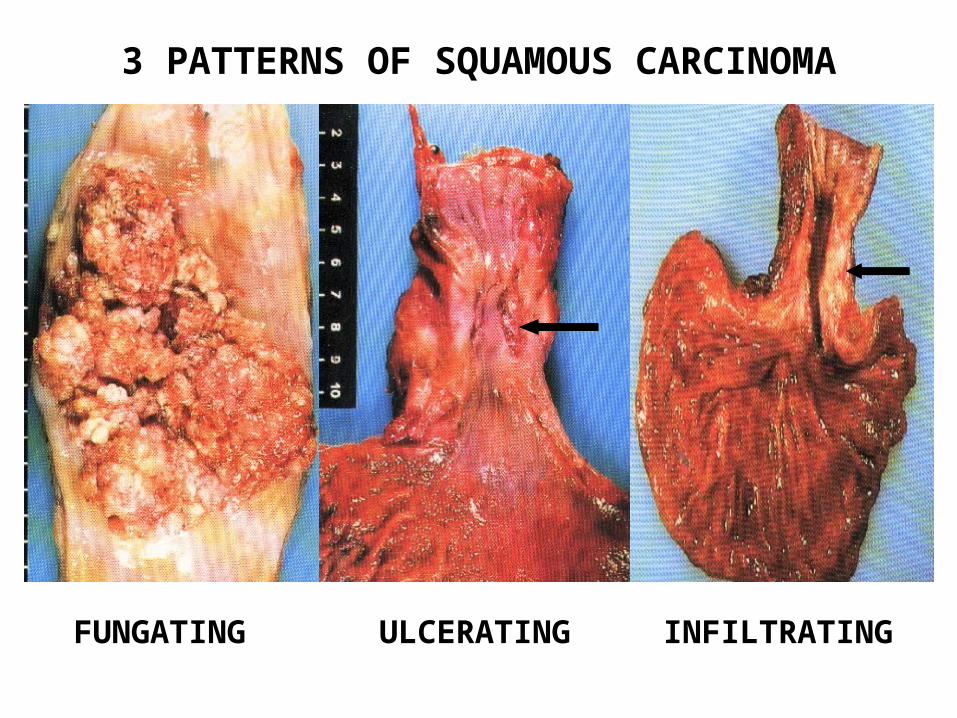
3 PATTERNS OF SQUAMOUS CARCINOMA
FUNGATING ULCERATING INFILTRATING
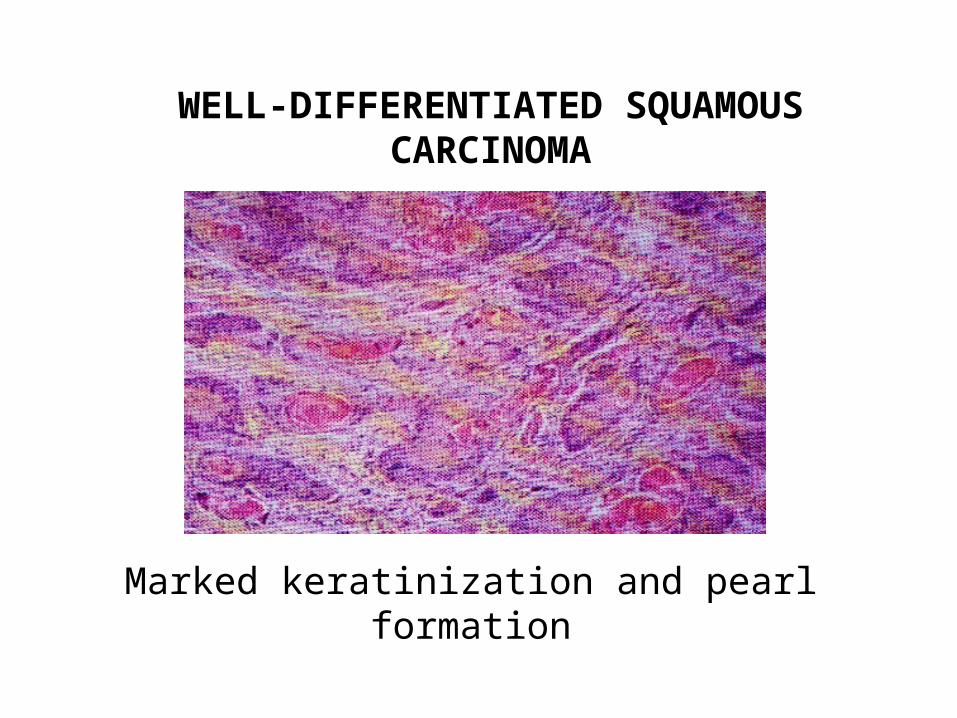
WELL-DIFFERENTIATED SQUAMOUS CARCINOMA
Marked keratinization and pearl formation
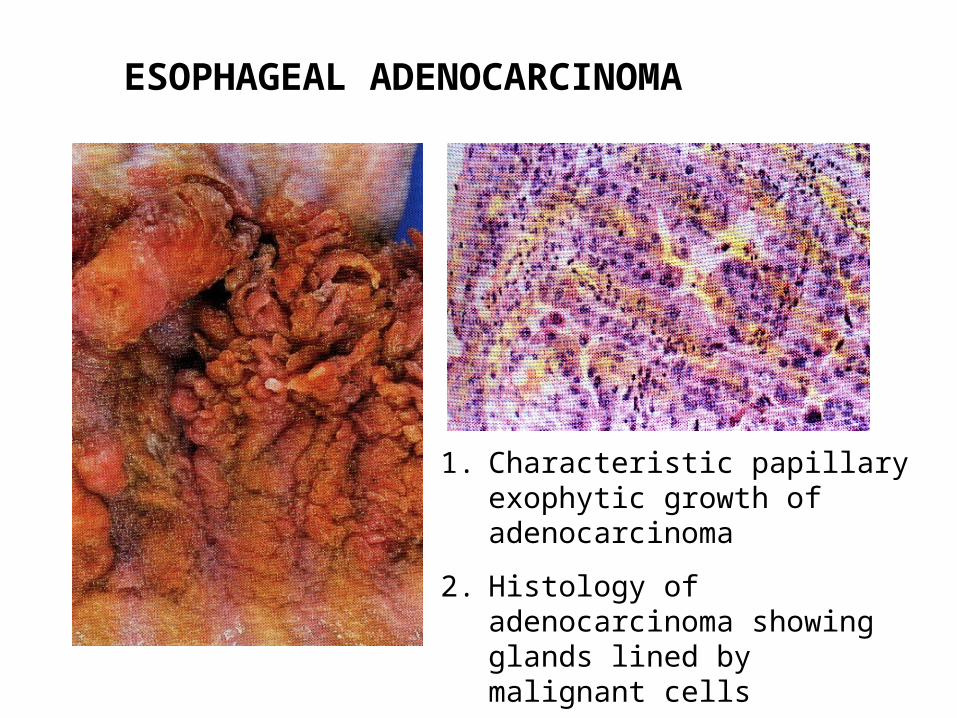
ESOPHAGEAL ADENOCARCINOMA
1. Characteristic papillary exophytic growth of adenocarcinoma
2. Histology of adenocarcinoma showing glands lined by malignant cells
Other malignant tumors tumors:
• Small cell carcinoma
• Leiomyosarcoma
• Malignant lymphoma
• Plasmacytoma
• Malignant melanoma
PART II
PATHOLOGY OF THE
STOMACH AND DUODENUM
Anatomic considerations in the Stomach:• mucosal surface and pits lined by mucus cells• neck mucus cells are progenitors for glandular
epithelium• glands of cardia and antrum similar to neck
mucus cells• fundic glands contain parietal and chief cells• antrum contains endocrine cells for
enteroendocrine, enterochromaffin, Kulchitsky’s or APUD cells
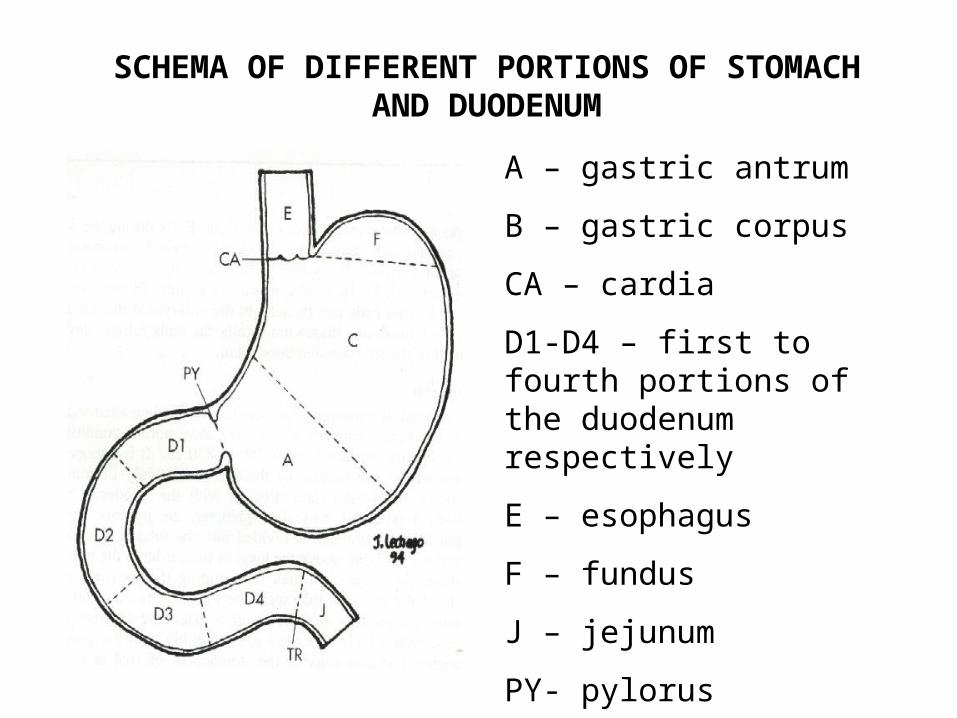
A – gastric antrum
B – gastric corpus
CA – cardia
D1-D4 – first to fourth portions of the duodenum respectively
E – esophagus
F – fundus
J – jejunum
PY- pylorus
TR – angle of Treitz
SCHEMA OF DIFFERENT PORTIONS OF STOMACH AND DUODENUM
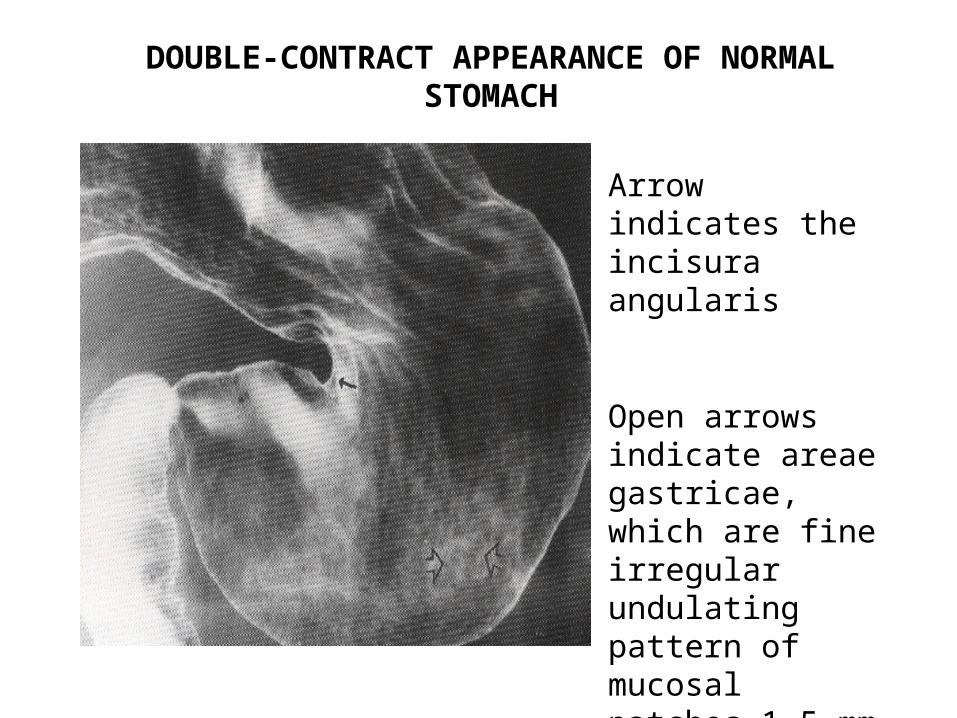
DOUBLE-CONTRACT APPEARANCE OF NORMAL STOMACH
Arrow indicates the incisura angularis
Open arrows indicate areae gastricae, which are fine irregular undulating pattern of mucosal patches 1-5 mm in diameter
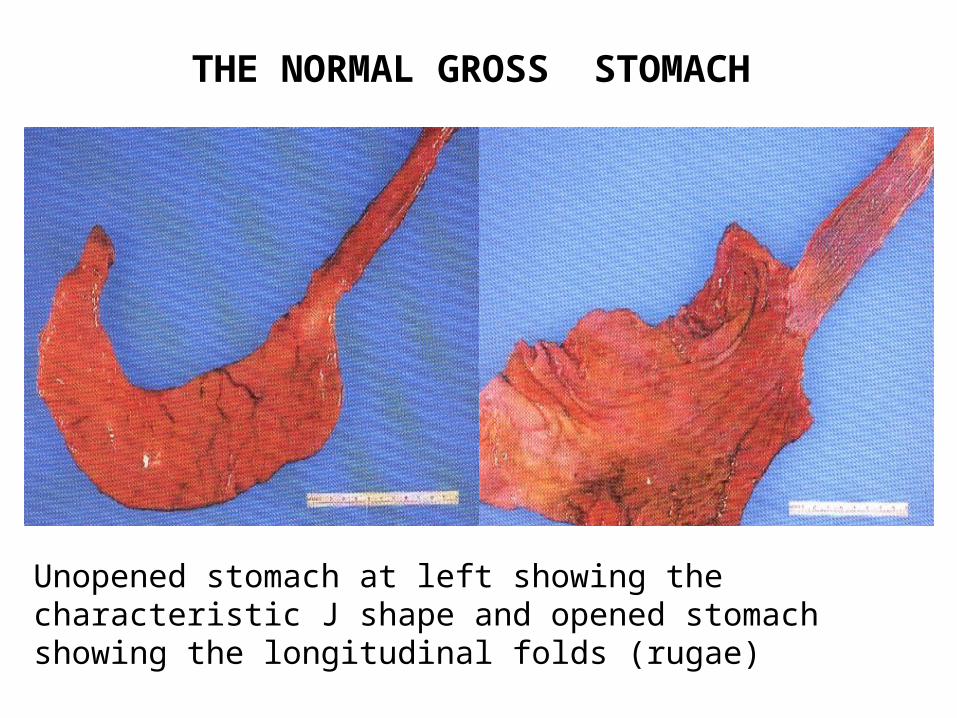
THE NORMAL GROSS STOMACH
Unopened stomach at left showing the characteristic J shape and opened stomach showing the longitudinal folds (rugae)
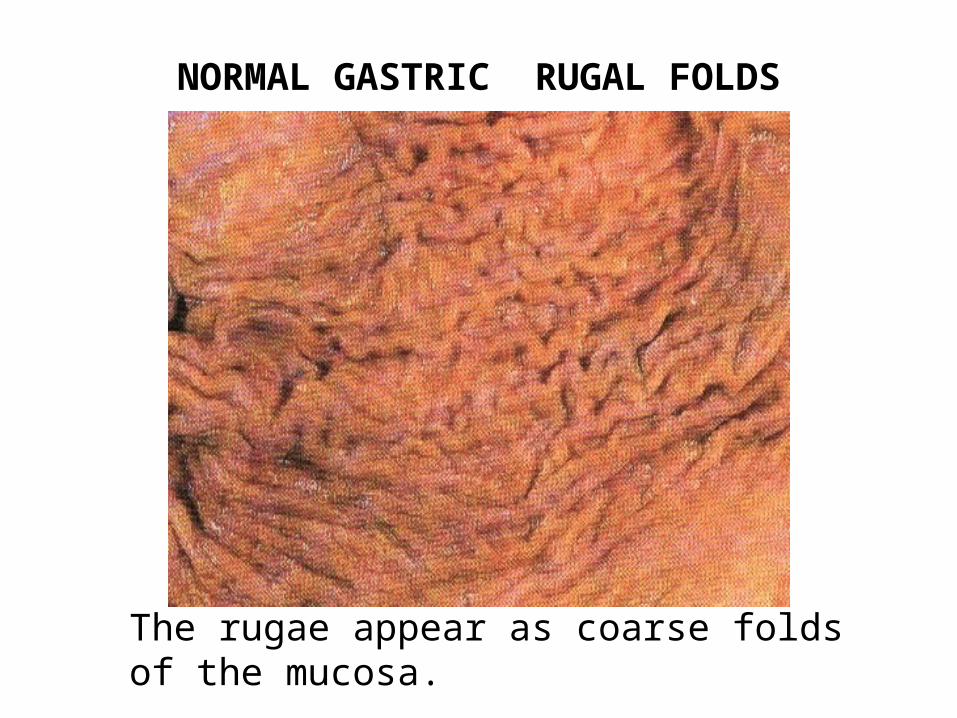
NORMAL GASTRIC RUGAL FOLDS
The rugae appear as coarse folds of the mucosa.
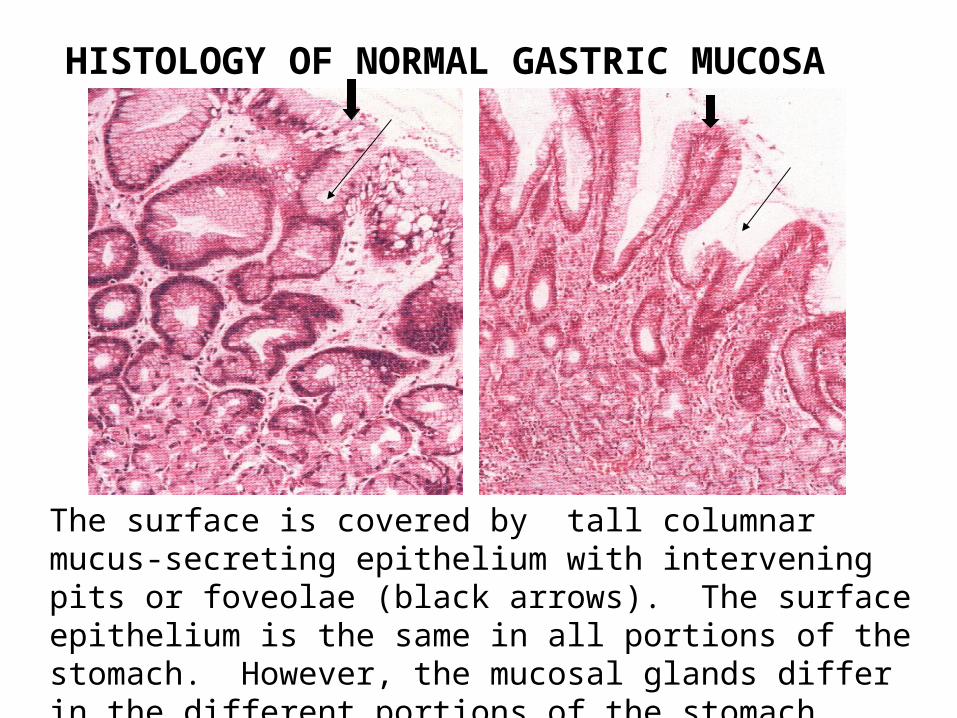
HISTOLOGY OF NORMAL GASTRIC MUCOSA
The surface is covered by tall columnar mucus-secreting epithelium with intervening pits or foveolae (black arrows). The surface epithelium is the same in all portions of the stomach. However, the mucosal glands differ in the different portions of the stomach. The block arrows indicate the surface mucus epithelium.
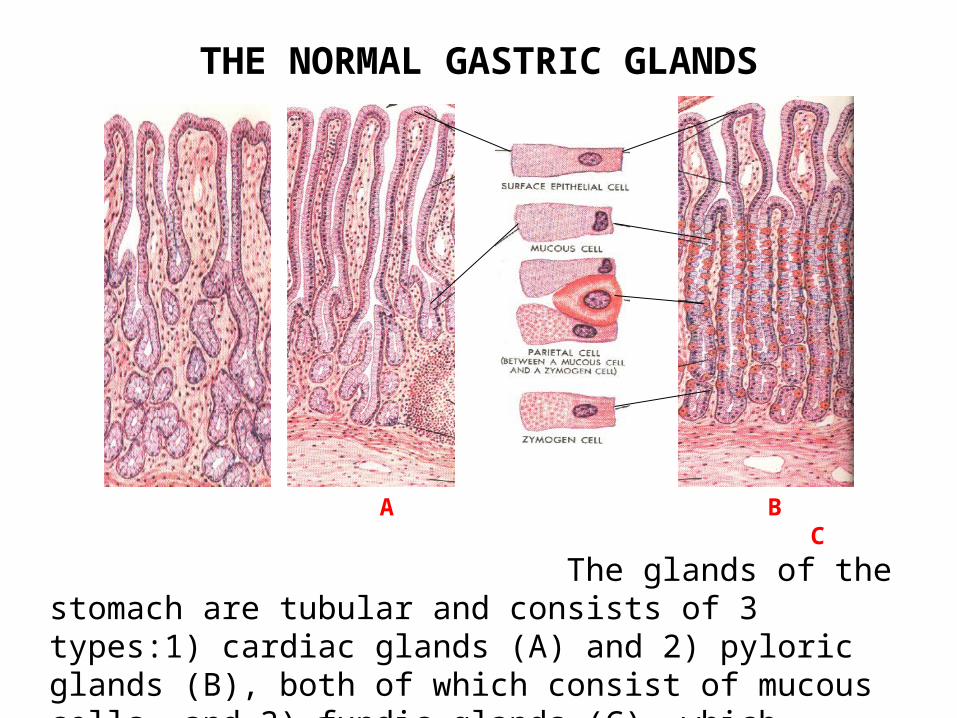
THE NORMAL GASTRIC GLANDS
A B C
The glands of the stomach are tubular and consists of 3 types:1) cardiac glands (A) and 2) pyloric glands (B), both of which consist of mucous cells, and 3) fundic glands (C), which consists of parietal and basophilic or chief cells (C).
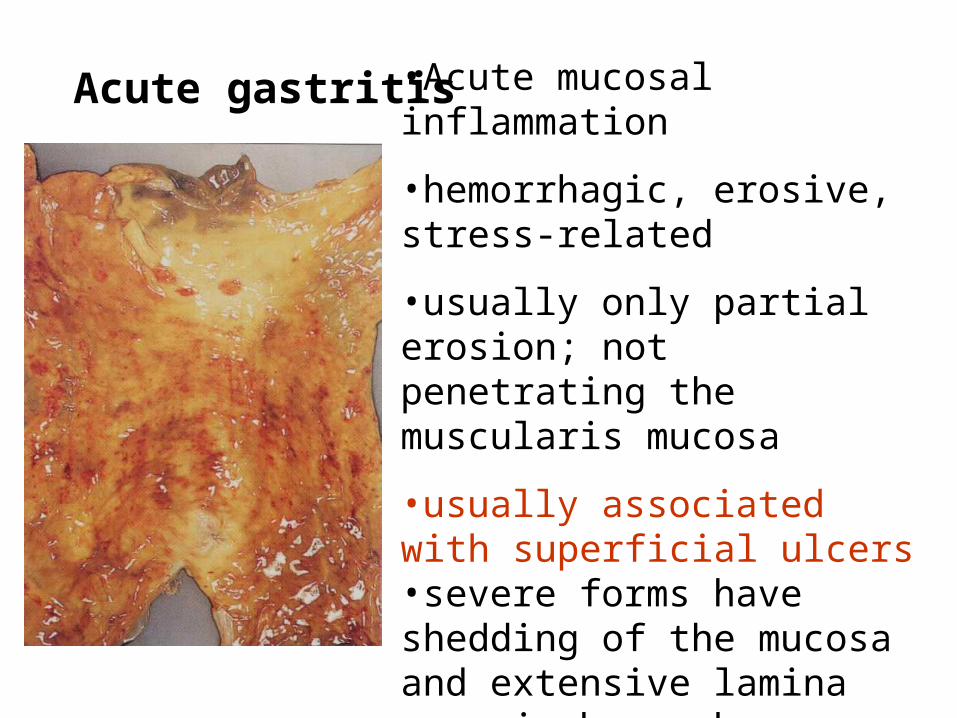
Acute gastritis •Acute mucosal inflammation
•hemorrhagic, erosive, stress-related
•usually only partial erosion; not penetrating the muscularis mucosa
•usually associated with superficial ulcers•severe forms have shedding of the mucosa and extensive lamina propria hemorrhages•mortality can exceed 50% in acute hemorrhagic erosive form
Causes of Acute gastritis:
• excessive alcohol consumption, heavy smoking • chronic aspirin or non-steroidal anti-inflammatory
drugs (NSAID) intake • anti-cancer drugs• hypovolemia / shock• surgery• severe stress• severe burns (Curling’s ulcers)• trauma (when associated with intracranial
pressure - Cushing’s ulcers)
ACUTE GASTRITIS
1. Mechanism of ulcer formation may be involve:
1. back-diffusion of acid secretion
2. decreased bicarbonate buffer production
3. reduced blood flow
4. direct damage to epithelium
5. disruption of mucus secretion
2. Oxygen free radicals have been implicated
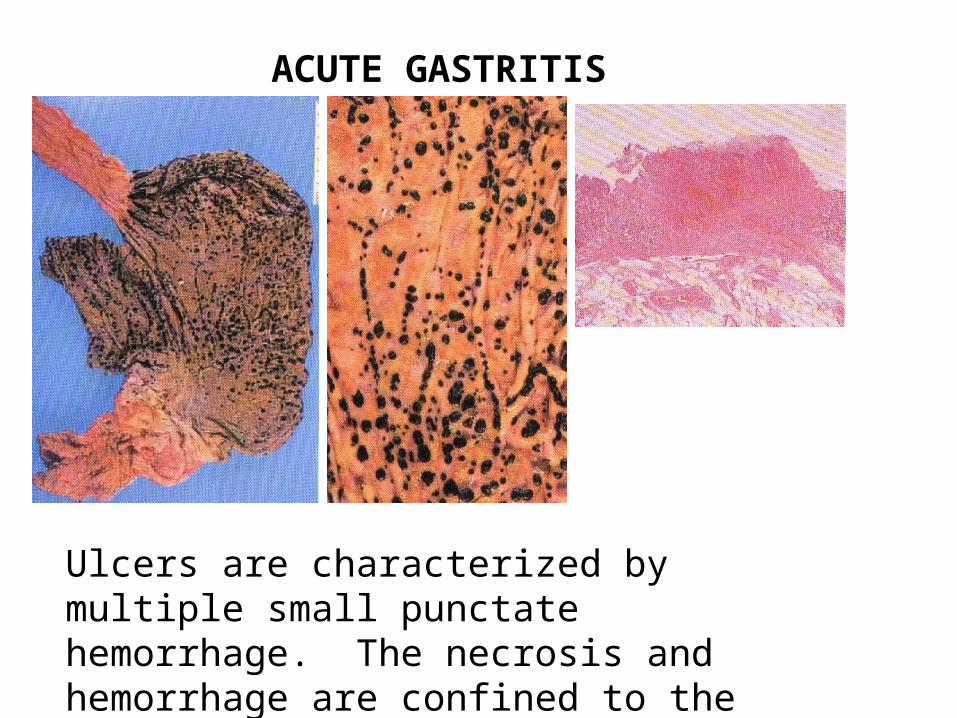
ACUTE GASTRITIS
Ulcers are characterized by multiple small punctate hemorrhage. The necrosis and hemorrhage are confined to the mucosa as seen in histology.
CHRONIC GASTRITIS
1. Common causes are: a. immunologic, associated with pernicious anemia b. infection, especially Helicobacter pylori c. alcohol d. cigarette smoking e. reflux of bile
2. Inflammation may be superficial involving only the upper 3rd of the mucosa or may involve full thickness
3. Mucosal inflammatory changes may progress to atrophy, intestinal metaplasia, dysplasia, and carcinoma
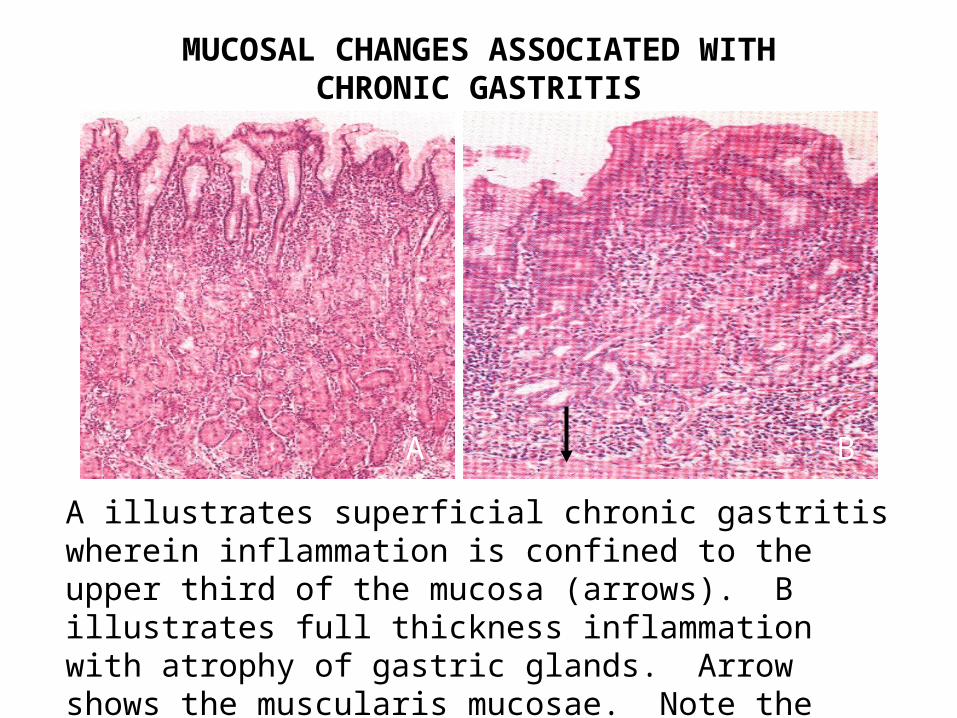
MUCOSAL CHANGES ASSOCIATED WITH CHRONIC GASTRITIS
A illustrates superficial chronic gastritis wherein inflammation is confined to the upper third of the mucosa (arrows). B illustrates full thickness inflammation with atrophy of gastric glands. Arrow shows the muscularis mucosae. Note the reduction in mucosal thickness and loss of gastric glands.
A B
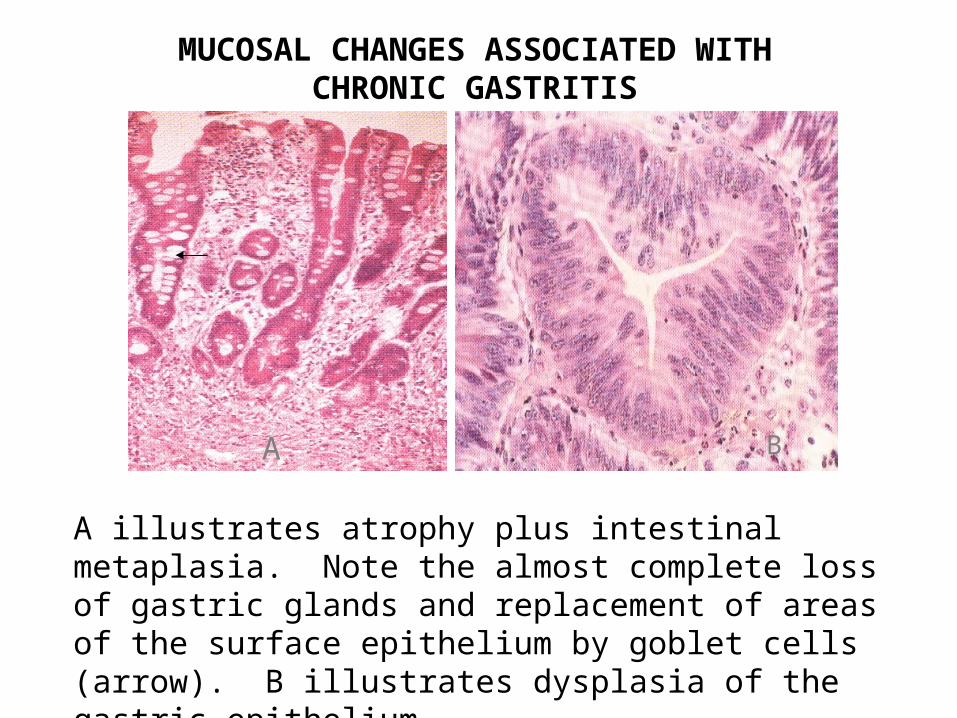
MUCOSAL CHANGES ASSOCIATED WITH CHRONIC GASTRITIS
A illustrates atrophy plus intestinal metaplasia. Note the almost complete loss of gastric glands and replacement of areas of the surface epithelium by goblet cells (arrow). B illustrates dysplasia of the gastric epithelium.
A B
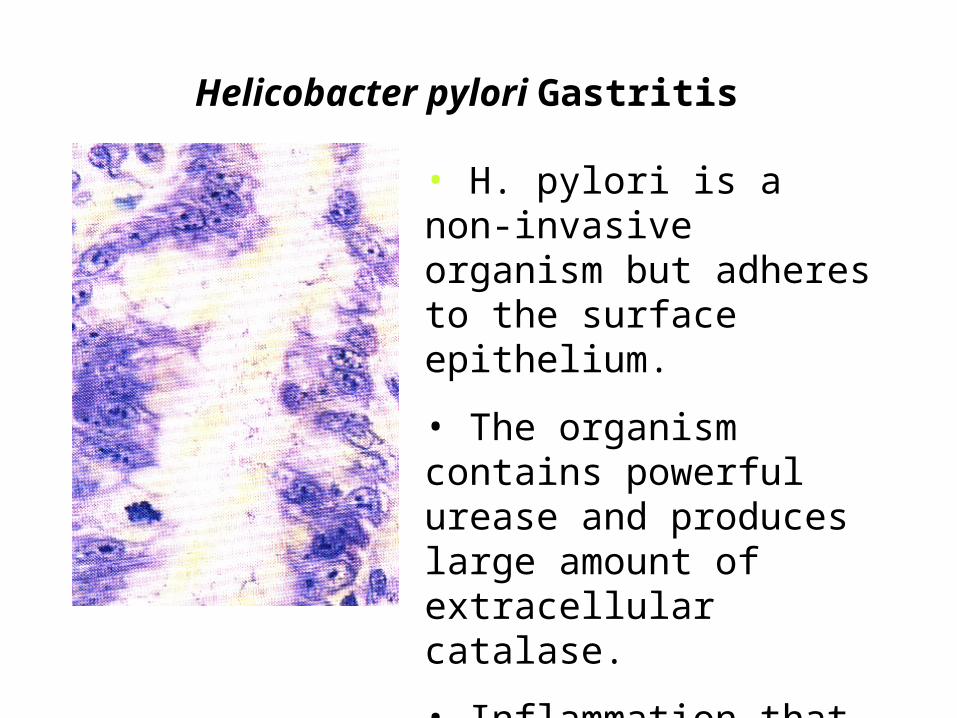
Helicobacter pylori Gastritis
• H. pylori is a non-invasive organism but adheres to the surface epithelium.
• The organism contains powerful urease and produces large amount of extracellular catalase.
• Inflammation that ensues further damages the mucosa.
PEPTIC ULCER DISEASE
1. Often solitary occurring anywhere along the gastrointestinal tract
2. Common location along the antrum of stomach and 1st portion of the duodenum
3. Produced by an imbalance between the gastroduodenal mucosal defense mechanisms and damaging forces
4. Gastric acid and pepsin are requisite for peptic ulceration
5. The role of H. pylori is important
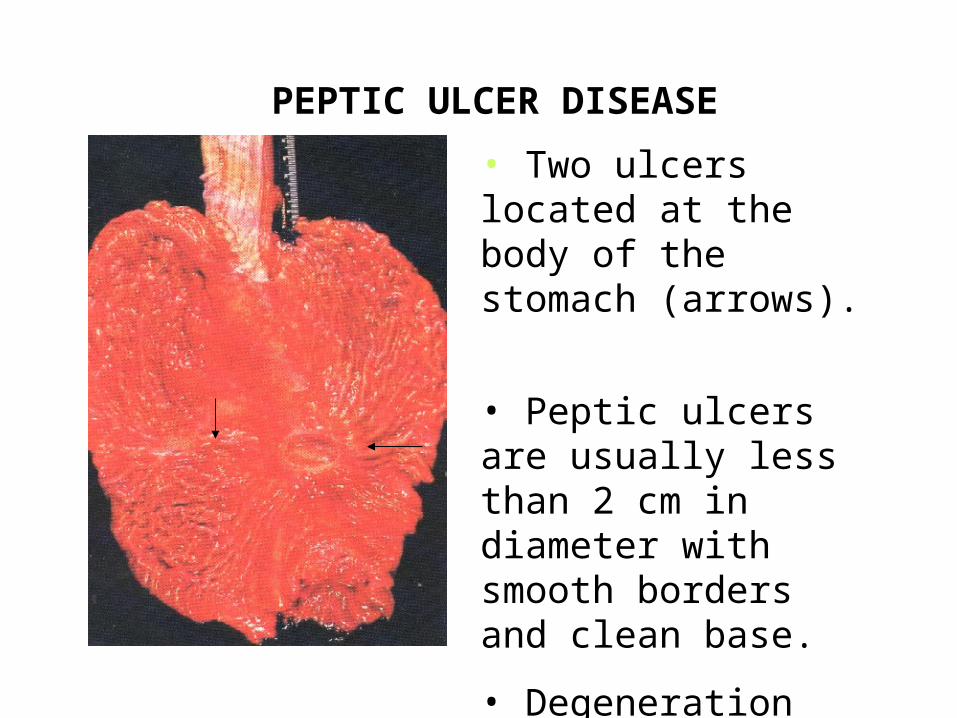
PEPTIC ULCER DISEASE
• Two ulcers located at the body of the stomach (arrows).
• Peptic ulcers are usually less than 2 cm in diameter with smooth borders and clean base.
• Degeneration into malignancy usually does not occur.
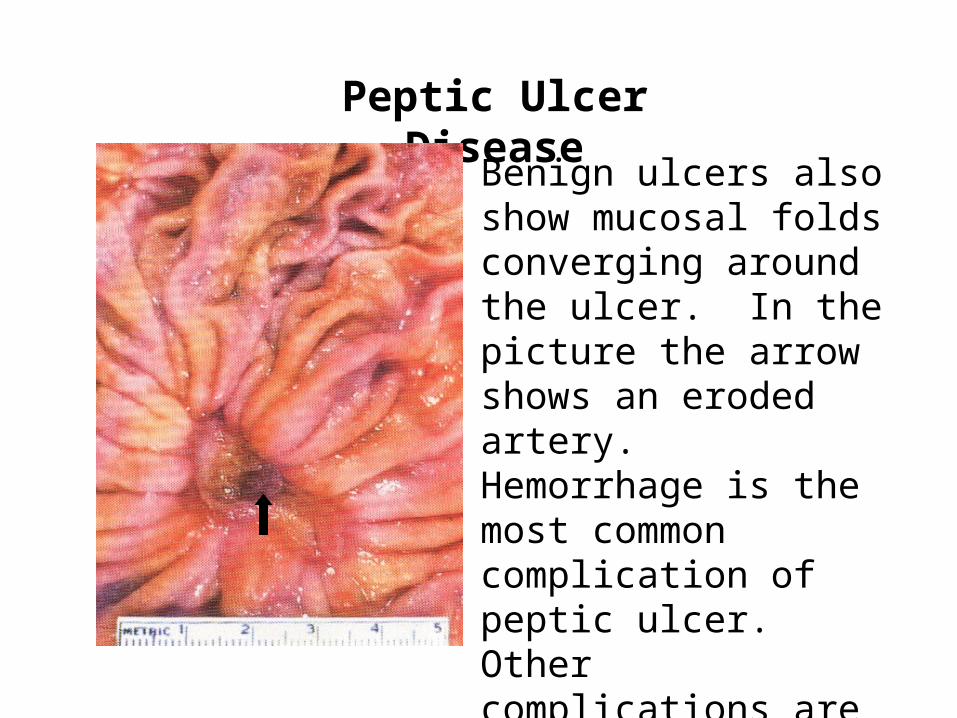
Peptic Ulcer Disease
Benign ulcers also show mucosal folds converging around the ulcer. In the picture the arrow shows an eroded artery. Hemorrhage is the most common complication of peptic ulcer. Other complications are perforation and obstruction due to fibrosis and subsequent stenosis.
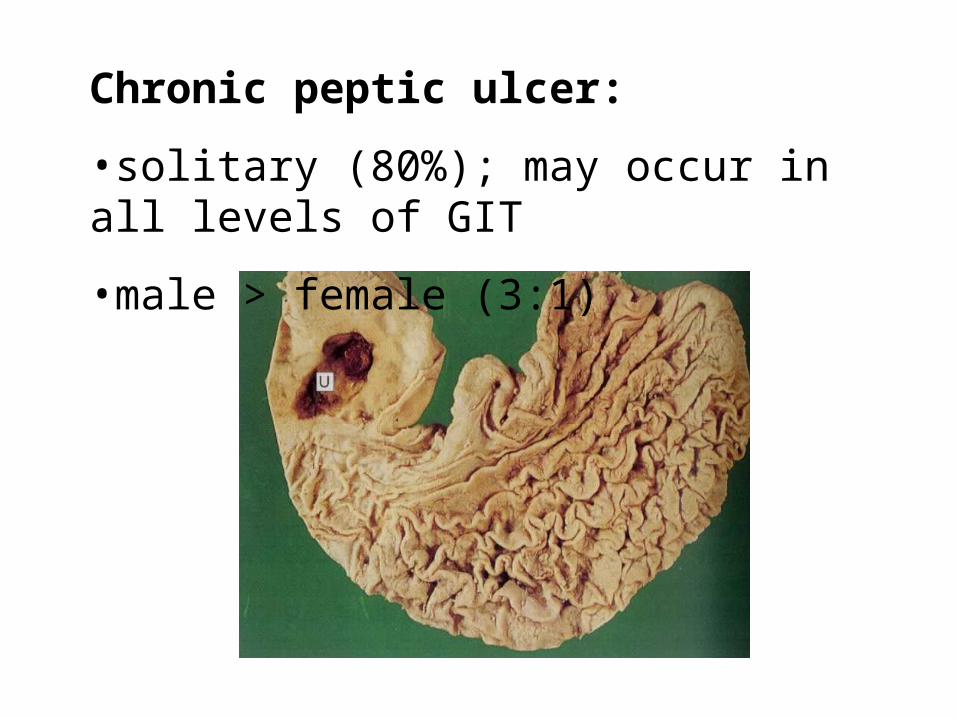
Chronic peptic ulcer:
•solitary (80%); may occur in all levels of GIT
•male > female (3:1)
PEPTIC ULCER DISEASE
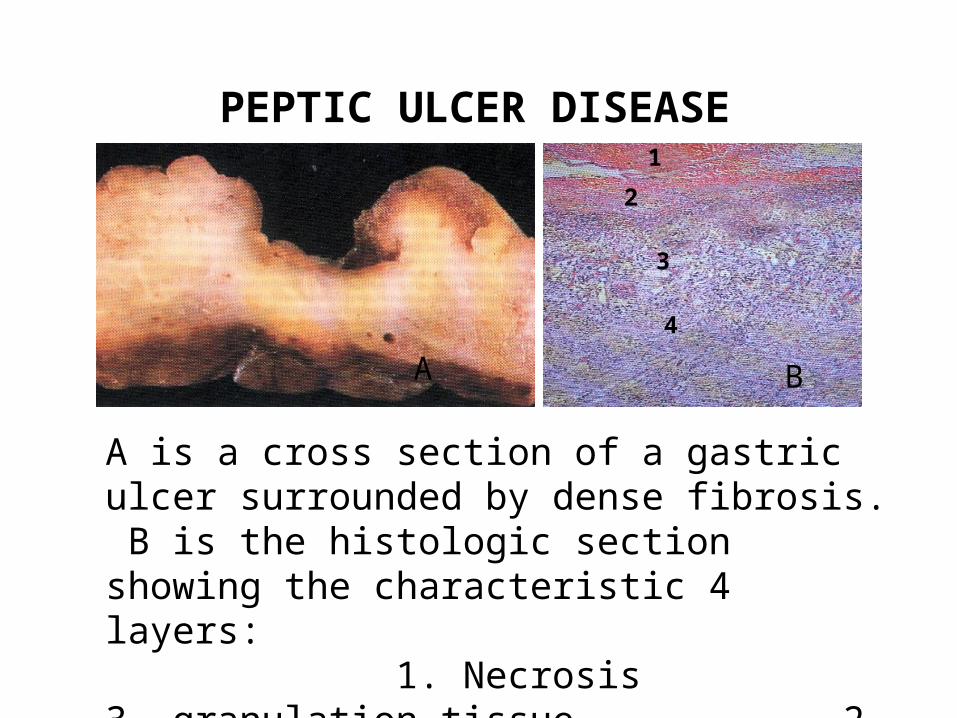
A is a cross section of a gastric ulcer surrounded by dense fibrosis. B is the histologic section showing the characteristic 4 layers: 1. Necrosis 3. granulation tissue 2. inflammatory cells 4. fibrosis.
1
2
3
4
A B
GASTRIC CARCINOMA
1. Incidence reveals marked national variation
2. Etiologic factors, probably dietary in nature, appear to act early in the life of individuals
3. Within a given country, a higher incidence is often found in mountainous regions suggesting possible role of soils and trace elements
4. The role of H. pylori chronic gastritis has been recognized
5. Gastric atrophy, intestinal metaplasia and dysplasia are recognized are predisposing lesions
GROSS PATTERNS OF GASTRIC CARCINOMA
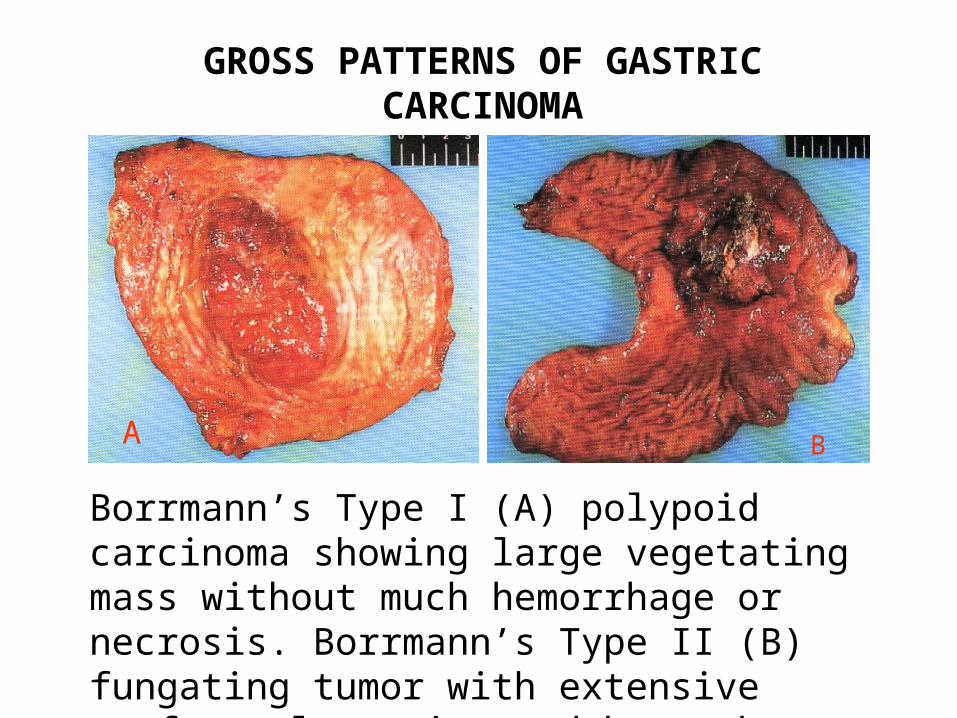
Borrmann’s Type I (A) polypoid carcinoma showing large vegetating mass without much hemorrhage or necrosis. Borrmann’s Type II (B) fungating tumor with extensive surface ulceration and hemorrhage.
A B
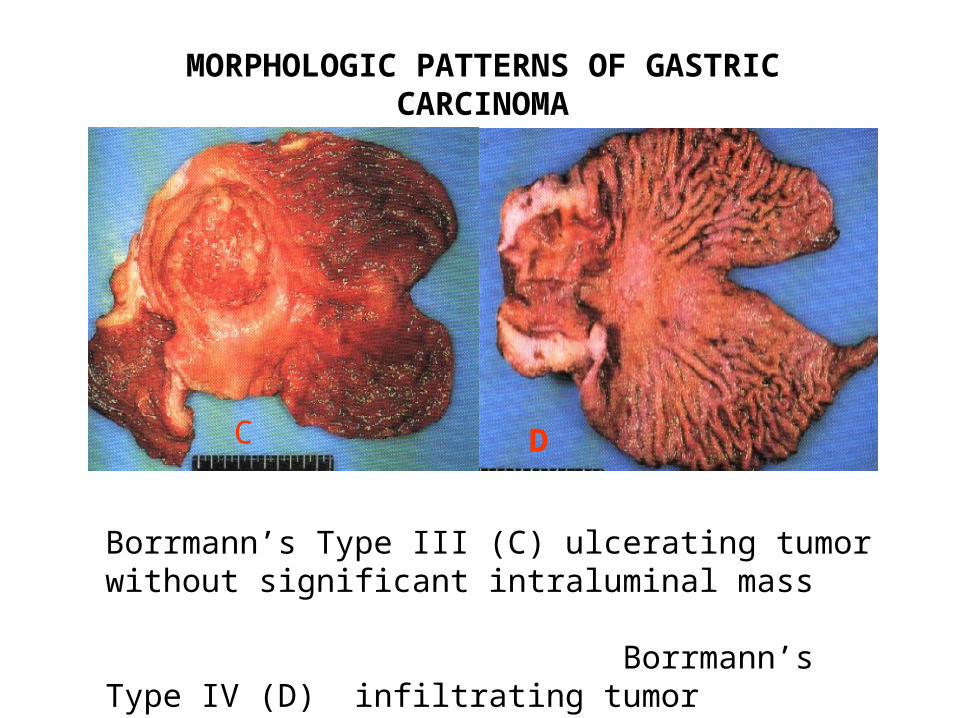
MORPHOLOGIC PATTERNS OF GASTRIC CARCINOMA
Borrmann’s Type III (C) ulcerating tumor without significant intraluminal mass Borrmann’s Type IV (D) infiltrating tumor involving the entire wall
C D
Part III
PATHOLOGY
OF THE
SMALL AND LARGE
INTESTINES
ANATOMY OF SMALL INTESTINE
1. Measures about 27 feet long and extends from the gastric pylorus to the ileocecal valve
2. Divided into the 1) duodenum, 2) jejunum and 3) ileum
3. Characterized by numerous mucosal folds and villi
4. The basic structure of all portions is similar
5. Main functions are digestion, absorption and immunologic defense
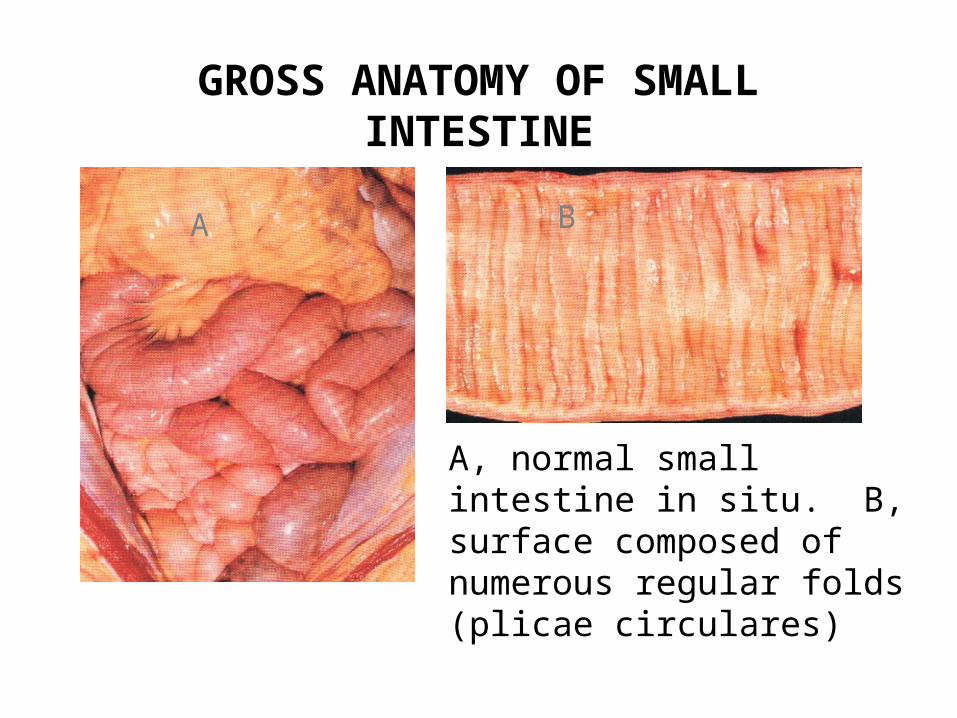
GROSS ANATOMY OF SMALL INTESTINE
A B
A, normal small intestine in situ. B, surface composed of numerous regular folds (plicae circulares)
HISTOLOGIC FEATURES OF SMALL INTESTINE
1. Intestinal surface is studded with innumerable villi.
2. At their bases, the simple tubular invaginations (crypts of Lieberkühn) extend to the muscularis mucosae but do not penetrate it.
3. Villi are fingerlike or leaflike mucosal evaginations lined by epithelium with a highly cellular connective tissue core containing lamina propria, a capillary network and lacteals.
HISTOLOGY OF SMALL INESTINE
4. The lining is composed of:
- absorptive cells
- goblet cells
- cup cells
- Paneth’s cells
- undifferentiated crypt cells
- tuft and M cells
- endocrine cells
FUNCTIONS OF SMALL INTESTINAL LINING CELLS
Absorptive cells - most abundant cells on the villi; absorb various nutrients including lipids, sugars & amino acids; possess enzymes for terminal digestion of carbohydrates & proteins; have conspicuous brush border.
Goblet cells - secrete mucus, ions and water; most abundant in the crypts; distended by mucus assuming the shape of a brandy goblet; increase in number along the length of the small intestine being most numerous in the lower ileum.
Cup cells - not easily seen; may have affinity for distinctive bacterial pathogens and thus may play a role in the initiation of intestinal disease
M and Tuft cells: M cells play a role in protein uptake and a route for selective antigen absorption; role of Tuft cells is unknown.
Paneth’s cells - occur at the base of the crypts; have secretory granules contain arginine-rich basic protein, glycoproteins and lysozyme; lysozyme is believed to play a major role in bacterial protection.
Endocrine cells - interspersed among the absorptive cells; produce hormones essential for digestion and intestinal motility.
Undifferentiated crypt cells - most abundant at the lower crypt; responsible for the replacement of all types of intestinal cell
HISTOLOGY OF SMALL INTESTINE
A B C
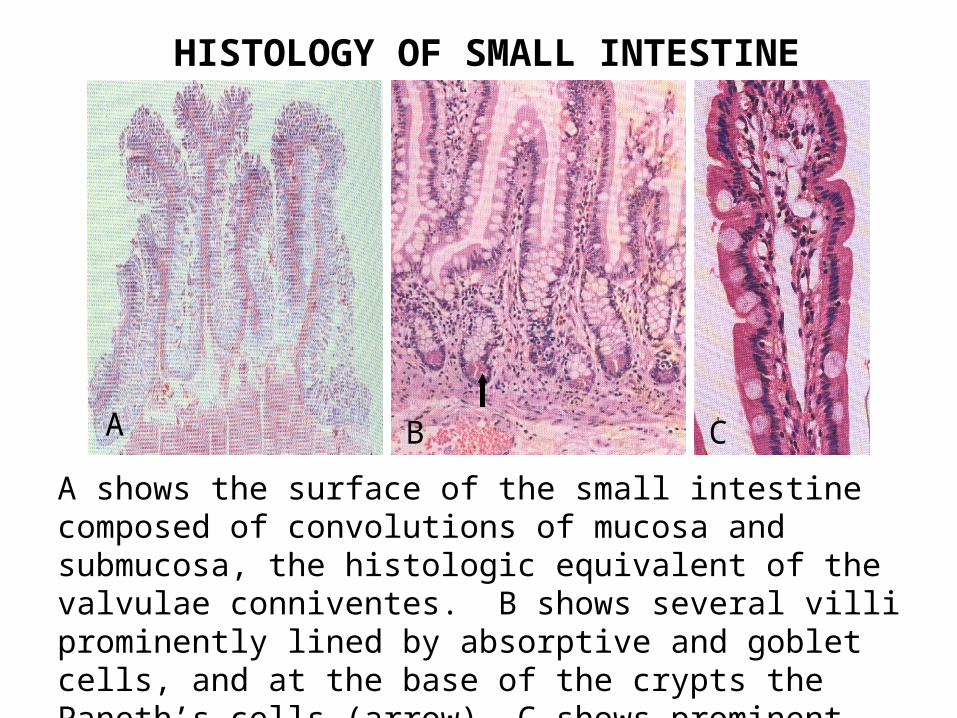
A shows the surface of the small intestine composed of convolutions of mucosa and submucosa, the histologic equivalent of the valvulae conniventes. B shows several villi prominently lined by absorptive and goblet cells, and at the base of the crypts the Paneth’s cells (arrow). C shows prominent brush border, absorptive and goblet cells and central empty lacteal space.
HISTOLOGY OF SMALL INTESTINE
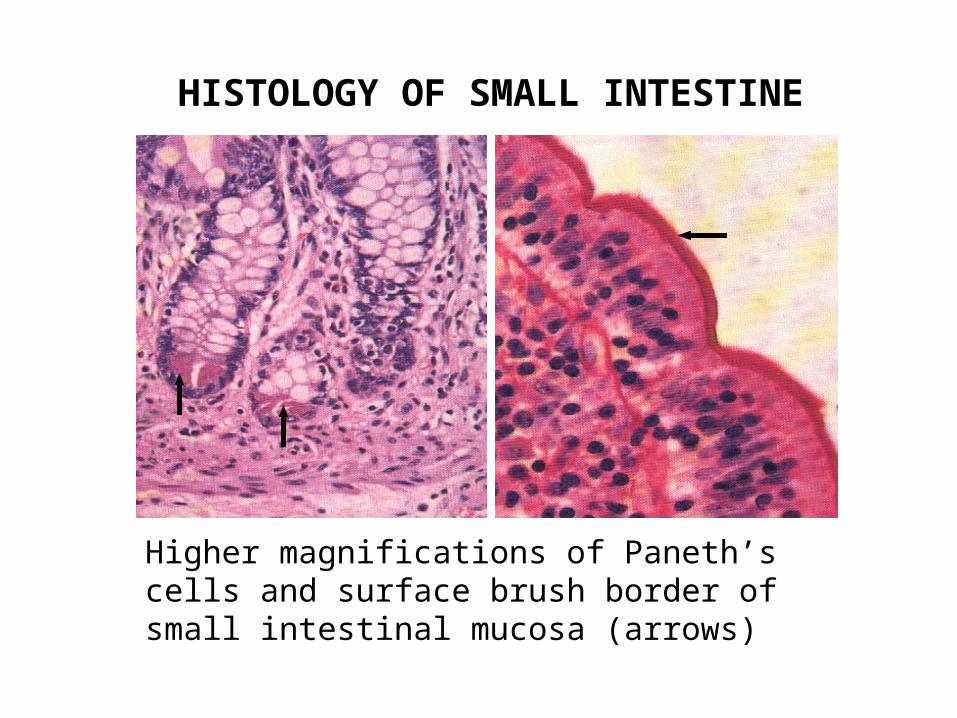
Higher magnifications of Paneth’s cells and surface brush border of small intestinal mucosa (arrows)
ANATOMY OF THE DUODENUM
1. Approximately 25 cm long and has 4 parts.
2. It is roughly C shaped, enclosing in its concavity the head of the pancreas, which is adherent to it.
3. Except for its 1st part, it is retroperitoneal.
4. The common bile and pancreatic ducts enter the 2nd portion at the ampula of Vater.
5. The ligament of Treitz is attached to the 4th portion, which is difficult to distinguish from the 3rd portion.
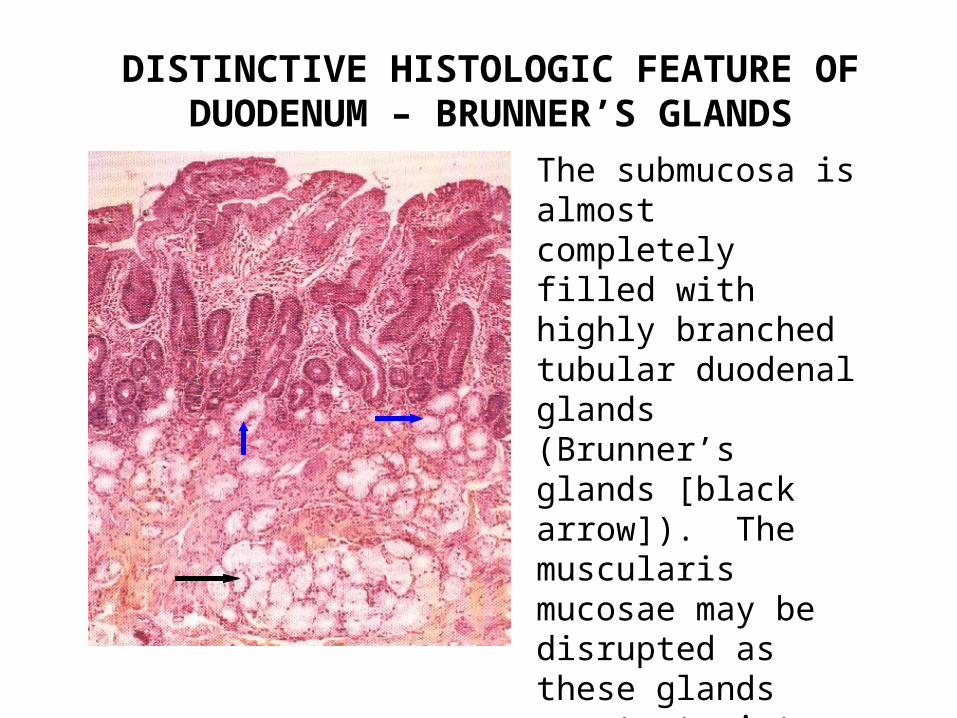
DISTINCTIVE HISTOLOGIC FEATURE OF DUODENUM – BRUNNER’S GLANDS
The submucosa is almost completely filled with highly branched tubular duodenal glands (Brunner’s glands [black arrow]). The muscularis mucosae may be disrupted as these glands penetrate into the deep lamina propria of the mucosa (blue arrows)
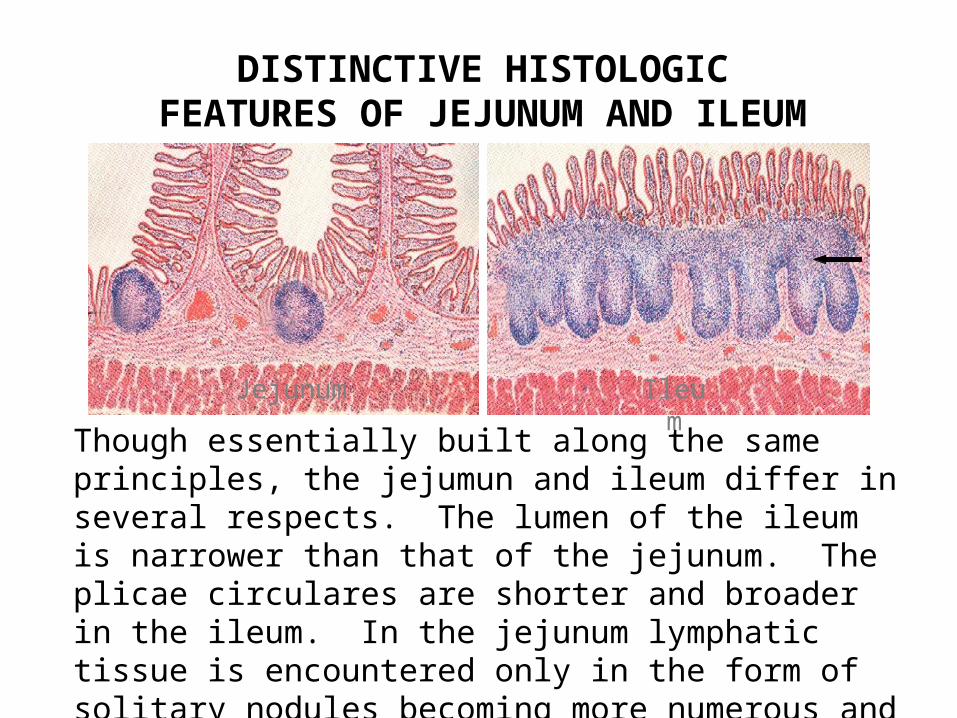
DISTINCTIVE HISTOLOGIC FEATURES OF JEJUNUM AND ILEUM
Jejunum Ileum
Though essentially built along the same principles, the jejumun and ileum differ in several respects. The lumen of the ileum is narrower than that of the jejunum. The plicae circulares are shorter and broader in the ileum. In the jejunum lymphatic tissue is encountered only in the form of solitary nodules becoming more numerous and more pronounced in the ileum. Aggregate nodules are called Peyer’s Patches (arrow).
ANATOMY OF THE LARGE INTESTINE
1. Consists of the cecum, vermiform appendix, ascending, transverse, descending and sigmoid colon, and anus.
2. Begins at the ileocecal valve and end at the anus; approx. 1.5 meters in length
3. Ascending colon extends from the ileocecal valve to the hepatic flexure and lies retroperitoneally.
4. The transverse colon is the longest; extends across the abdomen and attached to the stomach by the gastrocolic ligament; the omentum is attached to its anterior surface
5. Descending colon begins from the hepatic flexure and at the pelvic brim is continuous with the sigmoid.
9. The sigmoid colon passes opposite the third sacral vertebra to become the rectum
10. The rectum curves gently downward and anteriorly along the sacrococcygeal concavity onto the pelvic diaphragm for a distance of about 12 cm. It abuts against the prostate or the vagina inferiorly before turning posteriorly and caudad through the pelvic floor to become the anal canal at the dentate line.
11. Taeniae coli, a continuous coat of the longitudinal bands of the muscularis propria, runs from the cecum to the rectum. It is absent in the appendix and rectum.
12. Divided into segments called haustra, which is essential for colonic function.
13. Plicae semilunares are cresentric folds between sacculations that project into the lumen.
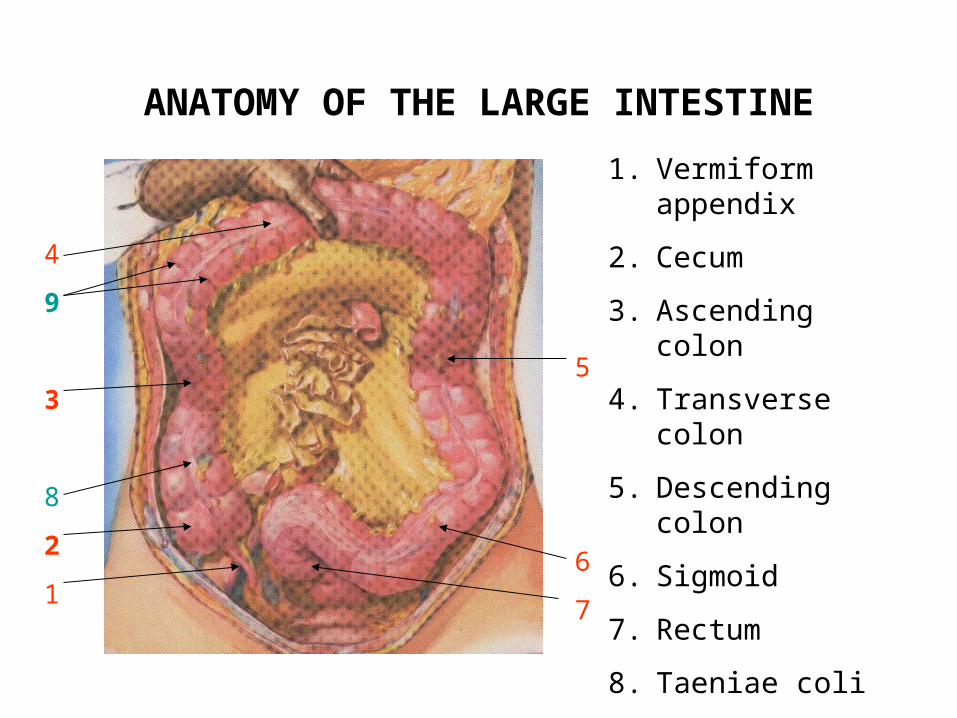
ANATOMY OF THE LARGE INTESTINE
4
9
3
8
2
1
5
6
7
1. Vermiform appendix
2. Cecum
3. Ascending colon
4. Transverse colon
5. Descending colon
6. Sigmoid
7. Rectum
8. Taeniae coli
9. Haustrations
ANATOMY OF LARGE INTESTINE
2
1
3
4
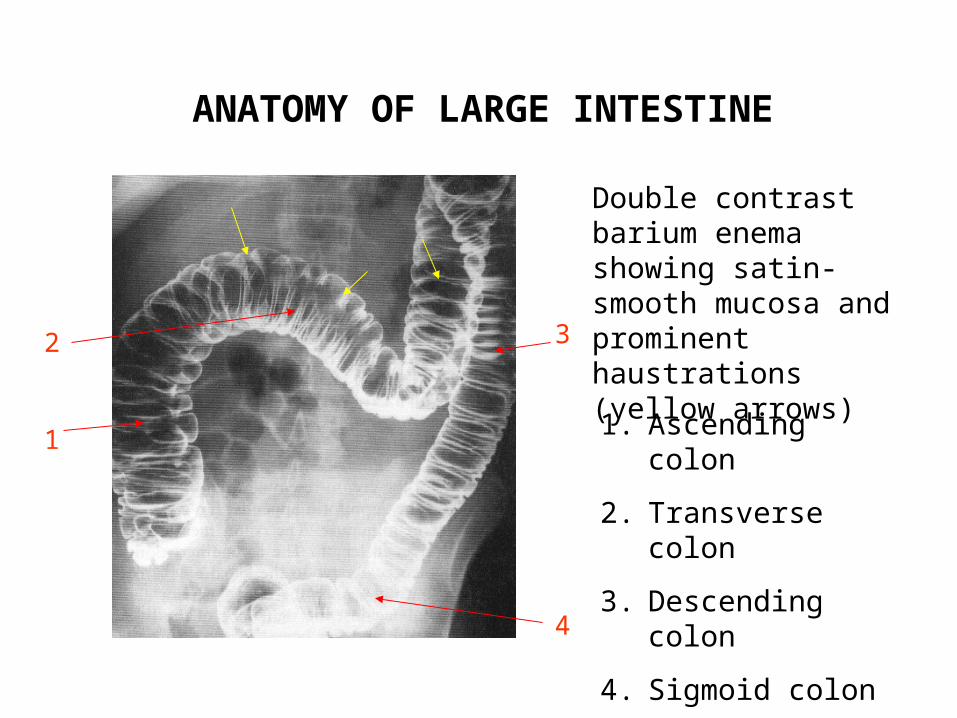
Double contrast barium enema showing satin-smooth mucosa and prominent haustrations (yellow arrows)
1. Ascending colon
2. Transverse colon
3. Descending colon
4. Sigmoid colon
ANATOMY OF LARGE INTESTINE
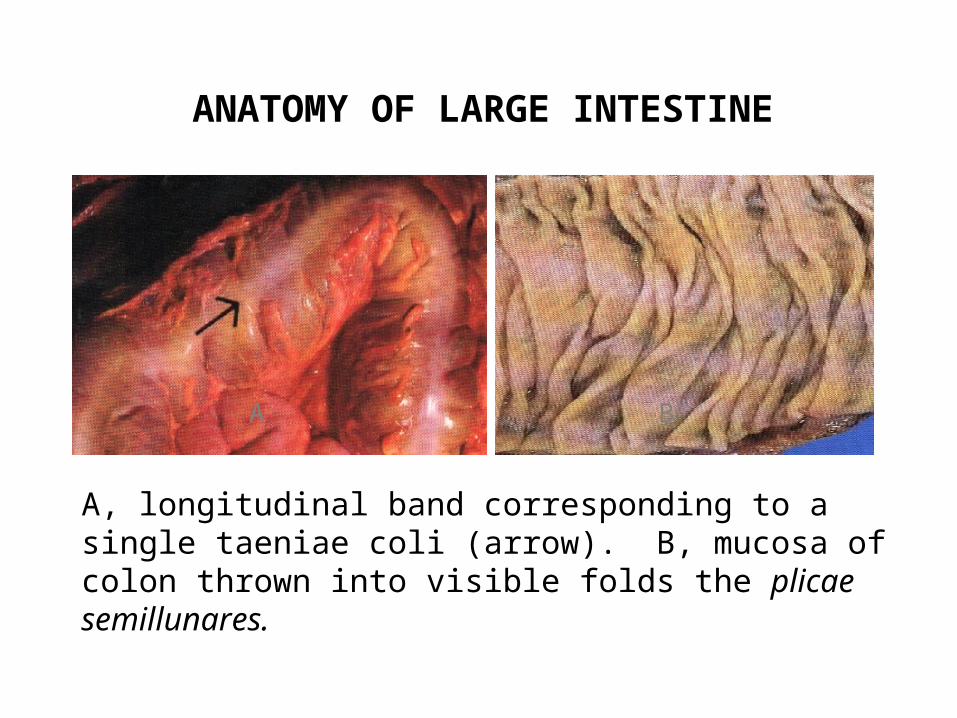
A, longitudinal band corresponding to a single taeniae coli (arrow). B, mucosa of colon thrown into visible folds the plicae semillunares.
A B
HISTOLOGY OF LARGE INTESTINE
1. Consists of smooth mucosal membrane without folds, except distally in the rectum
2. Epithelium is columnar without villi but with abundance of goblet cells and small number of endocrine cells.
• . The glands (crypts of Lieberkühn) are typically long, extending from the lumen to the muscularis mucosae and clustered into groups of five or six, separated by deep furrows. The crypts are lined by overlapping absorptive and goblet cells, and endocrine cells.
• No Paneth’s cells
• Like the ileum, the large intestine has large number of lymphoid tissue
HISTOLOGY OF LARGE INTESTINE
A B C
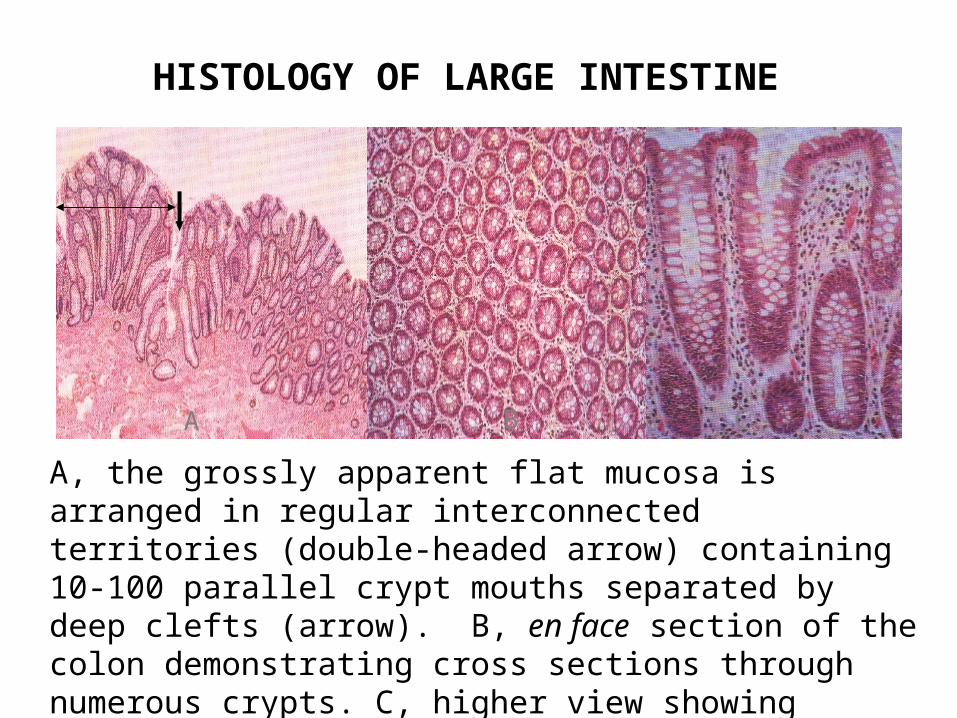
A, the grossly apparent flat mucosa is arranged in regular interconnected territories (double-headed arrow) containing 10-100 parallel crypt mouths separated by deep clefts (arrow). B, en face section of the colon demonstrating cross sections through numerous crypts. C, higher view showing absorptive and goblet cells lining the crypts.
CHOLERA
1. A form of enterotoxigenic diarrhea resulting from infection with Vibrio cholerae.
2. Cholera toxin binds to a specific receptor on epithelial cells of jejunum, which leads to increased adenylate cyclase activity, which in turn results in high cyclic-AMP levels in the intestinal mucosa.
3. Increased cyclic-AMP causes the absorptive cells to secrete large amount of water and sodium.
4. Bacteria do not invade host tissue.
5. Histologic changes are very mild and intestine may appear normal.
BACILLARY DYSENTERY
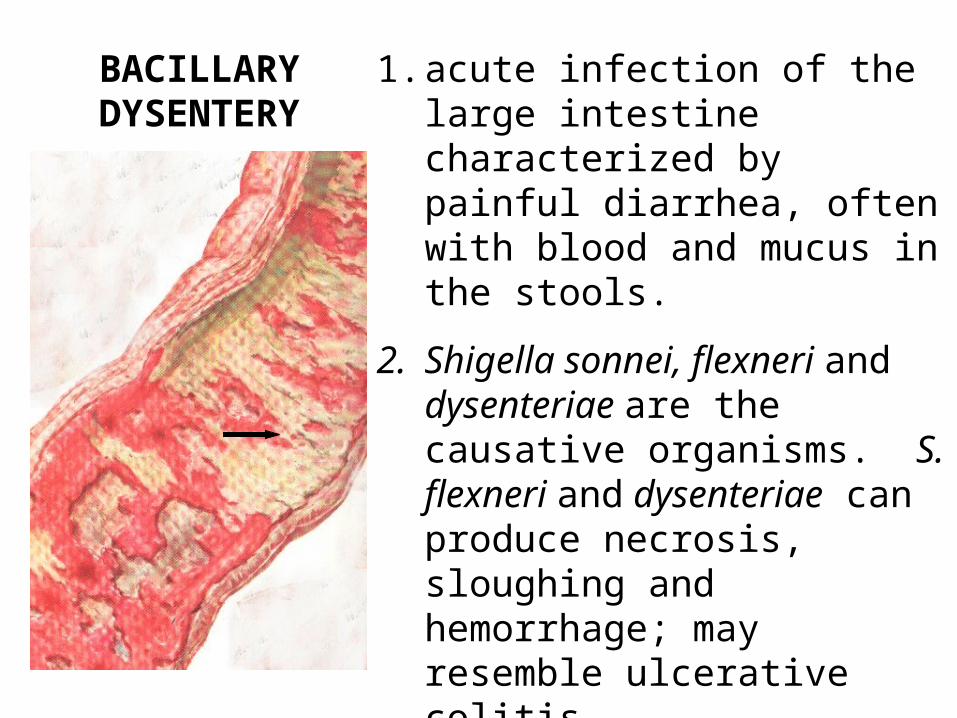
1. acute infection of the large intestine characterized by painful diarrhea, often with blood and mucus in the stools.
2. Shigella sonnei, flexneri and dysenteriae are the causative organisms. S. flexneri and dysenteriae can produce necrosis, sloughing and hemorrhage; may resemble ulcerative colitis.
3. Denuded areas are soon covered with fibrinopurument exudate (arrow).
AMEBIC DYSENTERY
1. Disease of large intestine resulting from infection with the protozoan Entamoeba histolytica.
2. Vegetative form in large intestine of passed out in the stools of infected persons; when ingested, resistant to gastric juice; cyst wall is dissolved on reaching the intestine, thus liberating the active ameba.
3. Ameba secrete a cytolytic enzyme which enable them to pass through the intestinal epithelium.
4. The disease can lead to discrete oval ulcers, which are characteristically ‘flask-shaped’ in section, or to a diffuse colitis
MORPHOLOGY OF AMEBIC COLITIS
A B
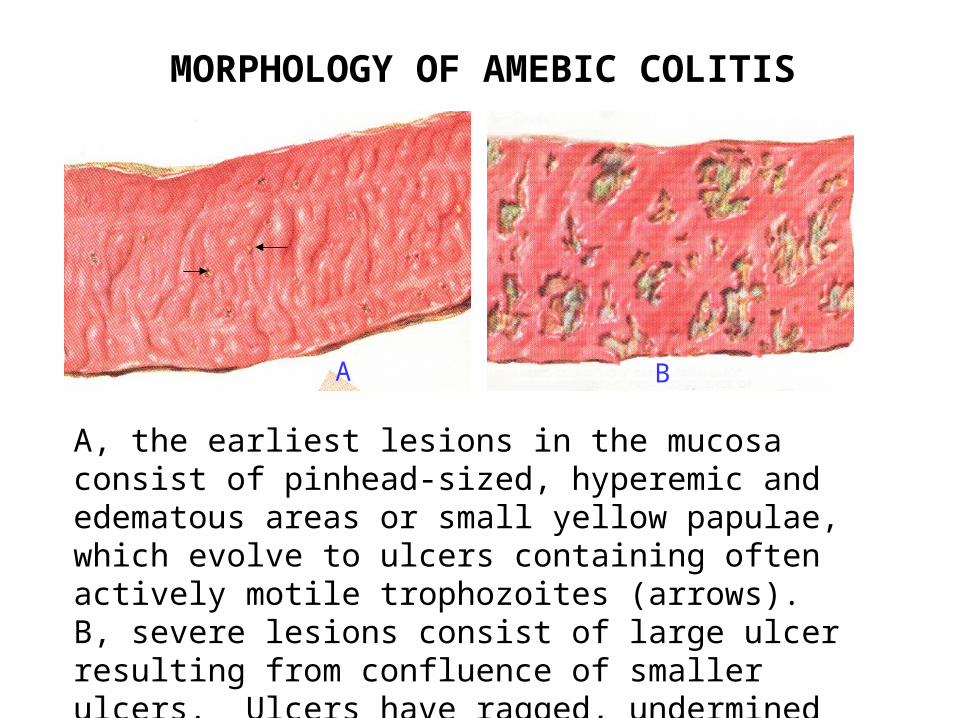
A, the earliest lesions in the mucosa consist of pinhead-sized, hyperemic and edematous areas or small yellow papulae, which evolve to ulcers containing often actively motile trophozoites (arrows). B, severe lesions consist of large ulcer resulting from confluence of smaller ulcers. Ulcers have ragged, undermined edges; intervening mucosa congested.
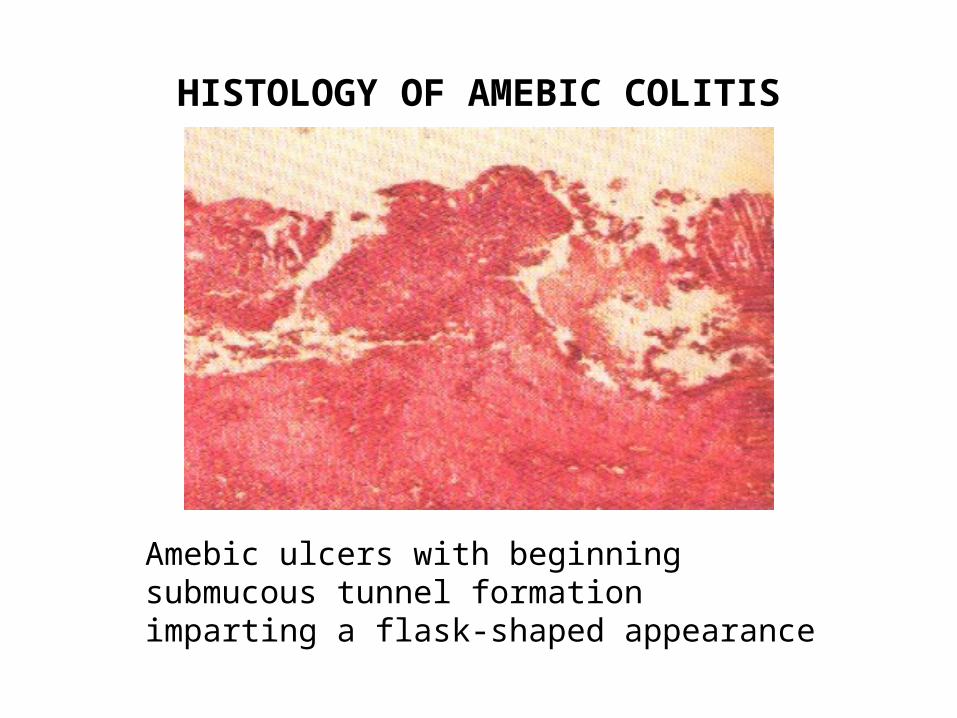
HISTOLOGY OF AMEBIC COLITIS
Amebic ulcers with beginning submucous tunnel formation imparting a flask-shaped appearance
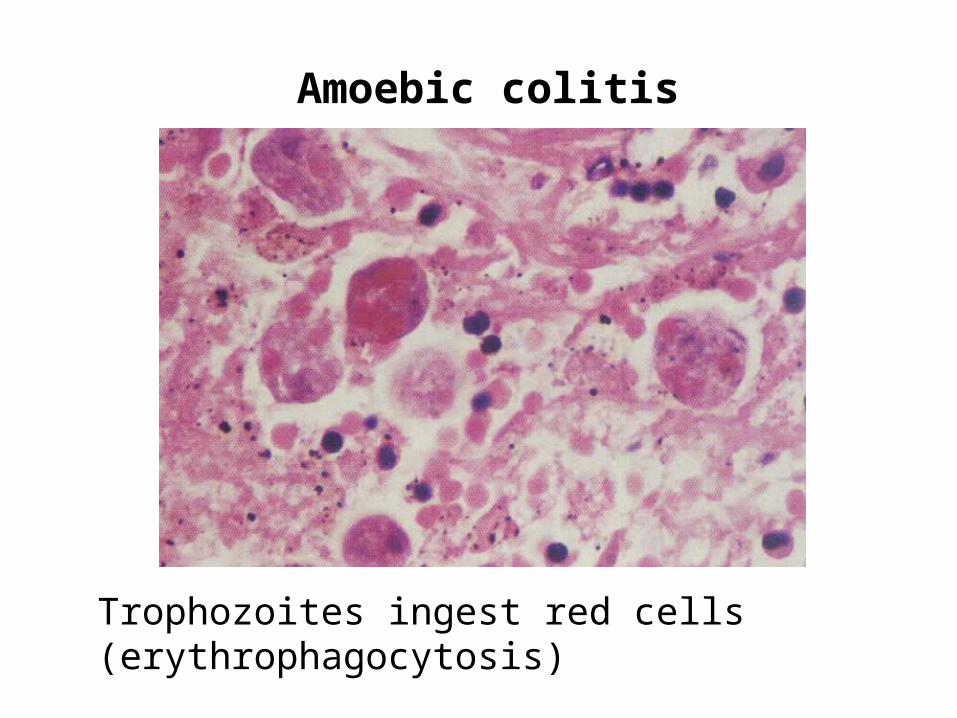
Amoebic colitis
Trophozoites ingest red cells (erythrophagocytosis)
TYPHOID ENTERITIS
1. Usually confined to the ileum as a consequence of typhoid fever.
2. Bowel involvement involvement is only part of a widespread symptomatic bacteremia.
3. Salmonella typhi and paratyphi are the causative organisms.
4. Organisms are ingested in contaminated water or in food.
5. Characteristic lesions are seen in the intestinal lymphatic tissue, especially in the terminal portion of the ileum.
6. The mucosa-associated lymphoid tissue, particularly the Peyer’s patches become enlarged and eventually ulcerated.
7. Inflammatory infiltrates mostly mononuclear cells with erythrophagocytosis
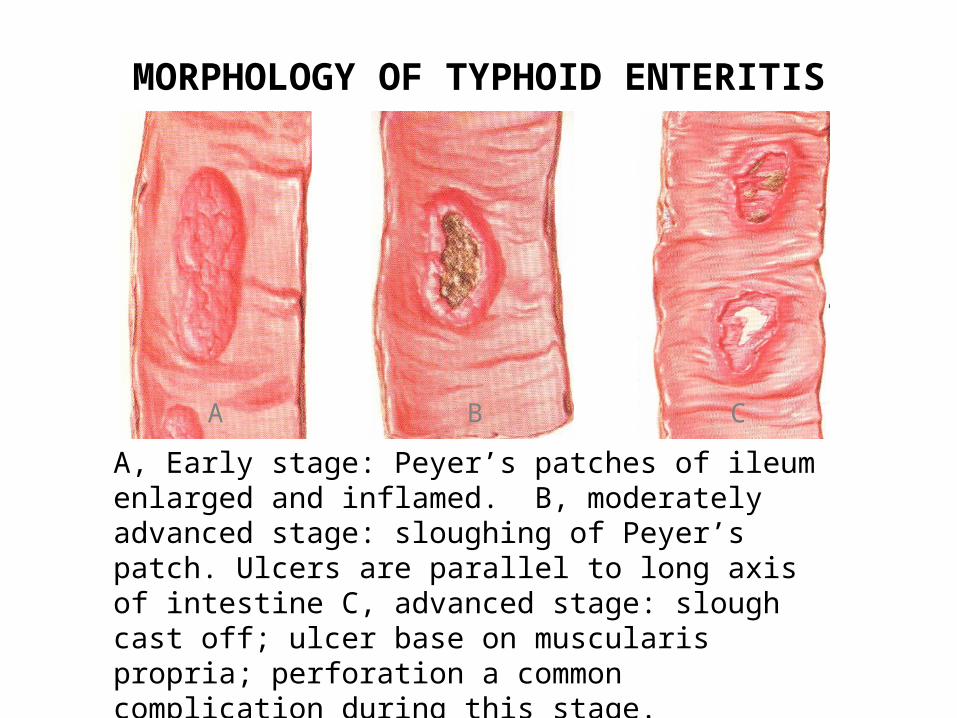
MORPHOLOGY OF TYPHOID ENTERITIS
A B C
A, Early stage: Peyer’s patches of ileum enlarged and inflamed. B, moderately advanced stage: sloughing of Peyer’s patch. Ulcers are parallel to long axis of intestine C, advanced stage: slough cast off; ulcer base on muscularis propria; perforation a common complication during this stage.
TUBERCULOSIS OF THE INTESTINES
1. Most cases in the Philippines are caused by swallowed infected sputum from a pulmonary cavitary lesion.
2. Usually affects the terminal ileum and cecum causing ulceration of the mucosa
3. Accompanied by fibrous wall thickening and enlargement of regional lymph nodes.
4. Major complications are intestinal obstruction by strictures and adhesions, perforation of ulcers (uncommon), and malabsorption if involvement is widespread.
Tuberculosis of Intestines
5. May be divided into two distinct forms:
- ulcerative
- hypertrophic
6. Ulcerative form is most common
7. Initial lesions usually affect the Peyer’s
patches and solitary lymphoid nodules
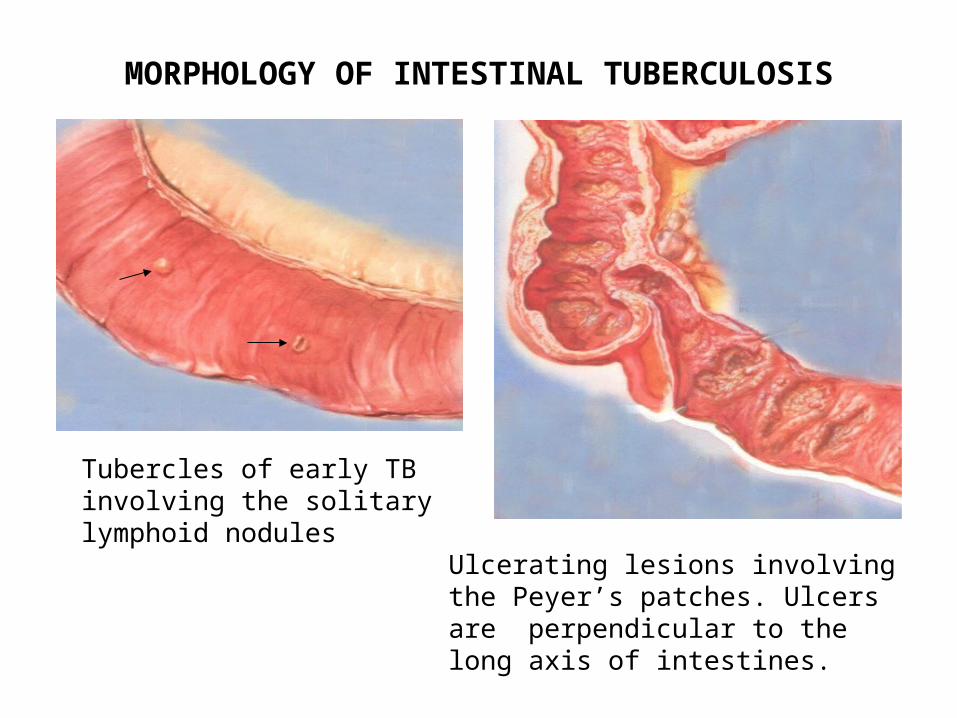
MORPHOLOGY OF INTESTINAL TUBERCULOSIS
Tubercles of early TB involving the solitary lymphoid nodules
Ulcerating lesions involving the Peyer’s patches. Ulcers are perpendicular to the long axis of intestines.
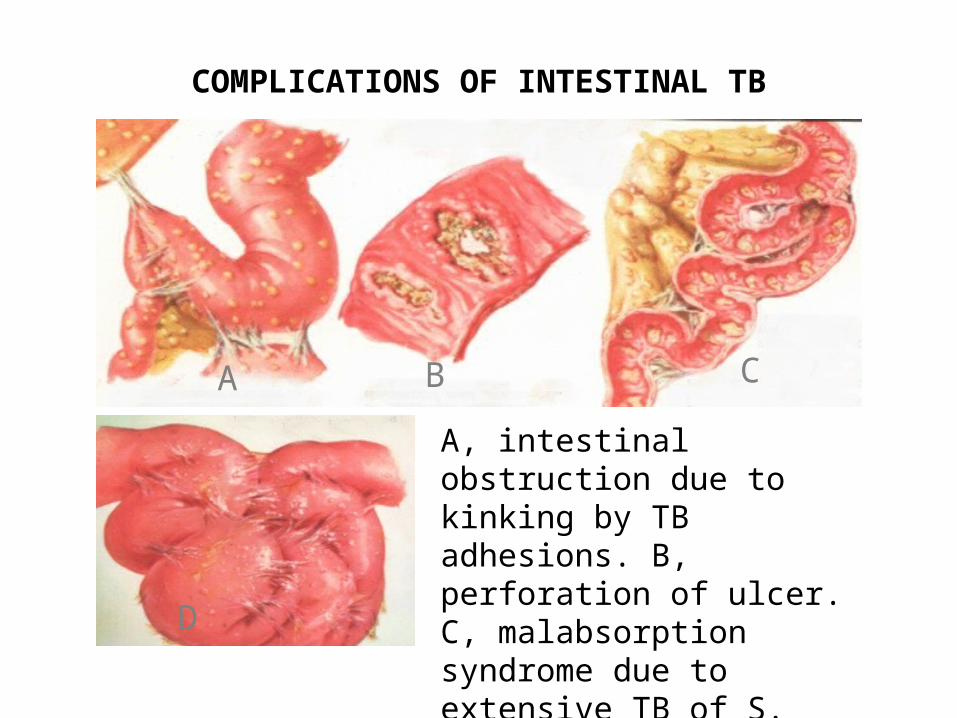
COMPLICATIONS OF INTESTINAL TB
A B C
D
A, intestinal obstruction due to kinking by TB adhesions. B, perforation of ulcer. C, malabsorption syndrome due to extensive TB of S. intestine and mesenteric lymph nodes.
ACUTE APPENDICITIS
1. Common cause of ‘acute abdomen’
2. Inflammation often precipitated by obstruction due to fecalith, lymphoid hyperplasia or tumor.
3. Superimposed ischemia due to tissue pressure on blood vessels and thrombosis may cause gangrene.
4. Common complication is perforation with subsequent peritonitis
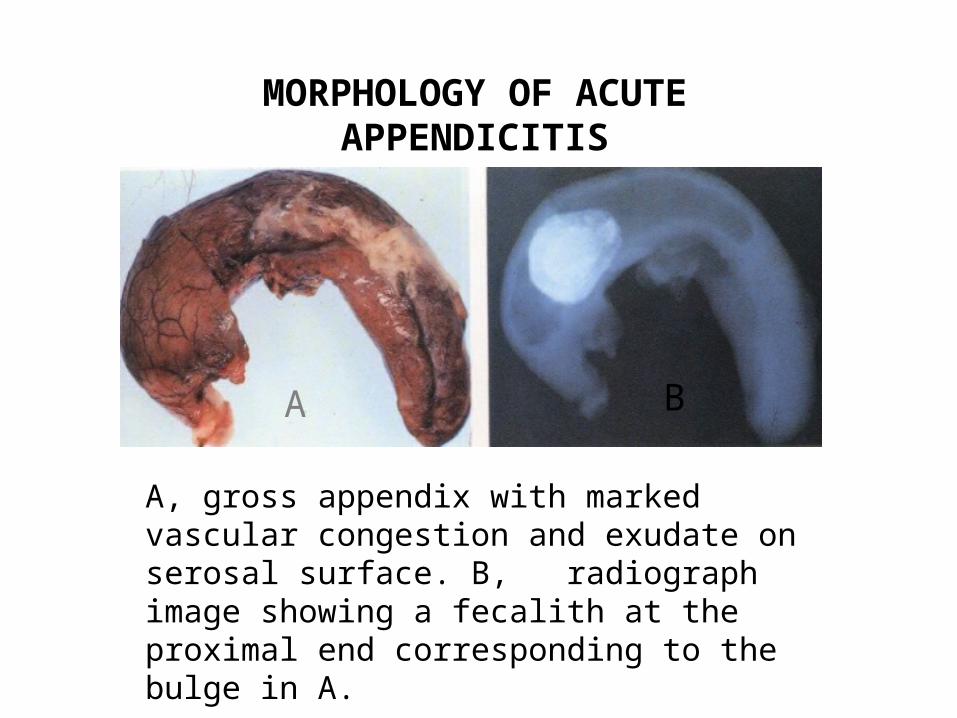
MORPHOLOGY OF ACUTE APPENDICITIS
A, gross appendix with marked vascular congestion and exudate on serosal surface. B, radiograph image showing a fecalith at the proximal end corresponding to the bulge in A.
A B
HIRSCHPRUNG’S DISEASE Aganglionosis of Intestine
1. Results from a failure of migration of neuroblasts from the vagus into the developing gut, such that the intramural parasympathetic nerve plexuses fail to develop, thus affecting peristaltic movement of the affected segment.
2. Rectum and distal colon are usually involved.
3. Effects may be from life-threatening total obstruction to mild cases causing chronic constipation.
4. Also called Congenital Megacolon.
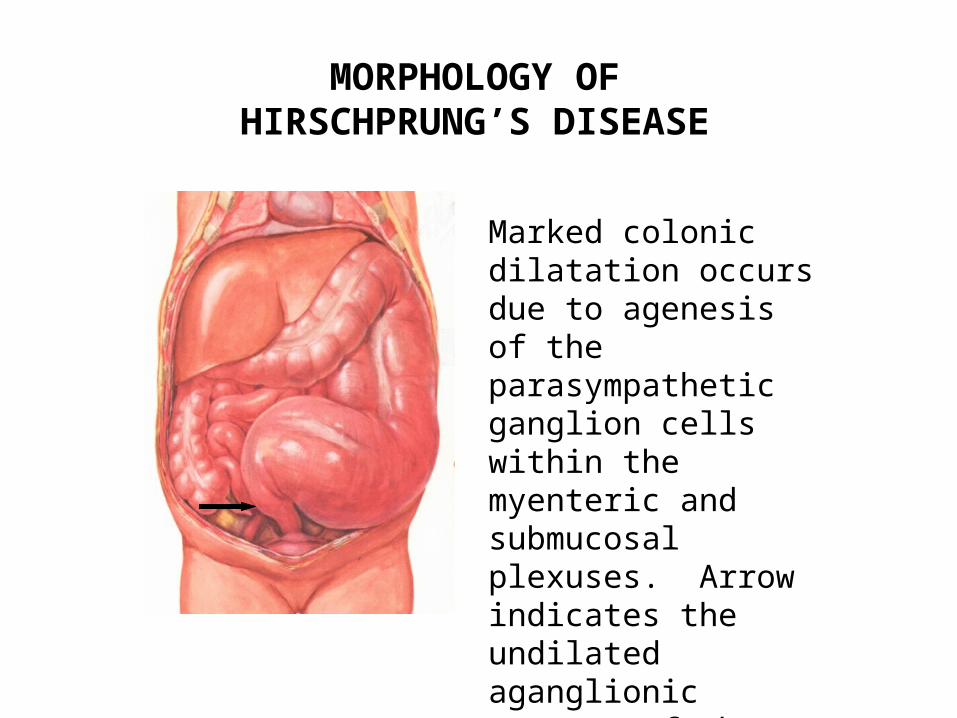
MORPHOLOGY OF HIRSCHPRUNG’S DISEASE
Marked colonic dilatation occurs due to agenesis of the parasympathetic ganglion cells within the myenteric and submucosal plexuses. Arrow indicates the undilated aganglionic segment of the rectum.
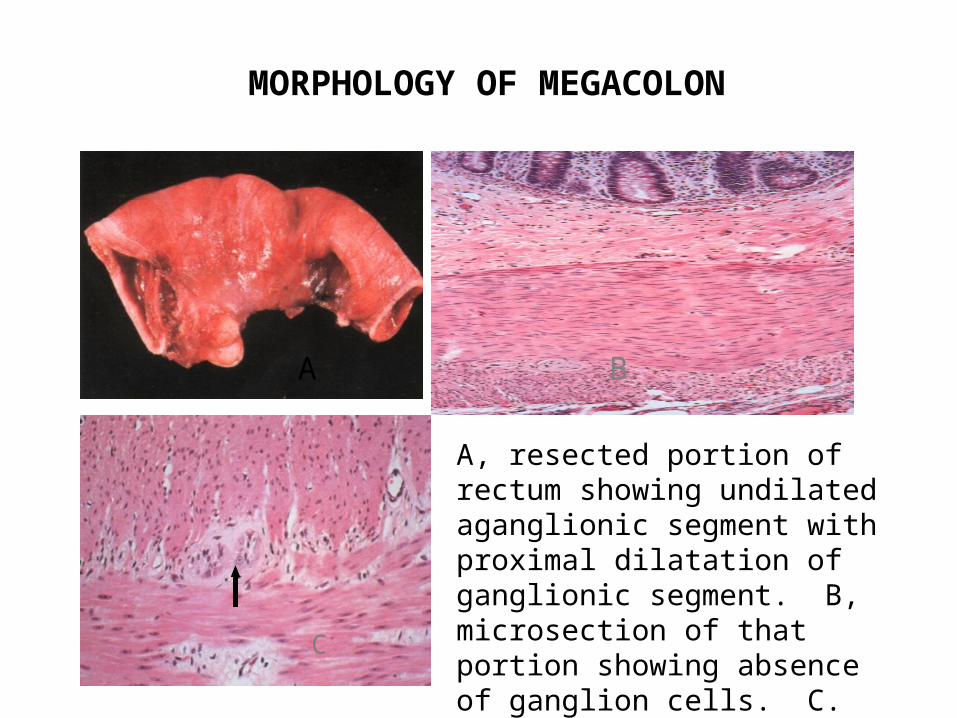
MORPHOLOGY OF MEGACOLON
A, resected portion of rectum showing undilated aganglionic segment with proximal dilatation of ganglionic segment. B, microsection of that portion showing absence of ganglion cells. C. normal colon showing ganglion cells (arrow)
A B
C
INTESTINAL OBSTRUCTION
Common causes are:
1. Intussusception, which is the invagination of a bowel segment into the next distal segment.
2. Volvulus, which is the twisting of the bowel occluding its lumen.
3. Hernias are intestinal protrusions through weakened or defective portions of the peritoneal cavity; commonly in inguinal and femoral canals.
4. Adhesions
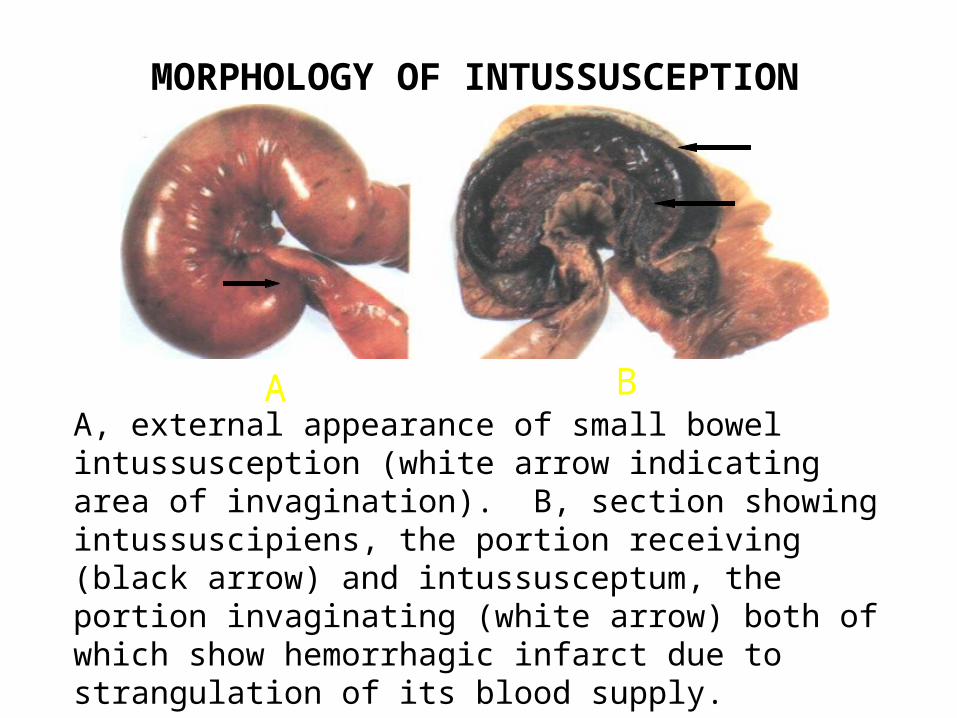
MORPHOLOGY OF INTUSSUSCEPTION
A BA, external appearance of small bowel intussusception (white arrow indicating area of invagination). B, section showing intussuscipiens, the portion receiving (black arrow) and intussusceptum, the portion invaginating (white arrow) both of which show hemorrhagic infarct due to strangulation of its blood supply.
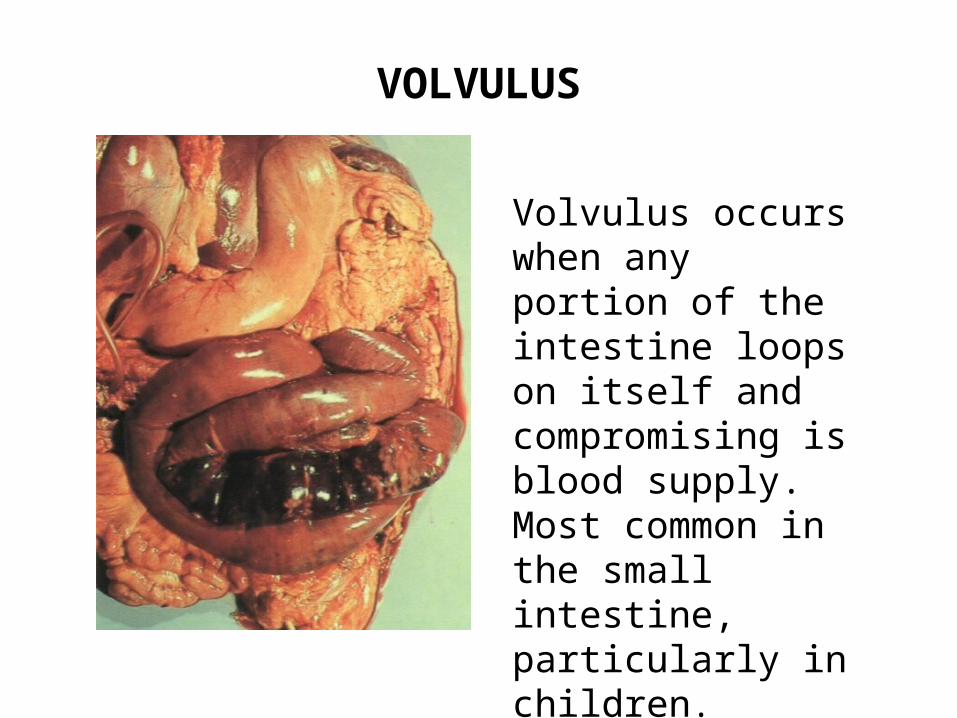
VOLVULUS
Volvulus occurs when any portion of the intestine loops on itself and compromising is blood supply. Most common in the small intestine, particularly in children.
IDIOPATHIC INFLAMATORY BOWEL DISEASE
1. Two conditions: Crohn’s disease and ulcerative colitis
2. Crohn’s disease most commonly affects the small bowel, but any portion of the gut may be involved.
3. Ulcerative colitis usually confined to the colon and anus.
4. Cause in not clear; many theories have been proposed.
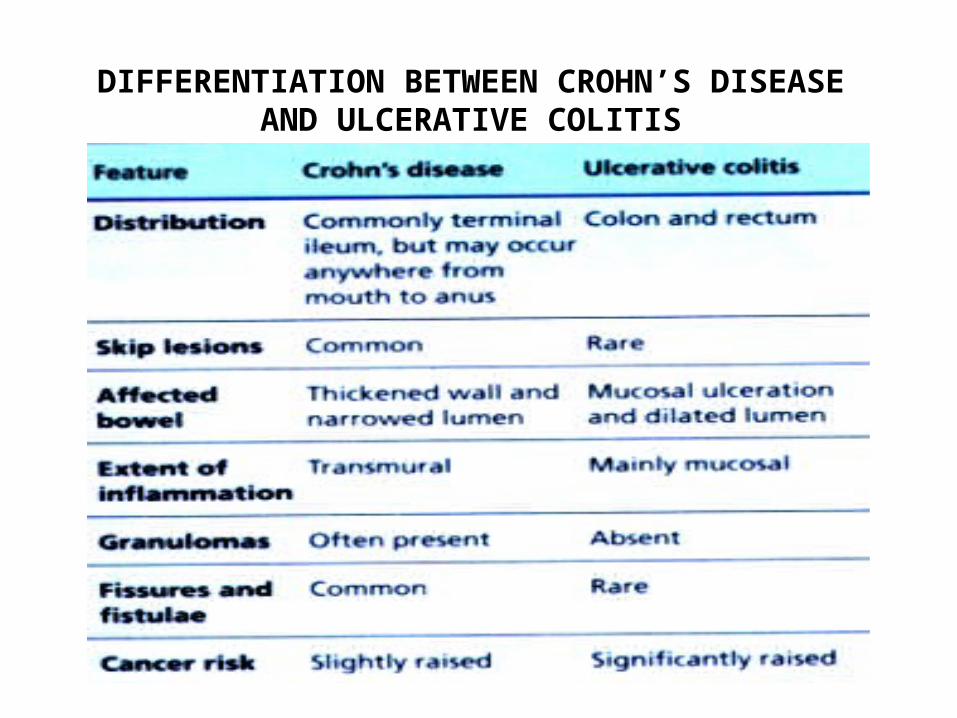
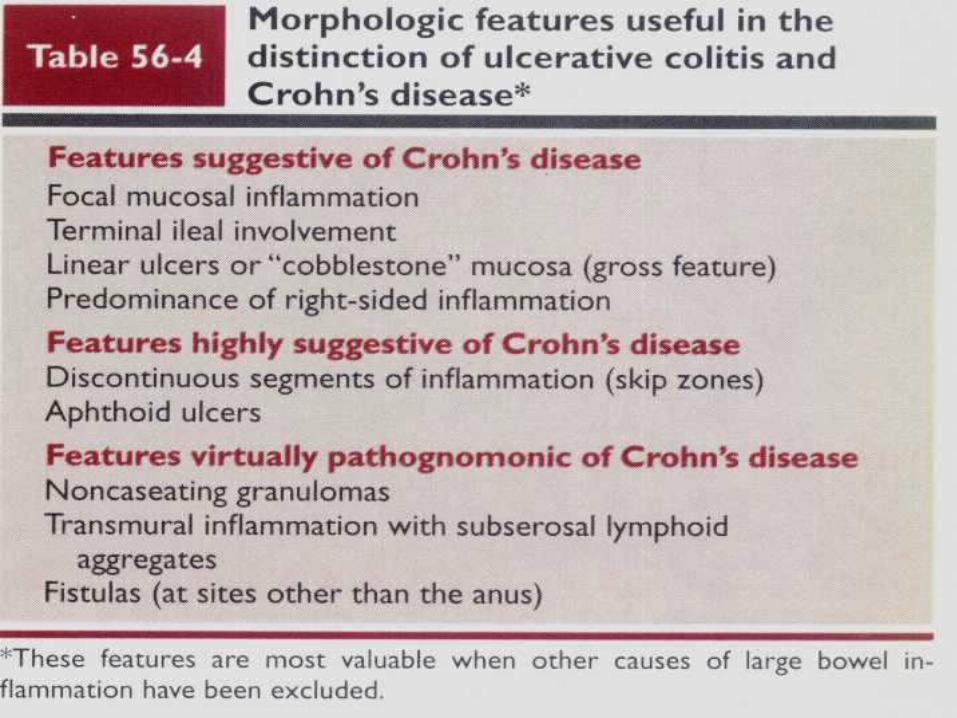
DIFFERENTIATION BETWEEN CROHN’S DISEASE AND ULCERATIVE COLITIS
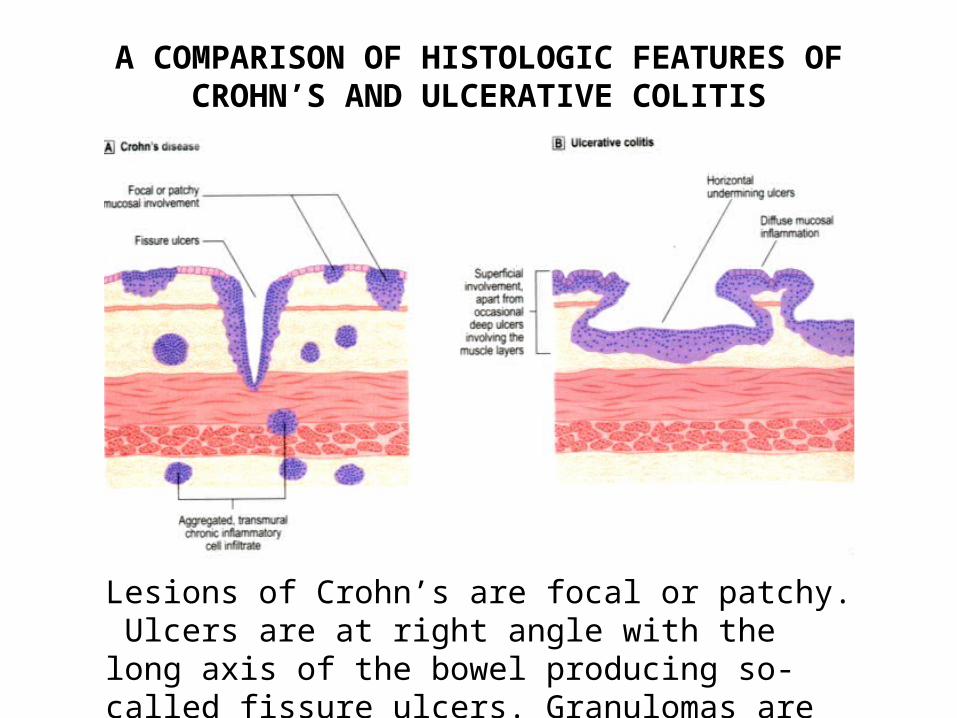
A COMPARISON OF HISTOLOGIC FEATURES OF CROHN’S AND ULCERATIVE COLITIS
Lesions of Crohn’s are focal or patchy. Ulcers are at right angle with the long axis of the bowel producing so-called fissure ulcers. Granulomas are more common in Crohn’s.
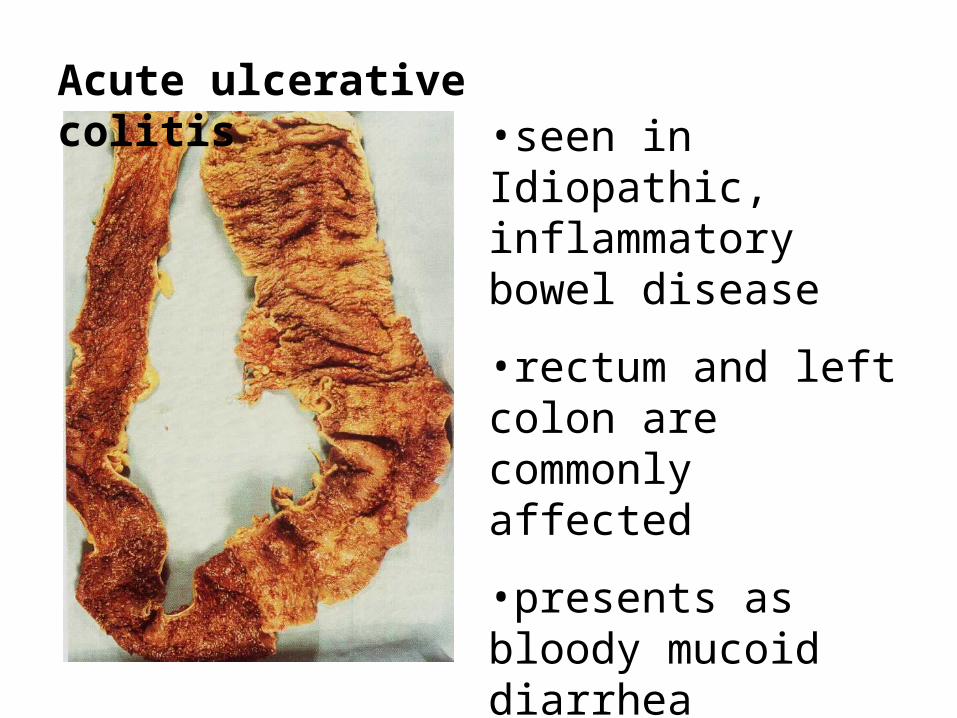
Acute ulcerative colitis•seen in Idiopathic, inflammatory bowel disease
•rectum and left colon are commonly affected
•presents as bloody mucoid diarrhea
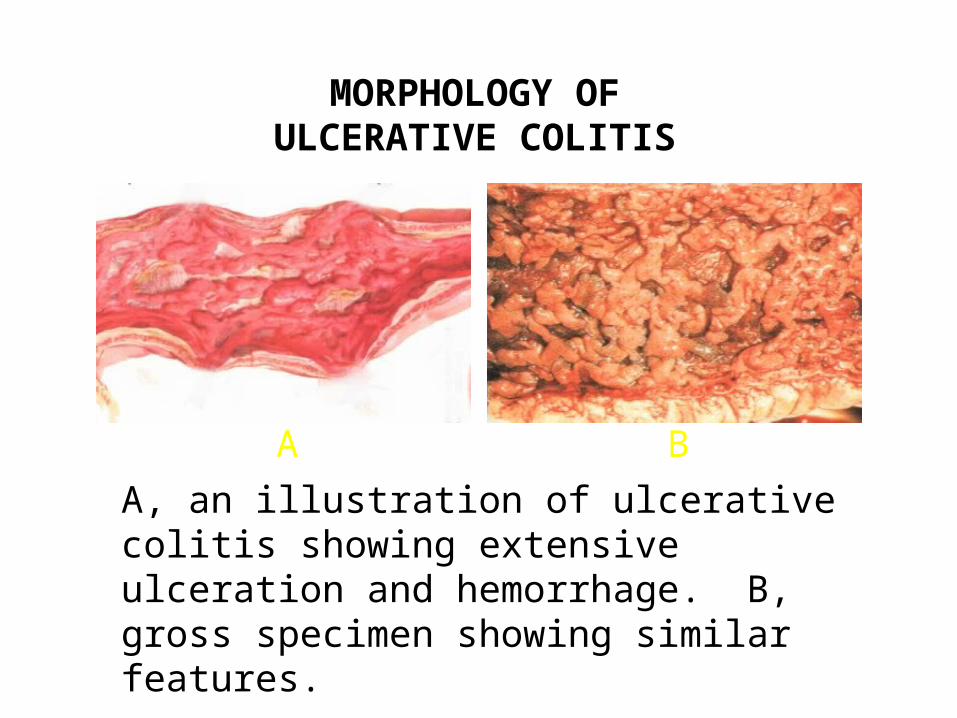
MORPHOLOGY OF ULCERATIVE COLITIS
A B
A, an illustration of ulcerative colitis showing extensive ulceration and hemorrhage. B, gross specimen showing similar features.
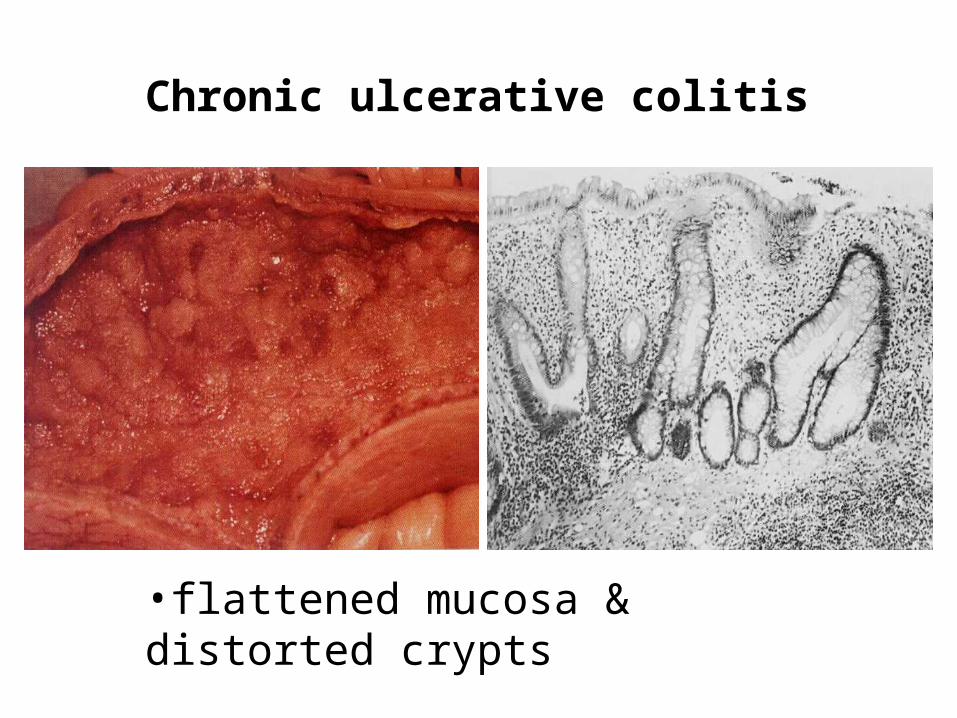
Chronic ulcerative colitis
•flattened mucosa & distorted crypts
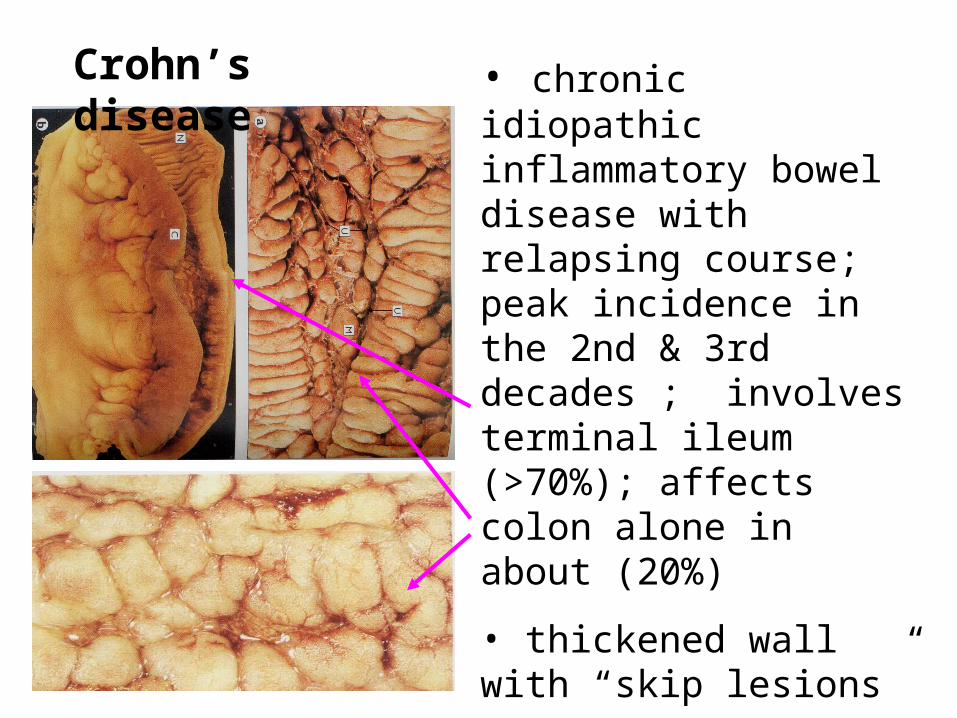
Crohn’s disease • chronic idiopathic inflammatory bowel disease with relapsing course; peak incidence in the 2nd & 3rd decades ; involves terminal ileum (>70%); affects colon alone in about (20%)
• thickened wall with “skip lesions”
•linear ulcers & cobblestone mucosa
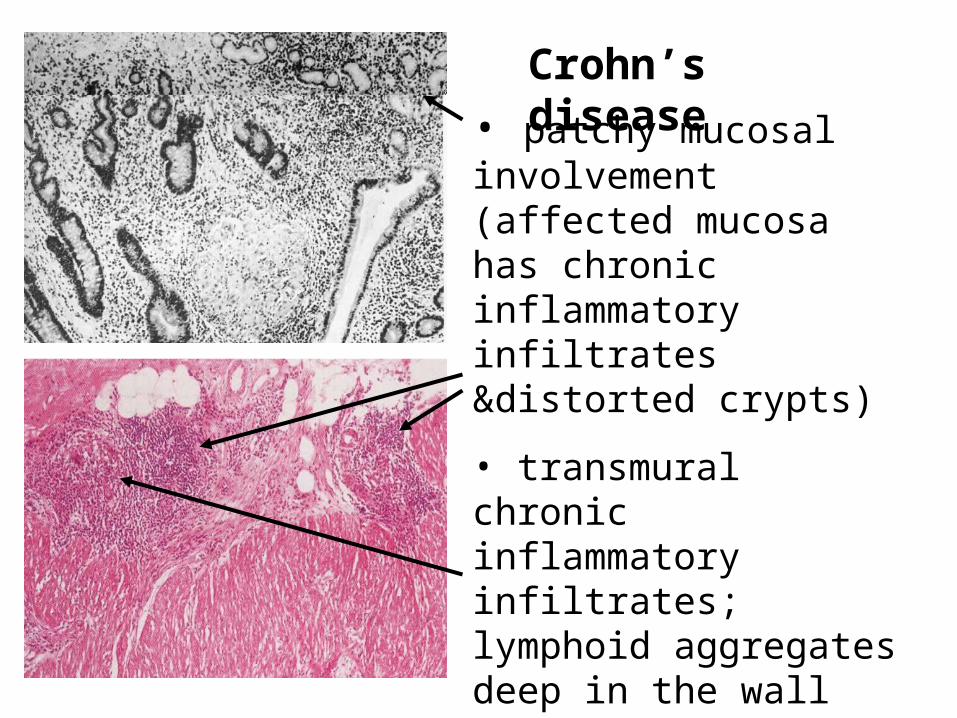
Crohn’s disease
• patchy mucosal involvement (affected mucosa has chronic inflammatory infiltrates &distorted crypts)
• transmural chronic inflammatory infiltrates; lymphoid aggregates deep in the wall
• formation of non-caseating granuloma
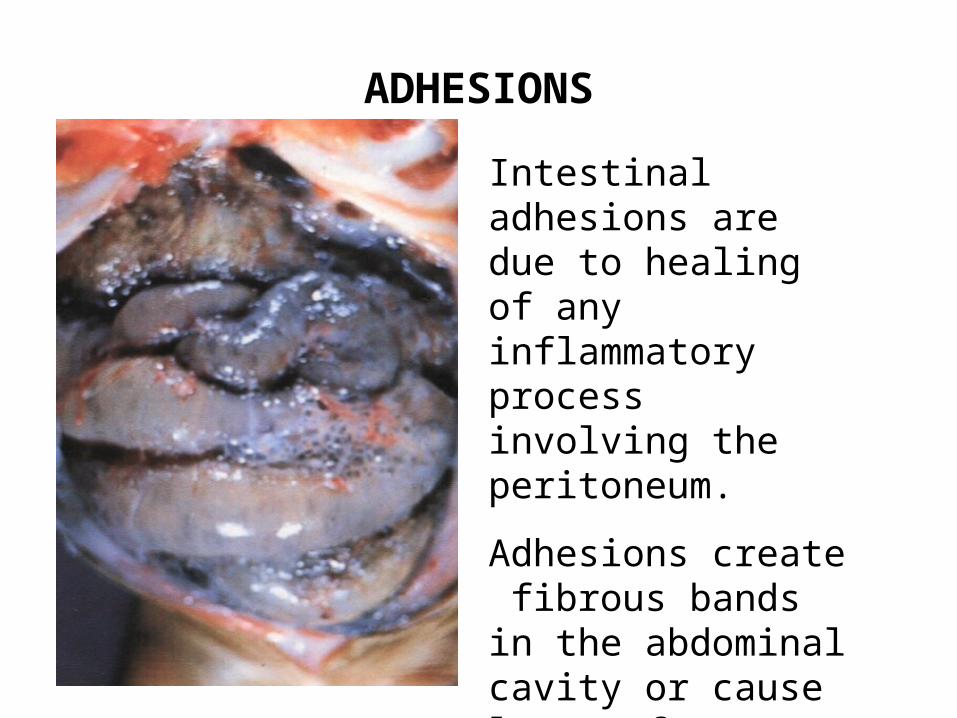
ADHESIONS
Intestinal adhesions are due to healing of any inflammatory process involving the peritoneum.
Adhesions create fibrous bands in the abdominal cavity or cause loops of intestine to adhere to one another.
DIVERTICULAR DISEASE
1. Diverticula are herniations of mucosa into the intestinal wall.
2. Herniations are of the pulsion type usually at sites of weakness particularly where lymphoid aggregates breach the muscularis mucosae.
3. Most common in the colon, particularly the sigmoid.
4. Most diverticula occur between the mesenteric and anti-mesenteric longitudinal muscle band (taenia coli)
DIVERTICULAR DISEASE
5. Affected segment shows thickening of the muscularis propria, and prominence of the mucosal folds which occludes the lumen.
6. Due to a deficiency of fiber in the diet.
7. Sigmoid motility is sensitive to the bulk of the colonic content, and if low, due to a low fiber diet, abnormally high intra-luminal pressure are generated.
8. Complications are diverticulitis, perforation, peridiverticular abscess, fistula, peritonitis and hemorrhage.
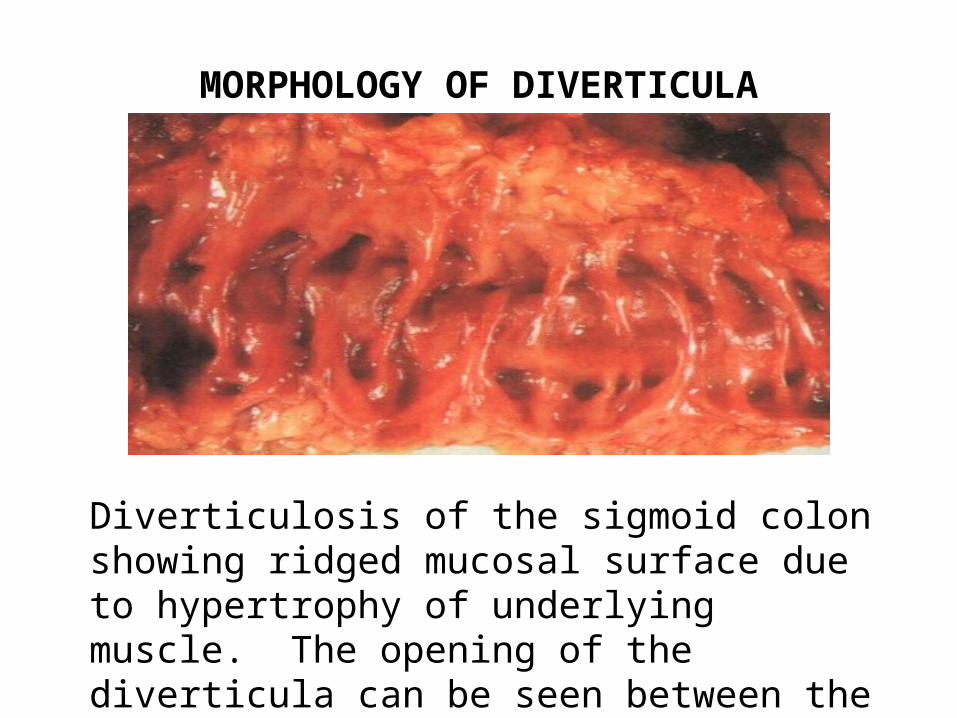
MORPHOLOGY OF DIVERTICULA
Diverticulosis of the sigmoid colon showing ridged mucosal surface due to hypertrophy of underlying muscle. The opening of the diverticula can be seen between the mucosal ridges.
POLYPS1. A polyp is simply a protuberant growth.
2. Wide variety of histologic types
3. Divided into epithelial (much more common) and mesenchymal
4. 4 types of benign epithelial polyp:
- inflammatory (pseudopolyps)
- metaplastic
- hamartomatous
- adenomas (most important because of adenoma-carcinoma sequence)
ADENOMAS
1. Can originate in any portion of the intestine, however, mainly in large intestine.
2. Benign glandular neoplasms originating from intestinal mucosal epithelium composed of dysplastic epithelium.
3. Probably the precursors of most colorectal carcinomas.
4. Adenomas and carcinomas are frequently found together in a resected segment of bowel.
5. Malignant risk is associated with increasing size, villous growth pattern, more severe degree of dysplasia.
MOLECULAR PATHOLOGY OF ADENOMA-CARCINOMA SEQUENCE
Genetic defects are:
1. Activation of oncogenes
2. Loss or mutations of tumor suppressor gene
3. Defective genes of the DNA repair pathway leading to genomic instability.
ACTIVATION OF ONCOGENES
1. Overexpression of c-MYC is a feature of most colorectal carcinoma
2. c-MYC encodes a nuclear phosphoprotein which is required for DNA synthesis.
3. Increased expression of c-MYC may be followed by increased cellular proliferation.
LOSS OF SUPPRESSOR GENE
• Point mutation or deletion of chromosome 5q of suppressor gene renders the cell more resistant.
• Damage which would normally results in apoptosis and elimination of the cell does not occur.
MORPHOLOGY OF ADENOMAS
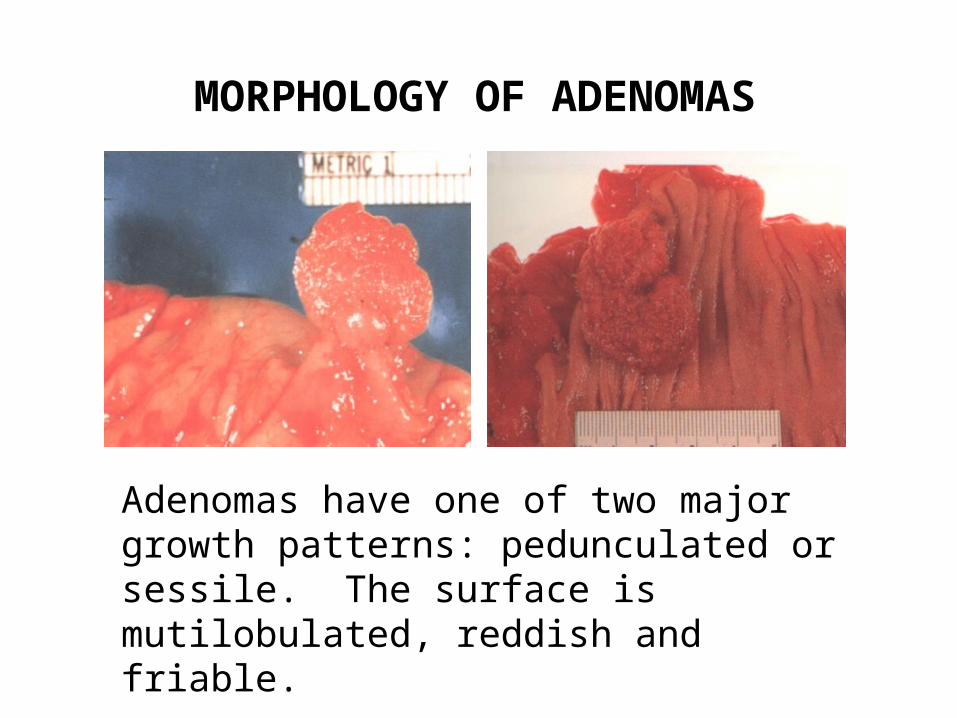
Adenomas have one of two major growth patterns: pedunculated or sessile. The surface is mutilobulated, reddish and friable.
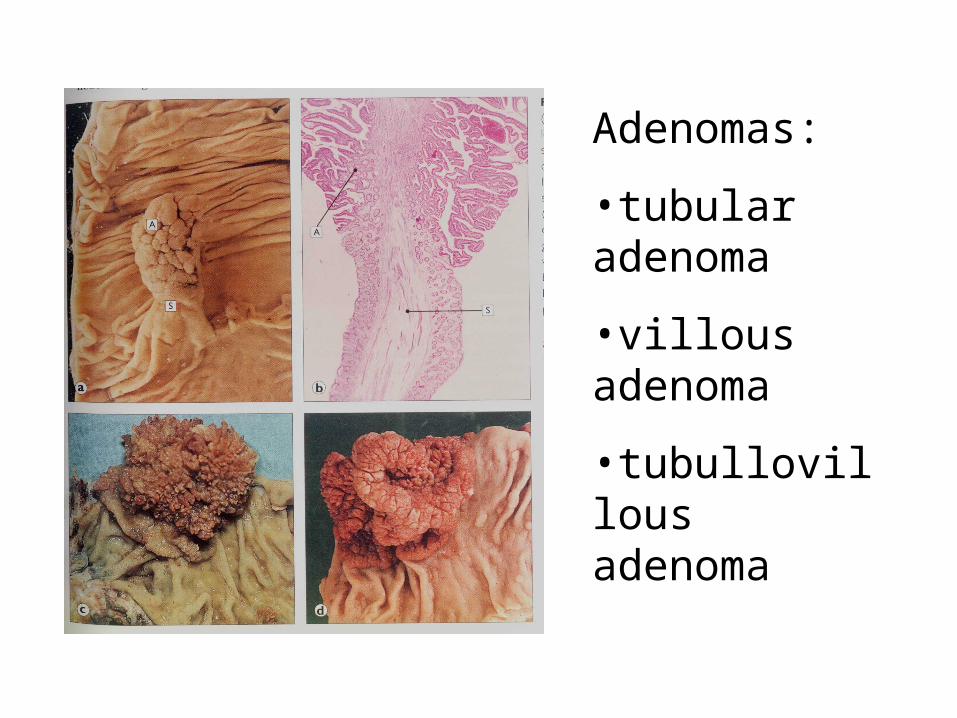
Adenomas:
•tubular adenoma
•villous adenoma
•tubullovillous adenoma
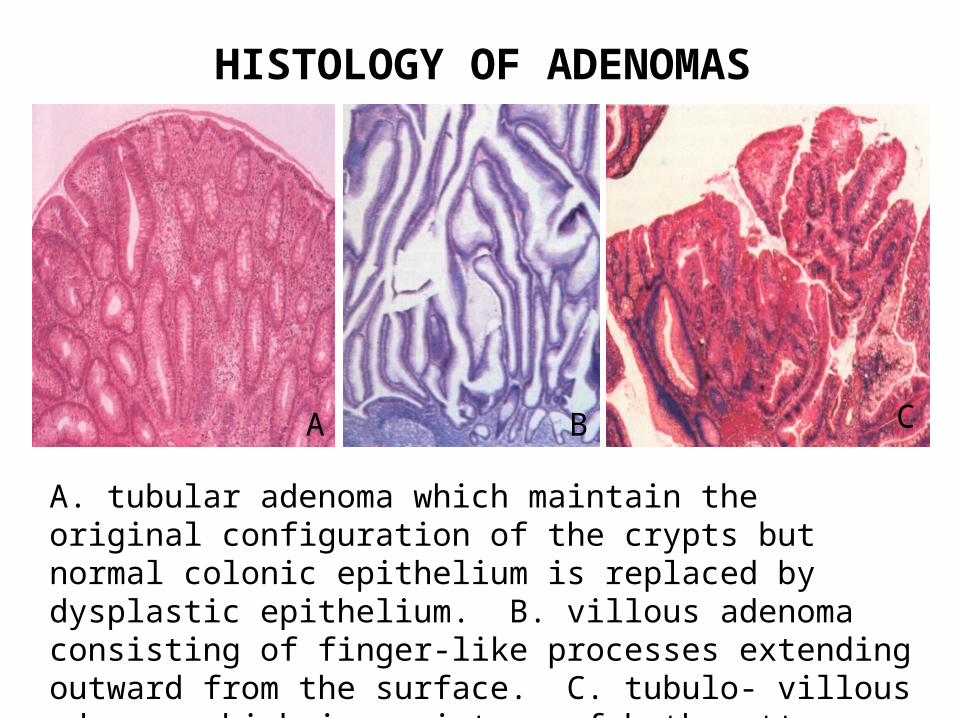
HISTOLOGY OF ADENOMAS
A B C
A. tubular adenoma which maintain the original configuration of the crypts but normal colonic epithelium is replaced by dysplastic epithelium. B. villous adenoma consisting of finger-like processes extending outward from the surface. C. tubulo- villous adenoma which is a mixture of both patterns.
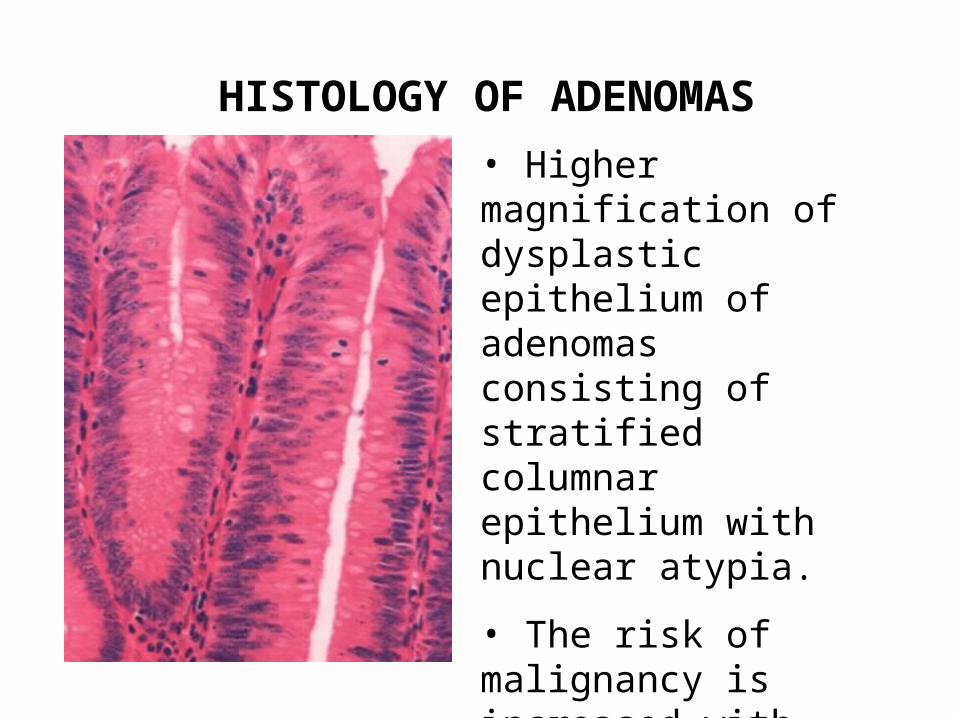
HISTOLOGY OF ADENOMAS
• Higher magnification of dysplastic epithelium of adenomas consisting of stratified columnar epithelium with nuclear atypia.
• The risk of malignancy is increased with increasing size, villous pattern and degree of dysplasia.
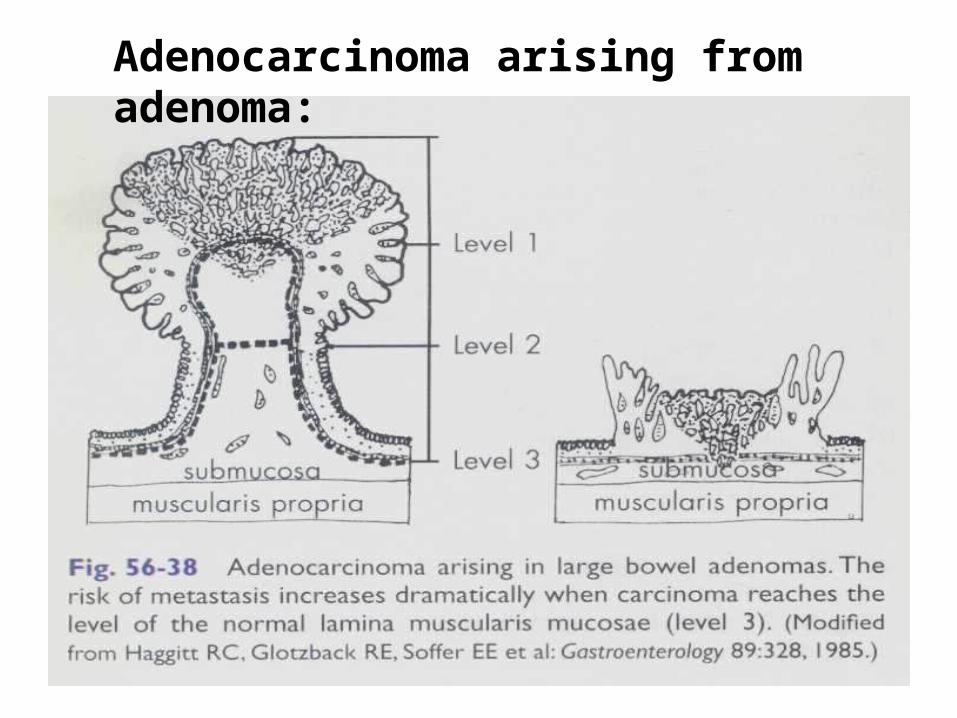
Adenocarcinoma arising from adenoma:
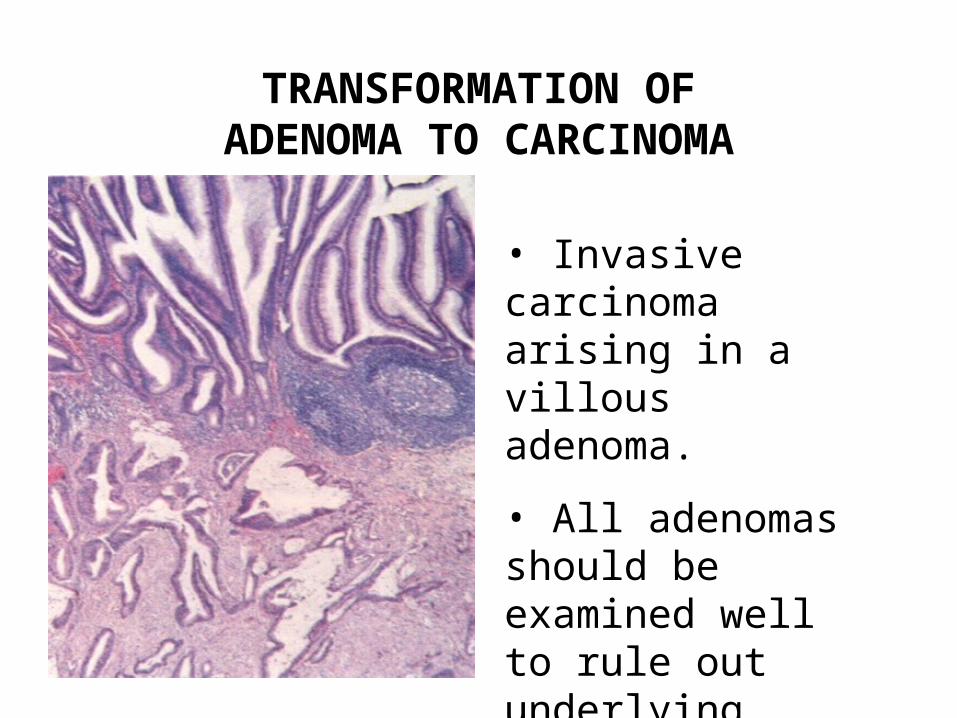
TRANSFORMATION OF ADENOMA TO CARCINOMA
• Invasive carcinoma arising in a villous adenoma.
• All adenomas should be examined well to rule out underlying carcinoma.
CARCINOMA OF THE COLON
1. Most common malignancy in developed country
2. All are adenocarcinomas
3. Increased risk in patients with adenomas and longstanding idiopathic ulcerative colitis
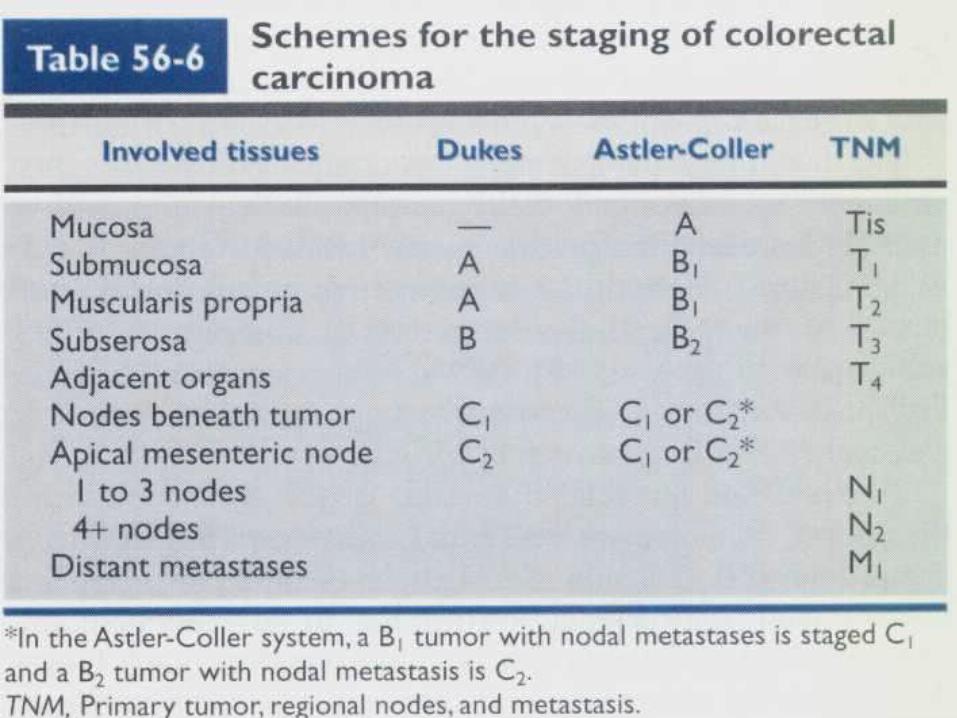
4. Dukes’ staging, based on local extent and metastatic status, is the best guide to prognosis
5. Inherited genetic factors and diet play a significant role in the pathogenesis
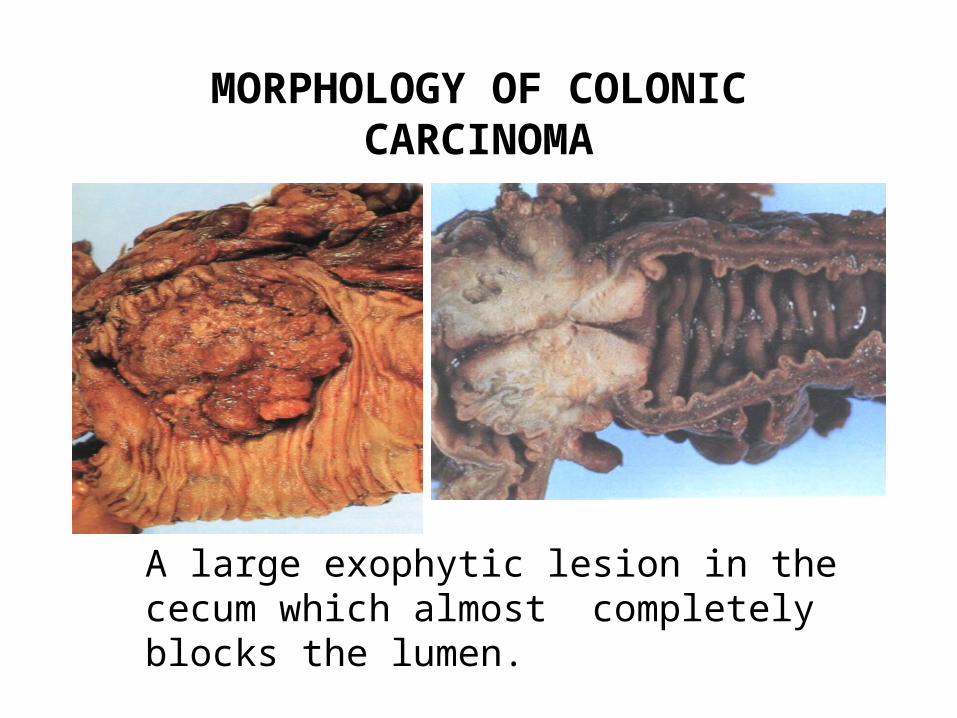
MORPHOLOGY OF COLONIC CARCINOMA
A large exophytic lesion in the cecum which almost completely blocks the lumen.
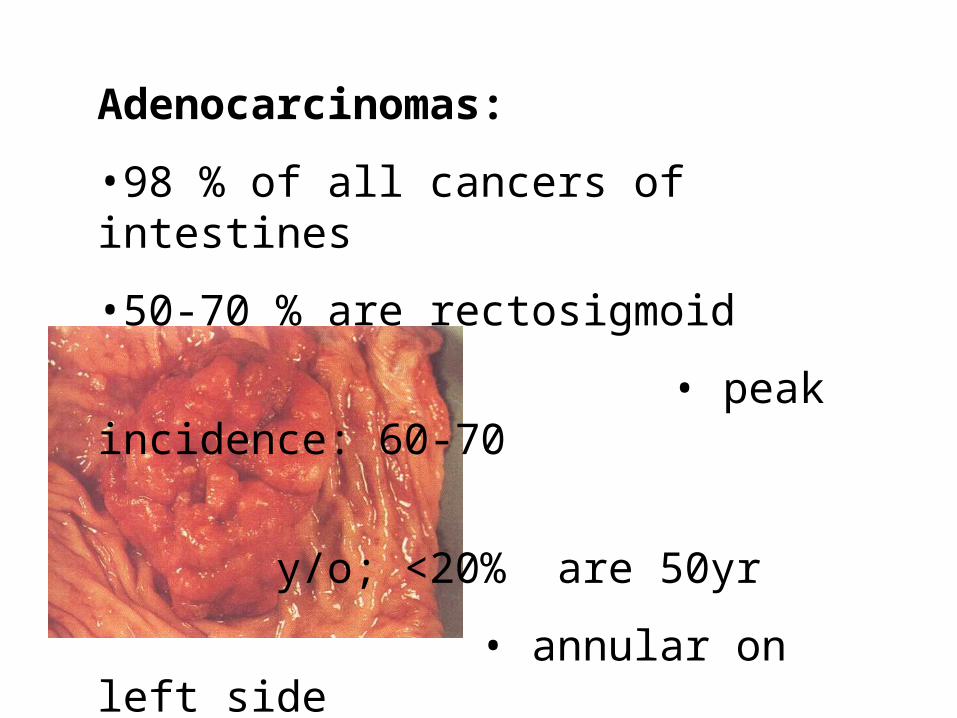
Adenocarcinomas:
•98 % of all cancers of intestines
•50-70 % are rectosigmoid
• peak incidence: 60-70
y/o; <20% are 50yr
• annular on left side
• polypoid/fungating on
the right side
Adenocarcinomas in the colon:
• associated RAS, p53 (17p,13), DCC (18q21) mutations
• (+) keratin & CEA (equally distributed)
Dietary factors:
• low fiber intake
• high carbohydrate intake
• high fat content
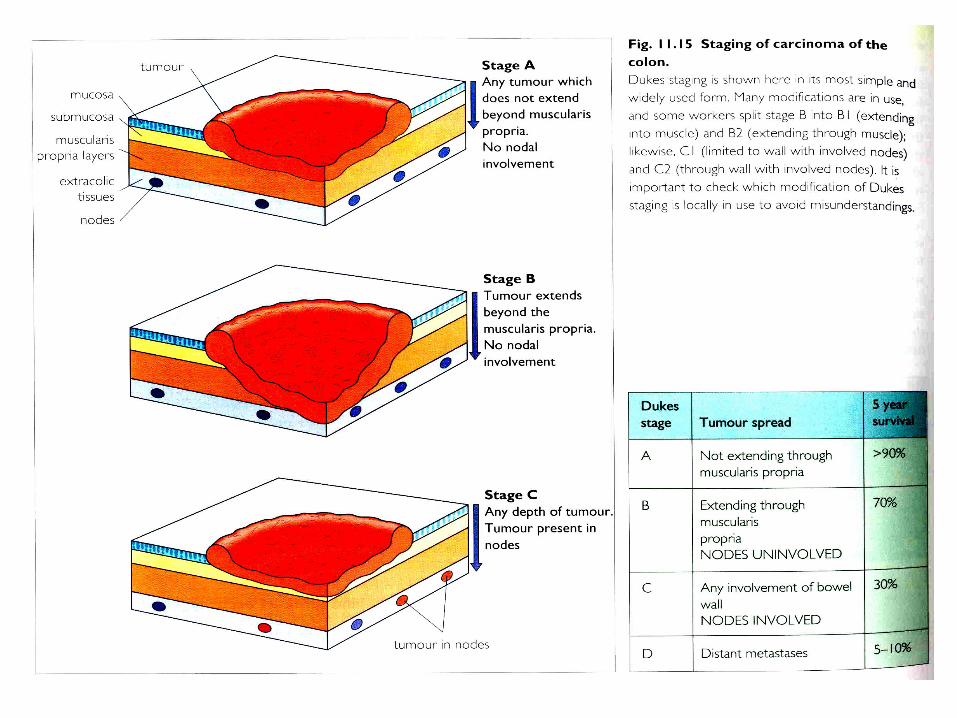
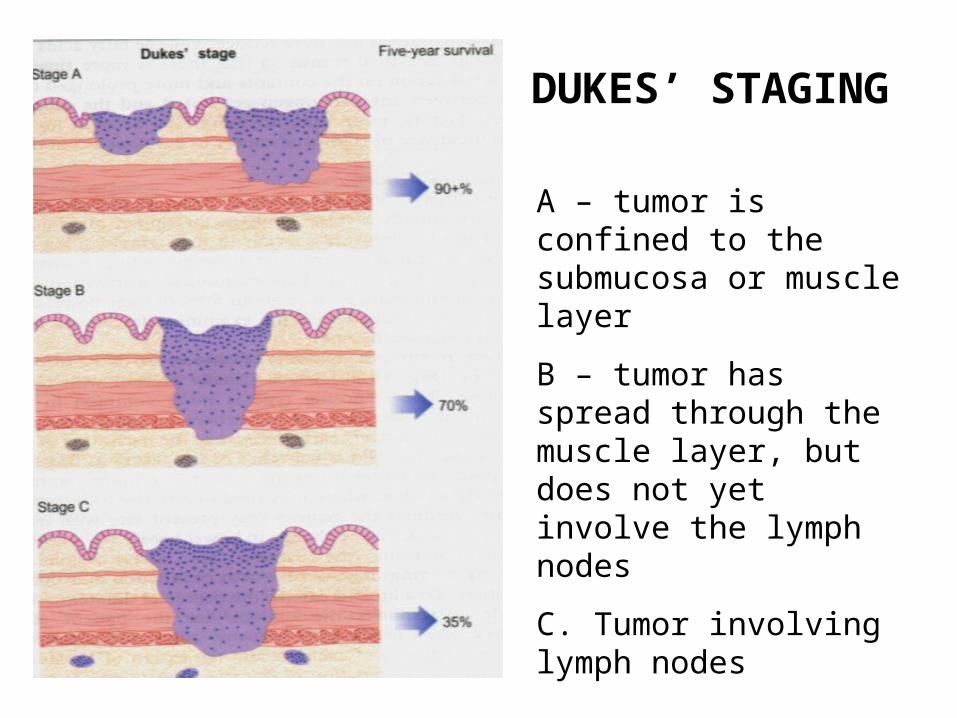
DUKES’ STAGING
A – tumor is confined to the submucosa or muscle layer
B – tumor has spread through the muscle layer, but does not yet involve the lymph nodes
C. Tumor involving lymph nodes
Mesenchymal tumors
• Lipoma - most common; submucosal
• Spindle cell stroma tumors:– arise from muscularis propria; appear as nodules
or polypoid masses– mostly leiomyomas or leiomyosarcomas– those with neural differentiation of lacking
differentiation are called Gastrointestinal stroma tumors (GIST)
– spindle cells in fascicles– size & mitotic rate are predictors of poor prognosis
Gastrointestinal lymphoma
• GIT is the most common site of extra-nodal lymphoma
• lymphoma accounts for 1-3% of GIT malignancies
• increased frequency with H.pylori associated gastritis, immunodeficiency, post-organ transplant immunosuppression, & celiac sprue and in the Mediterranean region
Pathologic Lesions of the Appendix
Mucocoele - dilation of appendix by mucinous secretions and may be caused by:
1. Mucosal hyperplasia - resembles hyperplastic polyp; uncommon
2. Mucinous cystadenoma - common; may rupture in about 1/5 of cases; benign such that appendectomy is curative
3. Mucinous cystadenocarcinoma - invasive tumor; penetrates wall of appendix; may rupture and implant on the peritoneum or ovary
Carcinoid tumors
• arise from GIT neuroendocrine cells• appendix is the most common site; also
commonly seen in the small intestine, rectum, stomach, colon
• gastric and ileal carcinoids are usually multicentric
• immunohistochemically (+) for chromogranin, symaptophysin and neuron-specific enolase
Carcinoid tumors• often asymptomatic but may produce
symptoms depending on the substances secreted:
– Cushing’s syndrome (ACTH)
– hyperinsulinism
– Zollinger-Ellison syndrome (gastrin)
– Carcinoid syndrome (serotonin) - episodic attacks of vasomotor instability, intestinal hypermotility & bronchoconstriction
Pseudomyxoma peritonei
• ascites composed of gelatinous material• may result from rupture of mucinous
custadenoma, cystadenocarcinoma of appendix or from tumors in other organs
• worse prognosis is expected if:– arises from adenocarcinoma– contains malignant epithelial tissue
admixed with the mucous (gelatinous) material
– widespread involvement
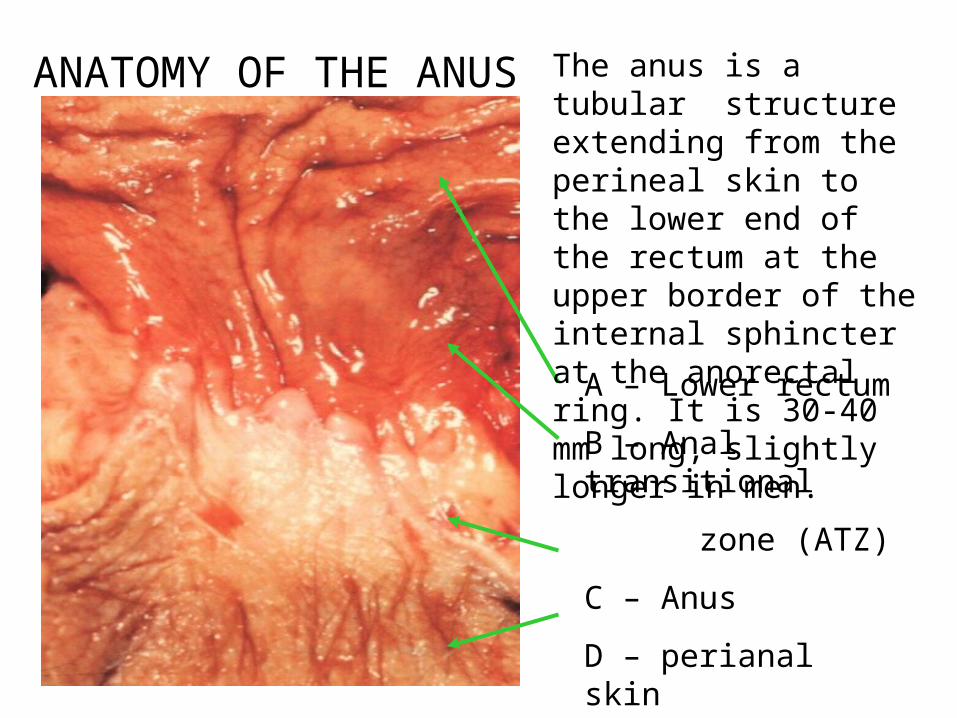
ANATOMY OF THE ANUS
A – Lower rectum
B – Anal transitional
zone (ATZ)
C – Anus
D – perianal skin
The anus is a tubular structure extending from the perineal skin to the lower end of the rectum at the upper border of the internal sphincter at the anorectal ring. It is 30-40 mm long, slightly longer in men.
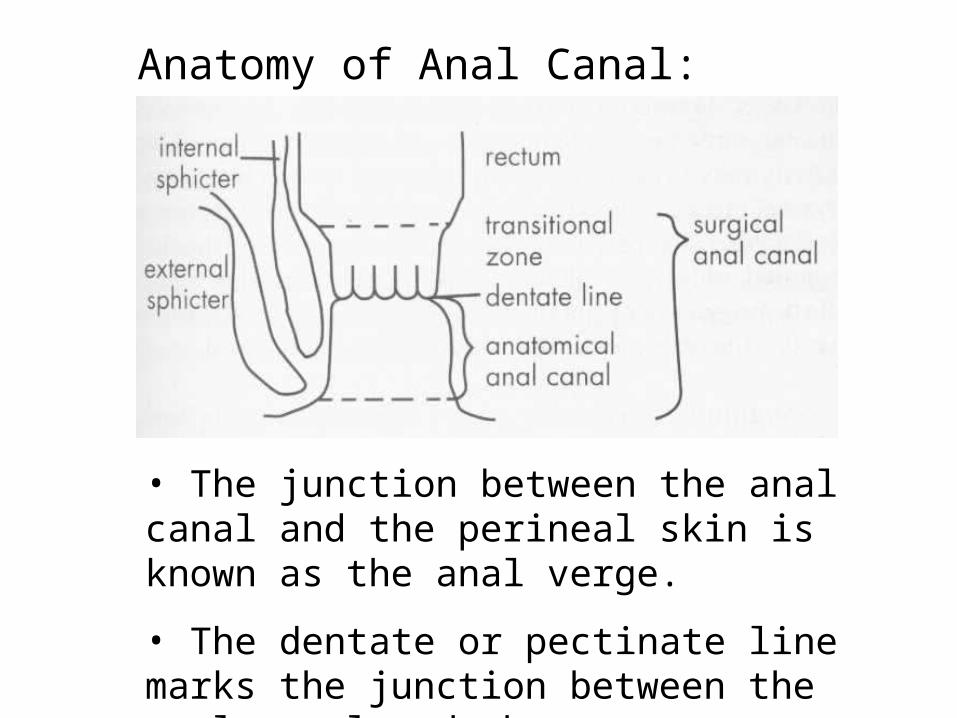
Anatomy of Anal Canal:
• The junction between the anal canal and the perineal skin is known as the anal verge.
• The dentate or pectinate line marks the junction between the anal canal and the rectum.
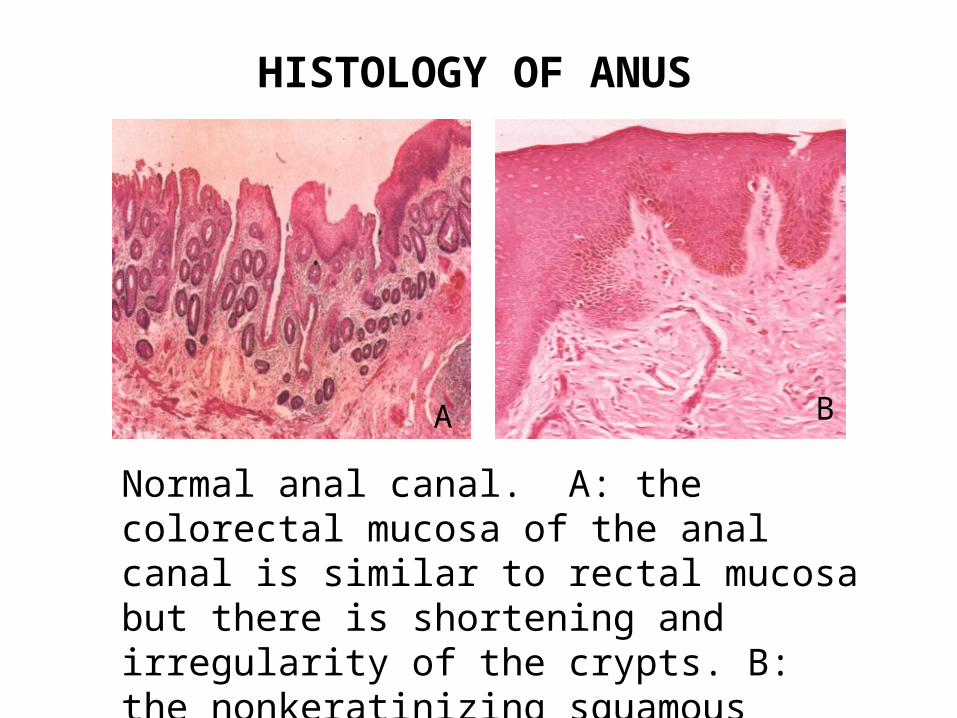
HISTOLOGY OF ANUS
A B
Normal anal canal. A: the colorectal mucosa of the anal canal is similar to rectal mucosa but there is shortening and irregularity of the crypts. B: the nonkeratinizing squamous layer below the transition zone contains increased melanocytes.
HEMORRHOIDS
1. Varicosities resulting from dilatation of the submucosal venous plexuses.
2. Underlying mechanism is not clear, although chronic constipation with straining at stool is most commonly invoked.
3. May present with bleeding; may prolapse through the anal verge; may undergo inflammation, thrombosis and infarction.
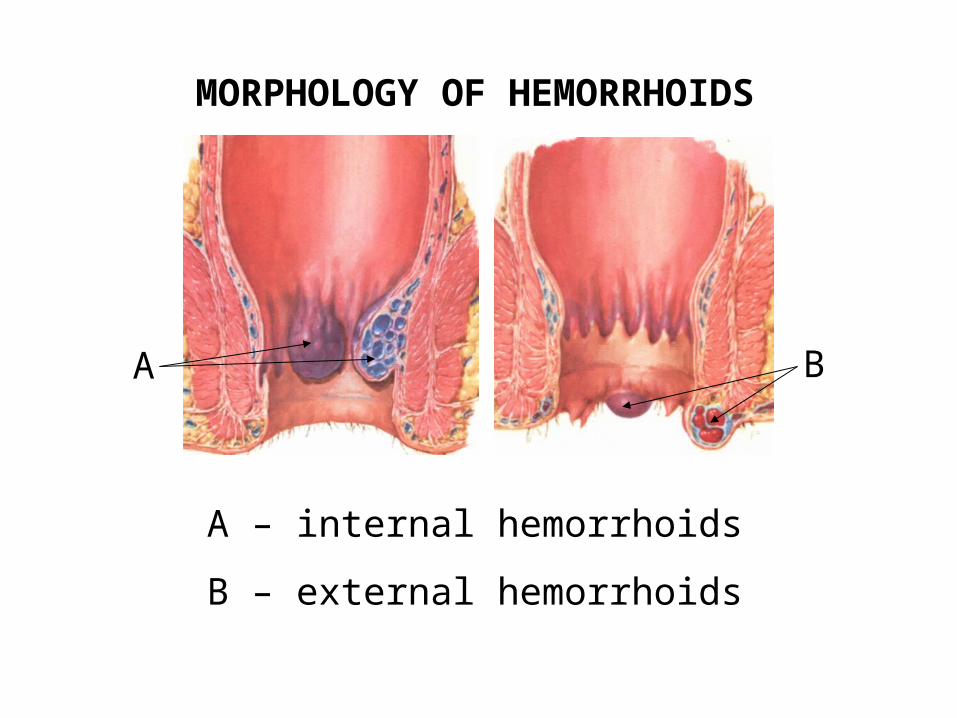
MORPHOLOGY OF HEMORRHOIDS
A B
A – internal hemorrhoids
B – external hemorrhoids
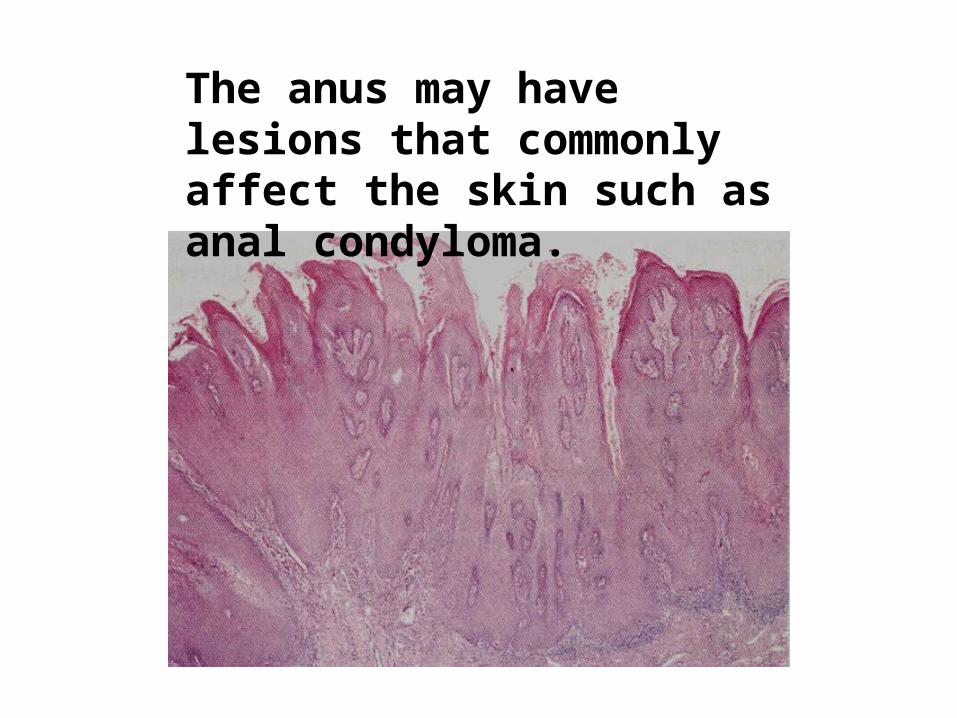
The anus may have lesions that commonly affect the skin such as anal condyloma.