Embed Size (px)
Citation preview
Digestive Pathology Lecture 7
Reproduction Prohibited
This file contains original text and images as well as materials adapted from copyrighted sources
For use only as a temporary educational aid
Partially or completely copying or distributing the contents of this file may constitute an infringement of the fair use exception for teaching
faculty of the U.S. Copyright Law
LSUHSC-New Orleans, 2015
Last updated October 1, 2015
Gallbladder, extrahepatic biliary tract
1. Congenital abnormalities2. Cholelithiasis
3. Cholesterolosis
4. Acute and chronic cholecystitis
5. Choledocholithiasis
6. Cholangitis
7. Neoplasms
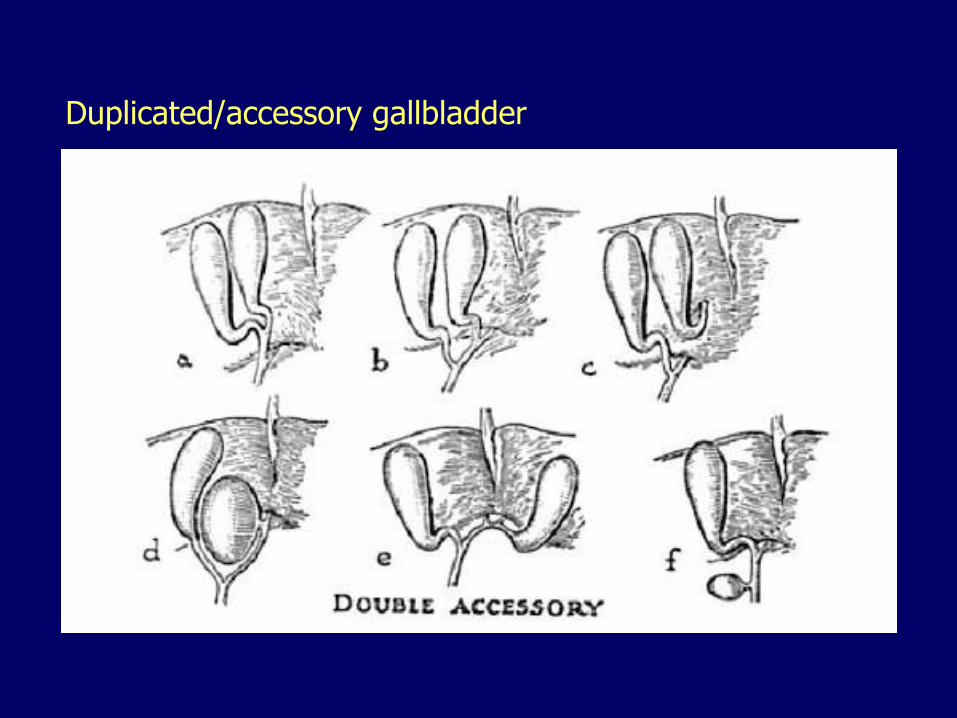
Duplicated/accessory gallbladder
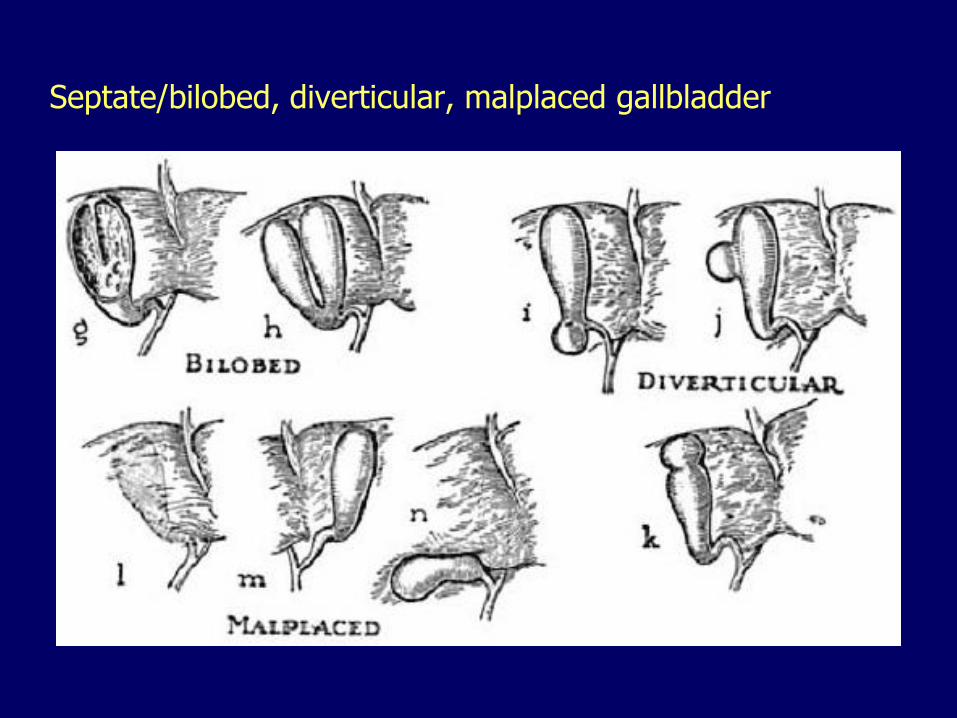
Septate/bilobed, diverticular, malplaced gallbladder
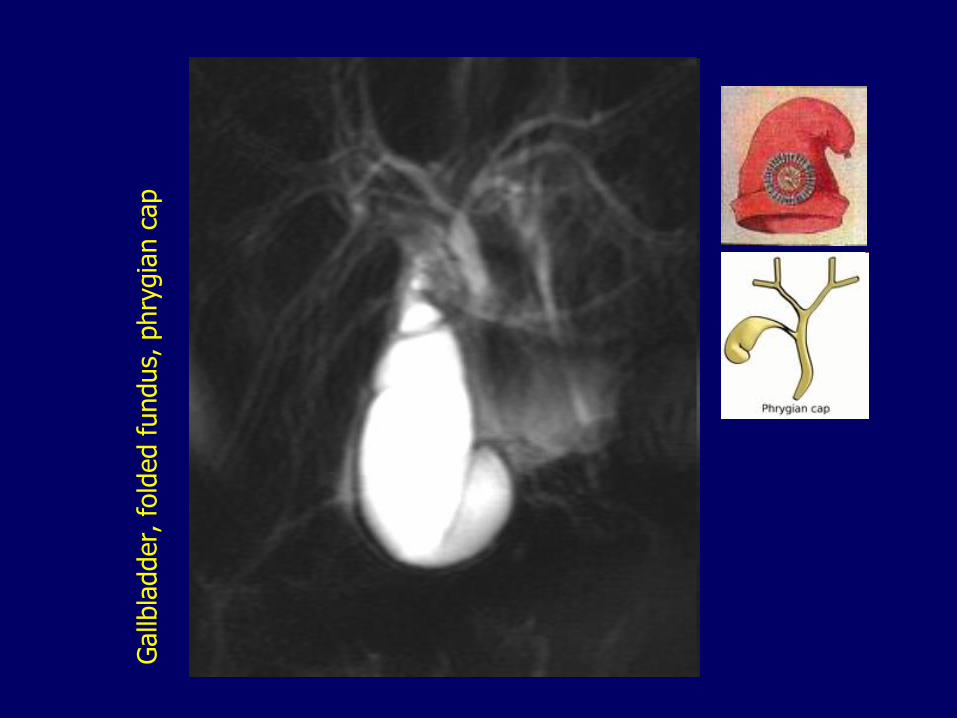
Gallb
ladder,
fold
ed fundus,
phry
gia
n c
ap
Biliary atresia
Complete obstruction
Manifest within the first 3 months of life
One-third of infants with neonatal cholestasis
If untreated, secondary biliary cirrhosis develops within 3-6 months
Accounts for 50-60% of children referred for liver transplantation
Is the most common cause of death from liver disease in early childhood
Biliary atresia, two forms
Fetal (aberrant development), 20%
Perinatal (normal development, secondary injury), the most common– Viral infection
– Apoptosis of bile duct epithelium
– Abnormal inflammatory response
– Genetic predisposition
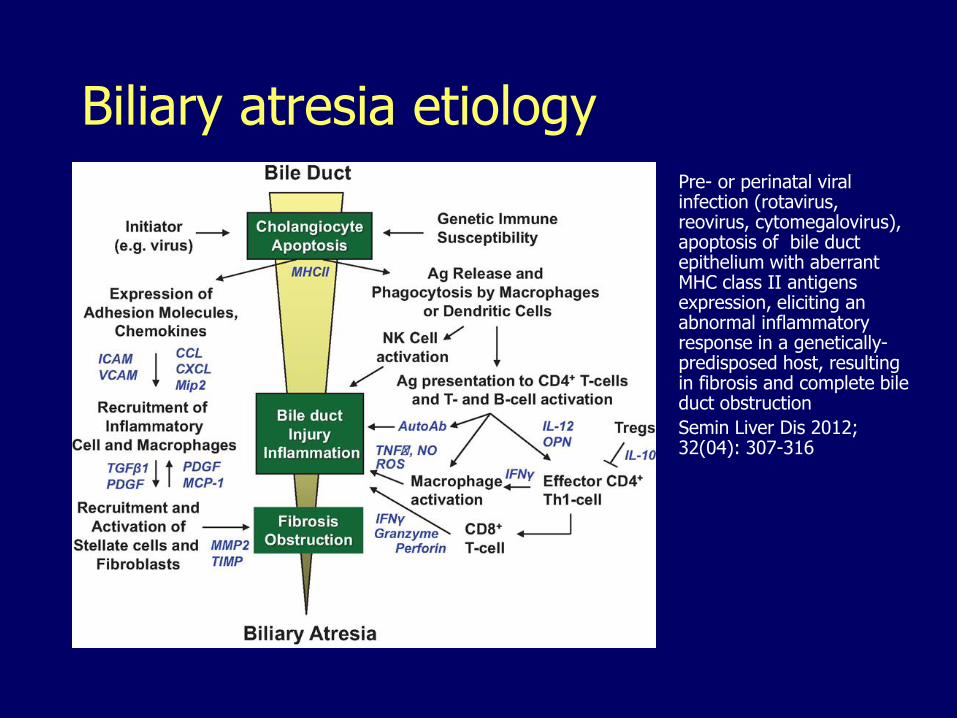
Biliary atresia etiologyPre- or perinatal viral infection (rotavirus, reovirus, cytomegalovirus), apoptosis of bile duct epithelium with aberrant MHC class II antigens expression, eliciting an abnormal inflammatory response in a genetically-predisposed host, resulting in fibrosis and complete bile duct obstruction
Semin Liver Dis 2012; 32(04): 307-316
Biliary atresia, Three types
Type I:– Common bile duct involved
– Patent proximal ducts
Type II:– Hepatic duct involved
– Patent (IIa) OR obliterated (IIb) cystic and common bile ducts
Type III (majority of cases):– Complete extrahepatic biliary atresia (including
right and left hepatic ducts)
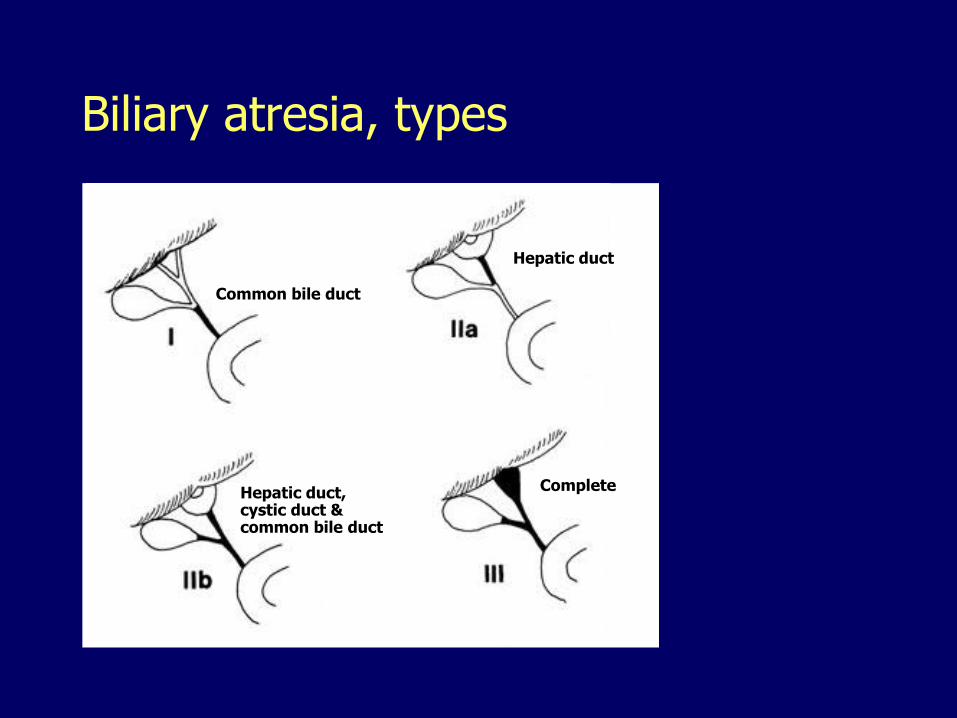
Biliary atresia, types
Common bile duct
Hepatic duct
Hepatic duct,cystic duct &common bile duct
Complete
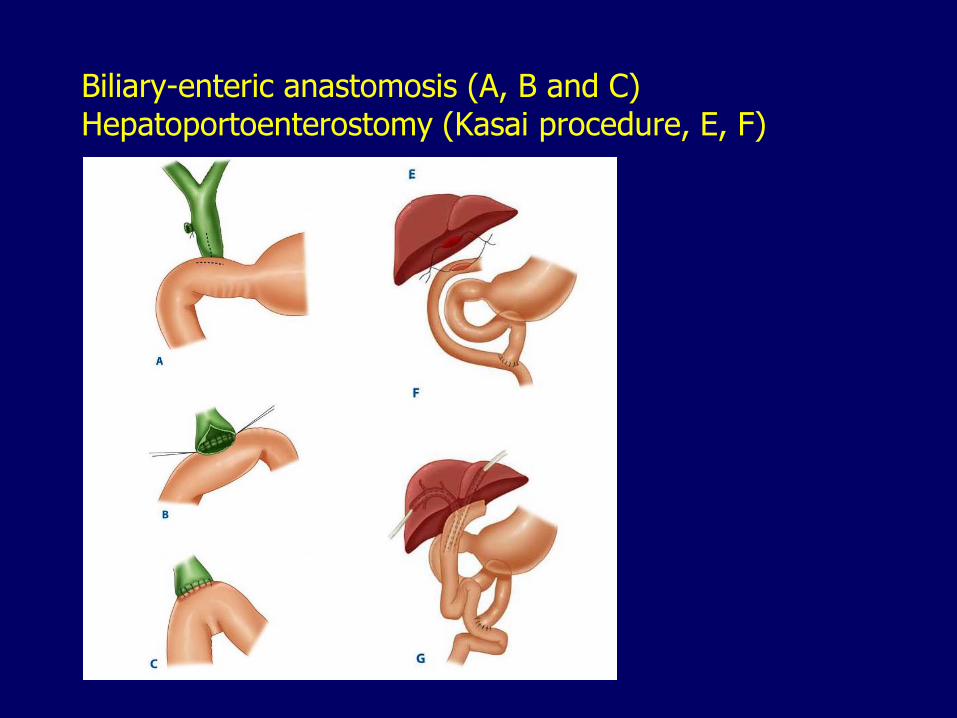
Biliary-enteric anastomosis (A, B and C)Hepatoportoenterostomy (Kasai procedure, E, F)
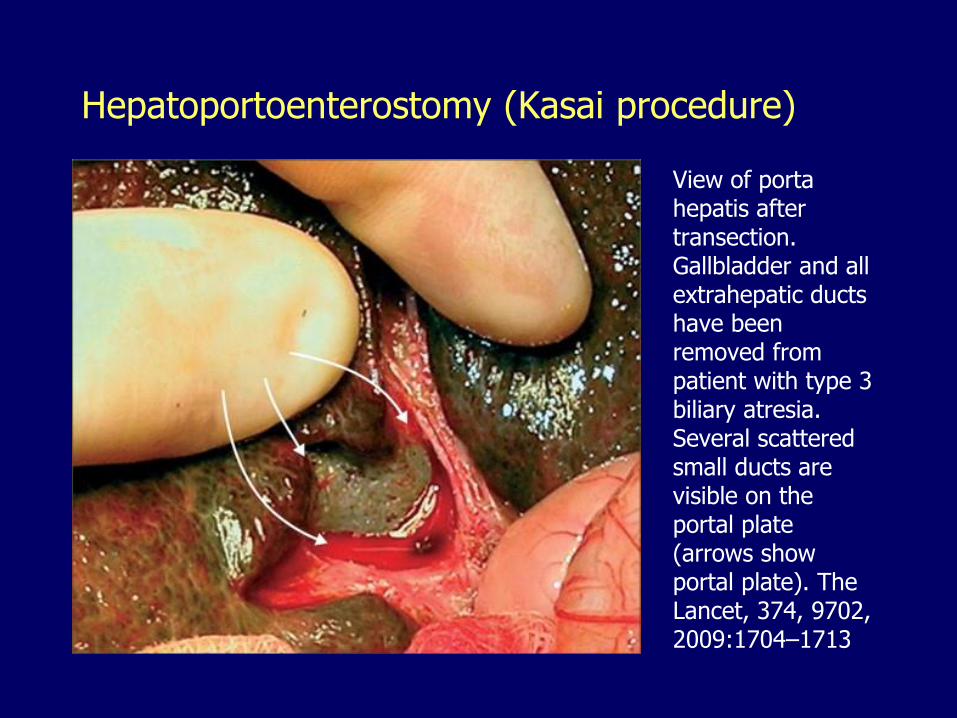
Hepatoportoenterostomy (Kasai procedure)
View of porta hepatis after transection. Gallbladder and all extrahepatic ducts have been removed from patient with type 3 biliary atresia. Several scattered small ducts are visible on the portal plate (arrows show portal plate). The Lancet, 374, 9702, 2009:1704–1713
Choledochal cysts
Congenital cystic dilatations or diverticula of the bile ducts
Most manifest before age 10
More common in females, 4:1
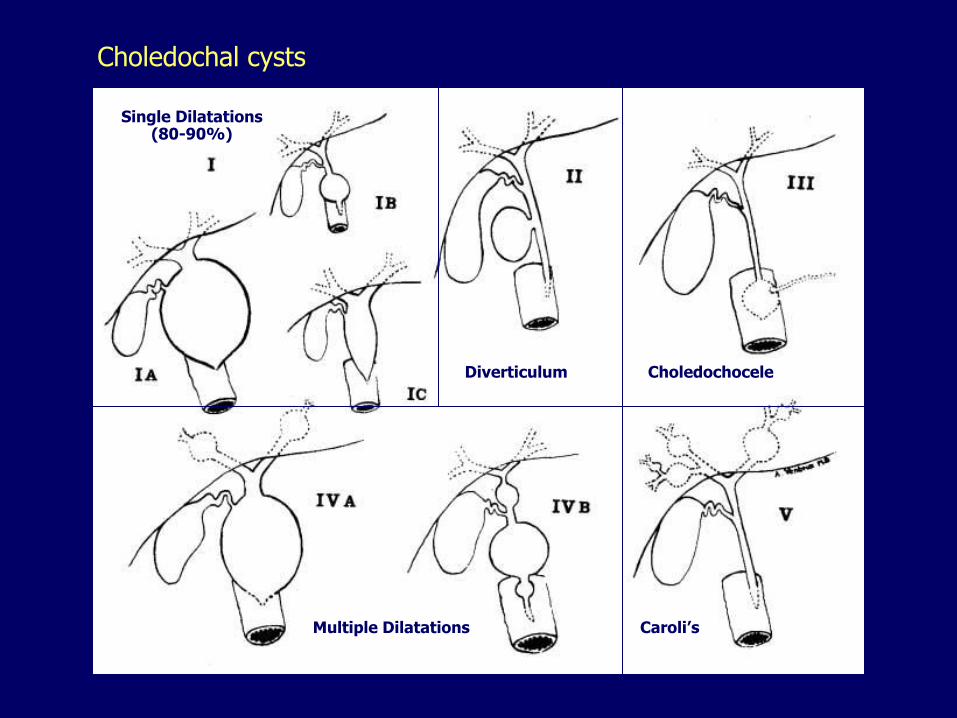
Choledochal cysts
Choledochocele
Multiple Dilatations
Single Dilatations(80-90%)
Diverticulum
Caroli’s
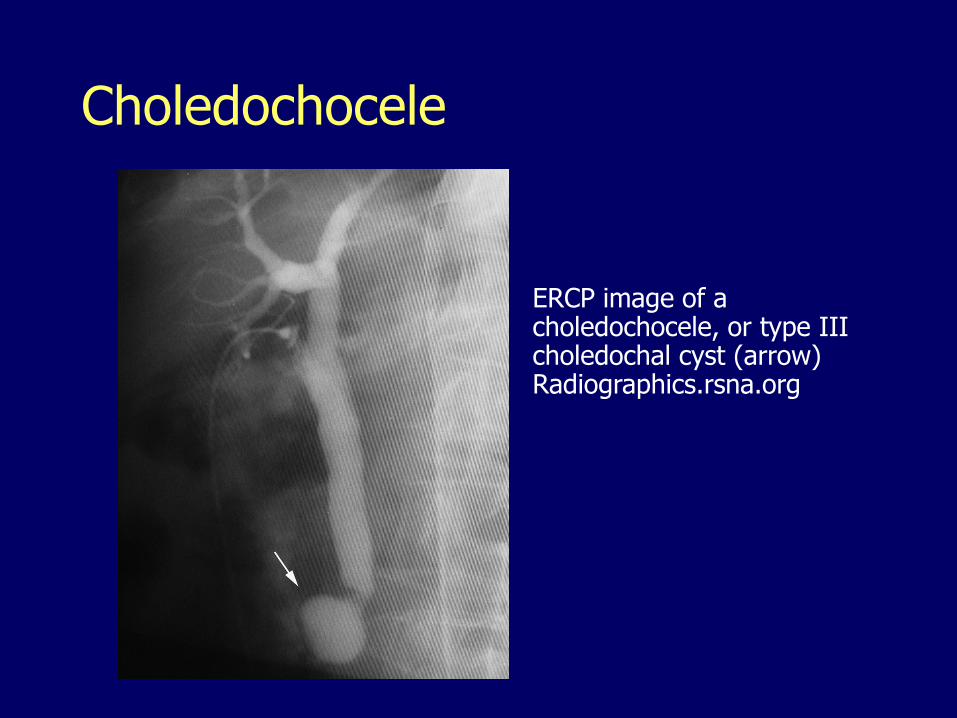
Choledochocele
ERCP image of a choledochocele, or type III choledochal cyst (arrow) Radiographics.rsna.org
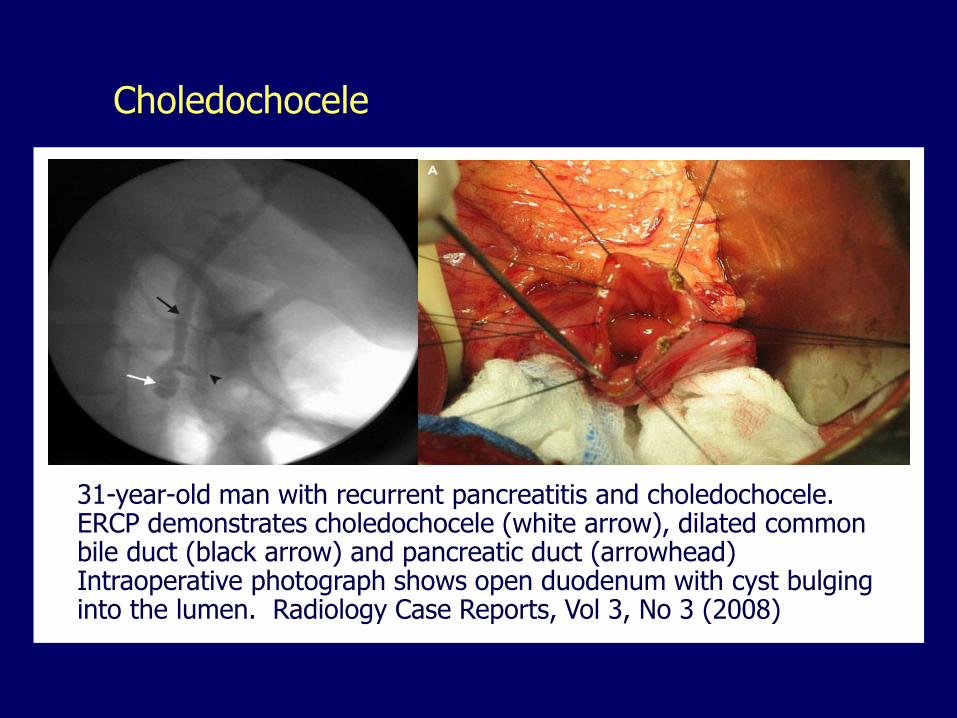
Choledochocele
31-year-old man with recurrent pancreatitis and choledochocele. ERCP demonstrates choledochocele (white arrow), dilated common bile duct (black arrow) and pancreatic duct (arrowhead) Intraoperative photograph shows open duodenum with cyst bulging into the lumen. Radiology Case Reports, Vol 3, No 3 (2008)
Choledochal cysts
May cause:
– Neonatal cholestasis
– Recurrent biliary colic and/or jaundice
– Pancreatitis
Predispose to:
– Stones
– Inflammation
– Stenosis
– Pancreatitis
– Cholangiocarcinoma
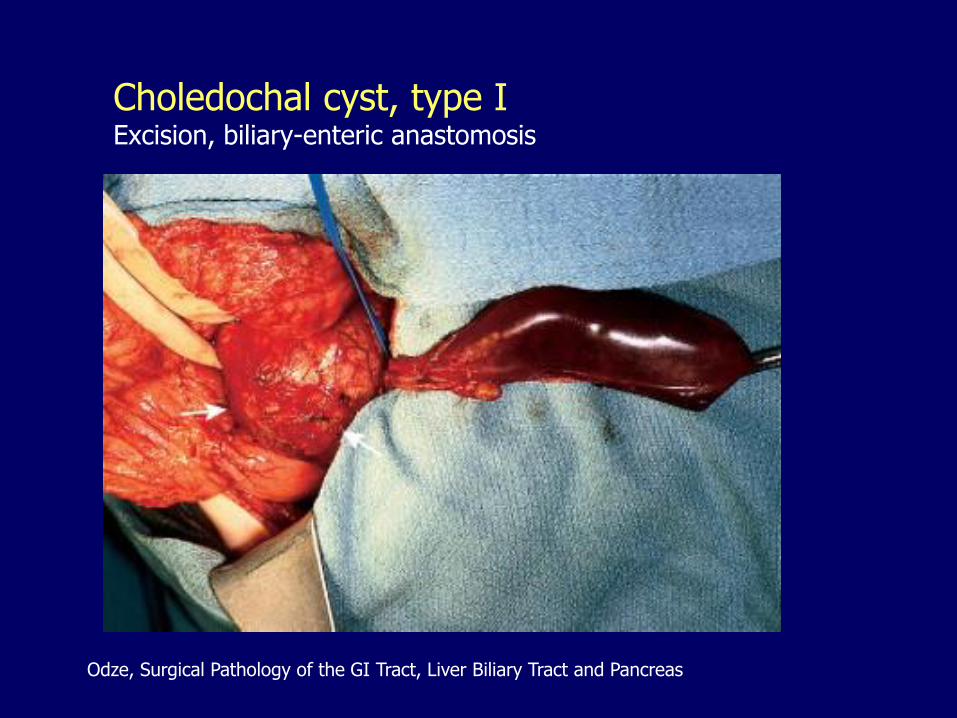
Choledochal cyst, type IExcision, biliary-enteric anastomosis
Odze, Surgical Pathology of the GI Tract, Liver Biliary Tract and Pancreas
Gallbladder, extrahepatic biliary tract
1. Congenital abnormalities
2. Cholelithiasis3. Cholesterolosis
4. Acute and chronic cholecystitis
5. Choledocholithiasis
6. Cholangitis
7. Neoplasms
Cholelithiasis
Calculi (stones) in the gallbladder (gallstones)
Present in 10-20% of the population
Most are silent May cause RUQ/epigastric pain
– constant or
– postprandial (after fat-rich meals)• Subsides gradually in 1 to 5 hours
– may radiate to the right scapular region
– may associate nausea and vomit
Gallstones, shape, size
When solitary or few: large, round or oval
When multiple: faceted (molded)
Size decreases in proportion to their number
Very small stones, called “gravel”, are more likely to escape the gallbladder and produce biliary obstruction
Thick bile is called “sludge”, may also cause obstruction

Gallstones, rounded, faceted
Gallstones, composition
Different amounts of:
– Cholesterol (yellow)
– Calcium bilirubinate (green-black)
– Calcium carbonate (gray-white)
Classified as:
– Pure
– Mixed (80%)
– Combined (nucleus, shell)
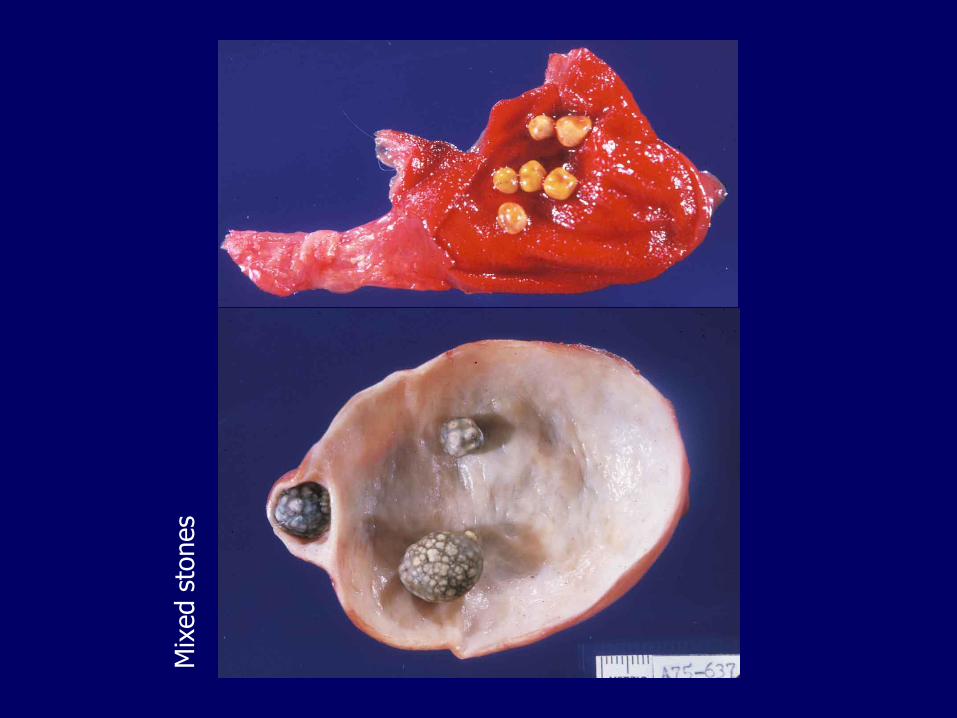
Mix
ed s
tones
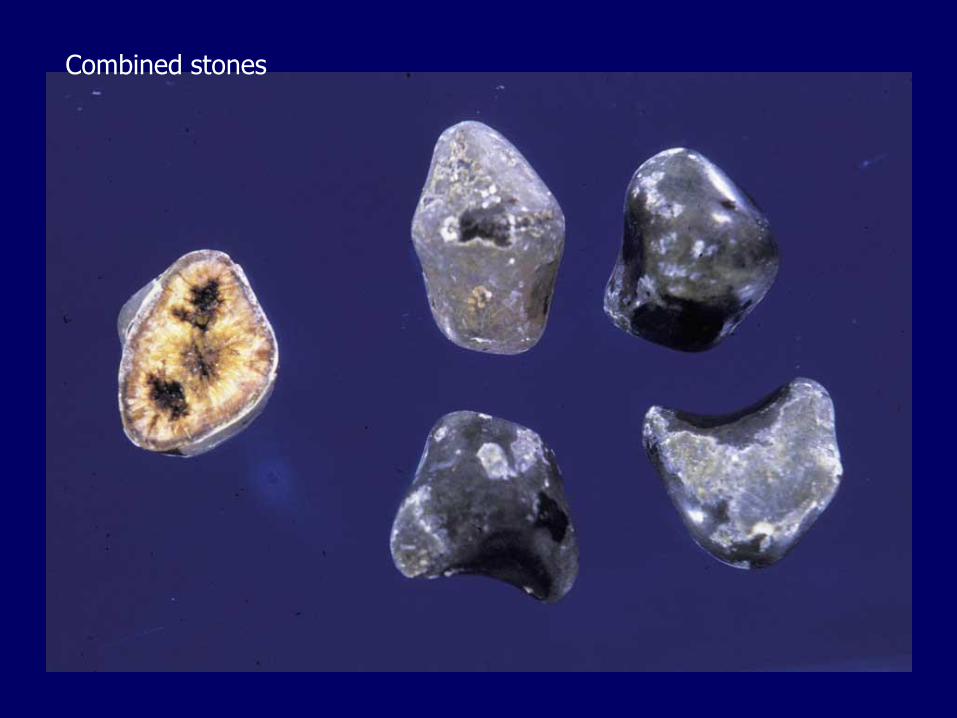
Combined stones
Gallstones, also classified as
Cholesterol stones (80%)
– When made predominantly of cholesterol
– Pale-yellow, yellow-green, yellow-gray
Pigmented
– When made predominantly of calcium bilirubinate
– Brown or jet black
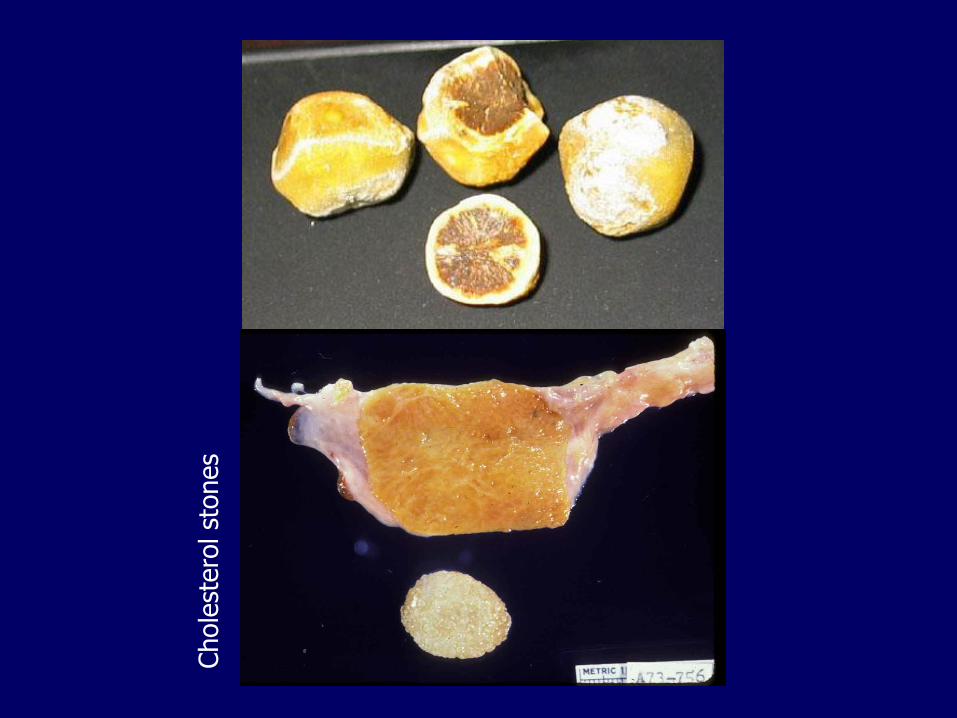
Chole
stero
l st
ones

Pig
mente
d s
tones
Gallstones, radiology
Pure cholesterol stones are radiolucent
Mixed/combined stones are radiopaque depending on their concentration of calcium

Gallstones, plain film

Gallstones, ultrasound
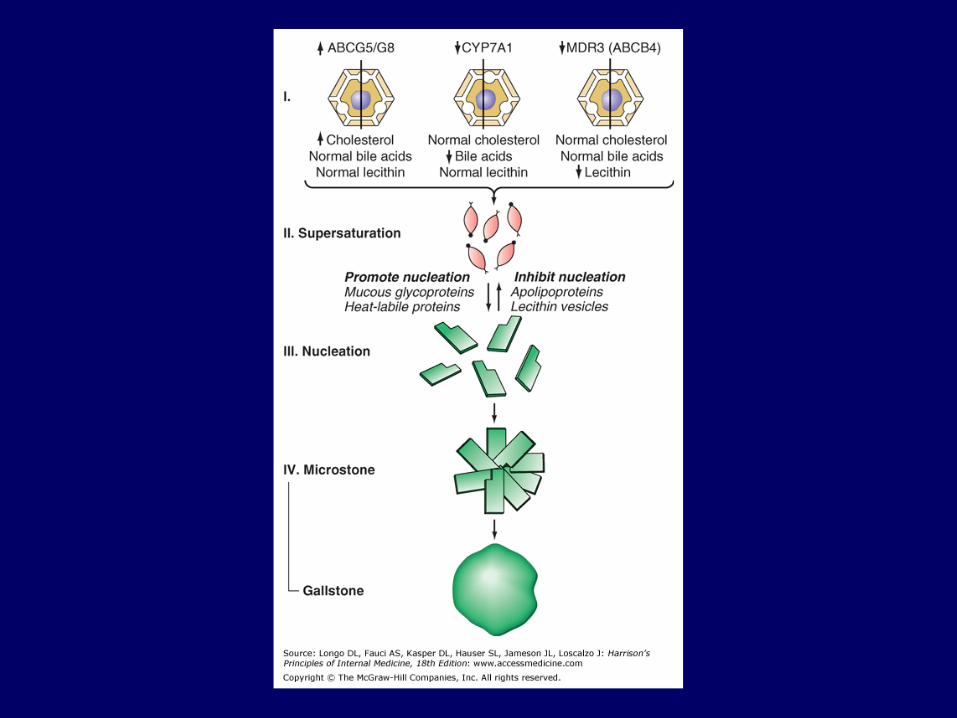
Cholesterol stones, nucleation
In the bile, cholesterol is kept soluble by aggregation with phospholipids and bile acids (lithogenic index)
Nucleation (crystallization) of cholesterol is promoted by
– Supersaturation of bile with cholesterol
– Microprecipitates of inorganic or organic calcium salts
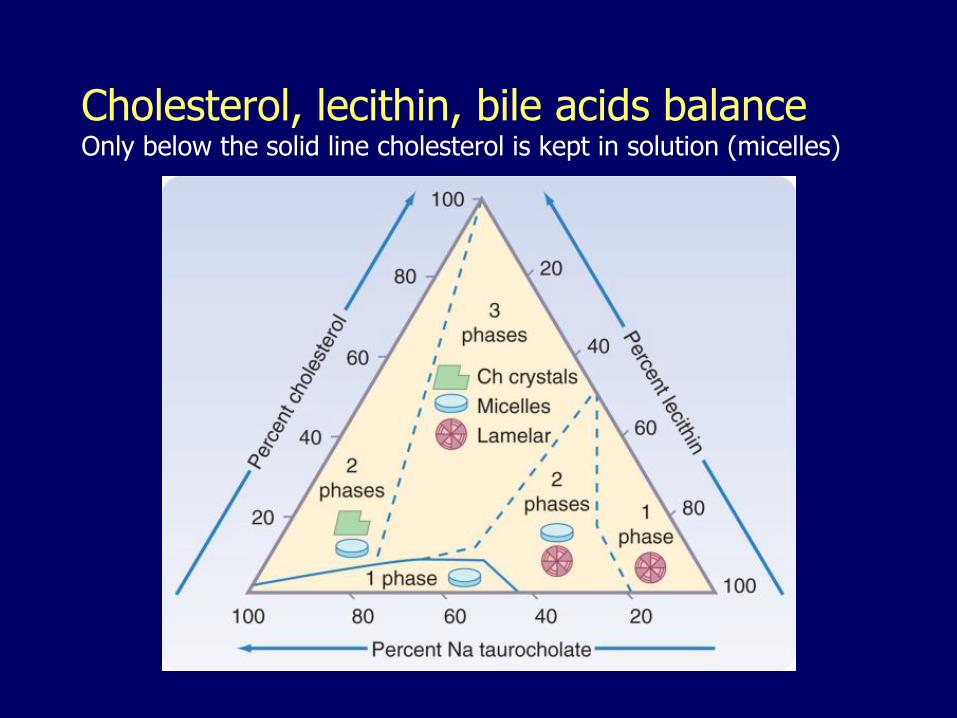
Cholesterol, lecithin, bile acids balanceOnly below the solid line cholesterol is kept in solution (micelles)
Risk factors, cholesterol stones
Native Americans, Hispanics, Northern European Age > 55 Female sex, oral contraceptives, estrogen
replacement therapy, pregnancy Obesity Rapid weight reduction (gastric bypass) Hyperlipidemia Some cholesterol-lowering medications (fibrates) may
increase the risk, others (statins) may decrease the risk
Ileal dysfunction or bypass Gallbladder stasis Family history
Genetic mechanisms
Cholesterol transporter ABCG5/G8 mutation:
– Cholesterol hypersecretion
CYP7A1 mutation:
– Deficiency in the synthesis of bile acids
MDR3 mutation:
– Defective phospholipid export pump in the canalicular membrane
Risk factors, pigmented stones
Asian populations
Hemolytic disorders (hyperbilirubinemia)
Bacterial colonization of the biliary tree (bacterial glucuronidases)
Parasitic colonization of the biliary tree (Ascaris lumbricoides, trematodes)
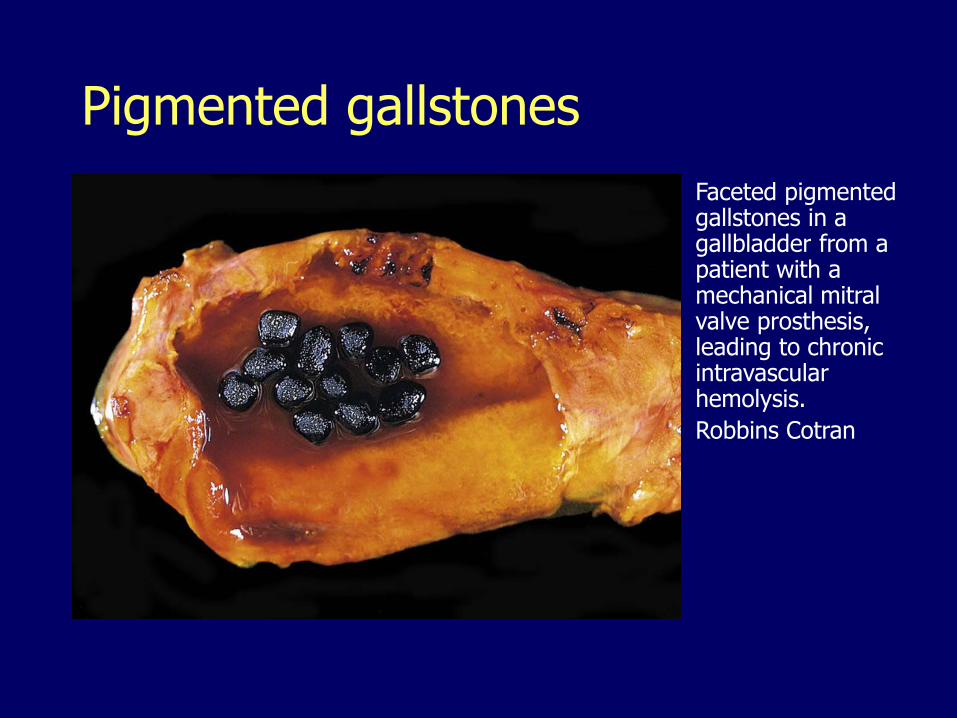
Pigmented gallstones
Faceted pigmented gallstones in a gallbladder from a patient with a mechanical mitral valve prosthesis, leading to chronic intravascular hemolysis.
Robbins Cotran
Gallbladder, extrahepatic biliary tract
1. Congenital abnormalities
2. Cholelithiasis
3. Cholesterolosis4. Acute and chronic cholecystitis
5. Choledocholithiasis
6. Cholangitis
7. Neoplasms
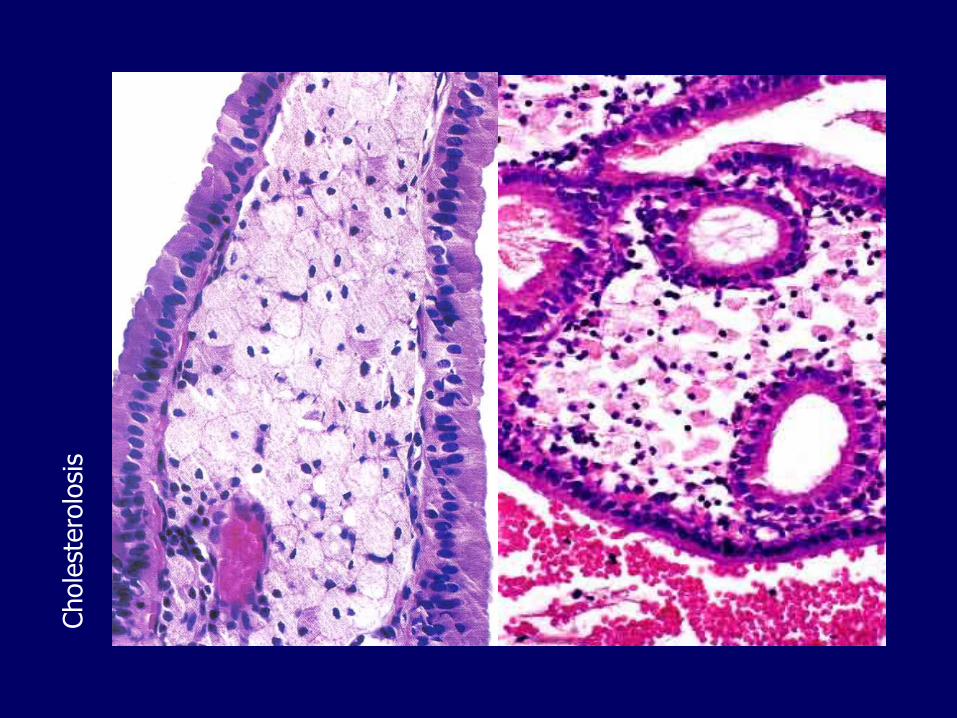
Cholesterolosis
Accumulation of cholesterol esters in foamy histiocytes within the lamina propria
Related to “cholesterol hypersecretion”
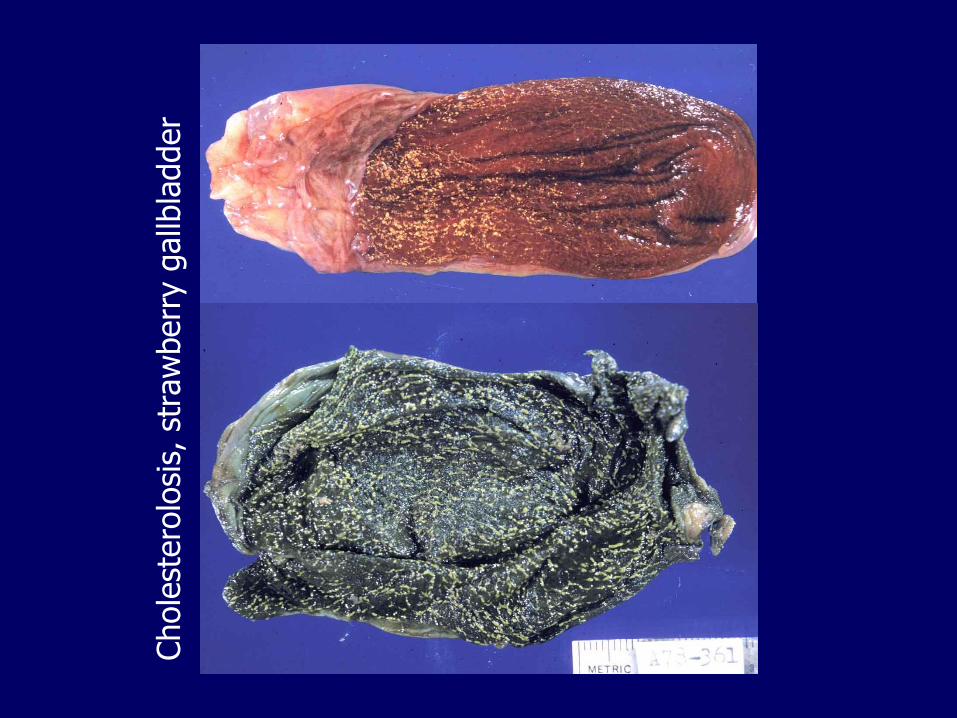
Grossly: “strawberry” gallbladder
Chole
stero
losi
s
Chole
stero
losi
s, s
traw
berr
y g
allb
ladder
Gallbladder, extrahepatic biliary tract
1. Congenital abnormalities
2. Cholelithiasis
3. Cholesterolosis
4. Acute and chronic cholecystitis5. Choledocholithiasis
6. Cholangitis
7. Neoplasms
Cholecystitis
Inflammation of the gallbladder
– Acute vs. chronic
– Calculus (majority) vs. acalculous
Acute cholecystitis
Obstruction of gallbladder neck or cystic duct, by stones, gravel or sludge (90%)
Acute acalculous cholecystitis
– Postpartum, postoperative, trauma, sepsis, shock
• Ischemia/shock (cystic artery is an end-artery with no collateral circulation)
– Prolonged restriction of oral feeding (lack cholecystokinin-induced contraction)
– Primary bacterial infection (diabetes, immunosuppression, HIV/AIDS)
Acute cholecystitis
Symptoms:
– Nausea, vomiting
– Right upper quadrant, epigastric pain > 6 hours
– Murphy’s sign
– Mild fever
– Mild to moderate leukocytosis
– Absence of high fever, chills, jaundice or hyperbilirubinemia
Usually subsides within days
May require immediate surgery
Recurrence is common
Acalculous cholecystitis is masked by underlying condition, high risk of gangrene and perforation
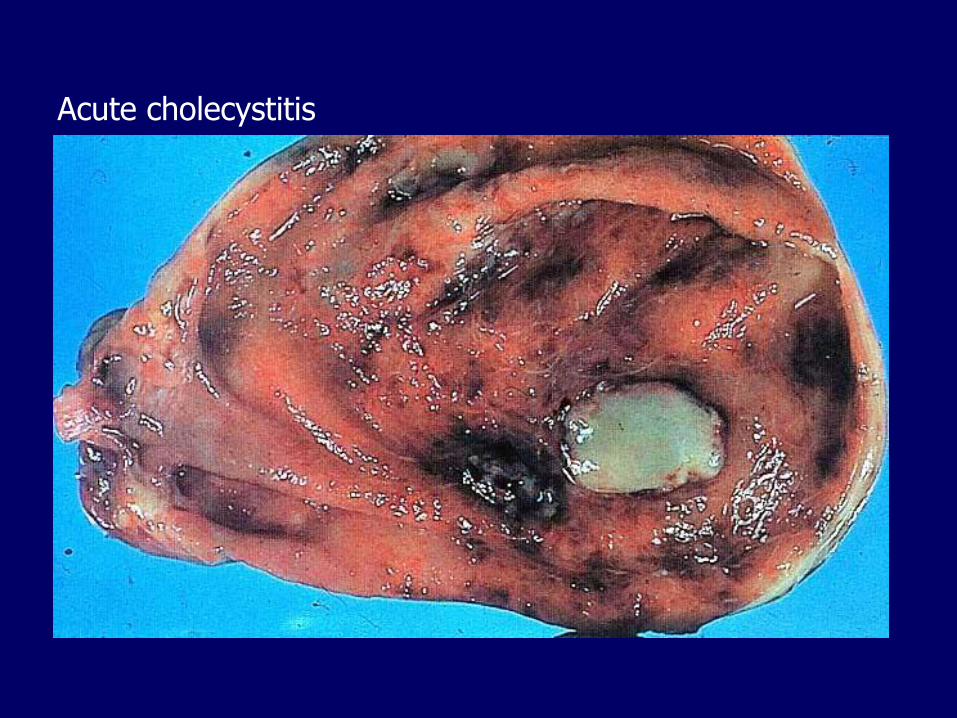
Acute cholecystitis
Chronic cholecystitis
Cholelithiasis >90%
Obstruction not always found
Clinically
– Recurrent attacks of RUQ/epigastric pain as described for cholelithiasis
Microscopically
– Chronic inflammation and fibrosis
– Outpouchings of the mucosa (Rokitansky-Aschoff sinuses)
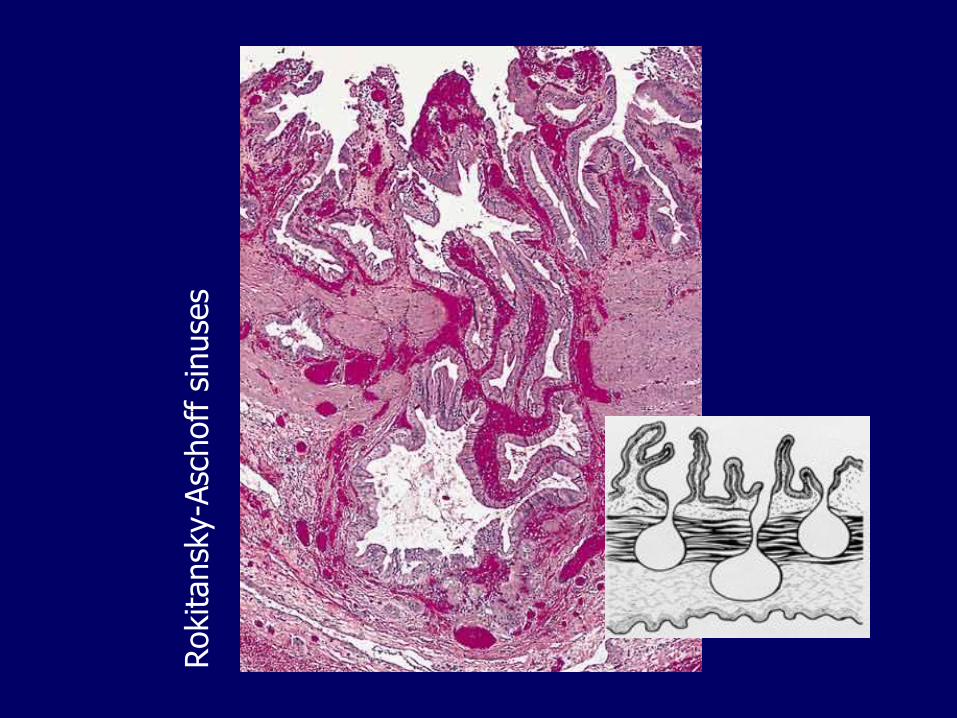
Rokitansk
y-A
schoff
sin
use
s
•
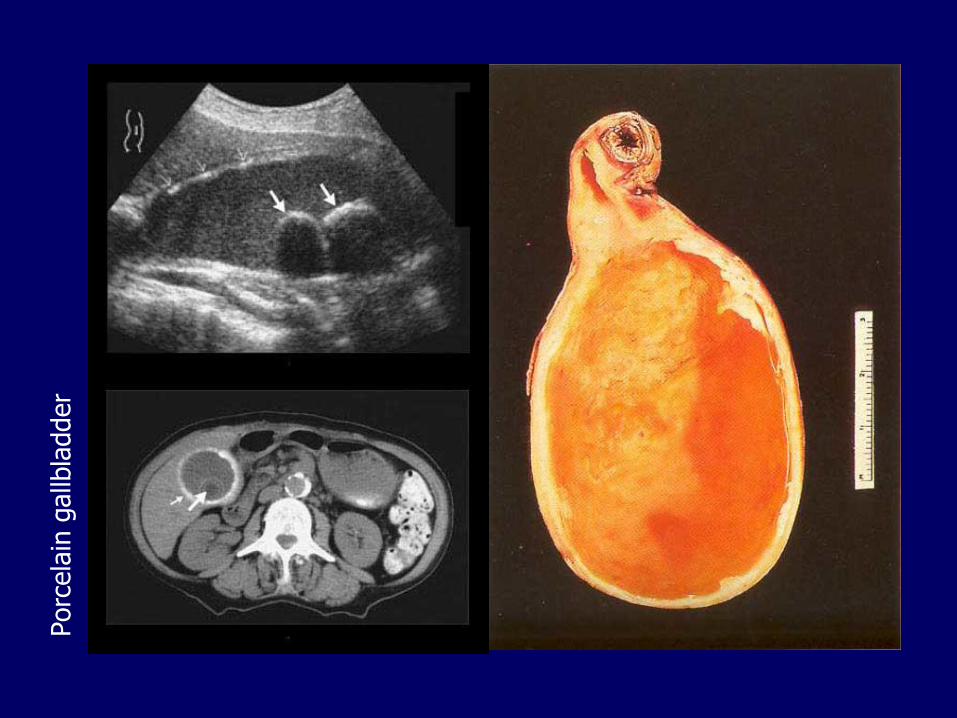
Porc
ela
in g
allb
ladder
Cholecystitis, complications
Choledocholithiasis, cholangitis
Sepsis
Perforation, abscess, peritonitis
Cholecystenteric fistula
– Gallstone ileus
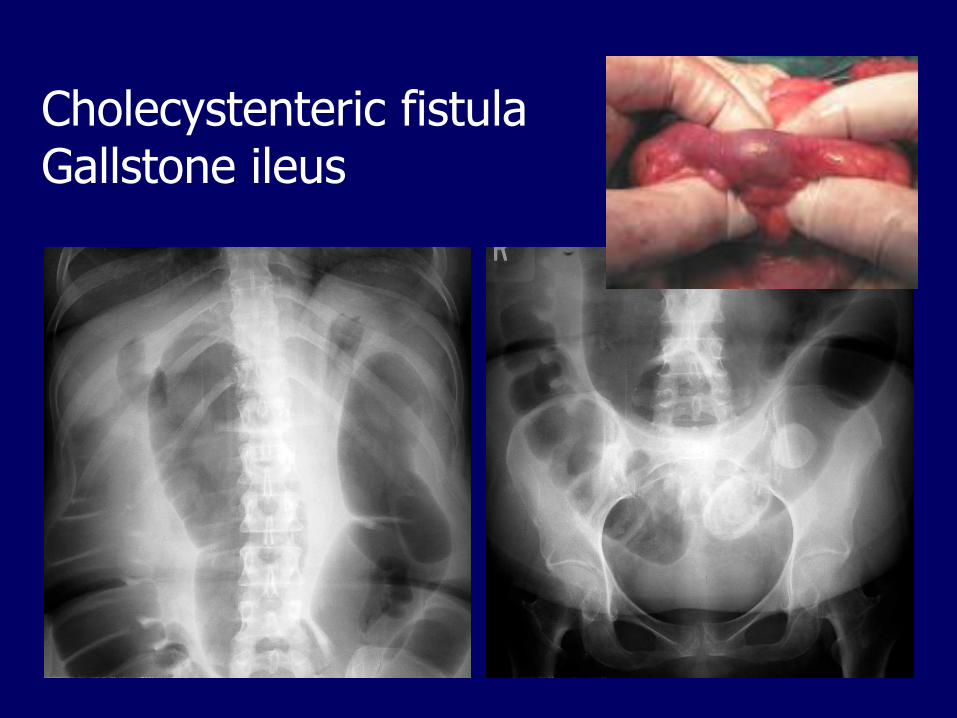
Cholecystenteric fistulaGallstone ileus
Gallbladder, extrahepatic biliary tract
1. Congenital abnormalities
2. Cholelithiasis
3. Cholesterolosis
4. Acute and chronic cholecystitis
5. Choledocholithiasis6. Cholangitis
7. Neoplasms
Choledocholithiasis
Stones within the common bile duct
– Most originate in the gallbladder
– May also form within the bile duct with cysts, bacterial and parasitic infections
Obstruction may cause:
– Pain and jaundice
– Cholangitis
– Secondary biliary cirrhosis
– Pancreatitis
Gallbladder, extrahepatic biliary tract
1. Congenital abnormalities
2. Cholelithiasis
3. Cholesterolosis
4. Acute and chronic cholecystitis
5. Choledocholithiasis
6. Cholangitis7. Neoplasms
Cholangitis
Inflammation of the biliary tract
Results most commonly from
– Choledocholithiasis
– Other sources of obstruction
• Indwelling catheters
• Strictures
• Tumors
• Parasites
• Acute pancreatitis
Cholangitis, clinical findings
The Charcot triad:
– RUQ pain
– Fever, chills
– Jaundice/hyperbilirubinemia
Cholangitis, complications
Is a medical emergency, requires
– Prompt antibiotic therapy
– Endoscopic biliary drainage
– Surgical evacuation
May cause:
– Hepatic abscesses
– Sepsis
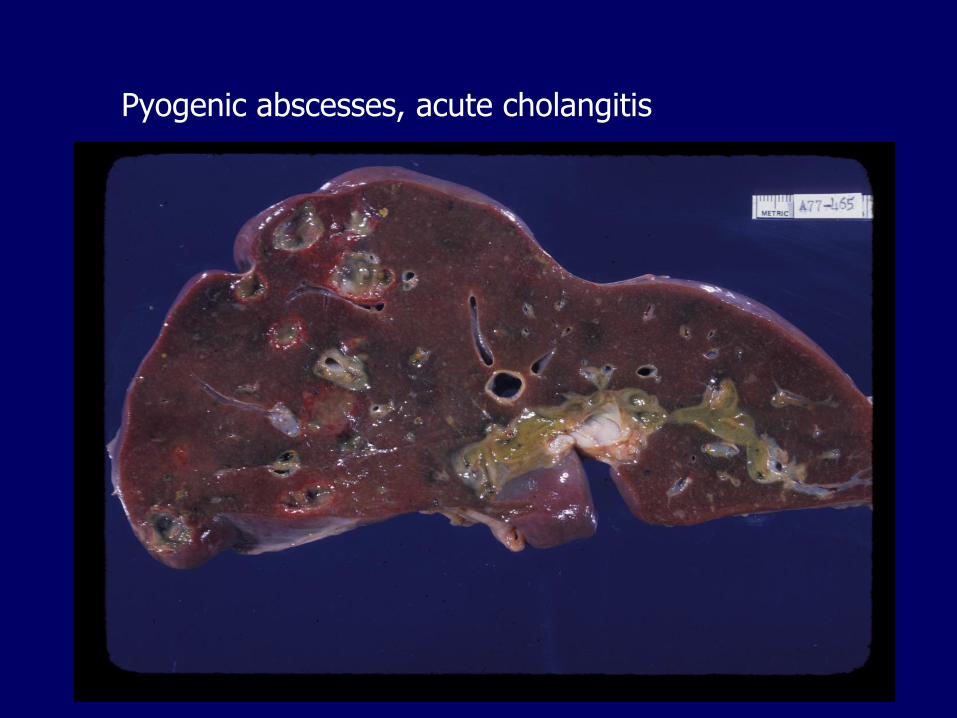
Pyogenic abscesses, acute cholangitis
Gallbladder, extrahepatic biliary tract
1. Congenital abnormalities
2. Cholelithiasis
3. Cholesterolosis
4. Acute and chronic cholecystitis
5. Choledocholithiasis
6. Cholangitis
7. Neoplasms
– Gallbladder adenomas
– Gallbladder carcinomas
– Carcinomas of the extrahepatic bile ducts
Gallbladder adenomas
Rare
Similar to colonic adenomatous polyps may have a tubular, tubulovillous or villousarchitecture
But are lined by gastric-type, intestinal-type or biliary-type epithelium
Have malignant potential
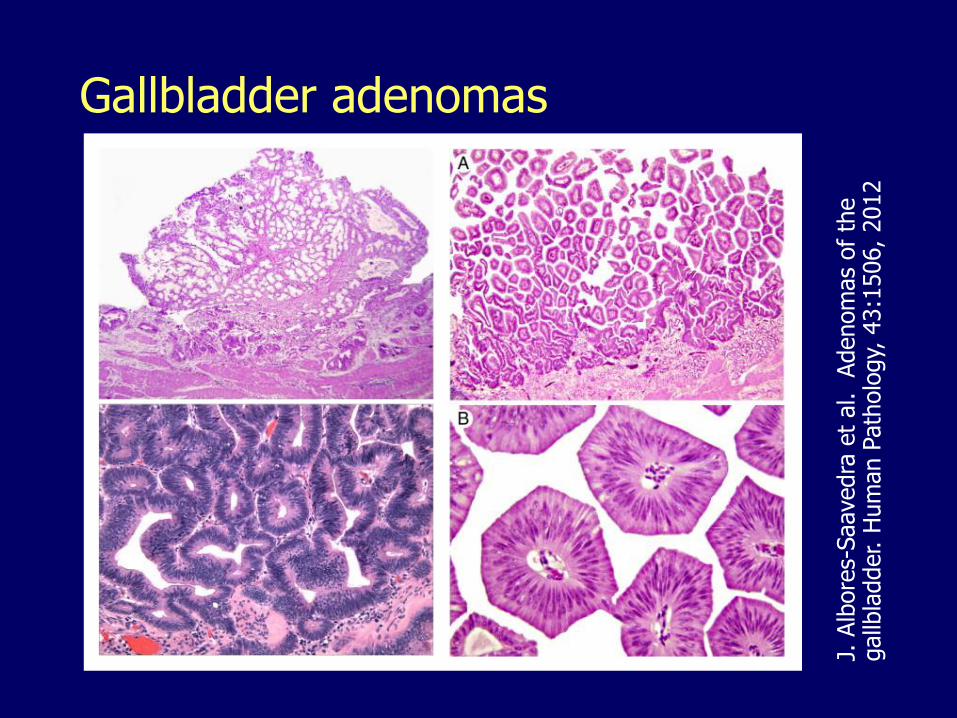
Gallbladder adenomas
J. A
lbore
s-Saavedra
et
al.
Adenom
as
of
the
gallb
ladder. H
um
an P
ath
olo
gy,
43:1
506,
2012
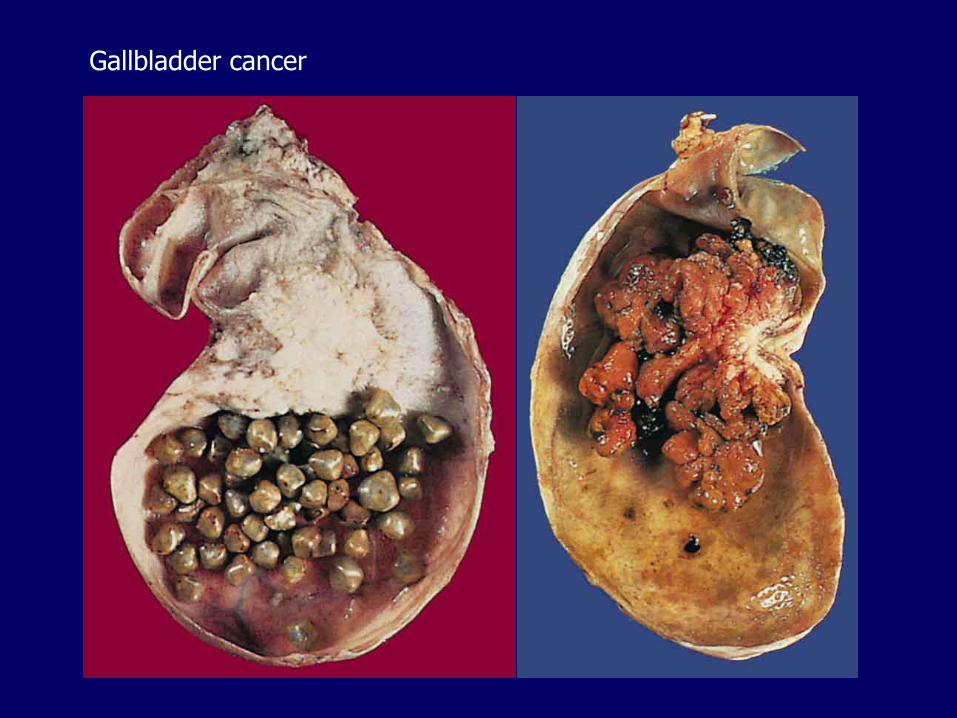
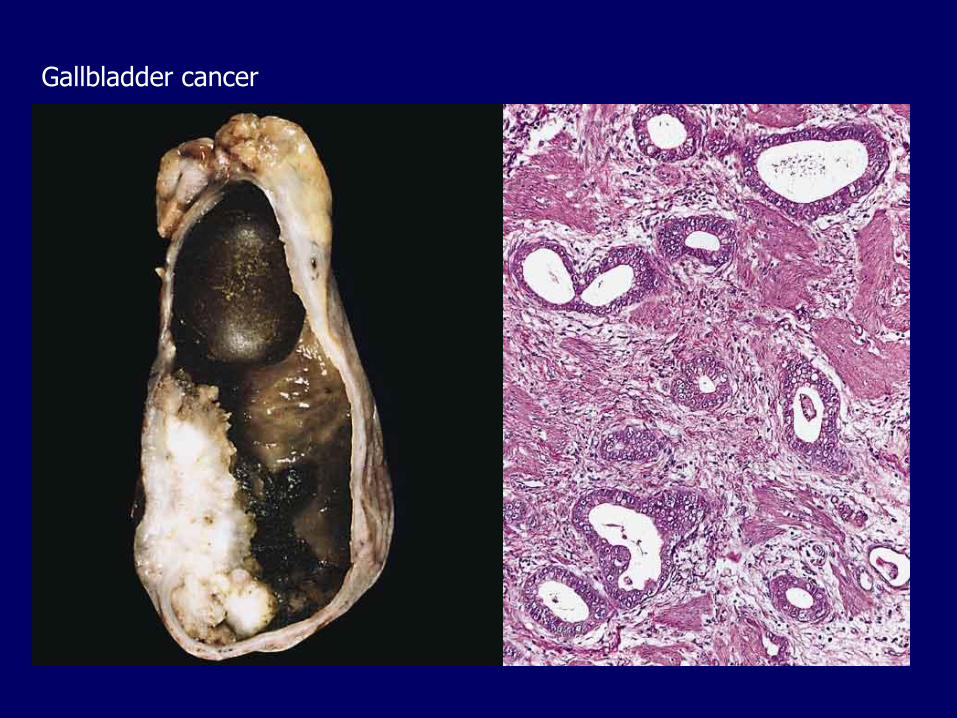
Gallbladder cancer
Infrequent
Most are adenocarcinomas
Risk factors:
– Gallstones (the strongest risk factor)
– Obesity
– Female sex, multiparity
– Old age
– In the US, higher rates in: Native Americans, Hispanics, Korean and Chinese
– Salmonella typhi/paratyphi, Helicobacter bilis, Helicobacter pylori, trematodes
– Anomalous pancreatobiliary junction
Gallbladder cancer
Gallbladder cancer
Gallbladder cancer
Preoperative diagnosis is exceptional
Symptoms are those associated with cholelithiasis
Dismal survival
Carcinoma of extrahepatic bile ducts
Most are adenocarcinomas
Slightly more frequent in men
Association with:
– Primary sclerosing cholangitis, IBD
– Choledochal cysts
– Trematodes
Carcinoma of extrahepatic bile ducts
Signs (Courvoisier’s sign):
– Progressive jaundice
– Painless, palpable gallbladder
Most are not resectable
Short survival
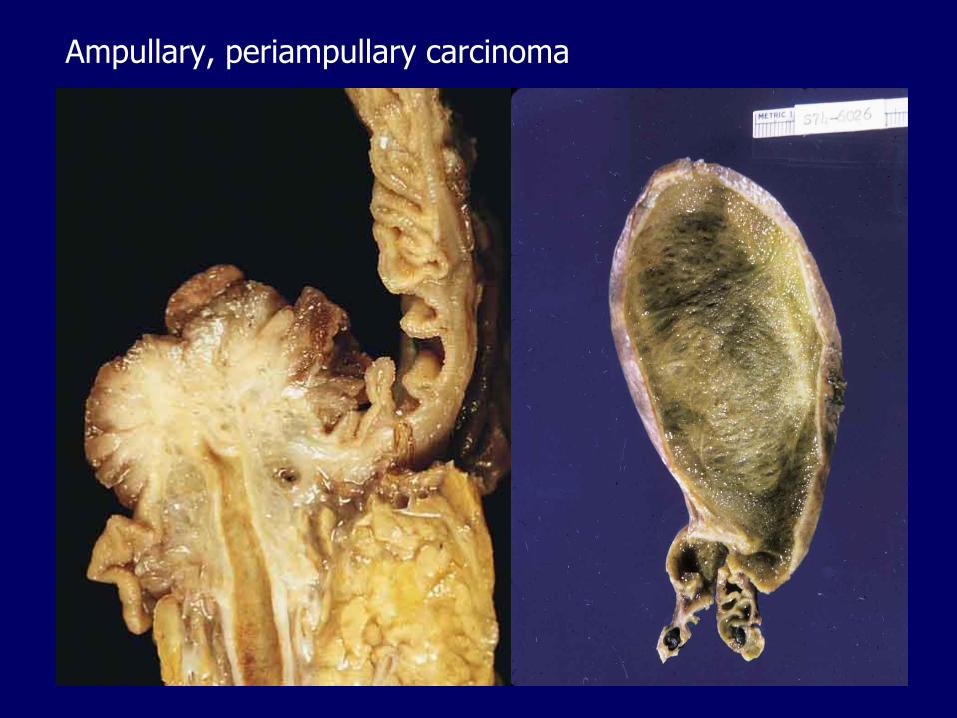
Ampullary, periampullary carcinoma
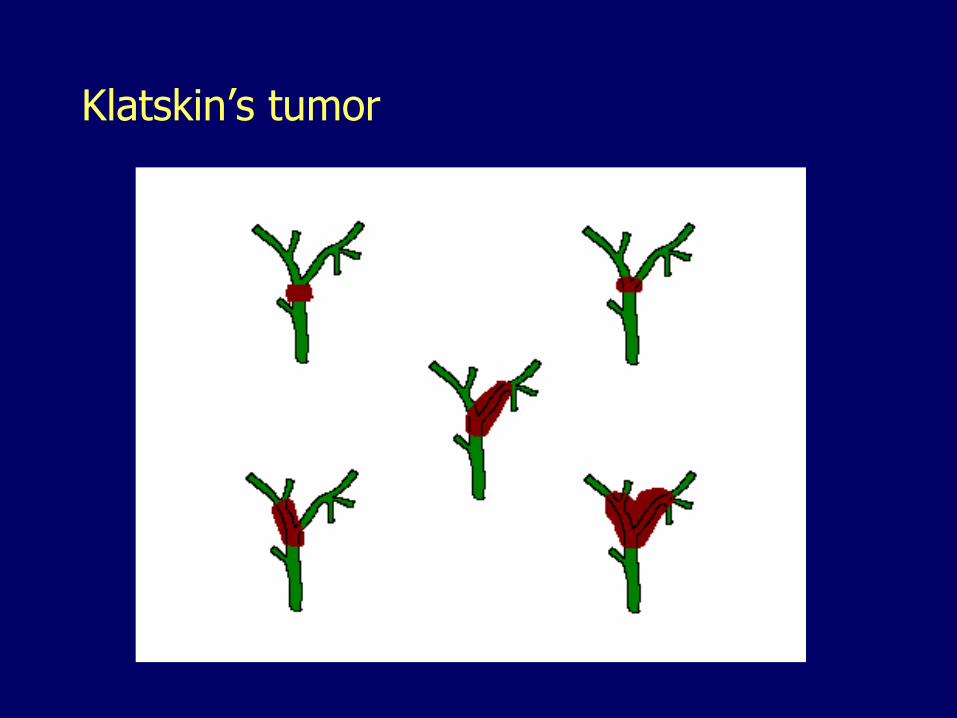
Klatskin’s tumor
Pancreas
1. Congenital malformations
– Pancreas divisum
– Annular pancreas
– Ectopic pancreas
– Congenital cysts2. Pancreatitis
3. Pancreatic cystic neoplasms
4. Pancreatic ductal adenocarcinoma
5. Pancreatic endocrine neoplasms
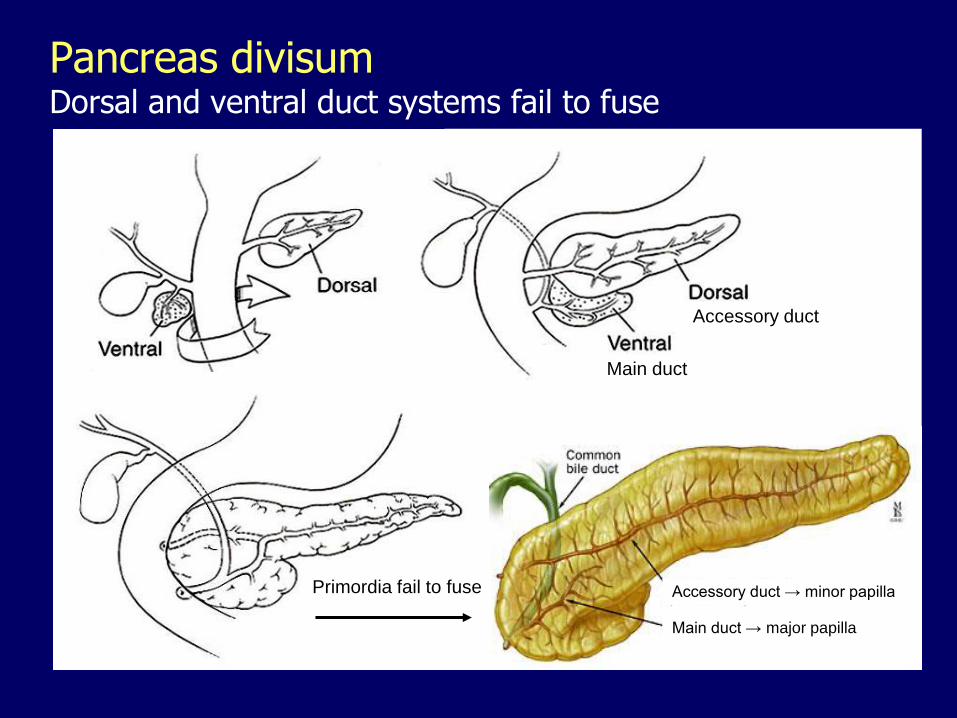
Pancreas divisumDorsal and ventral duct systems fail to fuse
Accessory duct
Primordia fail to fuse
Main duct
Main duct → major papilla
Accessory duct → minor papilla
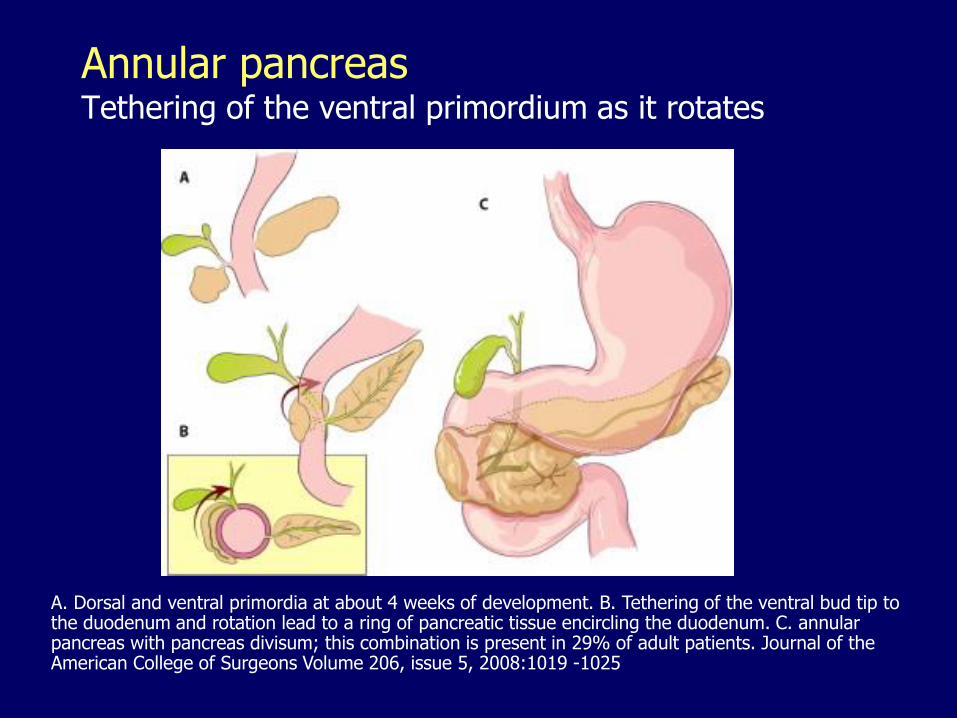
A. Dorsal and ventral primordia at about 4 weeks of development. B. Tethering of the ventral bud tip to the duodenum and rotation lead to a ring of pancreatic tissue encircling the duodenum. C. annular pancreas with pancreas divisum; this combination is present in 29% of adult patients. Journal of the American College of Surgeons Volume 206, issue 5, 2008:1019 -1025
Annular pancreasTethering of the ventral primordium as it rotates
Ectopic/accessory pancreas
Stomach
Duodenum
Jejunum
Ileum
Meckel diverticulum
Mesentery
May cause:
– Inflammation, bleeding
– Tumors
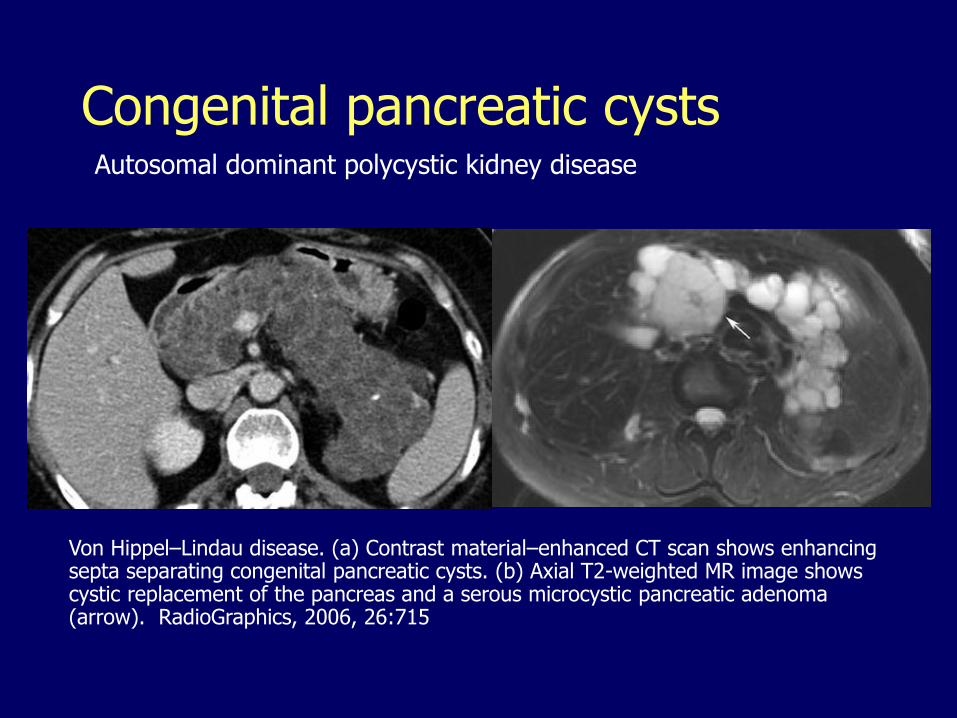
Congenital pancreatic cystsAutosomal dominant polycystic kidney disease
Von Hippel–Lindau disease. (a) Contrast material–enhanced CT scan shows enhancing septa separating congenital pancreatic cysts. (b) Axial T2-weighted MR image shows cystic replacement of the pancreas and a serous microcystic pancreatic adenoma (arrow). RadioGraphics, 2006, 26:715
Pancreas1. Congenital malformations
2. Pancreatitis
– Acute pancreatitis
Pancreatic pseudocyst
– Chronic pancreatitis
– Autoimmune pancreatitis3. Pancreatic cystic neoplasms
4. Pancreatic ductal adenocarcinoma
5. Pancreatic endocrine neoplasms
Acute pancreatitis, main causes
80% of cases:– Alcohol (males)
– Biliary obstruction by gallstones (females)
Cryptogenic: 10-20% (biliary sludge)
Acute pancreatitis, other causes
Pancreas divisum, annular pancreas, choledochocele
Periampullary tumors
Hypertriglyceridemia
Hypercalcemia, hyperparathyroidism
Drugs (thiazide diuretics)
Trauma (blunt, surgical)
Ischemia (shock, vasculitis)
Infections (Mumps)
Mutations in trypsinogen
Mutations in serine protease inhibitor
Mutations causing abnormal bicarbonate secretion
Defense mechanisms
Most pancreatic enzymes are secreted as proenzymes
Proenzymes are activated by trypsin
Trypsinogen is activated in the duodenum by enteropeptidase, avoiding intrapancreatic activation of other proenzymes
Pancreatic acinar and ductal cells secrete trypsin inhibitors (serine protease inhibitor Kazal type 1)
Lipase is secreted in its active form; however, for optimal function it requires colipase that does require activation by trypsin in the intestinal lumen
Acute pancreatitis, pathogenesis
Pancreatitis occurs when normal defenses are deranged mostly by abnormal intrapancreatic activation of trypsin
Alcohol– Direct toxic effect
– Protein-rich secretion, protein plugs
– Contraction of sphincter of Oddi
Obstruction by stones, gravel, sludge, choledochocele, tumors
Viruses, drugs, trauma… (direct acinar injury)
Hereditary pancreatitis
Cationic trypsinogen gene mutation: – Cleavage-resistant trypsin
Serine protease inhibitor Kazal type 1 mutation:– Inactive serine protease, an essential trypsin
inhibitor
Cystic fibrosis CFTR gene mutation: – Abnormal bicarbonate secretion, inspissated
secretions
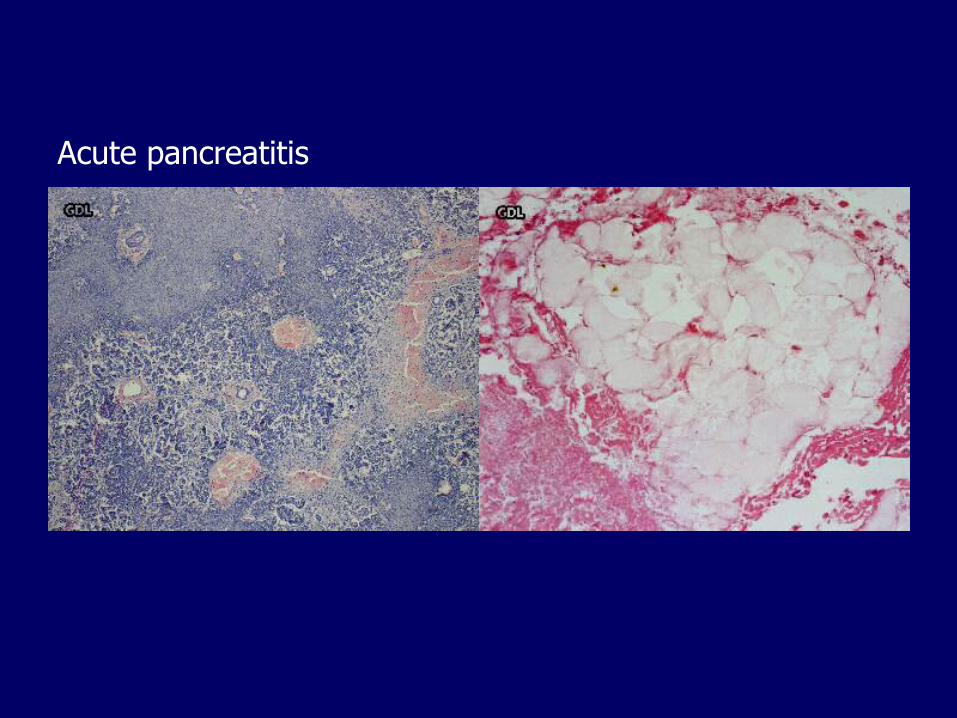
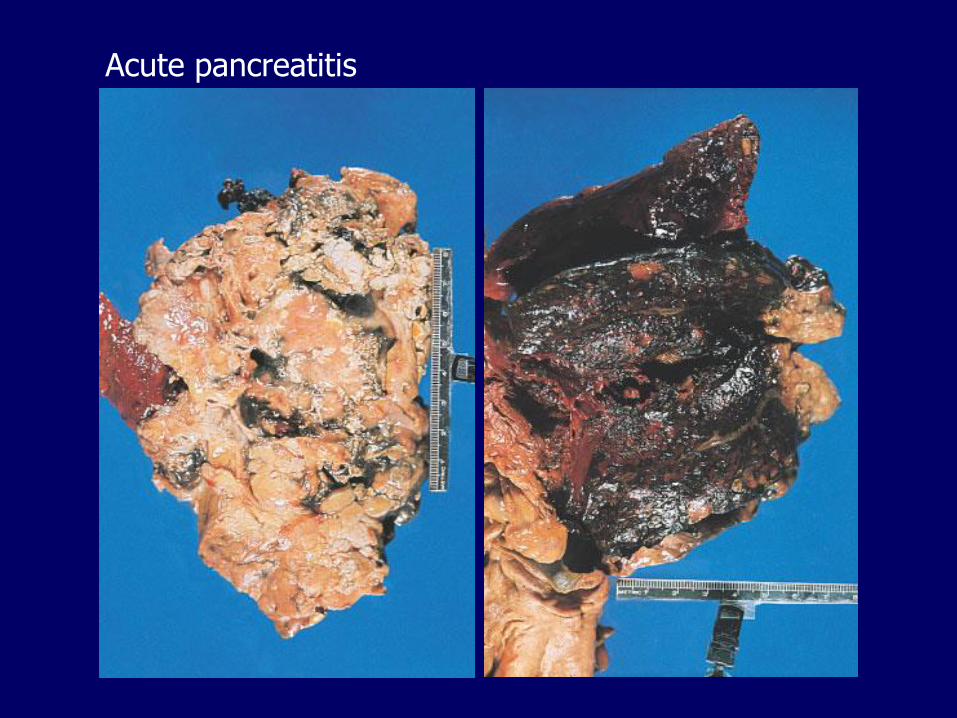
Acute pancreatitis, morphology
Inflammation
Fat necrosis
Released fatty acids combine with calcium to form dark precipitates
Destruction of the parenchyma and vessels, hemorrhage
Acute pancreatitis
Acute pancreatitis
Acute pancreatitis
Precipitated by:
– Alcoholic binge
– Overeating
– Drugs (opiates)
Epigastric pain
– Stabbing, severe, referred to the upper back
Jaundice
– If there is concomitant obstruction of the bile duct
Hemorrhagic exudates:
– Periumbilical ecchymosis
– Flank ecchymosis
– Nodules of subcutaneous fat necrosis

Cullen’s sign
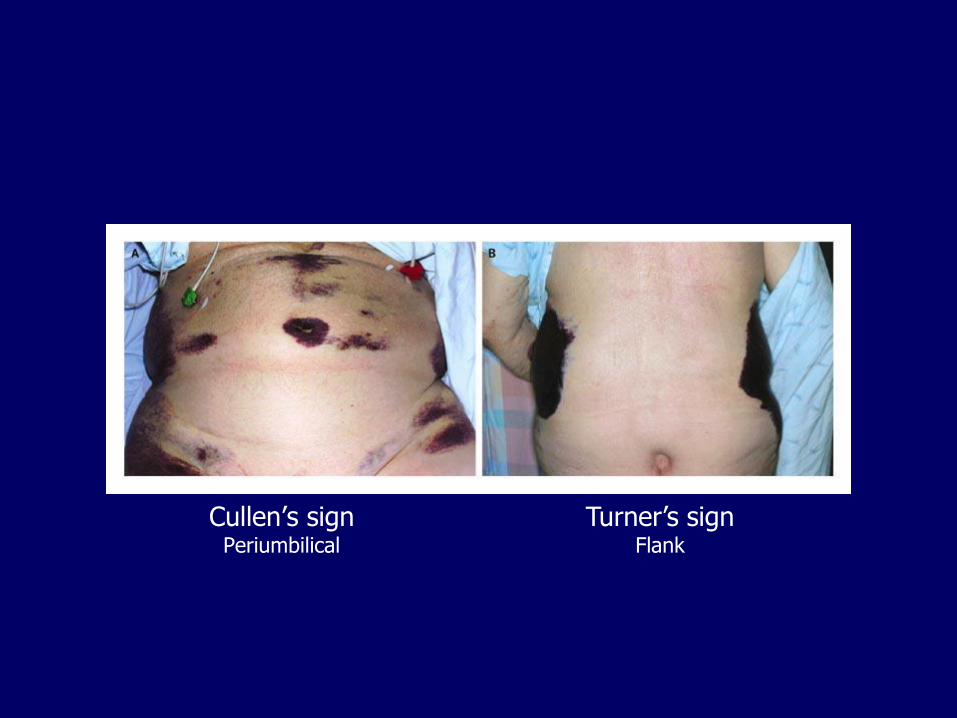
Cullen’s signPeriumbilical
Turner’s signFlank
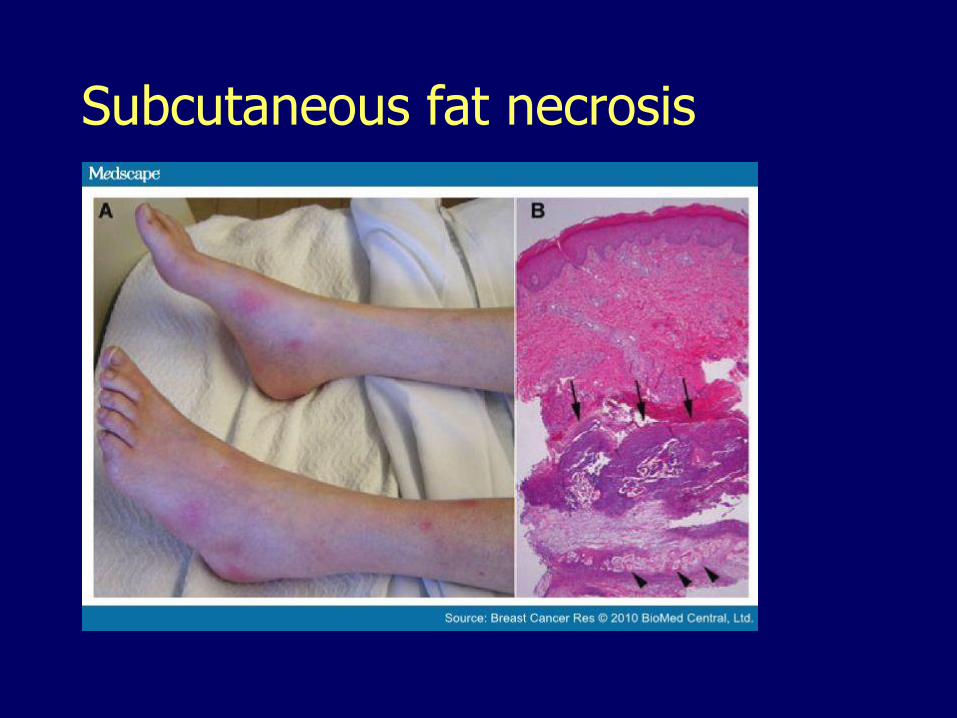
Subcutaneous fat necrosis
Acute pancreatitis, laboratory
Elevation of amylase
Elevation of lipase
Hypocalcemia
Hyperglycemia
Leukocytosis
Electrolyte disturbances
Acute pancreatitis, complications
Disseminated intravascular coagulation
Acute respiratory distress syndrome
Shock, acute renal failure
Abscess (sterile or infected)
Splenic/portal venous thrombosis
Pancreatic pseudocyst
Pancreatic pseudocyst
Walled-off collection of debris and fluid rich in pancreatic enzymes
Wall lacks epithelial lining
Usually solitary
Arise after episodes of acute pancreatitis, chronic pancreatitis with acute exacerbation
May be caused by trauma (blunt, penetrating or operative)
May retain a communication with the ductal system
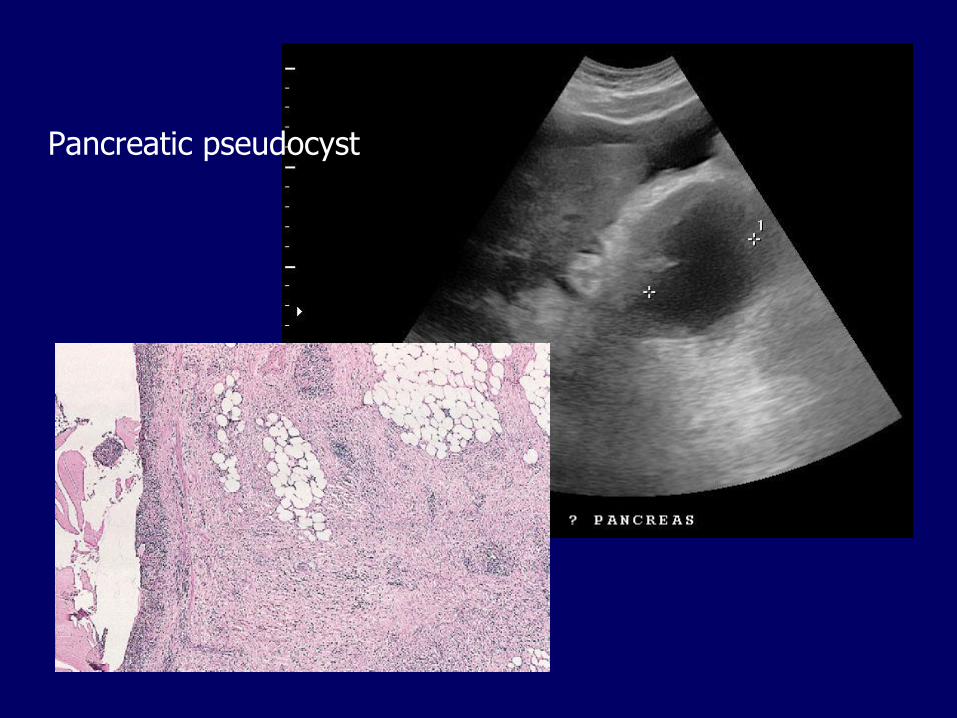
Pancreatic pseudocyst
Pancreatic pseudocyst
May
– Resolve spontaneously
– Become infected
– Compress adjacent structures
– Erode into adjacent vessels causing abundant bleeding
– Rupture
Chronic pancreatitis, causes
Repeated bouts of acute pancreatitis
Alcoholism, the most common cause
Long-standing pancreatic duct obstruction (gallstones, neoplasms)
Pancreas divisum
Hereditary pancreatitis
Tropical pancreatitis
Autoimmune pancreatitis
Idiopathic, up to 40%
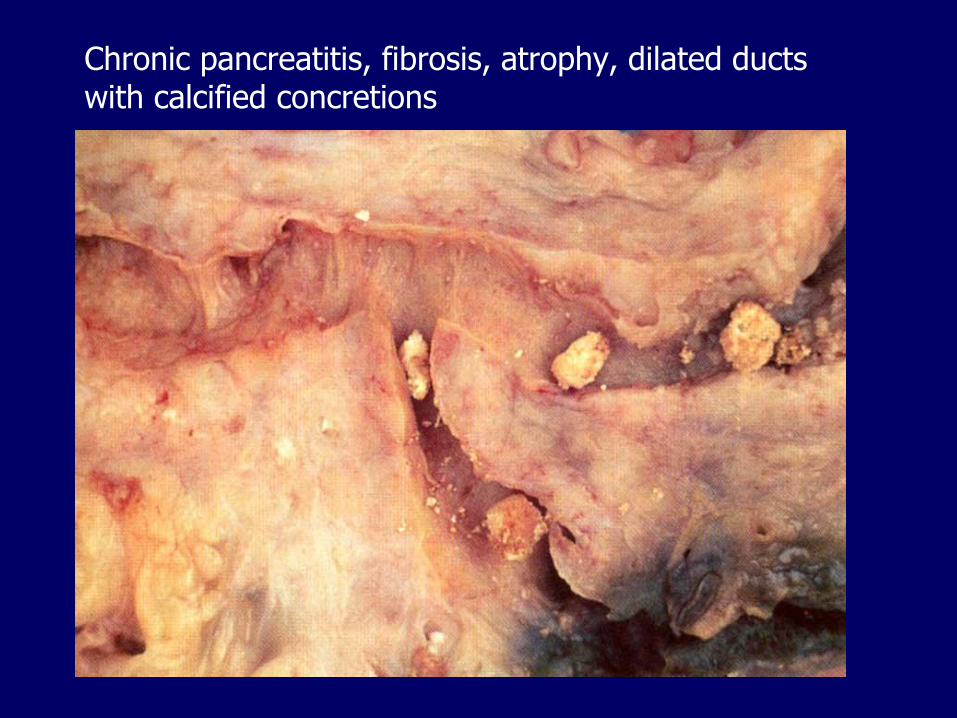
Chronic pancreatitis, fibrosis, atrophy, dilated ducts with calcified concretions
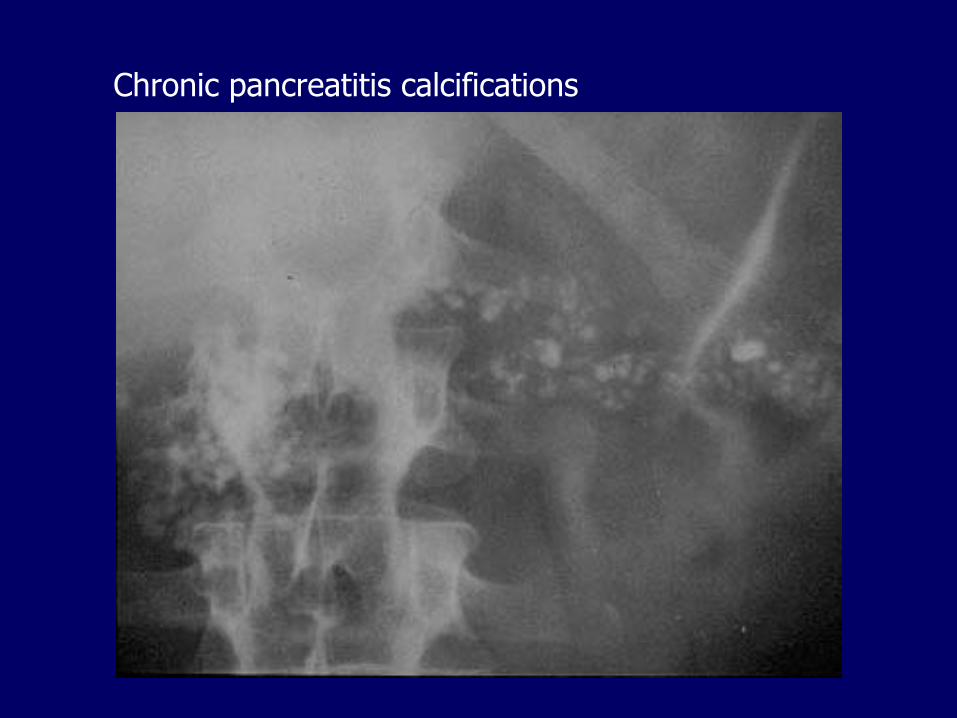
Chronic pancreatitis calcifications
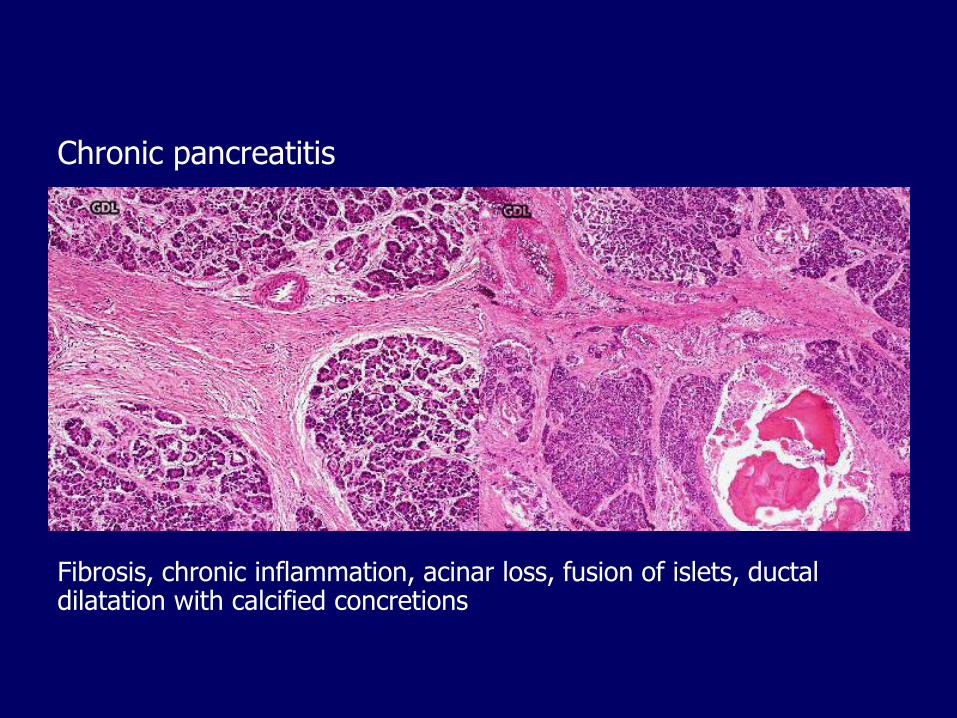
Chronic pancreatitis
Fibrosis, chronic inflammation, acinar loss, fusion of islets, ductal dilatation with calcified concretions
Chronic pancreatitis, outcome
Atrophy:
– With repeated attacks of acute pancreatitis amylase and lipase may fail to elevate after a substantial portion of the acinar parenchyma is lost
– Malabsorption (pancreatic insufficiency)
– Diabetes
Chronic pain
Pancreatic cancer
– With hereditary pancreatitis, 40% risk
Autoimmune pancreatitis
Periductal inflammation with abundant IgG4-secreting plasma cells
Periductal fibrosis with ductal narrowing
Response to steroid treatment
Older men
Involvement of bile ducts and gallbladder and many other organ systems (IgG4-related disease)
Often presents with obstructive jaundice, mimicking pancreatic cancer
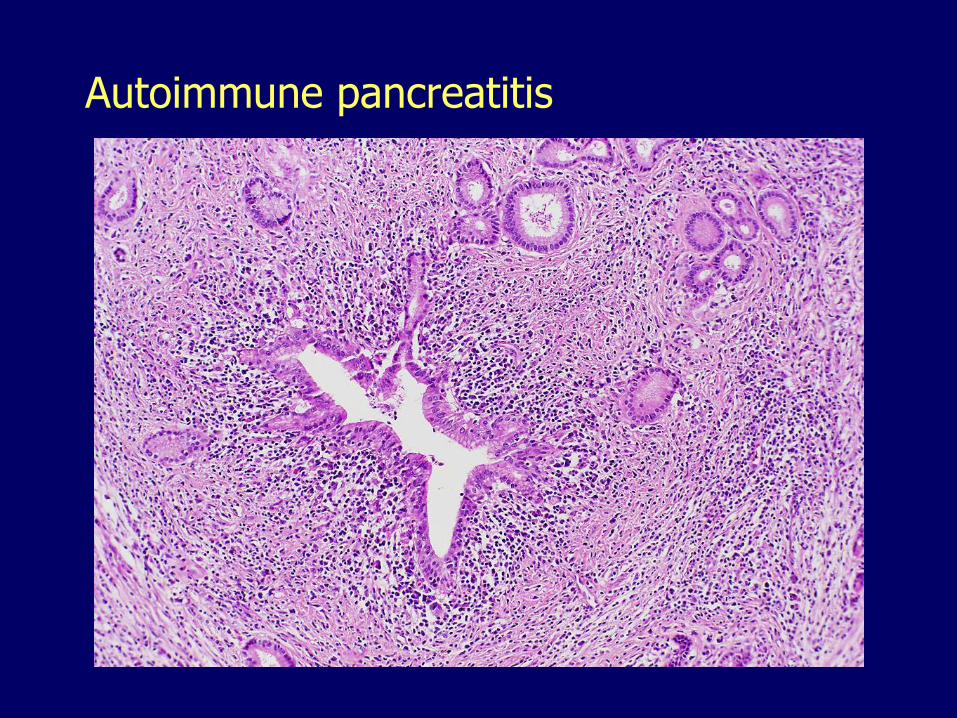
Autoimmune pancreatitis
Pancreas1. Congenital malformations
2. Pancreatitis
3. Pancreatic cystic neoplasms
– Serous
– Mucinous
– Intraductal papillary mucinous
4. Pancreatic ductal adenocarcinoma
5. Pancreatic endocrine neoplasms
Serous cystadenomas
More common in women
Microcystic (numerous small cysts)
Clear, thin, straw-colored fluid
Low cuboidal epithelium
Almost always benign
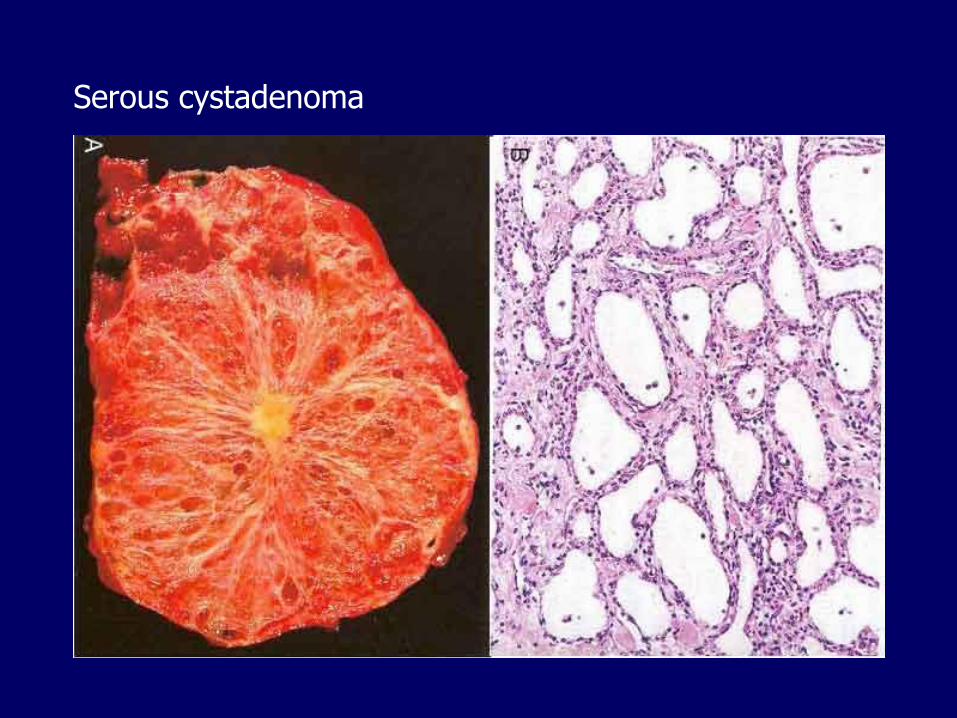
Serous cystadenoma
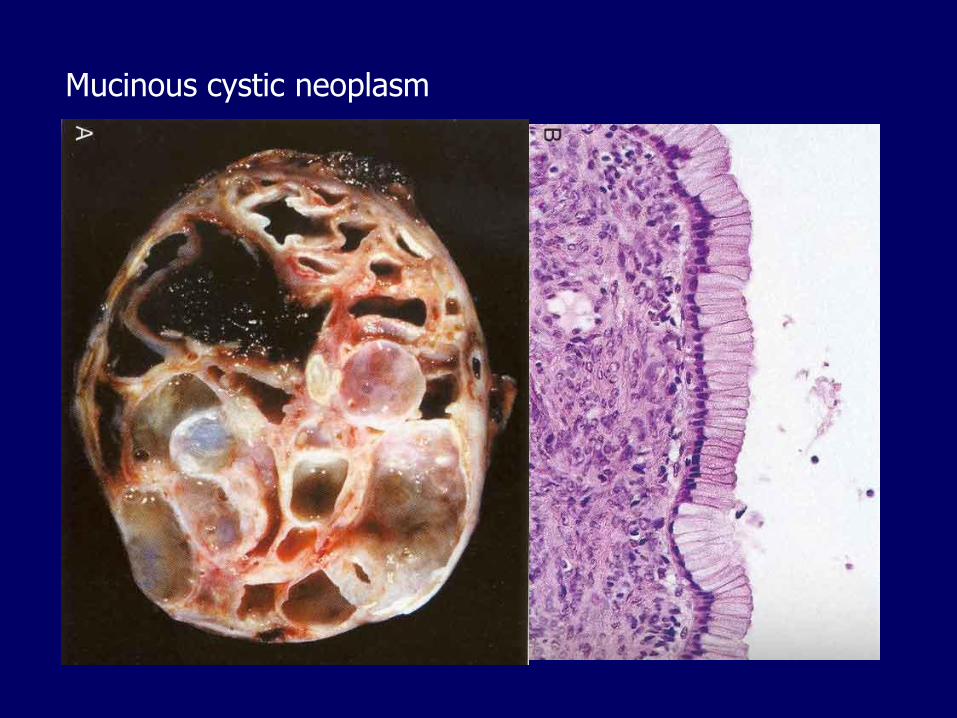
Mucinous cystic neoplasm
Arise almost exclusively in women
Macrocystic (few large cysts)
Thick, mucinous fluid
Tall columnar epithelium
Can be benign or malignant
Mucinous cystic neoplasm
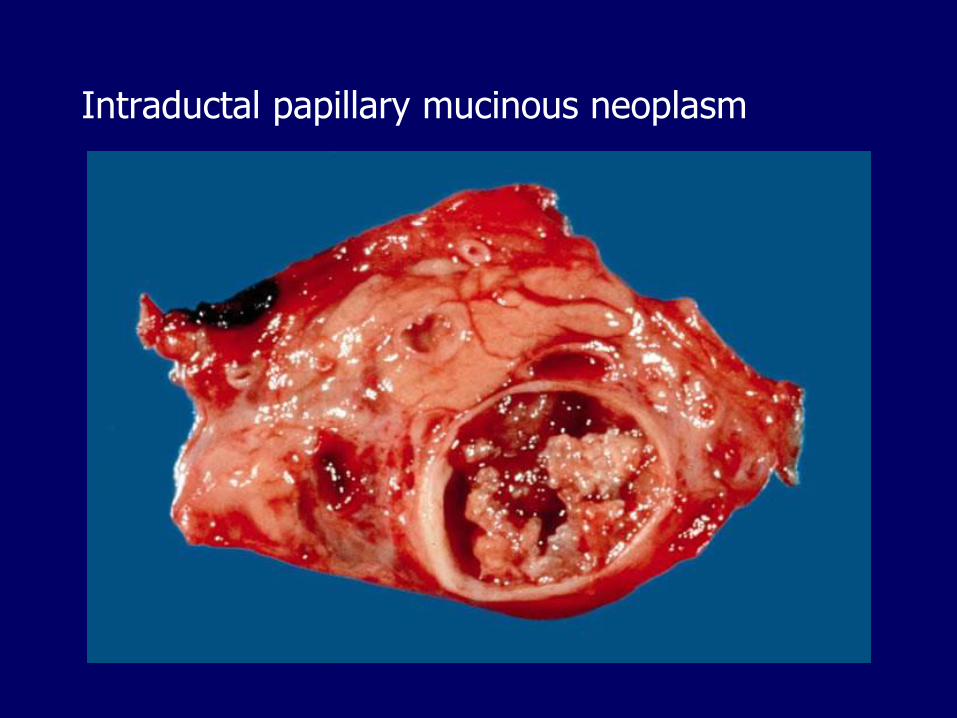
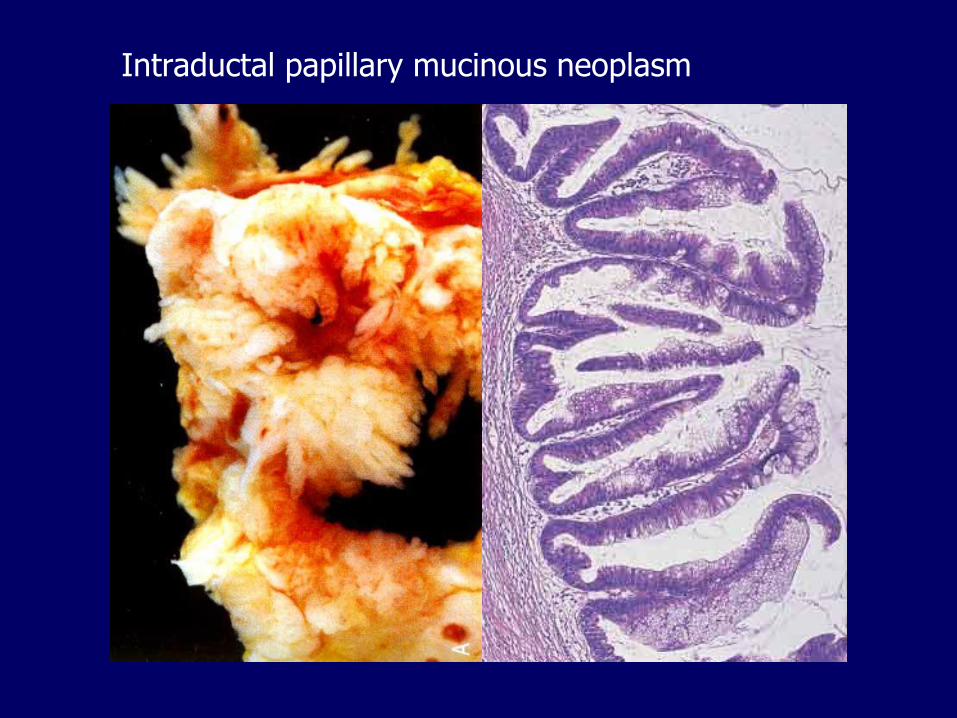
Intraductal papillary mucinous neoplasm
More common in men
Arise in the main pancreatic ducts
Intraductal proliferation of mucinous cells in papillary arrangements
Mucin accumulation leads to cystic dilatation
May be multifocal
Can be benign or malignant
Intraductal papillary mucinous neoplasm
Intraductal papillary mucinous neoplasm
Pancreas1. Congenital malformations
2. Pancreatitis
3. Pancreatic cystic neoplasms
4. Pancreatic ductal adenocarcinoma5. Pancreatic endocrine neoplasms
Pancreatic (ductal) adenocarcinoma
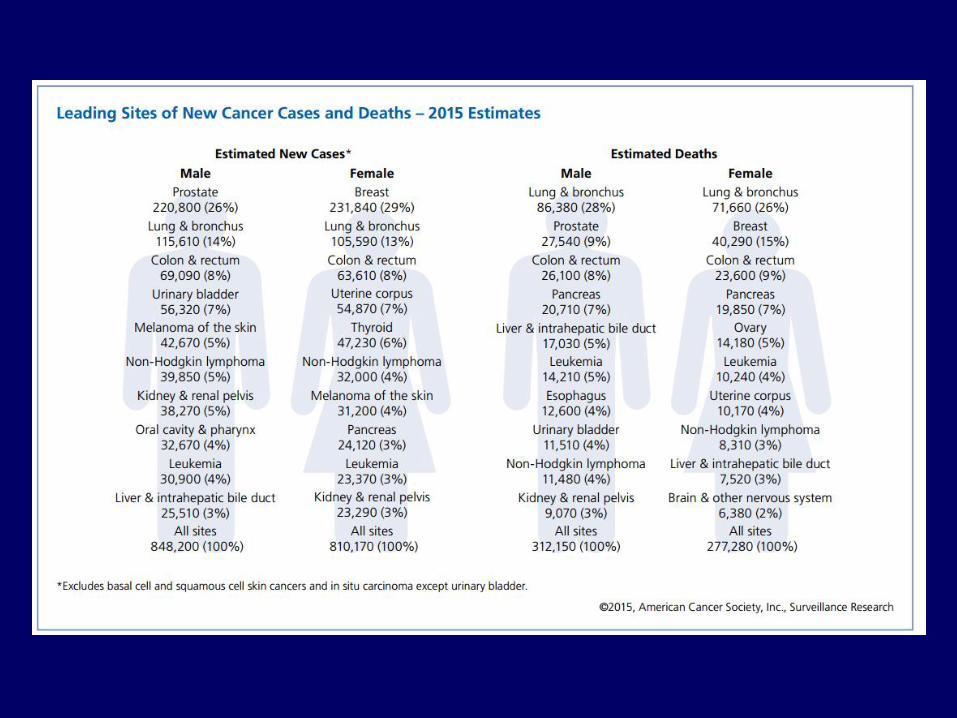
Incidence and mortality
– Greater in men than in women
– Greater in blacks than in whites
– Greater in Acadiana
5-year survival rate < 5%
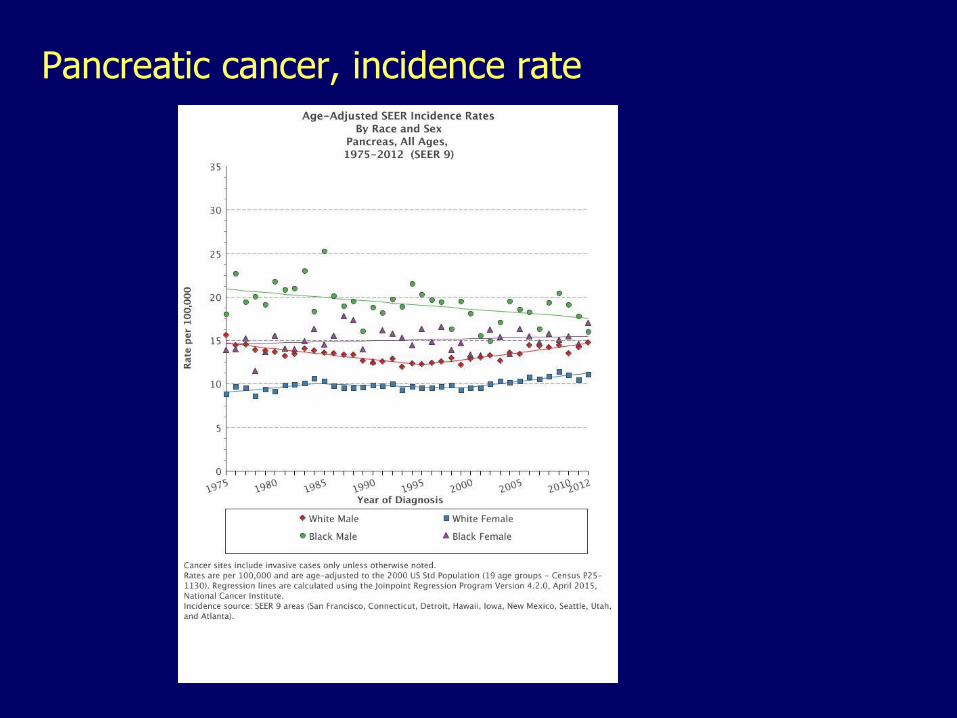
Pancreatic cancer, incidence rate
Pancreatic adenocarcinoma, risk factors
Smoking
High-protein, high-fat diets
Chronic pancreatitis, diabetes
Hereditary pancreatitis
Alcohol
Exposure to gasoline products, pesticides
Hereditary nonpolyposis colorectal cancer
BRCA2, hereditary breast and ovarian cancer
Peutz-Jeghers syndrome
p16 mutation, 95%
KRAS mutation, 80-90%
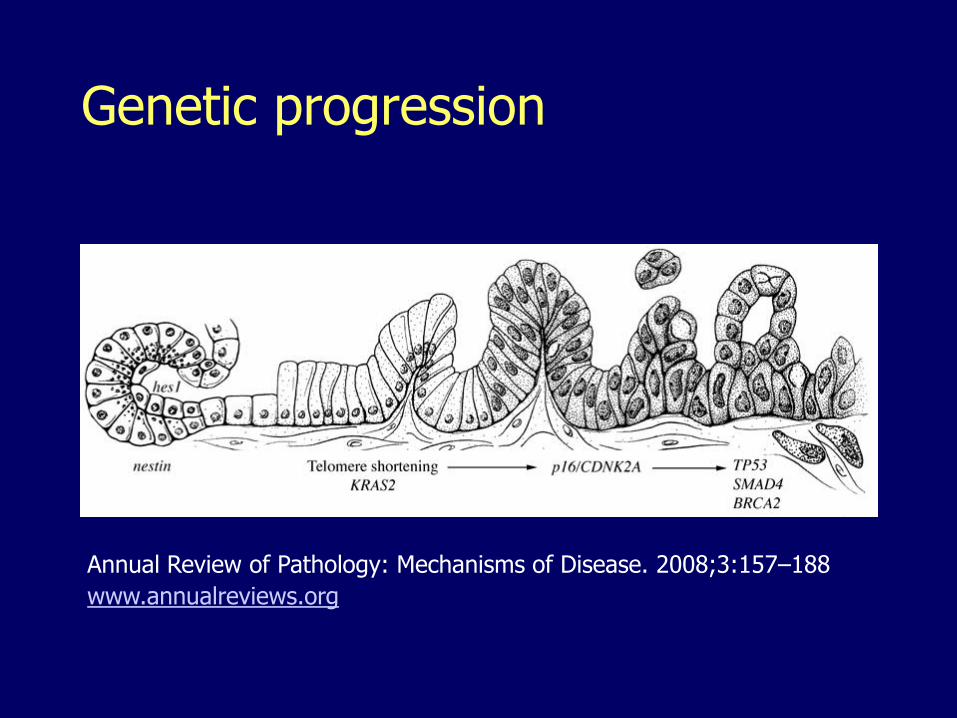
Genetic progression
Annual Review of Pathology: Mechanisms of Disease. 2008;3:157–188
www.annualreviews.org
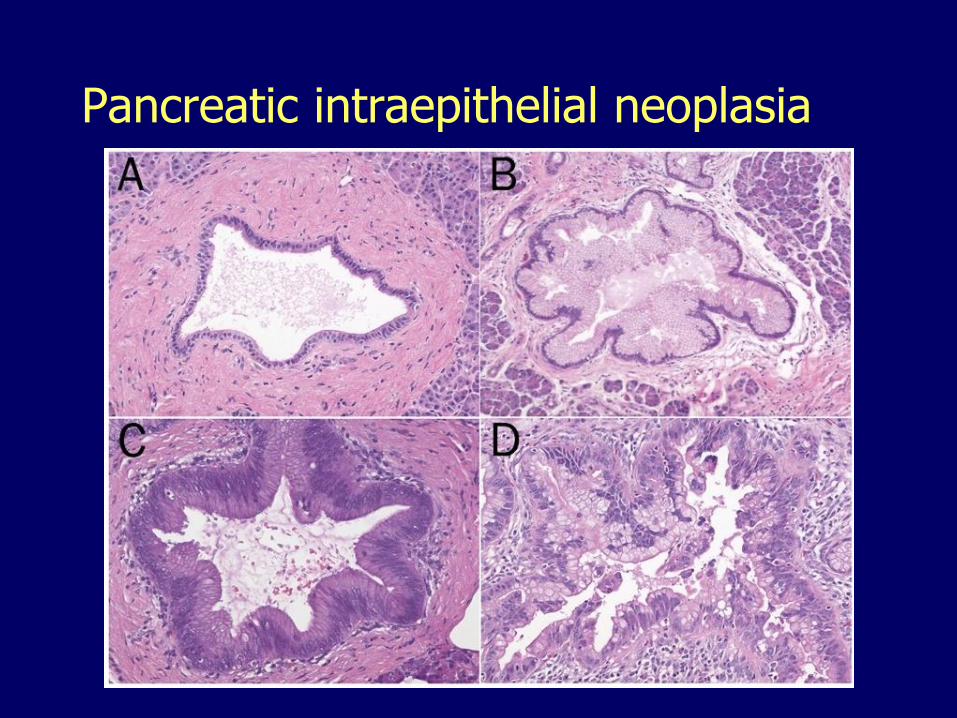
Pancreatic intraepithelial neoplasia
Pancreatic adenocarcinoma, morphology
Location:
– 60% arise in the head
– 20% diffusely
– 15% in the body
– 5% in the tail
Microscopically:
– High invasiveness (perineural invasion, lymphatic invasion)
– Desmoplastic (scirrhous, fibrous)
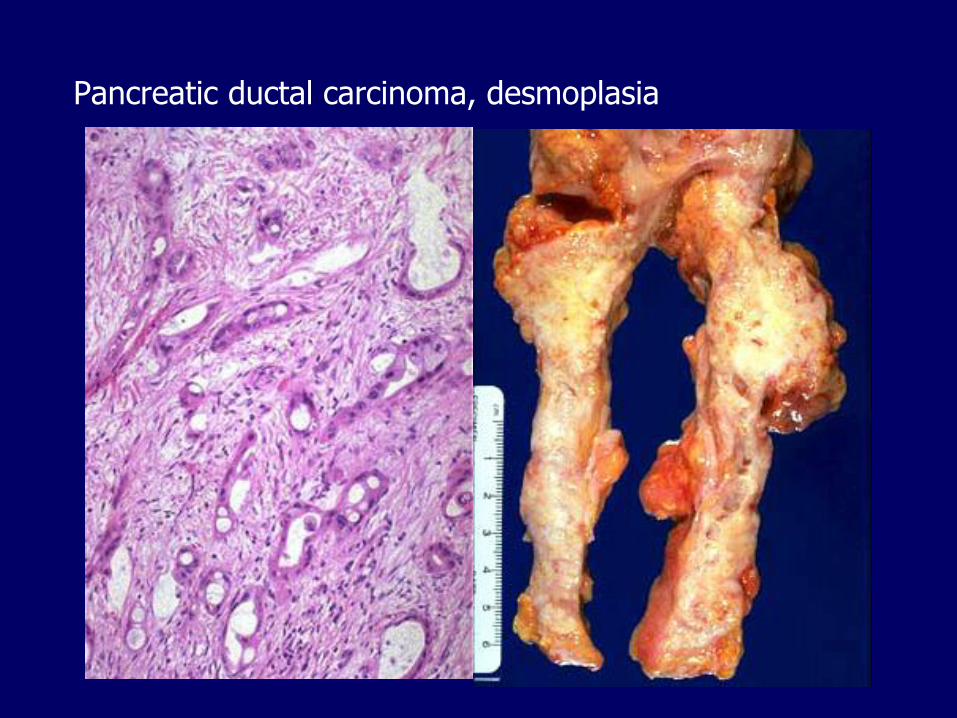
Pancreatic ductal carcinoma, desmoplasia
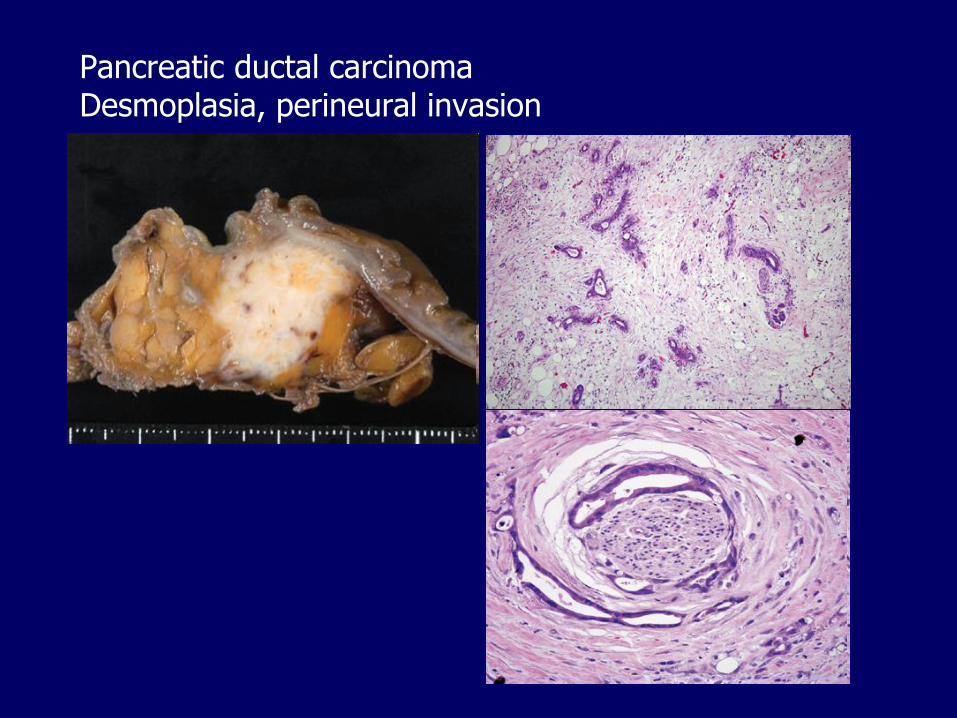
Pancreatic ductal carcinomaDesmoplasia, perineural invasion
Clinical findings
Pain
Obstructive jaundice, palpable non-tender gallbladder (Courvoisier’s sign)
Migratory thrombophlebitis (Trousseau sign)
– Tumor procoagulants
Tumor marker:
– CA19-9
Fewer than 20% are resectable
Pancreas1. Congenital malformations
2. Pancreatitis
3. Pancreatic cystic neoplasms
4. Pancreatic ductal adenocarcinoma
5. Pancreatic endocrine neoplasms
– Insulinoma
– Gastrinoma
– Glucagonoma
– Other
Pancreatic endocrine neoplasms
Only 2% of all pancreatic neoplasms May elaborate hormones
– Some are non-functional
Morphologically similar to carcinoids May be associated with MEN I syndrome,
hyperplasia or adenomas in:– Pancreatic islets– Adrenal cortex– Parathyroid– Pituitary
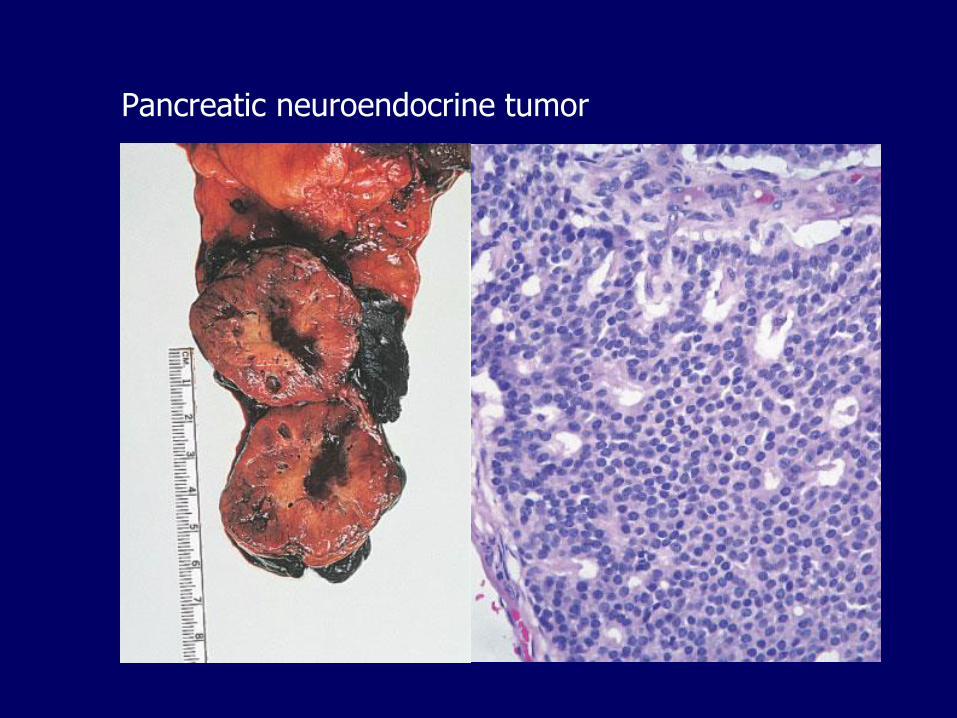
Pancreatic neuroendocrine tumor
Beta-cell tumors (insulinomas)
The most common type
May cause severe hypoglycemia
Whipple triad:
– Fatigue, confusion, stupor, coma, convulsions
– Glucose < 50 mg/dL
– Attacks precipitated by fasting/exercise and relieved by feeding/glucose
Usually small and encapsulated
Only about 10% metastasize
G-cell tumors (gastrinomas)
Located in the “gastrinoma triangle”: duodenum, pancreas and peripancreatic soft tissues
Zollinger-Ellison syndrome
– Hypergastrinemia
– Multiple peptic ulcers (gastric, duodenal, jejunal), unresponsive to therapy
– Diarrhea
Over half locally invasive or have metastasized at the time of diagnosis
Alpha-cell tumors (glucagonoma)
Cause the glucagonoma syndrome:
– Mild diabetes
– Necrolytic migratory erythema
– Deep vein thrombosis
– Anemia
– Tendency to develop overwhelming infections
Seen mostly perimenopausal and postmenopausal women
Approximately 50% have metastases at the time of diagnosis
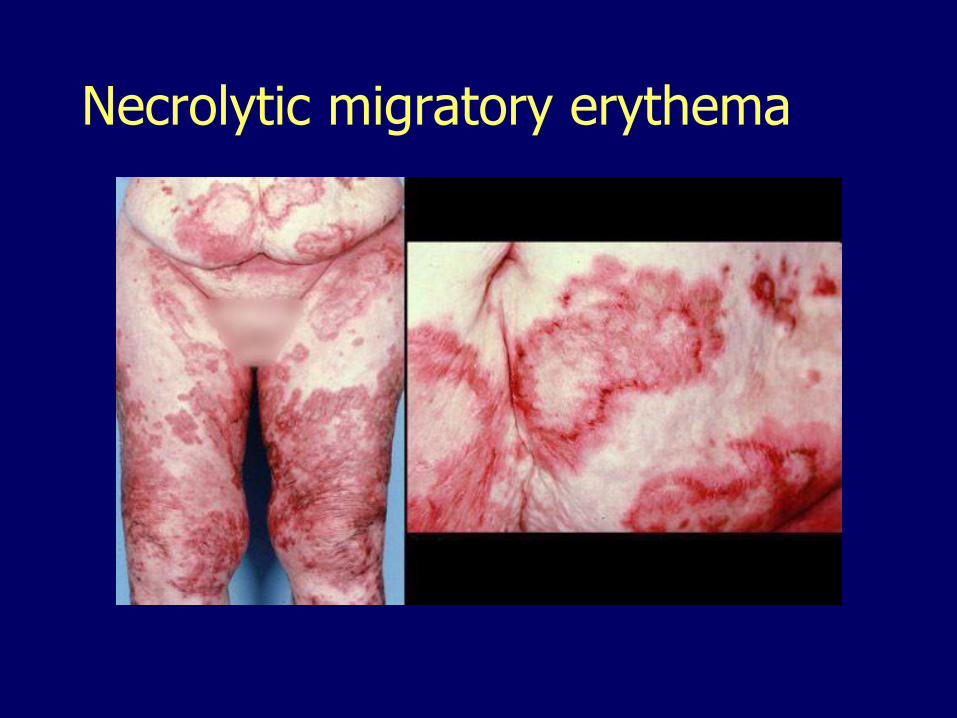
Necrolytic migratory erythema
Other endocrine neoplasms
Somatostatinoma (Delta-cell tumors), may present with diabetes
VIPomas (vasoactive intestinal peptide), may present with secretory diarrhea
Carcinoids
Tumors producing more than one hormone