Embed Size (px)
DESCRIPTION
Citation preview

Osteoid Osteoma

Index
IntroductionSpecial features IncidenceSites of predilectionSymptomsOther Clinical Features

Gross AppearanceMicroscopyRadiological findingsWhy relief with aspirin !!!!Differential DiagnosisTreatmentConclusion

Introduction
Osteoid osteomas are bone tumors less than 2 cm in greatest dimension and usually occur in patients in their teens and twenties.
In fact, 75% of patients are under age 25.
Osteoid osteomas can arise in any bone but have a predilection for the appendicular skeleton.

50% of cases involve the femur or tibia, where they commonly arise in the cortex.

Osteoid osteomas are painful lesions. The pain is caused by excess
prostaglandin E2 which is produced by the proliferating osteoblasts.
It characteristically occurs at night and is dramatically relieved by aspirin.

Special features
Failure to increase in size with time Spontaneous regression Replacement by scar tissue These features are unlike those of other benign tumors suggesting that the etiology still remains an enigma.

Incidence
10-11% of all benign bone tumors 2.5%-5% of all bone tumors First three decades of life Most common-second decade Most common-in men (2:1)

Sites of predilection
Diaphysis of femur and tibia Medial side of neck of femur Posterior elements of spine Humerus Phalanges of hand Fibula Talus Ribs Skull

Symptoms
Pain which has characteristic pattern described variously as sharp,dull,boring deep,or intense often worst at night and very frequently relieved by salicylates*(aspirin)
Limp Muscular atrophy due to disuse Swelling and warmth if it is
superficial

Adjacent joint stiffness Scoliosis In children overgrowth and angular
deformities Nerve root compression or cord
compression Point tenderness over the lesion

Gross Appearance
Cherry red to gray red tissue Overlying cortex distorted Reactive periosteal new bone
formation Nidus may vary from few mm to 1.5 cm in diameter. Surrounding reactive bone usually thick hard and extensive..

Microscopy
Numerous osteoblasts forming highly irregular trabeculae of osteoid and woven bone
Numerous osteoclasts Woven bone trabeculae variably
mineralized Calcification more near centre of lesion.

At times no calcification of nidus Surrounding bone shows reactive
bone formation which is lamellar bone in contrast to woven bone of nidus
Thin zone of fibrovascular tissue between nidus and reactive bone .

Radiological findings
Small to round to oval focus of decreased density called nidus .sometimes nidus also sclerotic.
Surrounding area of sclerosis which is normal reactive bone .

Lesions usually in diaphysis
Mostly cortical sometimes inside medullary canal or subperiosteally
Periosteal reaction when occurs is large but smooth in contrast to “codman triangle” of malignant lesions

Bone scan
Useful in detecting small lesions “Double density sign” which is a
focal area of increased activity with a second smaller area of increased uptake superimposed on it is said to be diagnostic.

CT scan and MRI
Sometimes required to localise the lesion accurately.

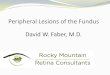
Osteoid osteoma. A lateral view (A) of the proximal tibia shows a very dense lesion in the posterior cortex. A darker central area contains a white nidus. This lesion in a 20-year-old man caused pain in this area, relieved by aspirin. B, A nuclear medicine bone scan in a different patient with an osteoid osteoma in the left lower tibia shows increased activity (arrows) at the site of the lesion.

Osteoid osteomas, especially those that arise beneath the periosteum, usually elicit a tremendous amount of reactive bone formation that encircles the lesion. The actual tumor, known as the nidus, manifests radiographically as a small round lucency that is variably mineralized
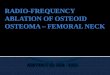
Specimen radiograph of intracortical osteoid osteoma. The round radiolucency with central mineralization represents the lesion and is surrounded by abundant reactive bone that has massively thickened the cortex.

Why relief with aspirin !!!!
High levels of prostaglandins present in osteoid osteoma which mediate pain receptor pathway
Aspirin (salicylates) act as prostaglandin synthetase inhibitors

Differential Diagnosis
Osteoblastoma Osteosarcoma Eosinophilic Granuloma Ewings Sarcoma Brodie’s Abscess Stress Fractures

Treatment
Surgical removal of lesion To relieve pain.secondary
manifestations like synovitis ,scoliosis, nerve root compression

Principle of surgery
Necessary to remove the “NIDAL” tissue

Surgical options
Block resection of the nidus Increases risk of subsequent # if
lesion is in cortical bone Alternative method is to shave the
reactive bone with sharp osteotome until the nidus is exposed ,then curette the exposed nidus

Intraoperative localization of nidus possible with pre operatively injected technetium labelled methylene diphosphonate and sterile wrapped geigercounter.
Intraoperative xrays of excised specimen to document complete removal of nidus

Excision of nidus using CT assisted localization
K-wire inserted into the nidus
Biopsy punch inserted over k-wire
Percutaneous CT guided resection using a trephine 2mm larger then the lesion to ensure complete removal.

Radiofrequency ablation
Done percutaneously Initial core needle biopsy after which
radiofrequency electrode is inserted through cannula of biopsy needle
Temperature at the tip raised to 90 degrees centigrade for 6 minutes
Results:claim to be equivalent to surgical excision
Used only in extraspinal lesions that are away from neurovascular structures

Conclusion Osteoid osteomas’ are considered
benign and are normally treated by conservative surgery. However there is a possibility of malignant transformation. This is rare except when treated with radiation, which promotes this complication.