Embed Size (px)
Citation preview

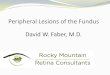
Dr. HARSH AMIN

Osteomas of skull are slowly growing benign tumors of membranous bone
often arising in the calvaria or paranasal sinuses.
Osteomas are the most common primary benign tumors of the calvaria, affecting 0.4% of the general population. They have an incidence approaching 5%, when small intracranial (dural and falcine) osteomas found at autopsy are included.
These benign tumors are typically solitary round lesions composed of dense cortical hyperostosis, usually no larger than 2 cm in diameter.
Multiple osteomas may occur with multiple colonic polyps in Gardner`s syndrome.
INTRODUCTION

Osteomas are found more commonly in the sinuses than over the calvarialvault.
The frontal sinus is the most frequent site of an osteoma, followed in order of frequency by the ethmoid, sphenoid, and maxillary sinuses. Osteomas also occur in the mandible and the orbit but are less frequent.
These benign lesions are usually first identified in adult life, with a peak age of discovery in the 30`s and 40`s.
They occur more often in females than in males (2:1).

They are most often asymptomatic masses found incidentally.
When an osteoma grows as an expansile mass in a sinus cavity, it may produce symptoms related to sinus obstruction, infection, or mass effect on the adjacent structures.
Occasionally they can expand and perforate through the sinus wall into the skull. They have been encountered as a cause of pneumocephalus.
A palpable protrusion or cosmetic deformity may occur if a calvarial osteoma is large.
Osteomas of the oral cavity frequently cause malocclusion or dysphagia as an important complaint.
Orbital osteomas can present with proptosis or double vision.
CLINICAL FEATURES

The radiographic study and the CT scan presentation of an osteoma are
usually diagnostic.
Typically, these imaging studies will demonstrate an eburnated (ivory-like) smooth round mass of bone arising from the periosteum of the outer table of the skull or within a sinus cavity.
This mass may be relatively flat and broad - based against the host bone, or may form a round, pedunculated ¨polyp¨ of bone attached to the calvaria by a narrow stalk.
INVESTIGATION


Surgical approaches

Supracilliary Approach

The supraciliary approach is usually chosen in patients
with small sinuses or small osteomas involving anterior table and solitary osteomas.The supracilliary approach may not give good aesthetic results and recurrence rates are relatively high.
Supracilliary Approach

Endonasal Approach(in case of paranasal sinus osteoma)

The indications for endoscopic endonasal approach are
limited to small osteomas of the posterior wall of the frontal sinus located close to the infundibulum. The reported postoperative complications of this approach have been ptosis, diplopia, supraorbital anesthesia, and rhinoliquoral fistula.
Endonasal Approach(in case of paranasal sinus osteoma)

Direct Approach

The direct approach is limited to small and solitary
osteoma.It has advantage of less extensive dissection but it gives visible scar.
Direct Approach

Bicoronal Approach

Bicoronal Approach

The indications for bicoronal approach are frontal
osteomas located at the anterior wall or laterally, very large tumors.
This approach is very helpful in case of multiple osteomas, but have disadvantage of extensive dissection.
This approach requires good hair density
Bicoronal Approach

No treatment is required for asymptomatic lesions.
Complete surgical excision is required for symptomatic relief, cosmetic reasons, cranial nerve decompression or any other complications.
The choice of the operative approach and extent of the osteotomy depend on the site of neoplasm, dimension of the neoplasm, involvement of posterior table, and density of hairs on scalp.
Detailed CT examination can provide precise information about the origin, dimension, and localization of frontal osteoma; skull CT (axial and coronal views) is mandatory for surgical planning.

Details of our case
A 10 year-old girl, has come to us with complain of swelling in lateral aspect of right eyebrow as well as second swelling at hairline on right side as shown which they noticed first when she was 4 years old . Swelling is growing slowly with age with no other complains.
On examination there was 3x3 cm right supraorbital and 1x1 cm swelling at right fronto-temporal region at hairline which was hard in consistancy.
On CT Scan homogeneously dense broad – based swelling found to involve the outer table only.

As patient was a young girl, parents were very much concerned about post operative scar.
The present report describes the results of a bicoronal approach in terms of radical excision of a large frontal osteoma to ensure no long term recurrence and good cosmetic results.
Treatment

In our case, choice of the bicoronal approach was made after carefully evaluating the location and the dimension of the tumor and the good hair growth of the patient.
We avoided the classic supra cilliary approach for swelling at right lateral brow and direct approach for swelling at hairline , which does not provide an adequate exposure of the operative field and therefore does not allow complete excision of large osteomas.
Moreover, high recurrence rates have been described with these techniques, and good aesthetic results were not obtained.
Bicoronal approach which we took provided an excellent surgical exposure, allowing the complete excision of the neoplasm limiting the postoperative complications, reducing the recurrence rates and giving an ideal aesthetic result.

Pre and Post operative photographs

Under general anesthesia we took a bicoronal approach with a subgaleal flap up to the superior orbital rim and put inverted U-shaped incision on the periosteum of both osteomas, Periosteum elevated and bone was chiseled with removal of involved outer table and contour of bone smoothened with burr and matched with surrounding bone.
On the 10th postoperative day, all stitches were removed.
A postoperative CT scan of the skull confirmed the radical excision of the tumor.
The patient did not have periorbital headache or contour deformity and the aesthetic result was excellent
Serial clinical evaluation once a month for first 3 months and then once in 3 month for next 1 year which showed no recurrence

THANK YOU




![Peripheral osteoma of the mandibular crest: a short case study · Osteoma is a benign osseous lesion characterized by the proliferation of cancellous and/or cortical bone [1]. It](https://img.pdfslide.us/doc/110x75/5fcec12c32d22e4f667c7367/peripheral-osteoma-of-the-mandibular-crest-a-short-case-study-osteoma-is-a-benign.jpg)






















