Embed Size (px)
DESCRIPTION
Male genital trauma
Citation preview

MALE GENITAL TRAUMA
Amy McAllister
April 2014

Contents
Anatomical approach Causes Symptoms & Signs Investigations Management Learning points

Introduction
GUT injury in ~10% of all trauma patients
Long term morbidity
-incontinence
-impotence
-psychological Usually not life threatening; need to rule
out other injuries

Aetiology Penetrating
- Knife, bullet Blunt
- MVA
- fall from height
- direct blow/ sports
- straddle injury
- Constriction, Instrumentation Also – avulsion, burns, radiation, iatrogenic

Penile injuries
Penile “fracture” Rupture of the tunica albuginea of one
or both of the corpora cavernosa.

Penile fracture Aetiolgy
- Frequently a sexually related accident but can also be from a direct blow
- May be associated with urethral injury
Investigations
- Usually history is enough
- Diagnostic cavernosography or MRI
Management
- Previous conservative treatment – high complication rates
- Surgery

Penile fracture
“Eggplant” deformityFascial layers of the penis

Penile amputation
Accidental or deliberate “Double Bag” preservation
Management Reimplantation - success has been
reported after 16 hours of cold ischaemia

Penile soft tissue injuries
Penetrating injuries Dog bites Constriction Degloving
Management Sutures Removal of constricting devices Surgery

Testicular injuries•Haematocele
•Haematoma
•Testicular rupture
•Testicular dislocation/ torsion

Testicular injuries
Signs Bruising, swelling, tenderness,
haematuria
Investigation USS Surgical exploration

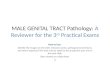
Testicular rupture
Normal testis Testicular rupture(6)

Urethral injuriesProstatic
Membranous
Bulbous
Pendulous
Anterior urethra
Posterior urethra (most common)

Posterior urethral injury
Commonly associated with pelvic # Violent mechanism

Posterior urethral injury
Signs
Blood at meatusGross haematuriaInability to voidEcchymoses, swelling of penisPelvic/suprapubic tenderness“High riding”/absent prostate on DRE

Anterior urethral injury
Direct trauma history Straddle injury Usually no pelvic # Similar signs to
posterior
Investigations Urinalysis Retrograde
urethrogram

Urinalysis
*False positives* Rhabdomyolysis Food – berries/beets Drugs – Rifampicin, Alphamethyldopa
etc
If more than a trace on dipstick – send for urinalysis

Retrograde urethrogram Patient tilted at 45 degrees Initial KUB film taken Penis sretched obliquely
over thigh to promote visualization of the entire urethra
Inject 25mls of water-soluble contrast using specialised adaptor or Foley catheter
Re-xray

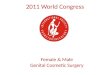
Goldman classification of urethral trauma

Retrograde urethrogram
Normal Goldman type III urethral injury

Urethral injuries Management
Posterior Partial tear - Foley catheter Complete tear – Suprapubic catheter, surgery
Anterior - surgery
NB. If Foley already in place and suspect tear, do not remove

Bladder injuries
Degree of injury
•Contusion (most common) •Extraperitoneal rupture•Intraperitoneal rupture•Combined intraperitoneal/extraperitoneal rupture

Bladder injuries Aetiology
- pelvic # in up to 70% of cases
- blunt abdominal trauma with full bladder

Bladder rupture

Bladder injuriesSigns Gross haematuria Microscopic haematuria with pelvic # Bruising, suprapubic tenderness, peritonism Must rule out urethral injury before placing Foley
Investigations Retrograde CT cystography
Management Contusions/extraperitoneal – conservative Intraperitoneal - surgery

Ureteral injuries
Ureter injury is rare except a complication of surgery/ penetrating trauma
No haematuria in 25% of ureter injuries Have high index of suspicion

Renal injuries
Usually blunt trauma Sudden deceleration MVA / bicycle accidents
Lumbar transverse process #

Renal injuriesSigns
• Eccyhmosis to back / flank / lower thorax / upper abdomen
• Haematuria• Shock
Delayed findings
•Fever•Palpable flank mass (urinoma)

Renal injuries
Investigations
CT with contrast IVP

Classification of renal injuries

Renal injuries
Management
ABCs Grade I and II – conservative Grade III and up – operative including
nephrectomy

Learning points
Rule out life threatening injuries first Identification prevents long term
problems No Foley if urethral trauma suspected –
wait for u/a and pelvic x-ray If Foley is in – do not remove if urethral
trauma suspected afterwards Gross haematuria or microscopic
haematuria plus shock = GUT trauma

References (1) Urol Clin North Am. 2013 Aug;40(3):323-34. doi:
10.1016/j.ucl.2013.04.001. Epub 2013 Jun 12.Current epidemiology of genitourinary trauma. McGeady JB1, Breyer BN
(2) Bhatt S, Kocakoc E, Rubens DJ, Seftel AD, Dogra VS (2005)Sonographic evaluation of penile trauma. J Ultrasound Med 24:993–1000, quiz 1001
(3) Kozacioglu Z., Degirmenci T., Arslan M., et al : Long-term significance of the number of hours until surgical repair of
penile fractures. Urol Int 2011; 87: 75-79 CrossRef (4) J Urol. 2004 Aug;172(2):576-9. Long-term experience with surgical and conservative treatment of
penile fracture. Muentener M1, Suter S, Hauri D, Sulser T. (5) Wei F.C., McKee N.H., Huerta F.J., et al : Microsurgical replantation of a completely amputated penis. Ann Plast
Surg 1983; 20: 317-321 CrossRef

References (6) Bhandary P, Abbitt PL, Watson L (1992) Ultrasound
diagnosis of traumatic testicular rupture. J Clin Ultrasound 20:346–348
(7) Lower male genitourinary trauma: a pictorial review Bruce E. Lehnert & Claudia Sadro & Eric Monroe &Mariam Moshiri
(8)Gomez RG, Ceballos L, CoburnMet al (2004) Consensus statement
on bladder injuries. BJU Int 94:27–32(2)Ramchandani P, Buckler PM (2009) Imaging of genitourinary trauma. AJR Am J Roentgenol 192:1514–1523
(9) Straddle injuries to the bulbar urethra: management and outcome in 53 patients Elgammal MA.Int Braz J Urol. 2009 Jul-Aug;35(4):450-8. .