Embed Size (px)
DESCRIPTION
KERATOCONUS
Citation preview

Dr. Christina

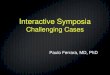
Progressive disorder in which the cornea assumes a conical shape secondary to corneal thinning and protrusion
Onset is around puberty- progresses untill 3rd or 4th decades of life
Both eyes affected usually Role of hereditary transmission is not
clear.

PRESENTATION
Presents usually during puberty. Impairment of vision due to
progressive myopia and irregular astigmatism.
Asymmetrical nature. Approximately 50% of normal fellow
eyes will progress to keratoconus within16 years.


DIAGNOSIS
Central or paracentral stromal thinning, apical protrusion and irregular astigmatism
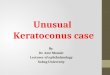
SIGNS: Direct ophthalmoscopy shows ‘oil
droplet sign’. Retinoscopy shows irregular’ scissor’
reflex’ Slit lamp microscopy showsfine,
vertical, deep stromal striae called vogts striae .

Epithelial iron deposits may surround the base of cone –’fleischer ring’.
Marked irregular myopic astigmatism with steep keratometry reading.
Bulging of the lower lid in down gaze- ‘munson sign’.
Corneal topography – sensitive method of detecting early keratoconus.

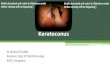
ACUTE HYDOPS
Caused by rupture of descemets membrane that allows influx of aqueous into the conea.
Causes sudden drop in visual acuity with discomfort and watering.
Usually the break heals within 6-10 weeks and edema clears but scarring results
Treatment is keratoplasty after edema resolves.


ASSOCIATIONS
SYSTEMIC DISORDERS LIKE Down, Turner, Ehler-Danlos and Marfan syndromes, atopy, oesteogenesis imperfecta, MVP, mental retardation.
OCULAR DISORDERS like vernal kerato conjunctivitis, blue sclera, aniridia, ectopia lentis, RP

TREATMENT
Spectacles in early stages. Rigid contact lenses for higher
degrees of irregular astigmatism..Piggy back lenses.
Keratoplasty : both lamellar and penetrating keratoplasty especially in cases of severe corneal scarring.

THANK YOU