Embed Size (px)
DESCRIPTION
Improving end of life care in chronic obstructive pulmonary disease (COPD): testing the case for change
Citation preview

Improving end of life care inchronic obstructive pulmonarydisease (COPD): testing thecase for change
NHS Improvement - Lung: NationalImprovement Projects
NHSNHS Improvement
Lung
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE


Introduction
Key Learning
Section 1-3: Case studies
One - Breathing Space, Rotherham
Two - Solihull Community NHS Care Trust
Three - Hartlepool Primary Care NHS Trust
Acknowledgments
References
Contents
NHS Improvement - Lung National Improvement Projects -Improving end of life care in chronic obstructive pulmonarydisease (COPD): testing the case for change
4
6
9
13
15
17
18
3Contents

Introduction4
Introduction
National position and workstreamcontext
Around half a million people dieevery year in England. The end of life isinevitably something everyone must face,but it is perhaps the most difficult andsensitive issue within society today. Evenfor healthcare professionals it is widelyacknowledged that it can represent oneof the most challenging clinical areas inwhich to specialise.
In 2008, the Department of Healthpublished the End of Life Care Strategyin response to the significant variation inservice provision across the country. Ithighlighted the need for the NHS andsocial care services to provide holistic,high-quality care for all adults at the endof life, and their families and carers, andadvocated the value of supported carepathways to help make this a reality. Carepathways have been successfullydeveloped for a number of potentiallyterminal illnesses, such as dementia, heartdisease and stroke, and should now beevolved for chronic obstructive pulmonarydisease (COPD) which accounts foraround 23,000 deaths a year.
Currently, less than 50% of clinicalservices for COPD in the NHS have aformal arrangement for users of theseservices to gain access to specialist end oflife care. In order to meet this challenge,clinical staff must ensure that COPD isrecognised as a cause of death amongstpatients. It is also vital to give people theopportunity, and to help them to plan fortheir future care. In conjunction with this,commissioners and providers shouldensure access to end of life care services,in line with care provided to those withother life threatening illnesses such ascancer.
The projects in the NHS Improvement -Lung End of Life Care workstream are amajor step towards achieving these aims.They represent a wide variety of clinicalstaff who are focused on addressing thekey issues of: prognostic indication,Advance Care Planning and palliative care registers.
The following sections in this documentdescribe each of the NHS Improvement -Lung sites, aims, objectives and detailsthe learning and progress that hasemerged.
Summary of site projects
There were three End of Lifeimprovement projects running in thefollowing organisations:
• Solihull Community NHS Care Trust (West Midlands)
• Hartlepool Primary Care NHS Trust (North East)
• Breathing Space, Rotherham Primary Care NHS Trust (Yorkshire and the Humber).
Summary of key learning
The key learning (see next sectionfor more details) is centred on thefollowing themes:
Prognostic indicators – Sites weretesting two different indicators; theGold Standards FrameworkIndicators and the BOD (Body MassIndex, Obstruction, Dyspnoea score)which is an abbreviated form of theBODE index (Body Mass Index,Obstruction, Dyspnoea and Exercise– Celli et al, 2004). Evidencesuggests there was variability in thereliability and validity of usingindicators to accurately predict thelast six to 12 months of life.
Advance Care Planning – Givingpeople the opportunity to discusstheir wishes around issues such asresuscitation and representation onloss of capacity is important andshould be undertaken when thepatient is as well as possible.
There is a plethora of publishedpatient information available toclinical staff to aid them in theirdiscussions with patients but staffconfidence around advancedcommunication skills was very low.There is a considerable variationbetween the training which cancerclinicians receive and which isavailable for staff managing patientswith a long-term condition.
Raising awareness – The issue ofdeath and dying is a sensitive topicbut lack of awareness amongstpatients and more surprisinglyamongst staff about the potentiallylife threatening nature of thecondition impacts on the care COPDpatients receive in the final stages oflife.
The tendency to continue withproactive management of symptomsand maintain a positive prognosismeans seriously ill patients are at riskof not being able to plan ahead atthe right time with fullunderstanding of their condition.
End of life registers – Currently,palliative care Quality OutcomesFramework (QOF) registers areutilised in GP practices to identifythose people approaching the end oflife, thereby helping ensure that theirneeds are met. However, they aregenerally incomplete and biasedtowards the care of those withcancer.

5Introduction
The Department of Health End ofLife Care Strategy (2008) advocatedthe development of ‘End of Life CareLocality Registers’ as a means tosupport the provision of high qualitycoordinated care and to address theshortcomings in the current practiceregisters. The locality registers areelectronic records containingimportant details about careprovision and the preferences ofpatients identified as being at theend of life. This information can bethen easily accessed by all healthcareprofessionals that the patient comesinto contact with. Key to theeffective implementation of a localityregister is ensuring effectivemechanisms are in place to identifyall patients approaching the end oflife, whether this be a GP, a memberof the community team, or otherhealth and social care professional,and ensuring that effectiveeducation and training is in place forall the relevant professionals aroundidentification, communication andadvance care planning. Anevaluation of the pilots undertakenby Ipsos MORI is available at:www.endoflifecareforadults.nhs.uk/publications/localities-registers-report
together across boundaries to spot theopportunities and manage the change.And third, to act now, for the long term.
The ambition is to achieve efficiencysavings of up to £20 billion forreinvestment over the next four years.This represents a very significantchallenge to be delivered through thedetailed work the NHS has alreadyundertaken on Quality, InnovationProductivity and Prevention (QIPP) and theadditional opportunities presented in theEquity and Excellence: Liberating theNHS.
Many of the measures outlined in thisdocument are designed to support theNHS to meet the QIPP challenge, eitherby identifying where resources might bereleased or by improving understandingof the key interventions that havegreatest effect.
Considerations for future working
All the projects within this work streamhave been building the evidence for thecreation of a gold standard pathway forCOPD end of life patients but it isapparent that more work is still needed.
There is limited evidence over the validityand reliability of different types ofprognostic indicator and this should formthe basis for future work to addressdominance of certain indicators overothers and at what point in the patienttrajectory they should be used.The use of Advance Care Planning at theappropriate time has yielded positivefeedback from patients and carerstherefore it is hoped that adoption andspread throughout other parts of thecountry may occur.
Finally, it is hoped that this work willprovide an enhanced recognition ofCOPD across the medical community as aserious and invariably life-threateningdisease to ensure healthcare professionalsstart having discussions with peopleabout their wishes at end of life. This willensure patients receive care appropriateto their specific needs.
Hannah WallNational Improvement Lead,NHS Improvement – Lung
Phil DuncanDirector, NHS Improvement -Lung
Quality, Innovation, Productivity and Prevention (QIPP)
Demand for healthcare is increasing andthere are areas where we could increasethe quality, efficiency and value formoney of services as well as improvingoutcomes for people with COPD. Threethings need to be determined to makethis possible. First, improving qualitywhilst improving productivity, usinginnovation and prevention to drive andconnect them. Second, having localclinicians and managers working

6 Key learning
The end of life care pathway whichfeatures in the Department of Health Endof Life Strategy (2008) contains all thecomponents of a gold standard approachto care and is the model against whichNHS organisations should aim to plantheir services.
End of life care in chronic obstructivepulmonary disease (COPD) is a complexprocess but good care is essential asnearly 23,000 deaths occur each yearfrom the disease which is approximately5% of all deaths.
The three projects within the end of lifecare workstream have focused on testingkey elements of this pathway and toexamine what a pathway adaptedspecifically for patients with COPD mightbegin to look like.
Key learning
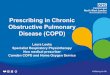
Prognostic indicatorsCentral to commissioning a high quality,cost effective service is a betterunderstanding of the end of life phase ofCOPD and one of the most challengingareas within this is the patient trajectory.
In malignant diseases, such as cancer, it iseasier to predict the rate of deteriorationand the amount of time which thepatient may have left to live because ofthe nature of the condition and gradualworsening of symptoms.
In COPD, the steady downward decline isreplaced with a relatively unpredictableseries of stable periods dispersed withtroughs. The troughs represent an acuteexacerbation (attack of breathlessness)from which the patient may recover backto a relatively good degree of health.
There can be many such exacerbationsduring the more severe stages of thedisease and this make prognosisextremely difficult.
End of Life Care Pathway (End of Life Care Strategy)
What could this like for COPD specific patients?
Trajectory of malignant disease
Trajectory of COPD
100
80
60
40
20
0Time >
Fun
ctio
n %
100
80
60
40
20
0Time >
Fun
ctio
n %
Death
Death
Discussionsas the endof lifeapproaches
Assessmentcareplanningand review
Coordinationof care
Delivery ofhigh qualityservices indifferentsettings
Care in thelast daysof life
Care afterdeath
PrognosticIndication
Advance CarePlanning(PreferredPriorities ofCare,resuscitation,AdvanceDecisions)
End of LifeCare GPPracticeRegisters
Acute/CommunityPalliativeCare Teams
LiverpoolCare PathwayAchievementof PreferredPriorities ofCare
Support forCarers
INFORMATION
Understandably, clinicians do not wish toinitiate end of life care until it becomesentirely appropriate but equally want togive patients realistic information on theseverity of their condition and time toplan ahead.

7Key learning
There are several sets of prognosticindicators which are in use at present.The most prolific is the Gold StandardsFramework indicators for COPD andcurrent guidelines recommend thatpatients who exhibit one or more of thefollowing symptoms may be entering theend of life stage.
Another indicator widely used is theBODE index (Celli et al, 2004) which takesa score from a collection ofmeasurements (Body Mass Index, FEV1obstruction, MRC dyspnoea score andexercise). Alternatively many clinicians useevidence based judgments to determinewhen the threshold is reached. However,the validity of all these indicators and theevidence of their effectiveness are still inthe process of being gathered.
Two workstream projects lookedspecifically at the use of prognosticindicators. Breathing Space in Rotherhamassessed the Gold Standards Frameworkindicators with patients on admission andthose outpatients attending pulmonaryrehabilitation to determine how manyindicators may be present and how thismay relate to time until death. Learningin the project suggested that overall atleast three were needed to accuratelypredict when the initial discussion waswarranted. The findings support this as itwas witnessed from the 83 patientdeaths which occurred during the project18 had three or more indicators presentat the time of death.
In contrast Hartlepool Primary Care NHSTrust used an adaptation of BODE whichwas the ‘BOD’ score. From data analysedthe project lead discovered that BOD maybe a predictor for the very early stages ofdecline amongst patients – perhaps thosewith more than the traditional six to 12month timescale which normally definesthe end of life. This may be extremelyimportant learning as it may signal aphase where changing interventions areconsidered and regular reviews may needto become more frequent in order tomaintain stability in disease control andslow the rate of disease progression.
Two of the sites (Solihull Community NHSCare Trust and Breathing Space) alsotested use of the ‘surprise’ question,which basically asks the clinician toconsider whether they would be surprisedif the patient was still alive in 12 monthstime. Both sites felt this very simple toolto be highly effective as a predictor ofdeath and both advocated its accuracy ason a par with or above the more formalprognostic indicators they tested.
Advanced Care Planning A key component of any end of life careservice, regardless of disease, is that ofAdvanced Care Planning. This is wherethe patient is given the opportunity todocument future wishes on a number ofareas such as:
• Their Preferred Priorities of Care e.g. their chosen place of death
• Their views on resuscitation and treatment through the use of an advance decision and do not attempt resuscitation documentation
• Who they would like to appoint in the event they loose capacity e.g. a Lasting Power of Attorney.
The use of supplementary writteninformation to aid clinicians when havingthese discussions with patients is usefulbut selecting which information to use,when to use it and how much to use is acomplex and sensitive area which requirescareful judgement on the part of theclinician involved.
The project sites found there was noshortage of available information theywere able to use or adapt. Some of thepopular choices included informationproduced by: the National End of LifeCare Programme, the National Councilfor Palliative Care, The Whittington NHSFoundation Trust, St Christopher’sHospice and the British Lung Foundation.Breathing Space in Rotherham weretrialling the British Lung Foundationliterature but have decided that ultimatelythey would like to produce their ownliterature which has information patientscan add to depending on their needs andhow much information they feel theywould like.
• Disease assessed to be severe e.g. (FEV1 <30% predicted – with caveats about quality of testing)
• Recurrent hospital admission (>3 admissions in 12 months for COPD exacerbations)
• Fulfils Long Term Oxygen Therapy Criteria
• MRC grade 4/5 – shortness of breath after 100 meters on the level or confined to house through breathlessness
• Signs and symptoms of right heart failure
• Combination of other factors e.g. anorexia, previous ITU/NIV/resistant organism, depression
• >6 weeks of systemic steroids for COPD in the preceding 12 months.
Gold Standards Framework PrognosticIndicator Guidance

8 Key learning
Some sites have found that there arepatients who do not wish to talk aboutdeath, dying or end of life care in relationto their COPD. They accept these patientswill always exist and that the wishes ofthe individual must be respected.
Breathing Space also found that a smallnumber of their patients were distressedwhen the subject of Advance CarePlanning was broached. Staff at thefacility considered that for some patientstiming of the discussions is very importantand as such an inpatient facility after anacute episode may not be right for them.Some staff and experts in end of life carebelieve that the right time is when thepatient is feeling relaxed and well,perhaps at an earlier stage in thediagnosis. This can often be lessdistressing and potentially more positivewith regard to planning.
Raising staff awarenessRaising the awareness of COPD as aterminal illness amongst clinical staff isone of the key imperatives in improvingend of life care for sufferers of thiscondition.
Respiratory staff understand that COPD isa very serious illness and will be familiarwith patients who have suffered severeexacerbations and have been very ill.However, the overriding evidence from allproject sites was felt that some staff werehesitant to acknowledge when proactivetreatment in a COPD patient may not beappropriate anymore and were thusreluctant to engage in the projects. Theywere also unsure of their competence totreat COPD patients when end of lifebecame a possibility. The desire to returnpatients to full health and the messageswhich patients received from clinical staffaround prognosis and recovery was oftenbased on this premise.
The first step the project sites took was indetermining the understanding andknowledge of staff in order to audit boththe awareness and the skills of individualson end of life care they had in the clinicalteams. There is some excellentinformation on undertaking skills auditsand determining what level ofcompetency and training staff need. Thesites carried out a training needs analysis,reviewed existing provision andbenchmarked it against nationalcompetences. They then used a needsbased approach to develop new trainingplans. For more information visitwww.endoflifecareforadults.nhs.uk/publications/talking-about-eolc
Once the improvement projects had thebaseline they were then able to initiateany training e.g. advancedcommunication skills, and clinicalsupervision which was needed. Withinthe projects some staff had alreadyreceived training through Association ofRespiratory Nurse Specialists (ARNS),some staff had in-house trainingarranged for them which was deliveredthrough small groups by a visitingpalliative care specialist, and others werethe need has been identified are nowwaiting to attend future courses.
The National End of Life Care Programmelaunched a new e-learning package inJanuary 2010: e-End of Life Care for All. It is freely available to all healthcare staff,with some public-facing modules forvolunteers/carers, and currently containsseveral sections on communication skills (for more information visit www.e-lfh.org.uk/projects/e-elca)
Primary care end of life registers forpatients with end stage COPDIt is widely acknowledged that patientswith COPD should be regularly reviewedin primary care. Patients who are deemedto be at the end of life should be addedto the practice end of life register (whichcould also be named ‘the palliative care’or ‘the Gold Standards Framework’register). This enables them to be placedon the correct pathway to accesstreatment and support.
Two of the projects looked at increasingthe numbers of COPD patients on theend of life registers (which nationallyaverages at about 14%). SolihullCommunity NHS Care Trust spent aconsiderable amount of time and effortundertaking some ‘leg work’ amongsttheir GP surgeries to generally raiseawareness of COPD as a life threateningcondition and also undertook training forprimary care staff in using prognosticindicators and undertaking Advance CarePlanning when COPD patients weremoved onto the end of life registers.
Hartlepool Primary Care NHS Trustworked with two practices to review theircurrent COPD registered patients usingthe BOD prognostic indicator tool. Someof learning identified the need to engageprimary care in this process to determineif the correct codes on the patient recordssystem are being used to record adiagnosis of COPD – as this willsignificantly affect how the patient ismanaged and ensures that the patient ison the correct clinical pathway inaccordance with their condition.

The background to the service Breathing Space is a unique nurse ledfacility in the heart of Yorkshire whichwas built in 2007 as a result of apartnership between the CoalfieldsRegeneration Trust, Rotherham PrimaryCare Trust and Rotherham MetropolitanBorough Council.
It is the largest multidisciplinarycommunity based chronic obstructivepulmonary disease (COPD) rehabilitationprogramme in Europe. Originally the soleaim was to care for patients with COPDand this has now been extended to otherchronic respiratory conditions. Its facilitiesinclude clinics for assessment andaccurate diagnosis, pulmonaryrehabilitation (for more than 400 patientsa year) and a 20 bed inpatient unitdedicated to providing care for acuteexacerbations.
At the time of joining NHS Improvement -Lung, the Nurse Consultant and ProjectLead, Gail South, had identified thatmany of the COPD patients at BreathingSpace had at least one of the GoldStandards Framework prognosticindicators often used to determine thelast 12 to six months of life. This providedthe catalyst for the service to look at theprovision of end of life care and how thispart of the pathway for patients at thefacility could be improved.
One - Breathing Space, RotherhamPrognostic indicators and advance care planning in chronicobstructive pulmonary disease (COPD)
The project aims and objectives The main aim of the project was toadvance the service delivery model forend of life care at Breathing Space as achoice for COPD patients and to supportthe carers of these patients during thisdifficult time.
The project hoped to answer some of thefollowing questions:
• Are Gold Standards Framework prognostic indicators for COPD predicting death within 12 months?
• Are COPD patients with at least one Gold Standards Framework prognostic indicator (and their carers) interested in participating in Advance Care Planning?
• Do staff feel that patients with at least one Gold Standards Framework prognostic indicator are appropriate forAdvance Care Planning?
• Do patients who have had Advance Care Planning achieve their preferred place of care and other goals?
• Do senior staff feel competent and confident at having these dscussions after appropriate training?
What they didA baseline audit was undertaken todetermine whether there was anyevidence to suggest prognostic indicatorswould be found amongst previouspatients who were admitted to BreathingSpace. This revealed 60% already had atleast one prognostic indicator.
Gail South (left) – Project Lead
9Breathing Space, Rotherham

10 Breathing Space, Rotherham
A paper audit form was then designed bysenior staff to be used to capture anyprognostic indicators present in patientsattending assessment as an outpatient tothe pulmonary rehabilitation programmeand at time of admission during an acuteexacerbation. The final page of the auditform asked the staff member responsiblefor admission to decide whether toinitiate an Advance Care Planningdiscussion with the patient. This includedgiving information to the patient, notablythe British Lung Foundation ‘Guide toCoping with the Final Stages of LungDisease’ and an adapted version of TheWhittington Hopsital NHS Trust patientleaflet on ‘Do Not Attempt Resuscitation’.
Patients and their carers were also giveninformation about their ‘PreferredPriorities for Care’ (PPC) and asked if theywanted to complete any of thedocuments either on their own or withassistance from staff.
Breathing Space used a PDSA (plan, dostudy, act) approach during August 2011to trial the form and they found quitequickly that one prognostic indicator wasnot necessarily an appropriate prompt forinitiating this kind of discussion andtherefore staff were documenting ‘notappropriate’. The form was changed touse three indicators as the trigger point,and if senior staff felt it was notappropriate to initiate this discussion atthis point, they were asked to documenttheir reasons as to why.
A spreadsheet recorded all the datainputted from the paper audit formscollected. In conjunction with this projectten staff on the inpatient unit attended apreliminary training session on advancedcommunication skills delivered by apalliative care specialist. This followed abaseline audit of training skills amongstall staff.
Issues and challengesDepartment of Health policy aimed attransforming community services meantthat Breathing Space integrated withRotherham Foundation NHS Trust inMarch 2011. This represented a challengein terms of the continuity for the projectas the then current provision of serviceswas reviewed by the new hostorganisation. In order to mitigate this thesenior team at Breathing Space involvedin the integration ensured that staff atRotherham Foundation NHS Trust werefully aware of the aims and objectives ofthe study and its progress by that date.
Locally the project lead spent a significantamount of time working on engagementand ownership of the project by thewhole team. Continuing to have regularmonthly meetings and emailing feedbackto all team members has helpedovercome communication barriers withstaff who rarely spend time together dueto changing shift patterns. Staff were alsocontinually encouraged to comment onthe project and data collection successesand difficulties.
Respiratory services also face their busiesttime over the winter months and highadmission rates and bed pressures haveimpacted on the progress of the projectwhere the time could be dedicated tosome of the data collection andadministrative functions.
Talks with staff indicated that many ofthem felt a certain level of unease whenasked to engage in an end of life carediscussion with patients. In order toensure staff felt empowered and skilledto undertake this sensitive andchallenging task, ongoing training incommunication skills and thedevelopment of clinical supervisionstrategies have given support to staffwhich has enabled reflective practice.
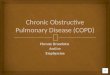
Key learningThe majority of patients who died duringthe period of the project had more thanthree Gold Standards Frameworkindicators present on their last admission,although overall staff felt the surprisequestion was perhaps a better predictorof death within a six to 12 month period.The ‘surprise’ question asks the clinicianto consider whether they would besurprised if the patient were still alive in12 months time.
Advance Care Planning materials used inthis project received mixed responsesfrom both staff and patients. The BritishLung Foundation booklet contained toomuch information for some patients andwas difficult for staff to use. BreathingSpace have decided to create their ownpatient folder which can be personalisedwith bite size information on differentelements of care which can be providedto the patient over a staggered period oftime.
Not surprisingly many clinical staff feltvery uncomfortable with end of life carediscussions. Even when patients hadthree prognostic indicators present onadmission, there were a sizeable numberof audit forms where staff had indicatedan Advance Care Planning discussion didnot take place. This could have been formany reasons, some included: previousbad experiences, lack of confidence in theskill to address this subject, a pre-perception that it was not necessary anda fear of worsening the patients mentalstate by introducing the topic of dying.Although these issues are still apparentthey are being addressed throughsupervision and training.

Breathing Space - Number of GSFindicators on death
60
40
20
0NR
Number of indicators
Nu
mb
er o
f Pa
tien
ts
1 2 to 3 3 or more
Outpatients
Inpatients
Perhaps less surprisingly, many COPDpatients felt uncomfortable with the ideaof end of life planning and some patientswere distressed when the offer ofAdvance Care Planning was madeavailable. Staff reflected on theseincidents and concluded that in somecases an acute inpatient admission maynot be the most appropriate time toinitiate this kind of discussion. They arenow considering the introduction of somegeneral end of life care informationduring the weekly pulmonaryrehabilitation sessions open to in andoutpatients of the service.
DataBetween 1 September 2010 and 31 July2011, a total of 683 patients with COPDwere either admitted to the inpatient unit(606) or attended an assessment forpulmonary rehabilitation (77).
Overall 186 (27%) patients had at morethan three prognostic indicators at timeof admissions.
83 patients died since 1 September 2010(76 inpatients and seven outpatients).Where recorded 18 out of 76 inpatientswho died had more than three prognosticindicators, nine had two to threeindicators and six had one indicator. Ofthe seven outpatients who died, threehad two to three prognostic indicatorsand two had one indictor where it hadbeen recorded.
However, there was a substantialimprovement in the recording of thenumber of GSF indicators in patients whodied as the project term went on.
GSF use in deaths in October -December 2010
1 GSF 2 - 3 GSF
Over 3 GSF GSF notrecorded
GSF use in deaths in January - March 2011
1 GSF 2 - 3 GSF
Over 3 GSF GSF notrecorded
GSF use in deaths in April - June 2011
1 GSF 2 - 3 GSF
Over 3 GSF GSF notrecorded
11Breathing Space, Rotherham

Breathing Space, Rotherham
Full year data from August 2010 to July2011 is shown below with regard to thenumber of patients with three or moreGSF indicators deemed appropriate forAdvance Care Planning and those whowent on to have the British LungFoundation booklet given and a PreferredPlace of Care recorded.
Project lead contact details
Gail SouthRespiratory Nurse ConsultantBreathing Space, Badsley Moor LaneRotherham S65 2QL
Tel: 01709 421700Fax: 01709 421701Email: [email protected]
Breathing Space - Comparison of pognostic indicators and end of life practice
GSF >3 and surprise =N ACP appropriate BLF completed PPC completed
18
16
14
12
10
8
6
4
2
0
Month
2010 2011
Nu
mb
er o
f Pa
tien
ts
8 9 1 2 3 4 5 6 710 11 12
12

Solihull NHS Care Trust
The background to the service Solihull Community NHS Care Trust hadalready adopted the Gold StandardsFramework in end of life care across all ofits 31 GP practices. Patients identified forthe Gold Standards Framework palliativeregister access community servicesthrough a supportive care pathway whichsupports holistic assessment, AdvanceCare Planning and proactive careplanning.
To date the pathway has improved theprovision of proactive coordinated carefor patients with end of life care needs inthe community. However, it wasrecognised that the number of patientswith chronic obstructive pulmonarydisease (COPD) accessing the pathwaywas limited.
It was felt the time was right to supportclinicians working in primary care and incommunity services with improvingidentification of patients with end stageCOPD for the Gold Standards Frameworkpalliative registers.
The project aims and objectives The project team worked with 12 out ofthe 31 GP practices in the geographicalarea. The main aim was to improveidentification of patients with end stageCOPD in primary care, to enable proactivecoordinated care and support preferredplace of care at the end of life.
Patients were supported by practices andcommunity teams using the GoldStandards Framework, the localsupportive care pathway and AdvanceCare Planning materials devised by localservices (MY COPD and MY LIFEbooklets).
Two - Solihull NHS Care TrustImproving identification of end of life care needs and Advance CarePlanning to support preferred place of care for patients with COPD
The main objectives for the project were to:
• Increase number of patients with COPDon Gold Standards Framework register from 8% (baseline) to 14% (the national average)
• Increase the number of patients supported in the community on the supportive care pathway
• Monitor the number of patients: with COPD on the GP practice Gold Standards Framework register, who are offered Advance Care Planning discussions and who have Preferred Priorities of Care recorded
• Monitor achievement of preferred placeof death and place of death for patients with COPD.
What they didBaseline data was collected to establishan overview of the current position withend of life care amongst the 12 GPpractices part of the improvementproject. This revealed that approximately9% of the total number of patientscurrently on the Gold StandardsFramework registers had an unconfirmedor confirmed diagnosis of COPD.
A letter of introduction was sent to thepractices to be involved. The project teamalso attended primary care meetings,such as a GP learning event in order toraise the profile of their work and spenttime in practices with community teamssharing information on the GoldStandards Framework prognosticindicators. They were also supported bysome concurrent care of the dying andcommunications skills training for staff inthe region which had been fundedthrough the Strategic Health Authority(SHA) and delivered by Education forHealth.
The information provided within thetraining sessions was formalised into localprognostic indicator guidance whichalong with the ‘My LIFE’ booklet wasshared amongst GPs, community matronsand community respiratory teams.
Guidance on read codes was pulledtogether as part of the preliminary workneeded before the use of ‘Graphnet’which is an electronic audit tool whichcan be used to search GP registers forpatients with certain diagnoses, as well asauditing patient outcomes relating tospecific read codes.
Sandy Walmsley – Project Lead Helen Meehan – Project Lead
13

14 Solihull NHS Care Trust
However, because of delays in being ableto implement the Graphnet tool theproject team reverted to using thecommunity care electronic records system(ePEX) to manually extract information onpatients they had identified throughpractice registers who were eligible butnot currently on the Gold StandardsFramework register.
A successful bid was entered to theStrategic Health Authority which resultedin funding for two GP champions forCOPD and end of life who were able towork for half a day per week with localpractices.
The team also developed a carer surveywhich was completed on bereavement.
Issues and challenges The main issue that delayed progress wasthe implementation of the Graphnet tool.There was recognition early on in theproject that baseline data from Graphnetcould not be captured retrospectively andthat some GP practices were usingvariable read codes which would havemade data extraction very difficult. Theonly solution for the team was to revertto manually collecting patient informationthrough their own community electronicrecord (ePEX) rather than interrogateindividual practice registers in primarycare. The team then faced furtherdisappointment in that due toorganisational changes due to thetransforming community services nationalwork the IT department was subsequentlydisbanded and the Graphnet tool couldnot be implemented.
Key learningAnecdotal evidence from practice staffsuggested that the Gold StandardsFramework indicators were not aseffective as the surprise question ( whichasks the clinician to consider whetherthey would be surprised if the patientwere still alive in 12 months time) as apredictor of death at six to 12 months.The project team are undertaking anaudit amongst GPs to determine morerobust evidence for this.
Advance Care Planning is vital tosupporting patients at end of life. Theteam benefited from already having thelocally designed and readily available ‘MyLIFE’ booklet which incorporates all therelevant information and is just forpatients with COPD.
The project team were also beensupported by two GP champions andincreased much needed awareness ofCOPD end of life issues by providingtraining to GPs and community teams.This was further reinforced withinformation on the palliative intranet site,which can be accessed by all GPs andcommunity services.
The integration of the community servicesand the acute Trust had some unforeseenbenefits for the project, mainly improvedcommunication between the respiratorycommunity team and the end of lifeprovision on the wards. Overallrelationships have been improved with allstakeholders and especially hospices,which now have greater awareness ofterminally ill patients with respiratorydisease.
DataFor the 12 GP surgeries the baseline dataat the start of the project demonstratedthat 214 patients were currently on theend of life practice registers, of which 20patients had a (confirmed andunconfirmed) diagnosis of COPD. Thisrepresented 9% of patients.
Midterm data showed the number ofCOPD patients on the register hadincreased to 28 – with 247 patients onthe register overall. This represented anincrease of COPD patients to a proportionof 11%.
End of project data was only availablefrom 11 practices and showed there were266 patients on the end of life registerwith 19 having a primary diagnosis ofCOPD (7%).
Data on place of death showed that forthe entire Primary Care Trust area (31practices in total) the number of patientsdying of COPD at home rose from 20%in 09/10 to 23% in 10/11.
The patient satisfaction survey revealedthat of those questioned 90% were verysatisfied with the overall experience ofcare they had received to date.
Project lead contact details Helen MeehanLead Nurse Palliative CareSolihull NHS Care TrustTel: 0121 712 8471Email: [email protected]
Sandy WalmsleyLead Respiratory Nurse SpecialistSolihull NHS Care TrustTel: 0121 329 0179Email: [email protected]

15North Tees and Hartlepool Primary Care NHS Trust
The background to the service The respiratory nursing care communityteam have a well established servicewhich operates out of the heart ofHartlepool in new facilities – ‘One Life’.The current team have a well establishedlink to the palliative care community teamand as part of their commitment todevelop effective and quality carepathways for patients they wanted toaddress the particular challenges of theend of life pathway in chronic obstructivepulmonary disease (COPD).
A multidisciplinary end of life groupadapted an existing set of indicatorsincluding: body mass index, FEV1obstruction and MRC dyspnoea score(originally including exercise and knownas BODE – Celli et al, 2004) whichbecame known as BOD.
The project team led by a British LungFoundation nurse and supported by arespiratory and a palliative care consultanttrialled BOD within two GP practices inthe Hartlepool locality.
The project aims and objectivesTo improve recognition of thedeteriorating COPD patient and their endstage / end of life potential by utilisingthe BOD tool as a prognostic indicatorand trigger tool to facilitate end of lifediscussion and referral to resources.
What they didTwo GP surgeries were approached andbaseline data collected on the number ofpatients on the COPD registers.
The BOD index was then used by theproject manager (Dorothy Wood) inconjunction with the practice teams toidentify patients on the COPD registerwho were eligible for discussion aroundtheir condition and given the opportunityfor Advance Care Planning.
Three - North Tees and Hartlepool Primary Care NHS TrustThe implementation of BOD in primary care
A process of staff awareness raising andtraining on BOD as a prognostic indicatortool and end of life care discussions tookplace alongside the case finding in orderto embed the new practice with staff andensure sustainability.
To date five practices are routinelyrecording BOD scores during routineCOPD patient reviews. Scores arerecorded on a template and an increasein score at future consultations willindicate a deteriorating patient.
Issues and challengesDespite a positive start with the two GPpractices more practice recruitment isrequired to demonstrate an evidencebased benefit from a qualitativeperspective and because of this a gradualapproach to recruiting GP practices hasbeen adopted. The implementation isconsidered part of an on-going plan to
improve shared decision making,autonomy and access to resources forCOPD patients. It is hoped that all of theGP practices in Hartlepool will beapproached and agree to record the BODIndex.
Staff shortages in community respiratoryservices made the project challenging,however, it is envisaged that once GPpractices understand the philosophy theywill be able implement the projectwithout intensive project teaminvolvement in the future. Input wouldthen be more of a supportive role.
Originally there was difficulty in obtaininga template for recording BOD scores aswell as obtaining a read code frominformation technology. Both wereeventually made available in April 2011.Practices that do not have this system willbe able to develop their own template.
Left to right: Dr Niall Kearney and Dorothy Wood

16 North Tees and Hartlepool Primary Care NHS Trust
The Trust covers two main urban areas:Hartlepool and Stockton. There was alesser degree of engagement from theStockton area and although threesurgeries voiced an interest inimplementing BOD due to pressure ofwork the support required to carry thisinterest through has not been available.
Key learningLearning on the use of BOD suggests it isa good predictor of the intermediarystage between the start of decline in thepatient condition rather than of death atsix to 12 months.
BOD was used as a trigger to facilitatediscussion about how the patient wasmanaging their condition and what thepatients concerns were. It also allowedthe professional to gather all of thoseconcerns together and engage in shareddecision making with the patient abouttheir future.
Practice nurses recognised that thosepatients with the highest BOD scoreswere predominantly those with thehighest morbidity and this ensured thepatient had the opportunity to plan fortheir death when they were feeling well(if they wished to) and had more timelyaccess to available resources.
As with other projects it was identifiedthat not all staff were confident instarting a planning ahead discussion withpatient. The Foundation Trust has nowinvested in training two members of staffto become facilitators in delivering SAGEand THYME™ training. (SAGE andTHYME™ is a communication model forhealth and social care professionals toenable them to communicate effectivelywith concerned or distressed people andrespond in a way that empowers thedistressed person). The two-day coursewill gradually be delivered to practice
nurses to enable them to improve theircommunication skills and confidence inmanaging planning ahead discussionseffectively.
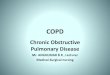
DataThe number of patients on the COPDregister for both practices remainedrelatively static throughout the projectperiod. Overall, by the end of the project189 patients had been reviewed usingthe BOD scoring system whichrepresented about 85% of the totalnumber of patients on the register atJune 2011 (223).
Project lead contact details Dorothy WoodBLF Lead Respiratory NurseONE LIFE HARTLEPOOLPark Road, Hartlepool TS24 7PW
Tel: 07917 172464Office: 01429 285712Email: [email protected]
Month
July 2010August 2010September 2010October 2010November 2010December 10January 2011February 2011March 2011April 2011May 2011June 2011
No of patients onCOPD register
229229229228225225225223223222223223
No of patientsreviewed
141519221615191420231813
Cumulative Total
142948707993102116136159177189
Total patients on COPD register
250
200
150
100
50
0
Month
Nu
mb
er o
f Pa
tien
ts
Jul 10 Aug 10 Sep10 Oct10 Nov10 Dec10 Jan11 Feb11 Mar11 Apr11 May11 Jun11
Patients reviewed using BOD this month
Progress in reviewing COPD patients in two GP practices in Hartlepool using BOD

17Acknowledgements
Acknowledgments
NHS Improvement - Lung would like tothank all national improvement projectsites for their hard work and dedicationto improve quality and care for peoplewith COPD, and for their contributions tothis document.
In addition, the following people haveprovided a source of expertise andsupport and their help is gratefullyacknowledged:
Eleanor Sherwen, End of Life CareProgramme Manager, End of Life CareProgramme
Phil Duncan, Director, NHS Improvement - Lung
Catherine Blackaby, NationalImprovement Lead, NHS Improvement -Lung
Ore Okosi, National Improvement Lead,NHS Improvement - Lung
Catherine Thompson, NationalImprovement Lead, NHS Improvement -Lung
Zoë Lord, National Improvement Lead,NHS Improvement - Lung
Alex Porter, Senior Analyst,NHS Improvement - Lung
For more information please contact:Hannah Wall, National ImprovementLead for End of Life Care and [email protected]

18 References
COPD and Asthma Outcomes Strategy forEngland and Wales (DH: 2011)
Consultation on a Strategy for COPDServices in England and Wales (DH: 2010)
End of Life Care Strategy (DH: 2008)
End of Life Care Strategy (Department ofHealth: 2008)
The Gold Standards Framework www.goldstandardsframework.nhs.uk
The BODE IndexCelli BR et al (2004): New EnglandJournal of Medicine 350 p1005-1012
The National End of Life Care Programmewww.endoflifecareforadults.nhs.uk
National Palliative Care Councilwww.ncpc.org.uk
The Whittington Hospital NHSFoundation Trustwww.whittington.nhs.uk
St Christopher’s Hospicewww.stchristophers.org.uk
British Lung Foundationwww.lunguk.org
References


NHSNHS Improvement
HEART
LUNG
CANCER
DIAGNOSTICS
STROKE
©N
HS
Impr
ovem
ent 20
11 |
All
Righ
ts R
eser
ved
Publ
icat
ion
Ref: IM
P/co
mm
s026
- N
ovem
ber 20
11
NHS Improvement3rd Floor | St John’s House | East Street | Leicester | LE1 6NB
Telephone: 0116 222 5184 | Fax: 0116 222 5101
www.improvement.nhs.uk
NHS Improvement
NHS Improvement’s strength and expertise lies in practical service improvement. It has over adecade of experience in clinical patient pathway redesign in cancer, diagnostics, heart, lung andstroke and demonstrates some of the most leading edge improvement work in England whichsupports improved patient experience and outcomes.
Working closely with the Department of Health, trusts, clinical networks, other health sector
partners, professional bodies and charities, over the past year it has tested, implemented, sustained
and spread quantifiable improvements with over 250 sites across the country as well as providing
an improvement tool to over 1,000 GP practices.
Delivering tomorrow’simprovement agenda for the NHS