Embed Size (px)
Citation preview

Hand Infections


Palmer Fascia
• Thick centrally Fibrous palmer aponeurosis– Triangular
– Proximally continous with flexor retinaculum and tendon of palmaris longus muscle.
– Distally forms 4 digital bands attached to bases of proximal phalanges
• Thin over the thenar and Hypothenar Eminences


Fibrous digital sheaths• Ligamentous tubes that enclose
– Synovial sheaths
– Superficial and deep flexor tendons
– Tendons of Flexor policis longus

Medial fibrous septum
• Medial border of palmer aponeurosis to 5th
metacarpel.– Medial to this is hypothenar compartment
Lateral Fibrous septum
• Lateral border of palmer aponeurosis to the 3rd metacarpel .• Lateral to this is thenar compartment

Central compartment
• Between thenar and hypothenar compartment
• Contains
– Flexor tendons and their sheaths
– Lumbricals
– Superficial palmer arterial arch
– Digital vessels and nerves

Adductor compartment
• Deepest muscular plane of palm
• Contains adductor pollicis

Radial bursa
• The radial bursa is a continuation of the flexor pollicis longus tendon sheath through the flexor retinaculum to a level 2.5 cm above the wrist joint
– Superiorly continous with common sheath
– Inferiorly extends upto distal phalanx of thumb.

Ulnar bursa
• Ulnar bursae includes little finger tendon sheath which begins at terminal phalanx and extends proximally half way up the palm.
• The long flexor tendons of the fingers (FDS and FDP) are enclosed in a common sheath while passing through the flexor retinaculum
• These two sheath extend above the flexor retinaculum and communicate with each other in carpel tunnel in 80 percent of cases.


Superficial pulp space• The pulp space of the fingers is a closed compartment
situated in front of the terminal phalanx of each finger
• Each space is subdivided into numerous smaller compartments by fibrous septa
• Infection of such a space is common and serious
• Commonly occurring in the thumb and index finger
• Bacteria are usually introduced into the space by pinpricks or sewing needles

Clinical significance
• Accumulation of inflammatory exudate within these compartment causes the pressure in the pulp space to quickly rise.
• In children, pressure on the blood vessels could result in necrosis of diaphysis
• Close relationship of the proximal end of the pulp space to the digital synovial sheath accounts for the involvement of the sheath in the infectious process when the pulp-space infection has been neglected



Paronychia

Paronychia
• Infection of the lateral nail fold
• If Infection extends to the eponychium
(defined as the thin membrane
distal to the nail wall at the base
of the nail), it is properly termed
an eponychia.
• When infection involves both lateral nail folds and eponychium, it is called a run-around infection

• In adults, Staphylococcus aureus is the most common pathogen
• Pathophysiology
• Infection occurs when there is violation of the seal between the nail plate and nail fold, allowing the inoculation of bacteria.
• Risk Factors– Hangnails,
– Manicures,
– Penetrating trauma,
– Constant exposure to a wet or moist environment,
– Nail biting or sucking

• Clinical presentation
• Initial swelling, erythema, tenderness with progression to fluctuance, and abscess formation are typical.
• Spontaneous decompression can occur, including tracking beneath the nail plate (subungual abscess).
• Deeper infections can involve the nailbed, pulp space, and bone, producing nailbed destruction, felon, or osteomyelitis
Treatment
• Early stage– Oral antibiotics,
– Warm soaks
– Rest and observation
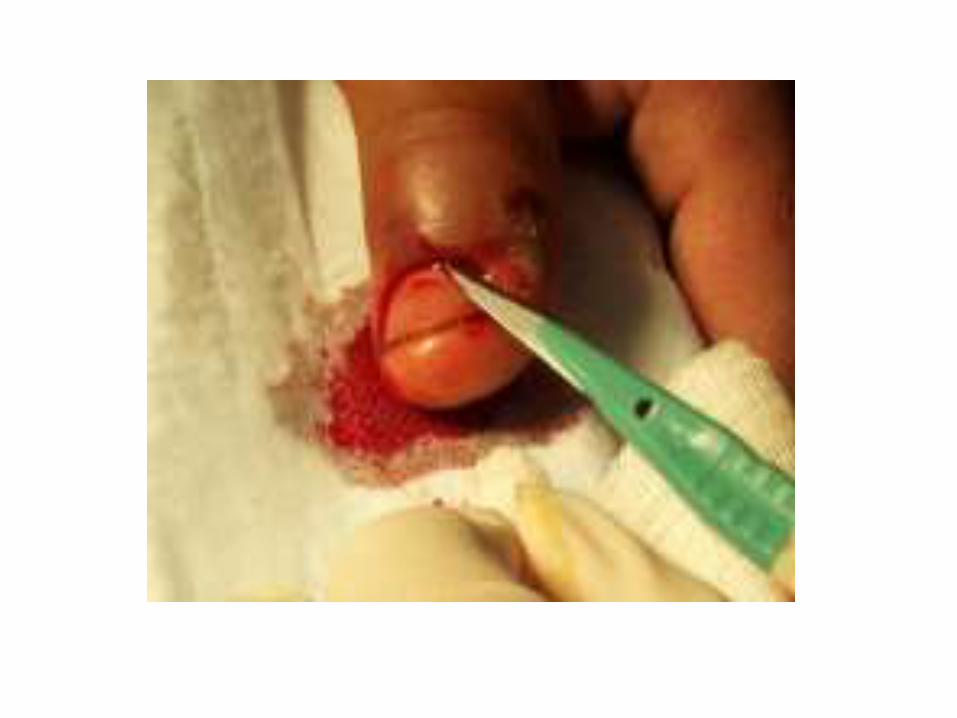
• Surgical decompression is the treatment of choice– Decompression is performed by carefully entering the
abscess cavity between the nail plate and nail fold with a scalpel blade .
– A small wick is placed for 24 to 48 hours to prevent the incision from closing and recurrence of the infection. The wick is removed, and saline warm soaks are begun

A: An infected lateral and proximal nail fold can be elevated by an elevator or scalpel. B:
For extensive infections, a relief incision(s) is made perpendicular to the edge of the nail
fold to allow for removal of a portion or all of the nail plate. (Reprinted from Seiler JG.
Essentials of hand surgery. Philadelphia: Lippincott Williams & Wilkins, 2002, with
permission. Copyright American Society of Surgery of the Hand.)

• Depending on the extent of the infection, a partial or complete nail plate removal with or without lateral nail fold relief incision(s)is performed.
• The incision should be made perpendicular to the edge of the nail fold.
• A single or double incision is used depending on the location of the infection
• Subungual abscesses are treated with removal of a portion of or the entire nail. The abscess is carefully debrided while protecting the sterile and germinal matrices

(A) Elevation of the eponychial fold with flat probe to expose the base of
the nail. (B) Placement of an incision to drain the paronychium and to
elevate the eponychial fold for excision of the proximal one-third of the
nail. (C-E) Incisions and procedure for elevating the entire eponychial
fold with excision of the proximal one-third of the nail. A gauze pack
prevents premature closure of the cavity.

• Chronic paronychia
• Chronic paronychia occurs more commonly in individuals constantly exposed to moist environments.
• Infections may be intermittent; clinically, the eponichial fold is thickened and painful
• Candida albicans is a frequent offending
organism
• Topical antifungal ointments are generally used
4 to 6 weeks.
FIGURE 5. Eponychial marsupialization is performed by removing a small, crescent-
shaped portion of the eponychial fold proximal to the distal edge of the eponychial fold.
Care is taken to not injure the underlying germinal matrix. (Reprinted from Seiler JG.
Essentials of hand surgery. Philadelphia: Lippincott Williams & Wilkins, 2002, with
permission. Copyright American Society of Surgery of the Hand.)

Felon

Felon
• A felon is a deep space infection or abscess of the distal pulp of the finger or thumb.
• It differs from the superficial apical infection involving the distal portion of the pulp skin, which often responds to a small, deroofing incision
• The organism most frequently cultured from a pulp space infection is S. Aureus

Felon
Pathophysiology• Infection typically is due to direct inoculation of
bacteria by penetrating trauma but may be caused by– hematogenous spread – local spread from an untreated paronychia.
• Most common in thumb and index finger.
Clinical presentation• Throbbing pain and• Tense swelling localized to the pulp

Felon
“Don’t wait for fluctuation if tension is severe”
• Infection results in edema increased pressure within the closed compartmentimpaired venous outflow local compartment syndrome
• Invasion of the bone may lead to osteomyelitis

Treatment• Surgical decompression.
• One of several incisions can be used,
– unilateral longitudinal incision,
– a J-shaped or hockey-stick incision,
– a through-and-through incision,
– or a volar longitudinal incision. A fishmouth incision should be avoided .
• Although the site of maximal induration often dictates the location of the incision
•
• Unilateral longitudinal incision is ideally performed on the noncontact surface of the involved digit. This includes
– the ulnar sides of the index and long fingers and
– the radial sides of the ring finger, small finger, and thumb

FIGURE 7. Incisions used for decompression of a felon. A: A
midlateral incision is preferred. B: A J-shaped or hockey-stick
incision. C: A through-and-through incision. D,E: A volar transverse
or longitudinal incision.

• The best is a longitudinal incision over the area of greatest fluctuance because it avoids– Skin slough– Digital nerve injury – Creation of an
unstable fat pad
• To avoid penetration of the tendon sheath, the incision should not extend to the distal interphalangeal crease.

Additional measures
• Pus should be taken for C&S
• Initial empiric antibiotic coverage with a second-generation cephalosporin, such as cefazolin, while awaiting culture identification and sensitivity is usually adequate.
• Addition of gram-negative coverage is recommended in an immunocompromised individual.
• Postoperative wound care, edema control, splinting, and motion optimization are preferably pursued with therapy supervision

Herpetic Whitlow

Herpetic whitlow
• Herpetic whitlow is an intensely painful infection of the hand involving 1 or more fingers that typically affects the terminal phalanx.– Commonly involves thumb and index fingers
Risk factors• Genital herpes in self or partner.
• Health care workers
• Children with gingivostomatitis
Adamson first described herpetic whitlow in 1909, and in 1959, it was noted to be an occupational risk among health care workers

Herpetic whitlowSymptoms
– Localized pain, pruritus, and swelling followed by the appearance of clear vesicles
– Typically localized to 1 finger only (symptoms involving more than 1 finger are more typical of coxsackievirus infection)
Clear vesicles on an erythematous border localized to 1 finger Pain, typically out of proportion to findings Edema Turbid or cloudy fluid in vesicles possibly suggesting a
superimposed pyogenic infection In later stages, coalescence of vesicles to form an ulcer Distal finger pulp remains soft, distinguishes HSV infections from
bacterial felon

Herpetic whitlow
Diagnosis • The diagnosis can be confirmed by a Tzanck test, which
demonstrates the presence of multinucleated giant cells in a scraping taken from the base of an unroofed vesicle.
Treatment • Self limited disease
• Incision is contraindicated as it spreads the infection may lead to herpetic encephalitis
• Unroofing relieves the pain
• Topical antifungals can be applied.

Web space infections

Web space infections•Communication:
–Palmar surface contiguous with dorsal subcutaneous
Borders: –Dorsal / Volar
•Dorsal hand fascia •Palmar fascia
Radial/Ulnar Digital extensor
mechanisms and MCP joint structures –Distal
Vertical septae of palmar aponeurosis, approx. 2cm proximal to interdigital webs

Web space infections
• Also known as a collar button abscess or hourglass abscess.
• Involves the subfascial palmar space between the digits
• Begins as an infected blister, an open wound, or a palmar callus or from the adjacent subcutaneous area.
• An abscess subsequently develops and extends either volarly or usually dorsally to include the contiguous subcutaneous space of the dorsal hand
Webspace infections
• Clinical presentation
• The involved adjacent digits are held apart from one another in a characteristic abducted posture.
• This clinical presentation, combined with prominent dorsal hand swelling and a tender palmar web space, usually makes the diagnosis clear

Webspace infectionsTreatment
• Incisional drainage is performed with separate dorsal or volar or combined approaches .
• The type of incision(s) used depends on the location of the abscess.
•
• A combined approach is used in cases in which the infection is noted both dorsally and volarly.
• A transverse incision in the web space itself should be avoided to prevent possible web space scar contracture .
• After formal debridement and irrigation of the wound, a 16-gauge polyethylene catheter can be sutured into an open wound to allow for subsequent saline irrigation (100 mL per hour) of the wound for 24 to 48 hours.

(A) Curved longitudinal volar incision for drainage of a web , (B) Dorsal
incision used in conjunction with A. (C) Volar transverse incision, can cause web
space contracture. (D) Volar exposure, used with dorsal incision B.

Dorsal Subaponeurotic Space Infections

• The dorsal subaponeurotic space is a potential space located deep to the extensor tendons and dorsal to the metacarpals
• Penetrating trauma usually introduces bacteria to this space, which can subsequently become an abscess
Dorsal subaponeurotic space infections

Treatment • Aggressive surgical incision and debridement are
recommended if in doubt.
• Two dorsal longitudinal incisions are preferable rather than a single central one, which may result in tendon desiccation.– One incision is centered over the second metacarpal.– the other is in the fourth-fifth intermetacarpal region to allow an
adequate intervening skin bridge.
• Care is taken to protect the dorsal veins to minimize hand swelling.
• The wounds are allowed to heal by secondary intention, and early hand motion is instituted to minimize extensor tendon adhesions


Palmer space Infections
• The deep palmar spaces are potential spaces in the hand and are divided into
– The midpalmar space,
– Thenar space,
– Hypothenar space,
– Posterior adductor space


Mid palmer space
• The midpalmar space Lies posterior to the long flexor tendons to the middle, ring and little fingers and in front of the interossei and the 3rd, 4th and 5th metacarpal bone
• Radially, it is bordered by the midpalmar or oblique fascial septum. This septum extends from the third metacarpal to the sheath, enclosing the long-finger flexor tendons (ulnar bursa in some people).
• Distally, the midpalmar space extends to the level of the vertical septa of the palmar fascia, ending approximately 2 cm proximal to the web spaces.
• Proximally, the space extends to the distal edge of the carpal canal.
– Midpalmer space is continous with the anterior compartment of forearm ( space of parona) via the carpel tunnel
Thenar space
• The thenar space is bordered – Medially by the vertical midpalmar septum
– Posteriorly and radially by the adductor pollicis fascia,
– Lies deep to the long flexor tendons to the index finger and in front of adductor policis muscle
• Communicates with web of thumb and under flexor retinaculum.



Clinical significance of thenar space
• The thenar space lies just superficial to the adductor pollicis muscle, forming a plane connecting the deep aspects of the radial bursa and the ulnar bursa.
• Abscess or space occupying lesions may spread transversely through the thenar space deep in the palm between the thumb and the carpal tunnel

Hypothenar space
• The hypothenar space is located ulnar to the midpalmar space,
– Contains the hypothenar muscles and is enclosed by their investing fascia.
• This space is bordered radially by a fibrous hypothenar septum coursing between the fifth metacarpal and palmar aponeurosis
Posterior adductor space
• The posterior adductor space is another potential space located dorsal to the adductor pollicis and palmar to the first dorsal interosseous.
Clinical presentation• Pain
• Erythema
• Swelling ,
• Guarding with tenderness at the focus of abscess.
• It is not unusual for a patient to present 48 to 72 hours after a penetrating injury with signs of infection.

In midpalmar space infections, the hand loses its normal palmar concavity with tenderness and induration over the palm. There is dorsal hand swelling and limited and painful motion of the middle and ring fingers
In thenar space infections, the thenar region is dramatically swollen and exquisitely tender. The thumb is abducted due to the increased pressure and volume in the thenar space. Motion of the thumb and index finger is painful.

Surgical incisions used for midpalmar space infection
• Options include
– a preferred curvilinear longitudinal approach,
– a transverse incision through the distal palmar crease,
– a distal palmar incision approach through the lumbrical canal,
– a combined transverse and longitudinal incision.

FIGURE 10. Incisions used for
decompression of midpalmar
space infections.. A: A transverse
incision through the distal palmar
crease. B: A distal palmar
incision approach through the
lumbrical canal. C: A combined
transverse and longitudinal
incision. D: A curvilinear
longitudinal approach (Reprinted
from Seiler JG. Essentials of hand
surgery. Philadelphia: Lippincott
Williams & Wilkins, 2002, with
permission. Copyright American
Society of Surgery of the Hand.)

Surgical incision for thenar space infection
• A thenar space infection may require a volar and a separate dorsal first web space incision (preferred) if dorsal extension has occurred around the adductor pollicis and first dorsal interosseous muscles. This is the so-called dumbbell, or pantaloon, abscess.
– On the volar side, an incision is made adjacent and parallel to the thenar crease. Great care is taken to avoid injury to the palmar cutaneous branch of the median nerve in the proximal part of the incision and motor branch of the median nerve in a deeper plane.
– A second, slightly curved longitudinal incision is made on the dorsum of the first web space

(A) Volar transverse approach to
the thenar space. Nerve injury is
a potential complication. (B)
Thenar crease approach. Nerve
injury can result from this
approach. It has the added
disadvantage of limited drainage
of the space behind the adductor
pollicis. (C) Dorsal transverse
approach. A contracture of the
web space can result if this
incision is placed too close to the
edge of the web. (D) Dorsal
longitudinal approach to the
thenar space.
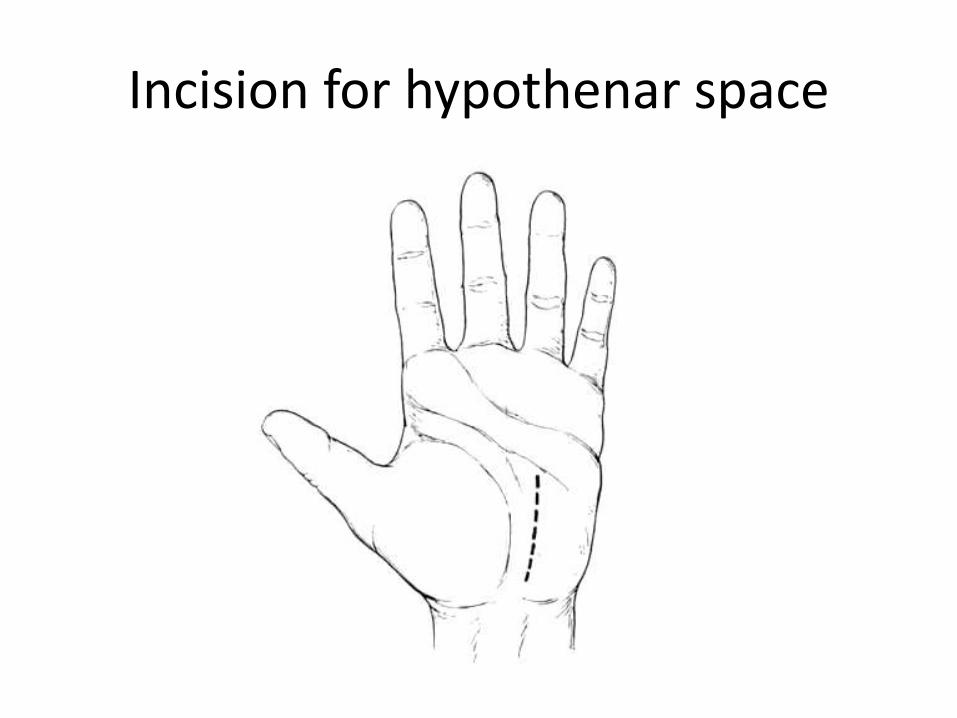
Incision for hypothenar space

Pyogenic Flexor Tenosynovitis
Relevant anatomy
• The flexor sheath is an intricate continuous synovial sheath originating at the level of the metacarpal neck and ending at the insertion of the flexor digitorum profundus.
• It separates into an outer parietal and an inner visceral layer.– The parietal layer thickens at different intervals, consistently
forming discrete annular and cruciform pulleys.
– The visceral layer is the epitenon.
– Between the two layers is the synovial space, which is essentially a closed space

Clicinal relevance• The flexor sheath of the little finger flexor digitorum profundus
tendon (and, on occasion, the ring, long, and index fingers) communicates with the ulnar bursa, which extends proximal to the wrist level.
• The flexor sheath of the flexor pollicis longus communicates with the radial bursa, which extends proximal to the wrist level as well.
• The radial and ulnar bursa can communicate at the level of the transverse carpal ligament through Parona's space producing a horseshoe abscess.
• Parona's space is a potential space in the distal forearm located between the pronator quadratus muscle and the flexor digitorum profundus tendons.


Pyogenic Flexor Tenosynovitis
• Pyogenic flexor tenosynovitis, or suppurative flexor teno-synovitis, is a bacterial infection of the digital flexor sheath.
• The majority of these infections are secondary to traumatic penetrating injuries; therefore, skin flora, including S. aureus, is the source of the most common infecting organisms

Clinical presentation
• Kanavel's four cardinal signs:
– tenderness along the flexor sheath
– a semiflexed resting posture of the involved digit
– symmetric digital swelling (sausage digit),fusiform swelling
– pain with passive extension of the digit (the most reproducible clinical sign),
*Not all signs may be present

Pyogenic tenosynovitis of index finger

Incisions for drainage of
tendon sheath infections. (A)
Open drainage incisions. (B)
Single incision for instillation
therapy of tendon sheath
infection. (C) Sheath irrigated
via needle proximally and
single distal incision. (D)
Incisions for through-and-
through intermittent
irrigation. (E) Closed tendon
sheath irrigation technique.
(F) Closed irrigation of ulnar
bursa.
Radial and ulnar bursa infection
• Infection of both 'bursa' may result from direct spread proximally along the associated tendon sheath or from a penetrating injury.
• Treatment is similar to that recommended for tendon infections: – open or closed irrigation, leaving a drain in situ – antibiotic cover


Principles of hand incisionsTake home message
• Incisions should be outlined by sterile surgical markersbefore making the actual incision to – confirm appropriate position,
– to confirm the adequacy of skin bridges should multiple incisions be used,
– to help guide closure.
• Incisions can be made in skin creases on the volar aspect of the hand but incisions in deep creases should be avoided due to– the thin subcutaneous tissue,
– tendency for maceration due to moisture,
– tendency toward poor apposition of skin edges on closure.

• Incisions perpendicular to a volar flexion crease should be avoided – to prevent scar formation and– secondary skin contractures that can lead to loss of motion
and functional impairment
• Incisions on the dorsal surface of the hand can be smaller due to the more mobile and loose nature of the dorsal skin
• Vertical, horizontal, and curved incisions can all be used with good facility as long as adequate skin bridges are maintained
Principles of hand incisionsTake home message

• Fingers can be exposed dorsally, volarly, or midaxially.– Dorsal incisions can be longitudinal or curvilinear.
– Volar incisions are best facilitated by a zigzag pattern that crosses creases laterally and at angles.
– Midaxial incisions are best placed at the junction of glabrous and nonglabrous skin, with attention being paid to the neurovascular bundle that sits in the plane of the flexor sheath. The neurovascular bundle can be taken volarly with the volar flap or can be left in place by carrying the dissection superficial to it.
Principles of hand incisionsTake home message



Compartment syndrome of the forearm of an anticoagulated patient after the radial artery was punctured while obtaining an arterial blood gas.


• Apply tourniquet to upper arm if ischemia is not threatening the extremity. Fasciotomy can be performed without use of tourniquet in emergency or if critical ischemia time is being approached.
• Exsanguinate the arm with an esmarch bandage and inflate tourniquet to 100mm Hg higher than systolic pressure.
• Make a curvilinear S-shaped skin incision on the volar aspect of the forearm. Incision should begin proximally medial to the biceps tendon (apex of flap is radial to medial epicondyle) and end distally between the hypothenar and thenar eminences. Make sure to cross flexion creases at an angle to avoid postoperative linear contractures across the antecubital fossa and wrist. S-shaped incision should be made in such a way to create a radial sided flap in the mid to distal forearm so that the median nerve will be covered.
• Proximally, divide the lacertus fibrosis.

• Incise and release the superficial volar compartment fascia throughout its entire length.
• Expose the deep compartment of the forearm by retracting the flexor carpi ulnaris and the underlying neurovascular bundle medially, and then retracting the flexor digitorum superficialis and median nerve laterally. The flexor digitorum profundus should now be visible.
• Incise and longitudinally release fascia overlying the flexor digitorum profundus.
• Perform carpal tunnel release by incising the transverse carpal ligament along the ulnar border of the palmaris longus tendon. Ensure median nerve is protected.
• Release ulnar nerve in Guyon’s canal if needed.
• If muscle still appears tense, perform epimysiotomy of individual muscle bellies.
• If median nerve is exposed in distal forearm, suture distal skin flap closed loosely over the nerve (see image below).
• Leave incision open, do not close the skin.
• Assess dorsal compartments to determine if fasciotomy needed.

Dorsal approach for release of dorsal compartments

• Pronate forearm.
• Make dorsal skin incision beginning distal to lateral epicondyle between extensor digitorum communis and extensor carpi radialis brevis, extending distally approximately 10 cm towards midline of wrist.
• Gently create skin flaps so that the mobile wad can be identified.
• Release the fascia overlying mobile wad of Henry and the extensor retinaculum.
• Leave skin incision open.
• Apply sterile moist dressings to volar and dorsal skin incisions.
• Place long-arm splint making sure to not flex the elbow beyond 90 º.

Locations for dorsal incisions over second and fourth metacarpals. Provides access to the dorsal and volar interosseous compartments and adductor compartment to the thumb.
Hand fasciotomy

Hand fasciotomy
Locations for thenar incision over radial aspect of the thumb metacarpal and mark for the hypothenar incision over ulnar aspect of the fifth metacarpal.

• Apply tourniquet to upper arm if ischemia is not threatening the extremity. (Fasciotomy can be performed without use of tourniquet in emergency or if critical ischemia time is being approached.)
• Make 2 dorsal longitudinal skin incisions over the second and fourth metacarpals —this will allow access to the dorsal and volar interosseous compartments as well as the adductor compartment to the thumb.
• Use tenotomy scissors to carefully carry incisions down on either side of the metacarpals to release the dorsal interossei.
• Continue deep dissection on the radial and ulnar borders of the index and ring finger metacarpals, thus releasing the first palmar interosseus, the adductor compartment to the thumb, and the palmar interossei.

• Make separate longitudinal volar incisions over the thenar and hypothenar compartments. These incisions should be placed over the radial aspect of the thumb metacarpal and the ulnar aspect of the small finger metacarpal, respectively.
• Assess digital swelling and perform digital fasciotomies if warranted.
• If digital fasciotomy is warranted, place mid-axial lateral incisions on the ulnar aspect of the index, ring, and long fingers and on the radial aspect of the thumb and small finger. Place the incision along the most dorsal portion of the joint flexion creases. A more volar incision could lead to a flexion contracture.


References • Hand Surgery
– Richard A. Berger– Arnold-Peter C. Weiss
• Sabiston Textbook of Surgery• Schwartz's Principles of Surgery, 9th Edition• Wheeless' Textbook of Orthopaedics• Medscape