Embed Size (px)
Citation preview

INTRODUCTION
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Geriatric SyndromeGERIATRIC SYNDROMES are common clinical conditions that don't fit into
specific disease categories but have substantial implications for:
functionality and life satisfaction in older adults
Besides leading to increased
mortality and disability,
decreased financial and
personal resources, and longer
hospitalizations, these
conditions can substantially
diminish quality of life
INTRODUCTION
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Geriatric SyndromeMain:
Pressure ulcers,
incontinence, falls,
functional decline
delirium.
Others:
Malnutrition,
eating and feeding problems,
sleeping
problems,
dizziness and syncope and
self-neglect have
5 COMMON CONDITIONS
Main:
Pressure ulcers,
incontinence, falls,
functional decline
delirium.
Others:
Malnutrition,
eating and feeding problems,
sleeping
problems,
dizziness and syncope and
self-neglect have
(Inouye, Studenski,
Tinetti, & Kuchel, 2007).
INTRODUCTION
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
NEW “EVOLVING” SYNDROMES
sarcopenia
polyprovider
polypharmacy
pain
frailty
INTRODUCTION
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Urinary IncontinenceGeriatric Syndrome
Alfie R. Espinosa, RNInfection Control Officer
Perioperative Nurse
What is UI?
URINARY INCONTINENCE
involuntary loss of urine that is sufficient to be a problem (Fantl et al., 1996)
the involuntary loss of urine so severe as to have social and/or hygienicconsequences for individuals and/or their caregivers, is a major clinicalproblem and a significant cause of disability and dependency.
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Continence Foundation of the Philippines, (2006)
14.6% for urinary incontinence amongfemales and 6.8% among males
UI is only half as prevalent among mencompared to women.
Whereas mixed urinary incontinence(58.7%) prevails among women
most reports show the predominance ofoveractive bladder or detrusoroveractivity (49%) among men.
ASIAN prevalence rate (1998):
URINARY INCONTINENCE
Continence Foundation of the Philippines, (2006)
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
URINARY INCONTINENCE
Cellulitis Pressure ulcers Urinary Tract Infection Falls with fractures Sleep deprivation Social withdrawal Depression Embarrassment (50%) Interference with activities Caregiver burden - contributes
to institutionalization Increase in healthcare cost Decrease quality of life
CONSEQUENCES of UI:
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Dementia 11-90%
Community Dwelling 8-38%
Homebound 15-33%
Hospitalized
10.5%
Post-Hip Surgery19-32%
Admission
36%
Additional: Hospitalized 13-42%
AACN Hartford Faculty Development
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
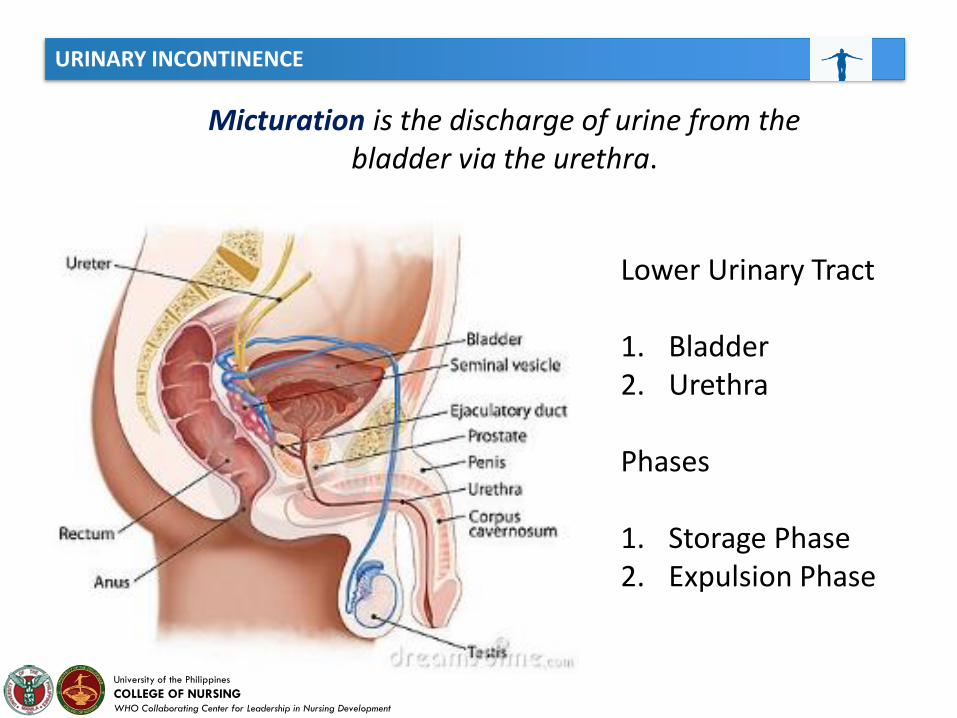
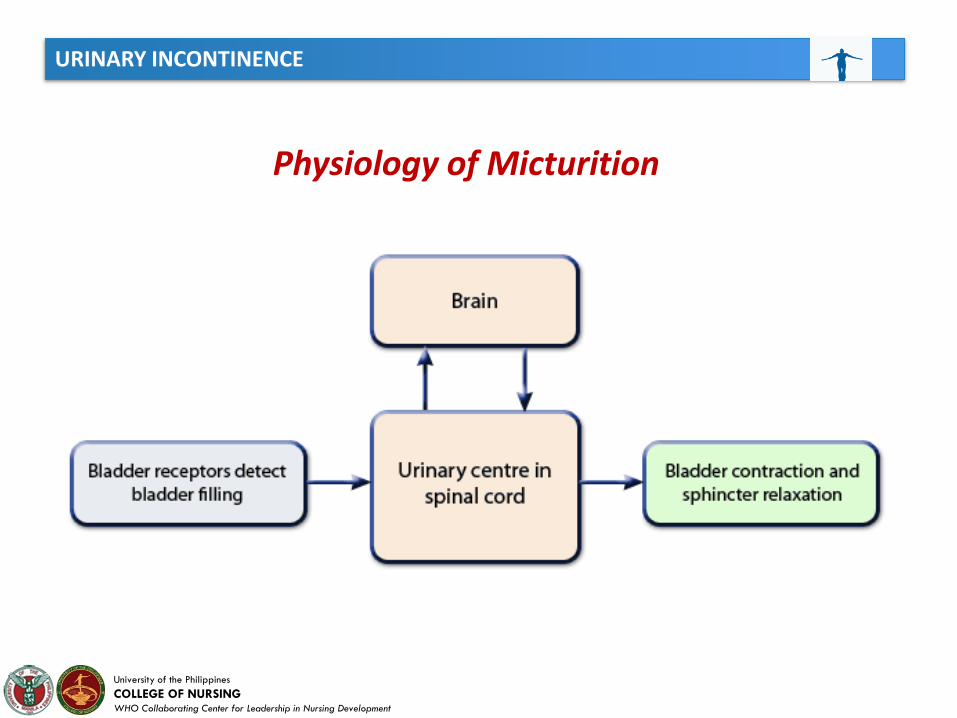
Micturation is the discharge of urine from the bladder via the urethra.
Lower Urinary Tract
1. Bladder2. Urethra
Phases
1. Storage Phase2. Expulsion Phase
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Physiology of Micturition
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
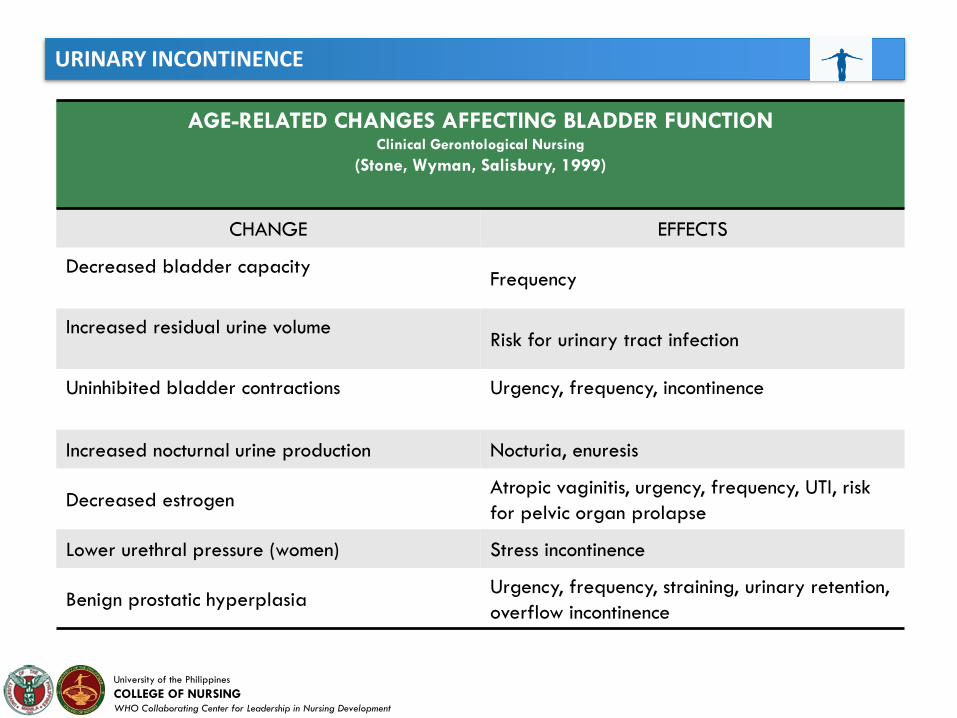
AGE-RELATED CHANGES AFFECTING BLADDER FUNCTIONClinical Gerontological Nursing
(Stone, Wyman, Salisbury, 1999)
CHANGE EFFECTS
Decreased bladder capacityFrequency
Increased residual urine volumeRisk for urinary tract infection
Uninhibited bladder contractions Urgency, frequency, incontinence
Increased nocturnal urine production Nocturia, enuresis
Decreased estrogenAtropic vaginitis, urgency, frequency, UTI, risk
for pelvic organ prolapse
Lower urethral pressure (women) Stress incontinence
Benign prostatic hyperplasiaUrgency, frequency, straining, urinary retention,
overflow incontinence
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
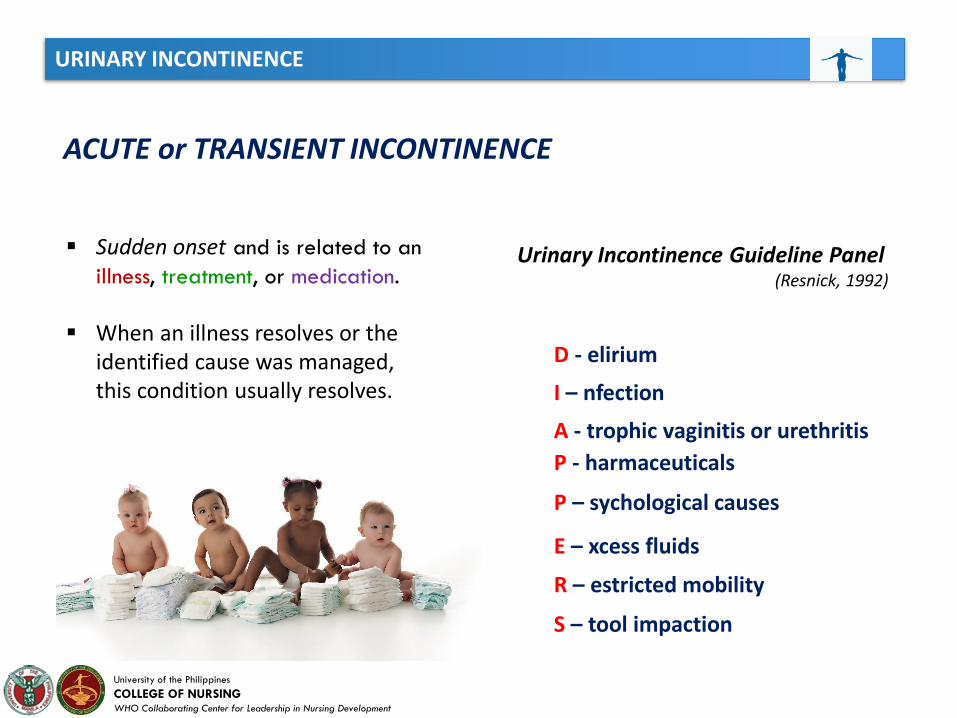
ACUTE or TRANSIENT INCONTINENCE
Sudden onset and is related to an
illness, treatment, or medication.
When an illness resolves or the identified cause was managed, this condition usually resolves.
D - elirium
I – nfection
A - trophic vaginitis or urethritis
P - harmaceuticals
P – sychological causes
E – xcess fluids
R – estricted mobility
S – tool impaction
Urinary Incontinence Guideline Panel(Resnick, 1992)

URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
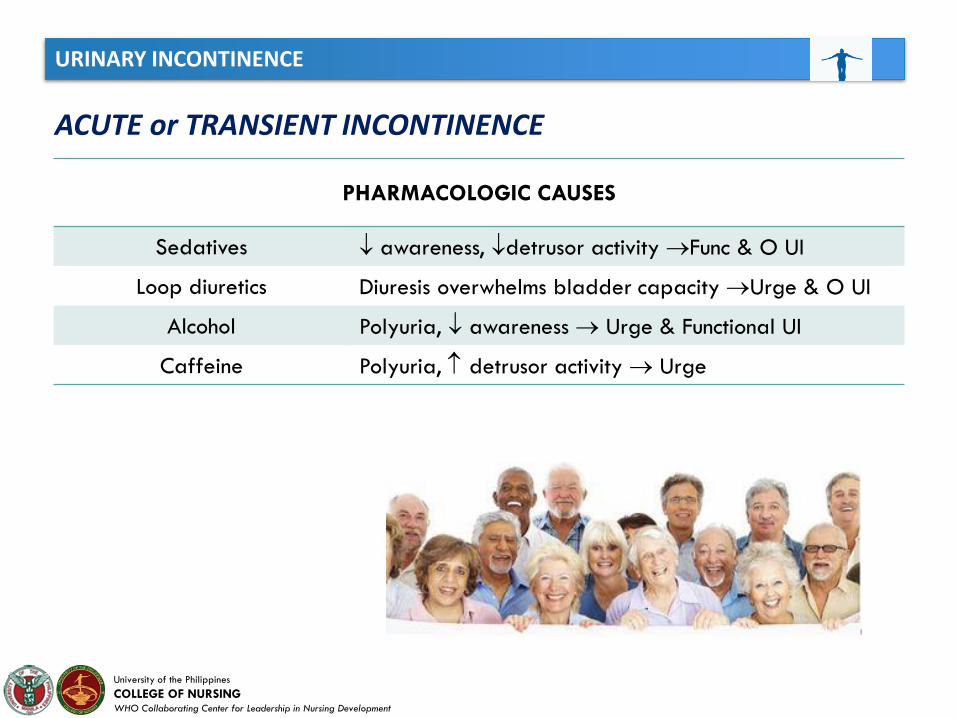
ACUTE or TRANSIENT INCONTINENCE
PHARMACOLOGIC CAUSES
Opiods
Depress detrusor activity &
produce urinary retention
and overflow incontinence
Calcium Channel Blockers
Anti-Parkinsons Drugs
Anticholinergic Drugs
Prostaglandin Inhibitors
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
ACUTE or TRANSIENT INCONTINENCE
PHARMACOLOGIC CAUSES
Sedatives awareness, detrusor activity Func & O UI
Loop diuretics Diuresis overwhelms bladder capacity Urge & O UI
Alcohol Polyuria, awareness Urge & Functional UI
Caffeine Polyuria, detrusor activity Urge
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
ESTABLIHED INCONTINENCE or PERSISTENT URINARY INCONTINENCE
Stress Incontinence
Urge Incontinence
Mixed Incontinence
Overflow Incontinence
Functional Incontinence
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
STRESS URINARY INCONTINENCE (SUI)
Characterized by loss of small amount of urine in the absence of detrusorcontraction usually during sudden increase in intraabdominal pressure such aswith:
Coughing Sneezing Laughing Lifting Bending
The underlying cause is the inability of the urethra to sustain pressure that exceeds that of the bladder,
particularly under EXERTIONAL EVENTS
(Diokno et al., 1986; Fantl et al., 1991; Makinen et al., 1992)
*more frequent in WOMEN than in MEN
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
URGE INCONTINENCE
Involuntary loss of urine in association with a strong sensation of urinaryurgency. This type of incontinence is characterized by strong urge to voidimmediately prior to the loss of the urine. (Stone, Wyman, Salisbury, 1999)
Results from:
detrusor (bladder) instability Hyperreflexia uninhabited bladder contractions
“KEY-IN-LOCK” SYNDROME
they loss urine in arriving home andunlocking their door.
It may include urine loss on the wayto the bathroom or the "key in thelock“ or "hand on the doorknob"syndrome (no urge to urinate untilthe key is in the doorlock or thehand is on the knob and then it isimpossible to wait).
womensbladderhealth.com
OVERACTIVEBLADDER
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
MIXED INCONTINENCE
Combination of STRESS andURGE INCONTINENCE
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
FUNCTIONAL INCONTINENCE
This pattern of urine loss is precipitated by factors outside the lower urinary tract, rather than abnormal bladder or urethral function
(Stone, Wyman, Salisbury, 1999)
(Malone, Fletcher, Plank, 2004)
Characterized by inability to get into the toilet on time as a result of the following:
1. physical impairments2. chronic cognitive impairments3. environmental or physical barriers4. or the lack of caregiving assistance
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
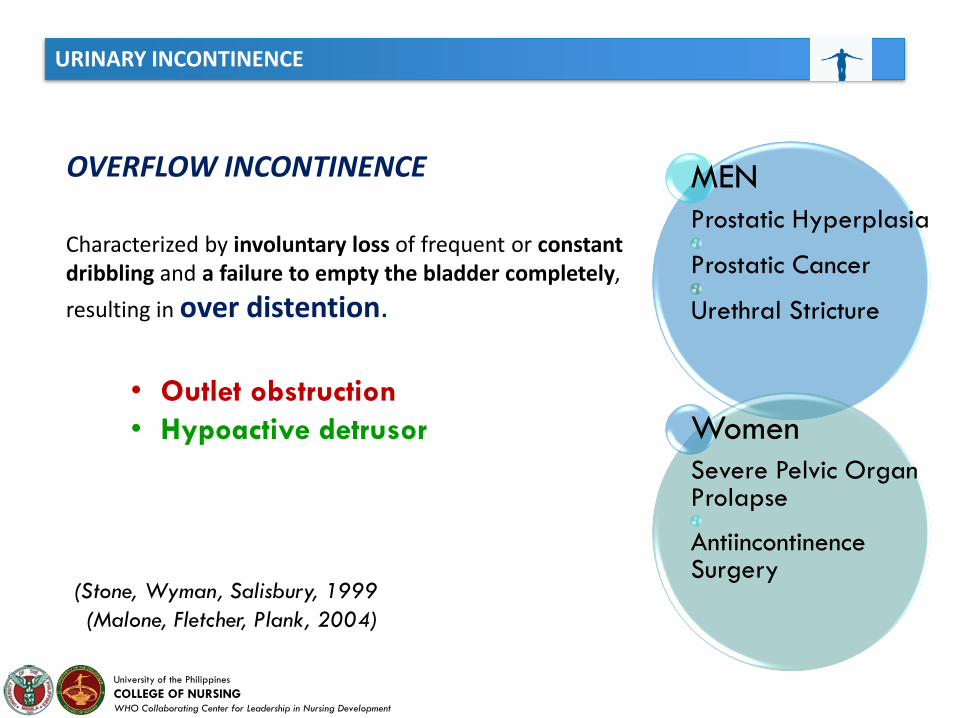
OVERFLOW INCONTINENCE
Characterized by involuntary loss of frequent or constant dribbling and a failure to empty the bladder completely,
resulting in over distention.
• Outlet obstruction
• Hypoactive detrusor
MEN
Prostatic Hyperplasia
Prostatic Cancer
Urethral Stricture
Women
Severe Pelvic Organ Prolapse
AntiincontinenceSurgery
(Stone, Wyman, Salisbury, 1999
(Malone, Fletcher, Plank, 2004)
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
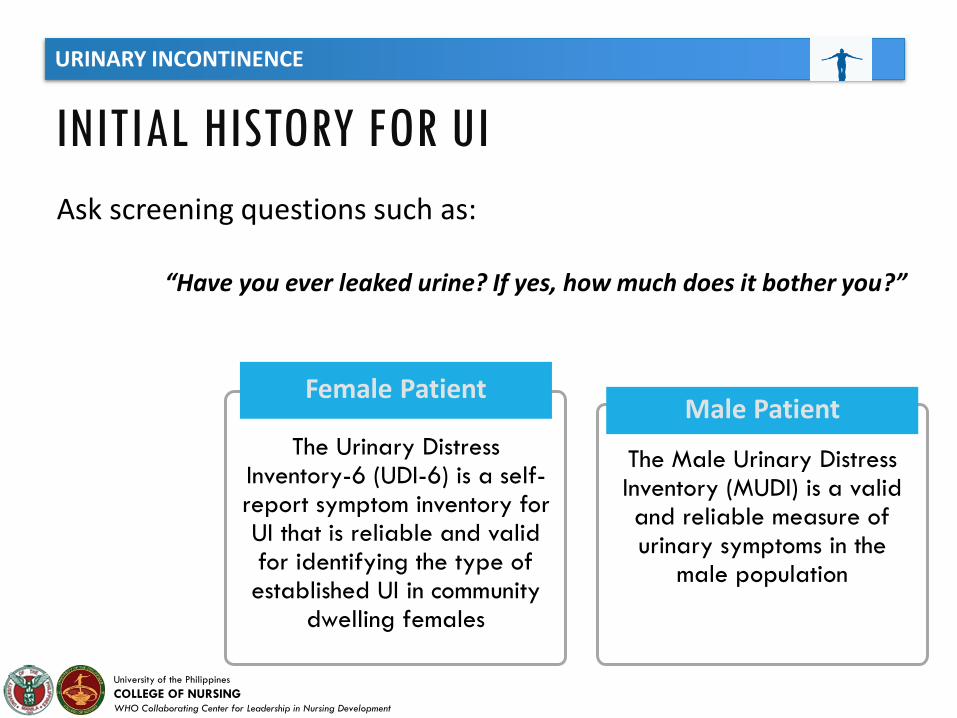
The Urinary Distress Inventory-6 (UDI-6) is a self-report symptom inventory for UI that is reliable and valid for identifying the type of established UI in community
dwelling females
Female Patient
The Male Urinary Distress Inventory (MUDI) is a valid and reliable measure of urinary symptoms in the
male population
Male Patient
INITIAL HISTORY FOR UI
Ask screening questions such as:
“Have you ever leaked urine? If yes, how much does it bother you?”
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
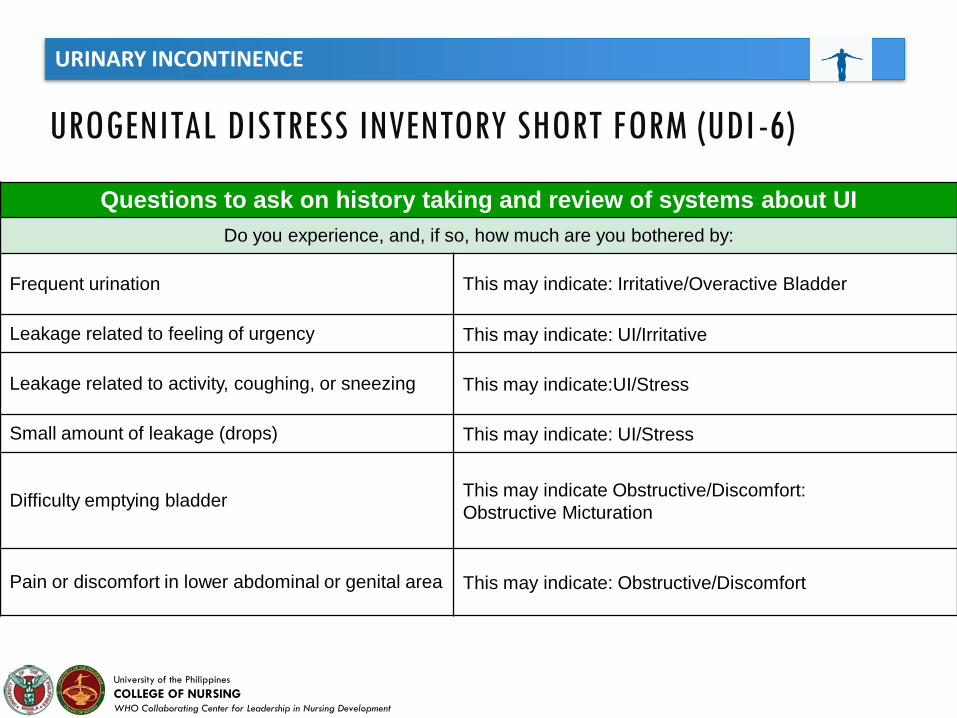
UROGENITAL DISTRESS INVENTORY SHORT FORM (UDI -6)
Questions to ask on history taking and review of systems about UI
Do you experience, and, if so, how much are you bothered by:
Frequent urination This may indicate: Irritative/Overactive Bladder
Leakage related to feeling of urgency This may indicate: UI/Irritative
Leakage related to activity, coughing, or sneezing This may indicate:UI/Stress
Small amount of leakage (drops) This may indicate: UI/Stress
Difficulty emptying bladderThis may indicate Obstructive/Discomfort:
Obstructive Micturation
Pain or discomfort in lower abdominal or genital area This may indicate: Obstructive/Discomfort
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
INITIAL HISTORY FOR UI
• Differentiate between transient and established UI because transientUI may convert to persistent UI
• The seven-day bladder diary or record is the most evaluated andrecommended tool to quantify UI and identify activities associatedwith unwanted urine loss
• A three-day bladder diary may be more feasible in the clinical setting
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
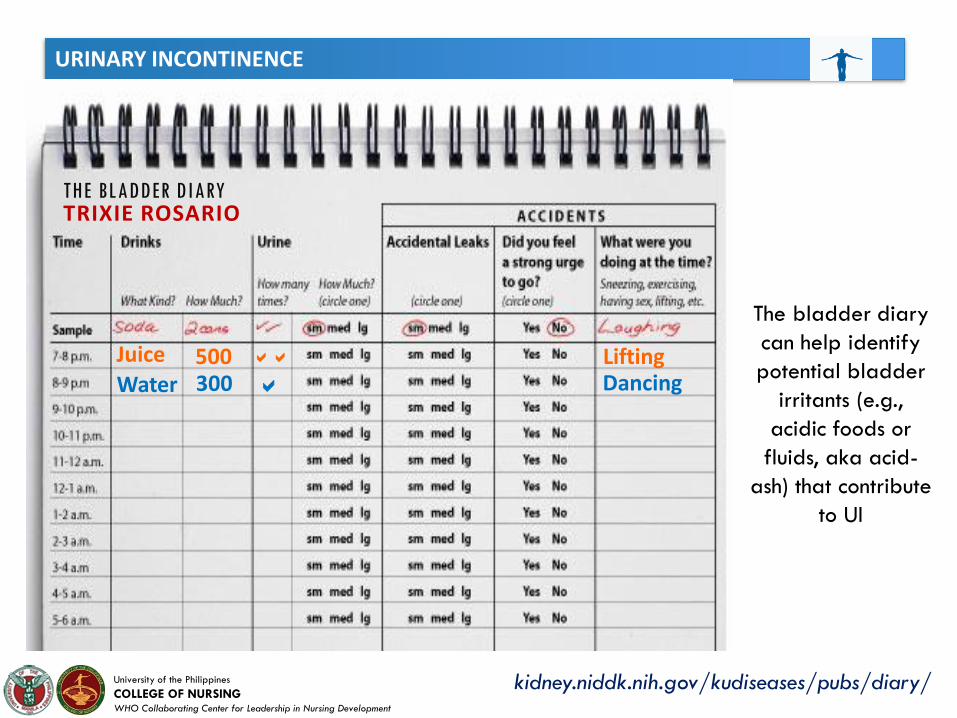
kidney.niddk.nih.gov/kudiseases/pubs/diary/
THE BLADDER DIARYTRIXIE ROSARIO
Juice 500 LiftingWater 300 Dancing
The bladder diary
can help identify
potential bladder
irritants (e.g.,
acidic foods or
fluids, aka acid-
ash) that contribute
to UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
THE BLADDER DIARY
• If the initial scheduled toileting time is set for 7 A.M., yet at 6:30 A.M. the patient consistently attempts to independently void or is noted to be incontinent, then the toileting time should be adjusted to 6 A.M.
• Prompted voiding requires the caregiver to ask if the patient needs to void, offer assistance, and then offer praise for successful voiding
Example
• To assess UI
• Develop an individualized scheduled toileting program
which mimics the patient’s normal voiding patterns
Continual assessment and evaluation improves success
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
PHYSICAL EXAM FOR UIObserve the patient during urination to determine ability to
remove undergarments, sit on toilet etc.
Abdominal exam:
• Determine the presence of bladder distention• Determine presence of stool impaction in left
quadrant
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Inspect male and female genitalia
*Note perineal irritation or long-standing pigmentation change, often indicative
urinary leakage
PHYSICAL EXAM FOR UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Valsalva maneuver (if not medically contraindicated) to detect pelvicprolapse (e.g., cystocele, rectocele, uterine prolapse) or urine leakage(suggestive of stress UI), as a result of increased intra-abdominal pressurewith bearing down
• Ask the patient to cough while observing for urinary leakage, especially important when performing a “Valsalva” maneuver is contraindicated
• During the genitalia examination, instruct the patient to cough while assessing for urine leakage that may be attributed to Stress UI
Female Patient
PHYSICAL EXAM FOR UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Look for signs of atrophic vaginitis post-menopausal women
1. Perineal inflammation
2. Tenderness and, on occasion, trauma as a result of touch)
3. Thin, pale genitalia tissues that are often friable and prone to bleeding
Perform digital rectal exam to identify constipation or fecal impaction
PHYSICAL EXAM FOR UI
Women
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
PHYSICAL EXAM FOR UI
Assess for “anal wink” (contraction of the external anal sphincter) by lightly stroking the circumanal skin.
• Indicative of intact sacral nerve routes• Absence of the “anal wink” may
suggest sphincter denervation
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
PHYSICAL EXAM FOR UI
Men
In men, palpate the prostate gland.
• Typically an enlarged prostate is readily detected andcorrelates with symptoms of:
1. urinary urgency2. incomplete bladder emptying3. decreased urinary stream4. nocturia
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
LAB TESTS FOR UI
Urinalysis and/ urine culture and sensitivity
Post void residual urine or simple bedside urodynamics
The International Continence Society (ICS) does not recommend urodynamic testing in the initial assessment and management of UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
TREATMENT VS REFERRAL
Initiate referral if any of the following apply:
Need for additional testing
Abnormal U/A or culture
Palpable abdominal or pelvic mass
Elevated PVR
Abnormal prostate exam
Vaginal bleeding; obstruction; new underlying disorder; surgical candidate
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
BEHAVIORAL MANAGEMENT
Scheduling Regimen
Scheduling regimens include:
• timed voiding• habit training• prompted voiding• bladder training
Success of this regimens when used in institutionalized patients relies on staff member’s training, compliance, and incentives for active participation. Thus, it is important to develop management
procedures to monitor the staff implementation of toileting interventions and to provide feedback about the performance (Schnelle, 1990).
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
BEHAVIORAL MANAGEMENT
TIME VOIDING
The fixed voiding schedule usually every 2 hours is used for:
• Stress UI• Overflow UI• Functional UI• Reflex UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
BEHAVIORAL MANAGEMENT
HABIT TRAINING
This is carried out through individualized and prescribed toileting schedule which involves toileting intervals adjusted to the patient’s voiding pattern.
• Stress UI• Urge UI• Functional UI• Reflex UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
BEHAVIORAL MANAGEMENT
PROMTED VOIDING
It consists 3 elements used by caregivers:
1. Monitoring the patient on regular basis2. Prompting the patient to try to use the toilet3. Praising the patient for maintaining continence and using the toilet
Prompted voiding is recommended for patients who can:
1. Ask assistance2. Respond when prompted to toilet3. Learn to recognize some degree of bladder fullness or need to void
(Fantl et al., 1996)
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
BEHAVIORAL MANAGEMENT
(Fantl et al., 1996)
BLADDER TRAINING
This technique consists of a:
• patient education in combination• progressive voiding schedule• positive reinforcement technique
It is usually used to treat outpatients who are cognitively intact and have Sx of:
• Urge UI• Stress UI• Mixed UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Kegel’s exercises
RATIONALE: PFMEs facilitate continence by increasing strength, endurance, and contractibility of the pelvic muscles, which
support the bladder neck, contribute to optimal anatomical positioning of the urethra, and facilitate neuromuscular control
necessary for continence
MenDuring the rectal
examination, male patients are instructed to squeeze
the rectal muscles
WomenTeach PFMEs during the pelvic
examination
Instruct the patient to squeeze (contract) her vaginal muscles around the examiner’s gloved
hand
MANAGEMENT OF UI: PELVIC FLOOR MUSCLE EXERCISES (PFMES) FOR STRESS URINARY INCONTINENCE

URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Ideally, each PFME should consist of a contraction lasting for 10 seconds,
followed by a relaxation period of 10 seconds
MANAGEMENT OF UI: PELVIC FLOOR MUSCLE EXERCIZES (PFMES) FOR STRESS UI
Patient should be instructed to avoidcontracting abdominal, buttocks, or
thigh muscles so as to not increase intra-abdominal pressure.
While there are variations on the number of PFME per day required, it is usual
practice to recommend 15 PFMEs three times per day
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
PFMEs may cause neuromuscular changes that promote a decrease in the autocontractility of the bladder,
thereby inhibiting the urge to urinate
There is evidence that PFMEs decrease incontinent episodes related to urge UI
(Bradway & Castronovo, 2015)
Available at: http://consultgerirn.org/uploads/File/aprncenter/slidelibrary/APRN-SlideLib_UI.ppt
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Urine stream interruption test (UST)
• is a simple measure of pelvic floor muscle
strength and provides a numerical value to
supplement data collection
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Patients may need several weeks to note improvement in bladder control
Once patients are confident with performing PFMEs they may benefit from “The Knack”
WomenUST should be under two
seconds in women reporting significantly fewer UI
episodes
MenUST is currently being tested
in a male sample
Urine stream interruption test (UST)
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Occlusive and Pelvic support devices
Surgical procedures
OTHER MANAGEMENT OF STRESS UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
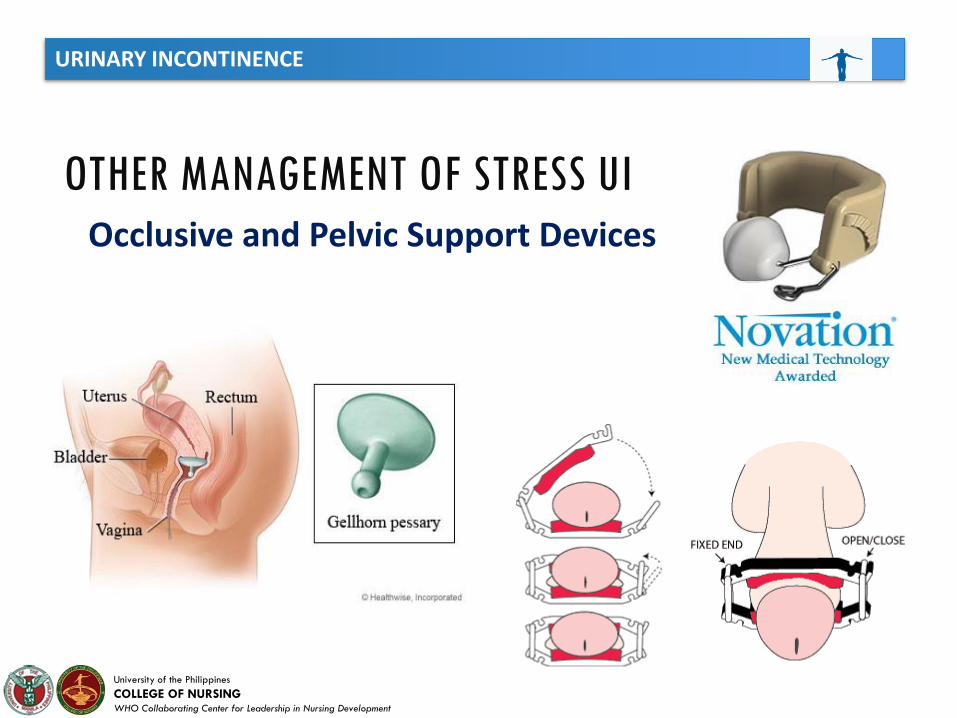
Occlusive and Pelvic Support Devices
OTHER MANAGEMENT OF STRESS UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Surgery
OTHER MANAGEMENT OF STRESS UI
Surgery is indicated in the treatment of stress
incontinence, overflow incontinence secondary to
Anatomical obstruction, and urge incontinence
secondary to lower urinary tract pathology. (e.g.
bladder stone, tumor, or diverticulum).
Augmentation Cystoplasty
• the surgery most often performed for severe urge incontinence.
• a part of the bowel is added to the bladder
Sacral Nerve Stimulation
• is a newer type of surgery. A small unit is implanted under your skin
• This sends small electrical pulses to the sacral nerve (one of the nerves that comes out at the base of your spine)
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
• oxybutynin (Ditropan®)
• tolterodine (Detrol®)
• darifenacin (Enablex®)
• trospium chloride (Sanctura ®),
• solifenacin succinate (Vesicare ®)
Long-acting formulations, transdermal patch preparations, and lower dose preparations are available.
MANAGEMENT FOR UI: MEDICATIONSAvailable Medications
Anticholinergic
(antimuscarinic)/antispasmodic
• This medications are commonly
prescribed for urge UI and OAB
because they reduce detrusor
overactivity and spasm, and in turn,
decrease urinary urgency, frequency,
and urge UI If prescribed, the nurse
should assess the patient for common
side effects
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
ENVIRONMENTAL MANAGEMENT
Environment plays a vital role in managing functional UI
Incontinence
• Individuals are often dependent on adaptive devices
(e.g., walker) or caregivers for assistance with voiding
• Facilitate access to toilets or toileting substitute may
prevent or reduce functional incontinence (urinal,
commode, bedpan)
• Wearing loosely fitting cloths with elastic waistbands
or snap or Velcro fasteners facilitates disrobing for
those patients with manual dexterity problems.
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Strategies specific to manage overflow UI include PFMEs if it is determined that bladder outlet obstruction is due to persistent contraction of the pelvic floor muscles
Interventions to manage overflow UI:
1. Crede’s maneuver
2. Timed voiding
3. Double voiding
4. Intermittent urinary catheterization
MANAGEMENT: OVERFLOW UI
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
MANAGEMENT: OVERFLOW UI
Crede’s maneuver: Cautiously used and requires manual
compression over the suprapubic area during bladder
emptying
Avoid: If vesicoureteral reflux or overactive sphincter
mechanisms are suspected as the Crede’s maneuver would
dangerously elevate pressure within the bladder
Double Void: Repositioning to void again directly after
the initial void.
For a patient with overflow UI the APRN should evaluate if medications
may be causing urinary retention
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
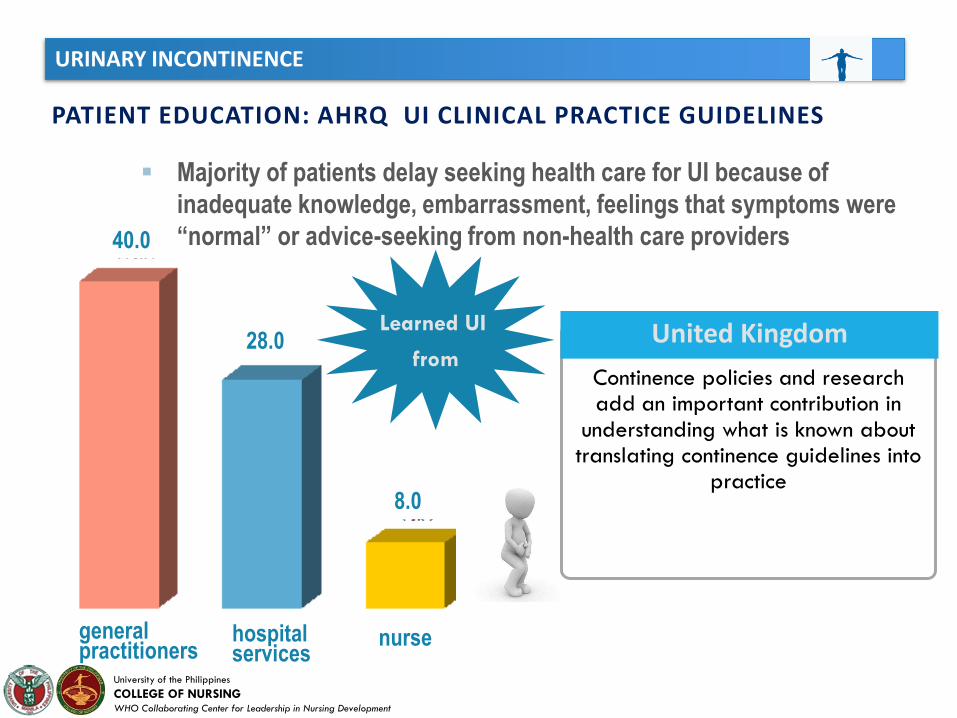
PATIENT EDUCATION: AHRQ UI CLINICAL PRACTICE GUIDELINES
Majority of patients delay seeking health care for UI because of
inadequate knowledge, embarrassment, feelings that symptoms were
“normal” or advice-seeking from non-health care providers
Continence policies and research add an important contribution in
understanding what is known about translating continence guidelines into
practice
United Kingdom
general practitioners
hospital services
nurse
Learned UI
from
40.0
28.0
8.0
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Work closely with older adults who fear that unwanted urine loss results from increased fluid intake
1. Focus education on the adverse consequence of inadequate fluid intake such as volume depletion, or potential for dehydration.
2. Emphasize that too little fluid intake causes urine to become concentrated which in turn, leads to increased bladder contractions and feelings of urinary urgency
3. To manage and limit nocturia, advise to limit fluid intake a few hours before bedtime
PATIENT EDUCATION: FLUID INTAKE
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
1. Examine and discuss medications contributing to UI with the prescribing health care provider
2. Determine the necessity of the medication or ideal scheduling to promote continence
PATIENT EDUCATION: MEDICATIONS
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
NURSING IMPLICATIONS/CONSIDERATIONS
1. Teach pelvic floor muscle exercises (DuBeau et al, 2010; Hodgkinson et al., 2008).
2. Provide toileting assistance and bladder training PRN (whenever necessary) (DuBois et al., 2010).
3. 3. Consider referral to other team members if pharmacological or surgical therapies are warranted.
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
NURSING IMPLICATIONS/CONSIDERATIONS
Overflow UI:
1. Allow sufficient time for voiding.
2. Discuss with interdisciplinary team the need for determining a post-void
residual (PVR) (Newman & Wein, 2009).
3. Instruct patients in double voiding and Crede’s maneuver.
4. If catheterization is necessary, sterile intermittent is preferred over
indwelling catheterization PRN.
5. Initiate referrals to other team members for those patients requiring
pharmacological or surgical intervention.
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
NURSING IMPLICATIONS/CONSIDERATIONS
Urge UI and OAB:
1. Implement bladder training (retraining) (DuBeau et al., 2010).
2. If patient is cognitively intact and is motivated, provide information on urge
inhibition.
3. Teach PFMEs to be used in conjunction with bladder training, and instruct in urge
inhibition strategies (Rathnayake, 2009)
4. Collaborate with prescribing team members if pharmacologic therapy is
warranted.
5. Initiate referrals for those patients who do not respond to the previous steps.
URINARY INCONTINENCE
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
NURSING IMPLICATIONS/CONSIDERATIONS
Functional UI:
1. Provide individualized, scheduled toileting, timed voiding, or
prompted voiding (Lee et al., 2009).
2. Provide adequate fluid intake.
3. Refer for physical and occupational therapy PRN.
4. Modify environment to maximize independence with
continence (Jirovec et al., 1988).
Pressure UlcersGeriatric Syndrome
Alfie R. Espinosa, RNInfection Control Officer
Perioperative Nurse
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
National Pressure Ulcer Advisory Panel (NPUAP) and
European Pressure Ulcer Advisory Panel (EPUAP):
"A pressure ulcer is localized injury to the skin and/or
underlying tissue, usually over a bony prominence, as a result
of pressure, or pressure in combination with shear. A number
of contributing or confounding factors are also associated with
pressure ulcers; the significance of these factors is yet to be
elucidated.“
Also known as DECUBITUS ULCERS
WHAT IS PRESSURE ULCER?

PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
ETIOLOGY
It is generally accepted that pressure ulcers are causally related to the effects of 3 tissue forces: pressure, shear, and friction.
Pressure is a perpendicular force that compresses tissues,typically between a bony prominence and an externalsurface, and can result in decreased tissue perfusion andischemia. Tissue necrosis can result when there is unrelievedpressure or ischemia that is potentiated by compromisedhost (eg, chronic medical conditions, protein-energymalnutrition, or sepsis).
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Shear is a force parallel to the skin surface. When thehead of the bed is raised or a patient slides downwardin a chair, the body is angulated above the supportsurface, causing skeletal muscle and deep fascia toslide downward with gravity while the skin andsuperficial tissues adhere to the chair surface or bedlinens.
This shear force can cause a change in the angle of the vessels, and thus, compromise blood supply, resulting in
ischemia, cellular death, and tissue necrosis.
ETIOLOGY
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Friction is the adherent force resisting shearingmovement of the skin, which may result in denudedareas of the dermis through repeated epidermalshedding or avulsion of sheets of epidermis.
Prolonged exposure of this tissue injury to moisture from perspiration, urinary or fecalincontinence, or wound exudate will further
weaken the intercellular bonds in the epidermal layers, causing maceration and
epidermal ulceration$
ETIOLOGY
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
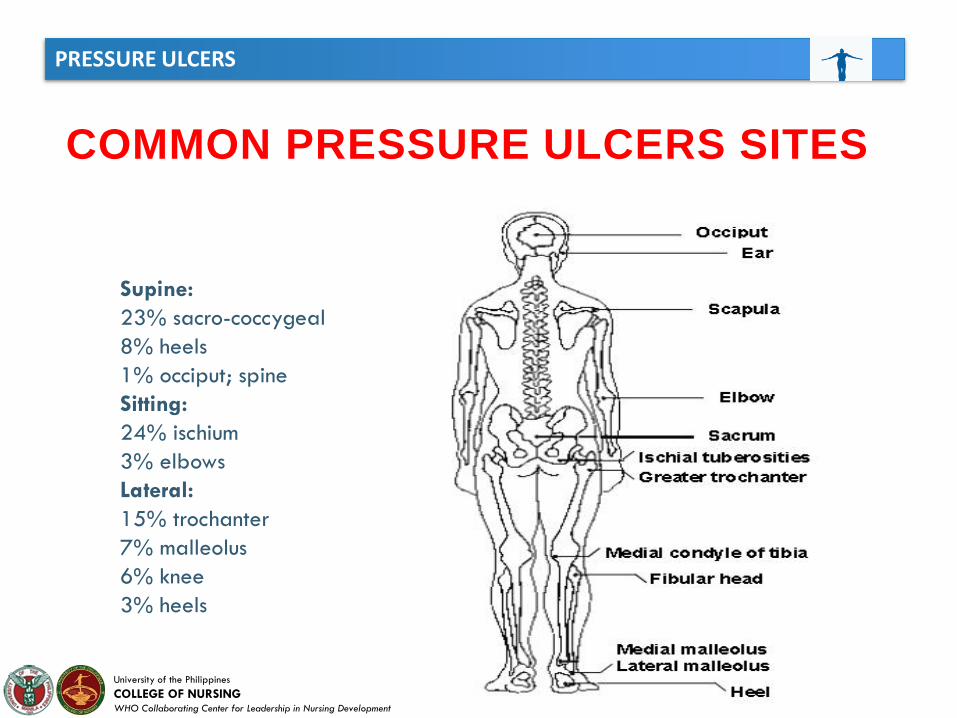
COMMON PRESSURE ULCERS SITES
Supine:
23% sacro-coccygeal
8% heels
1% occiput; spine
Sitting:
24% ischium
3% elbows
Lateral:
15% trochanter
7% malleolus
6% knee
3% heels
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
According to the NPUAP and EPUAP, there are 6 categories of pressure ulcers.
NPUAP refers to these categories as stages and EPUAP refers to them as grades.
Only the numbered categories (I through IV) represent increasing degrees of skin
and tissue damage. Two other categories are qualitative descriptors that do not
necessarily reflect the severity of the ulcer.
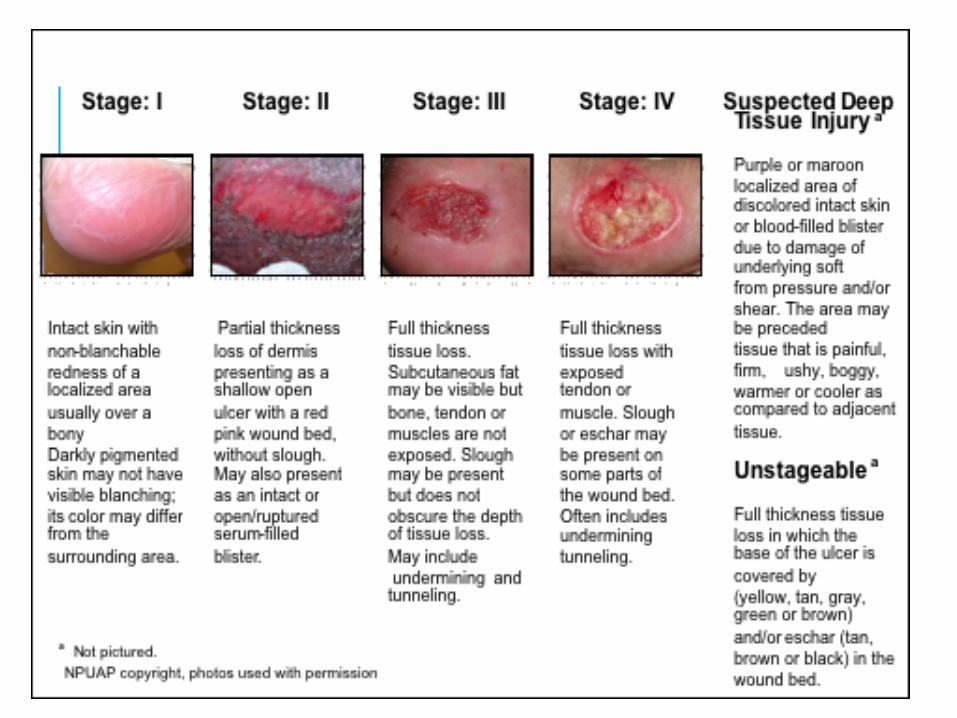
The classification system:
• Category I – Nonblanchable erythema
• Category II – Partial-thickness skin loss
• Category III – Full-thickness skin loss
• Category IV – Full-thickness tissue loss
• Suspected Deep Tissue Injury – Depth unknown
• Unstageable – Depth unknown
CLASSIFICATION OF PRESSURE ULCERS
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
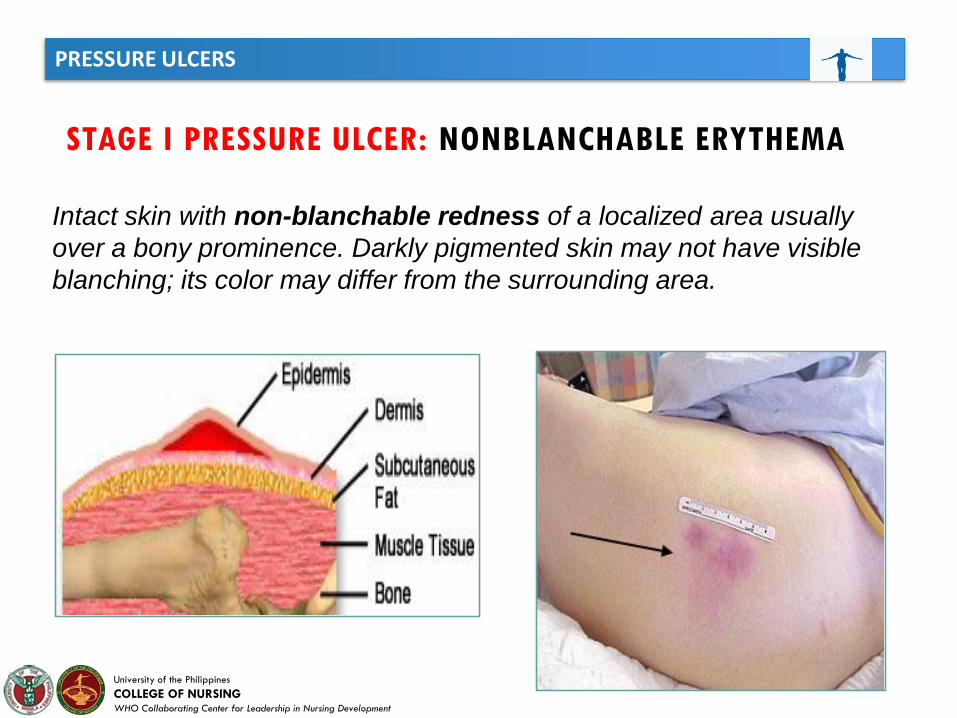
STAGE I PRESSURE ULCER: NONBLANCHABLE ERYTHEMA
Intact skin with non-blanchable redness of a localized area usually
over a bony prominence. Darkly pigmented skin may not have visible
blanching; its color may differ from the surrounding area.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
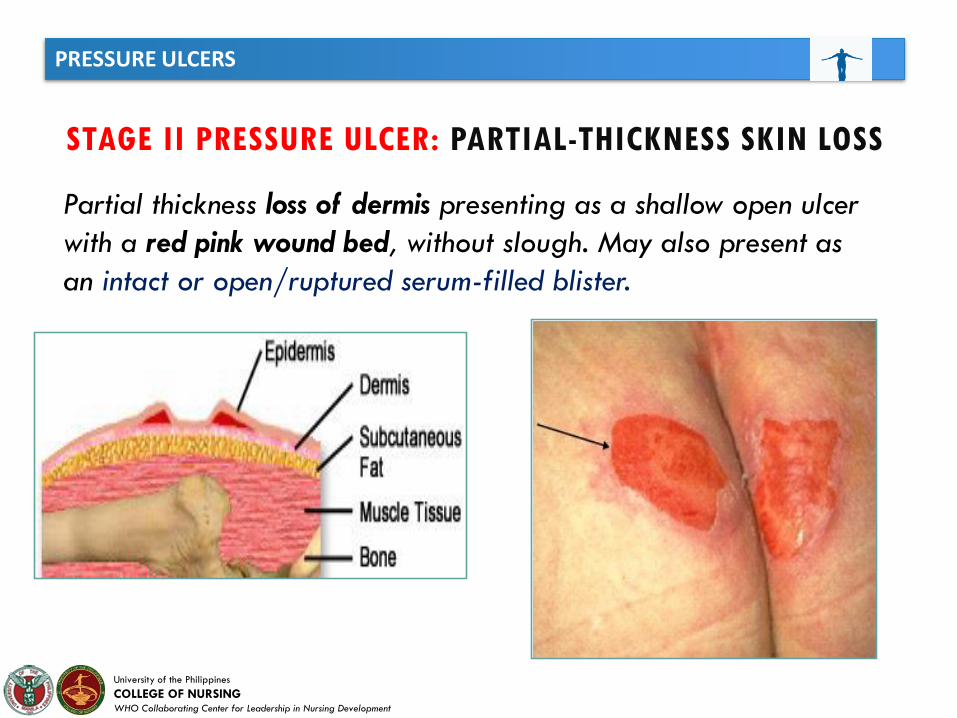
STAGE II PRESSURE ULCER: PARTIAL-THICKNESS SKIN LOSS
Partial thickness loss of dermis presenting as a shallow open ulcer
with a red pink wound bed, without slough. May also present as
an intact or open/ruptured serum-filled blister.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
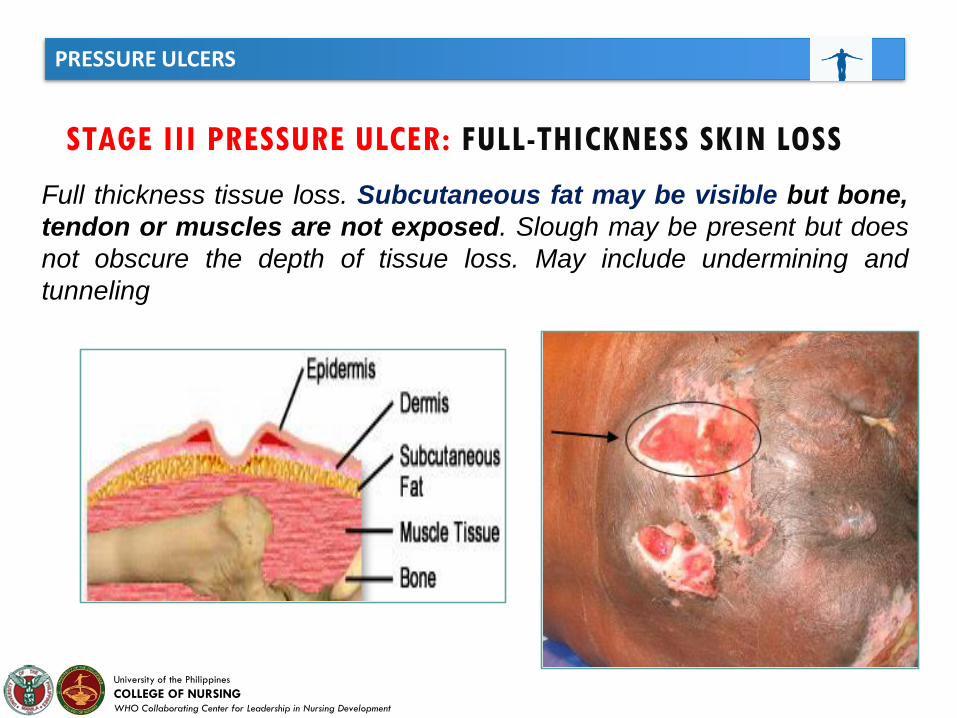
STAGE III PRESSURE ULCER: FULL-THICKNESS SKIN LOSS
Full thickness tissue loss. Subcutaneous fat may be visible but bone,
tendon or muscles are not exposed. Slough may be present but does
not obscure the depth of tissue loss. May include undermining and
tunneling
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
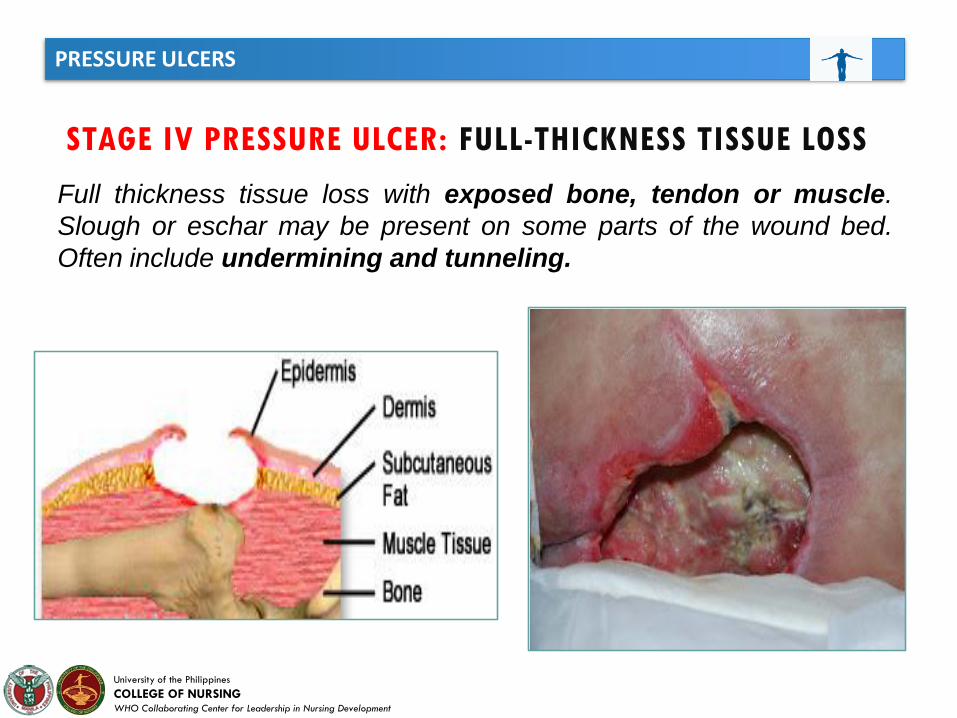
STAGE IV PRESSURE ULCER: FULL-THICKNESS TISSUE LOSS
Full thickness tissue loss with exposed bone, tendon or muscle.
Slough or eschar may be present on some parts of the wound bed.
Often include undermining and tunneling.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
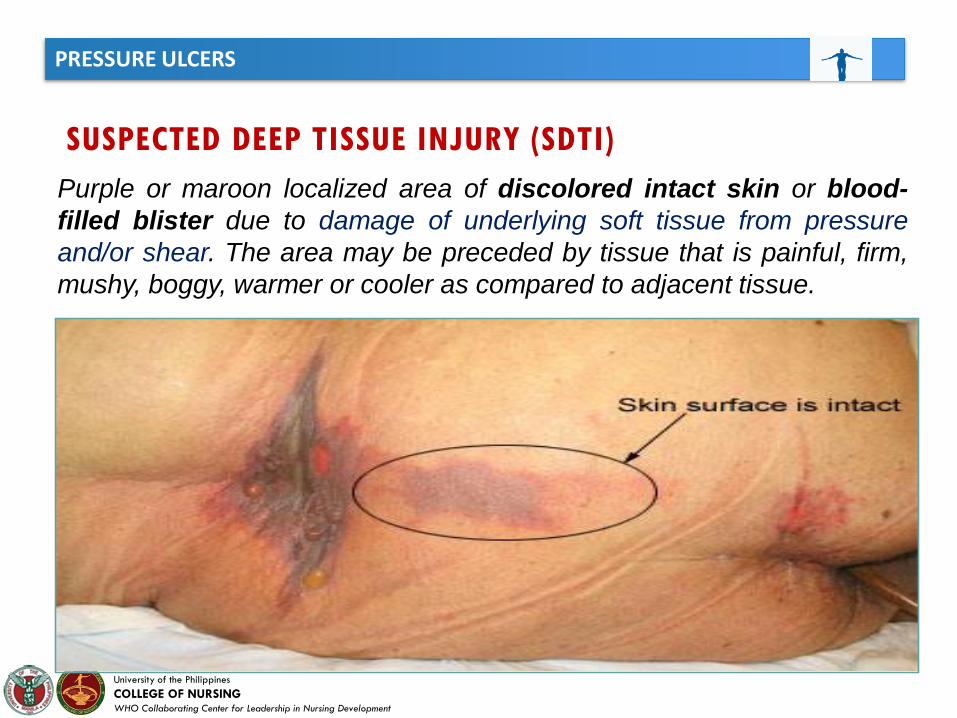
SUSPECTED DEEP TISSUE INJURY (SDTI)
Purple or maroon localized area of discolored intact skin or blood-
filled blister due to damage of underlying soft tissue from pressure
and/or shear. The area may be preceded by tissue that is painful, firm,
mushy, boggy, warmer or cooler as compared to adjacent tissue.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
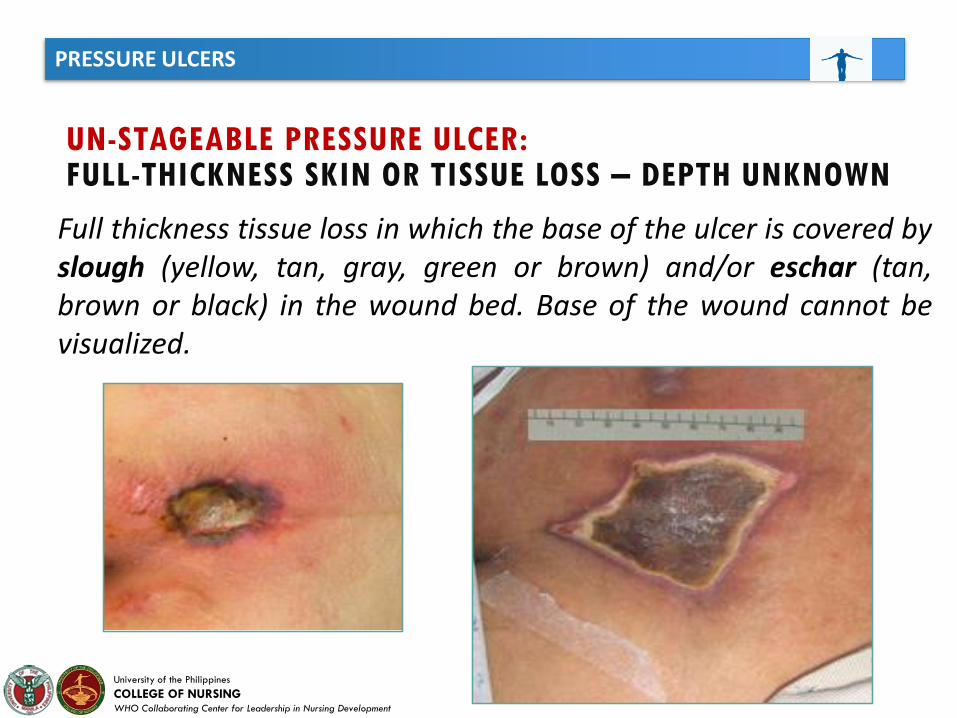
UN-STAGEABLE PRESSURE ULCER:FULL-THICKNESS SKIN OR TISSUE LOSS – DEPTH UNKNOWN
Full thickness tissue loss in which the base of the ulcer is covered byslough (yellow, tan, gray, green or brown) and/or eschar (tan,brown or black) in the wound bed. Base of the wound cannot bevisualized.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
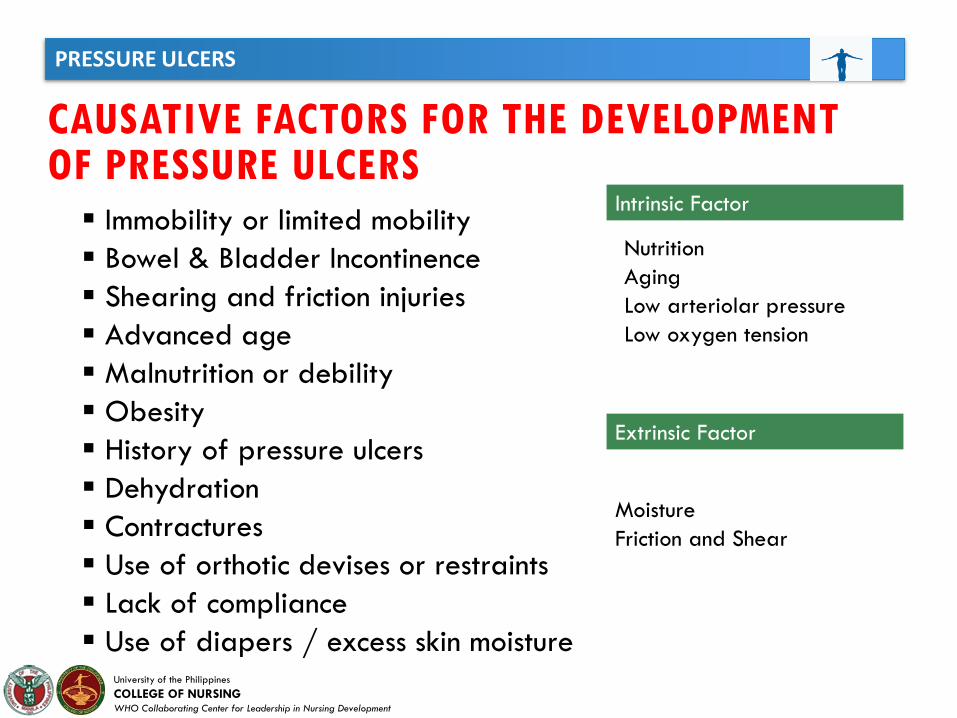
CAUSATIVE FACTORS FOR THE DEVELOPMENT OF PRESSURE ULCERS
Immobility or limited mobility
Bowel & Bladder Incontinence
Shearing and friction injuries
Advanced age
Malnutrition or debility
Obesity
History of pressure ulcers
Dehydration
Contractures
Use of orthotic devises or restraints
Lack of compliance
Use of diapers / excess skin moisture
Intrinsic Factor
Nutrition
Aging
Low arteriolar pressure
Low oxygen tension
Extrinsic Factor
Moisture
Friction and Shear
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
PRESSURE ULCER PREVENTION / NURSING INTERVENTIONS
Turn every 2 hours (q2h) Schedule: e.g. alternating positions Right/Back/Left
q2h. May place pillow under one hip at a time if patient cannot tolerate full
turning.
Maximal Remobilization: Passive range of motion, physical therapist (PT)
consult to plan appropriate measures for patient. Spinal Cord Injury and Disorder
(SCI&D) patients (or any patient with custom chairs) are to sit in their own
wheelchairs and cushions only.
Protect Heels: Support entire leg with pillows to allow heels to suspend above
the mattress or use heel protectors. Assess heels everyday for signs of pressure.
Consider pressure relieving / distribution bed surface.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Manage Moisture: Correct cause, (e.g., diarrhea), reduce or eliminate
incontinent episodes (e.g., bladder training); Use mild soap, rinse, and dry skin
well and apply moisture barrier cream. No diapers while patient in bed.
Manage Nutrition: Increase protein intake more than 100% RDA, if not
renal or liver impaired. Dietary consult to determine dietary needs and/or
effectiveness of tube feedings.
Reduce Friction and Shear: Use bed trapeze or pull sheet for lifting and
moving patient up in bed. Apply transparent film or hydrocolloid dressing
(Duoderm) over friction areas (e.g., elbows) Keep the head of the bed less
than 30 degrees as often as possible.
PRESSURE ULCER PREVENTION / NURSING INTERVENTIONS
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
MANAGEMENT OF STAGE- I
Stage I on Trunk of the Body
Manage incontinence, keeping area clean and dry.
Use moisture barrier cream PRN.
Off load area of pressure ulcer with pressure reducing / distribution
surface and turning and repositioning schedule.
Stage I on Heels
Ensure that heel(s) are floated at all times with frequent monitoring.

University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
MANAGEMENT OF STAGE- II
Dry Wound Bed
Cleanse with normal saline, apply small amount of hydrogel
and cover with non adherent dressing, change every day.
Off load area of pressure ulcer with pressure reducing /
distribution surfaces and turning and repositioning schedule.
Minimal Drainage
Cleanse with normal saline, apply hydrocolloid dressing
every three days and PRN soiling or dislodging. Monitor
placement every day.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
MANAGEMENT OF STAGE- III
Minimal Drainage and Clean Wound Bed
Cleanse with normal saline, apply small amount of hydrogel
and cover with non adherent dressing change every day.
Off load area of pressure ulcer with pressure relieving /
distribution surface and turning and repositioning schedule.
Presence of Slough with drainage
Sharp debridement / Enzymatic debridement
Use Foam or Calcium Alginate dressing for moderate to copious
drainage management.
Slough 30% or less in the wound, negative pressure wound
therapy is preferred treatment.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
MANAGEMENT OF STAGE- IVMinimal Drainage and Clean Wound Bed
Cleanse with normal saline, apply hydrogel and cover with
non adherent dressing change every day.
Off load area of pressure ulcer with pressure relieving
surface and turning and repositioning schedule.
Presence of Slough with drainage
Sharp debridement / Enzymatic debridement
Use Foam or Calcium Alginate dressing for moderate to
copious drainage management.
Slough 30% or less in the wound, negative pressure wound
therapy is preferred treatment.
Tunneling and undermining shall be filled appropriately.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
MANAGEMENT OF SUSPECTED DEEP TISSUE INJURY
Cleanse with normal saline, apply foam dressing
change every day.
Off load area of pressure ulcer with pressure
relieving / distribution surface and turning and
repositioning schedule.
Use Foam dressing for drainage management.
Castor oil / Balsam / Peru / Trypsin spray is the
preferred treatment.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
MANAGEMENT OF UN-STAGEABLE PRESSURE ULCERS
Cleanse with normal saline, apply hydrogel and cover with
non adherent dressing change every day.
Off load area of pressure ulcer with pressure relieving /
distribution surface and turning and repositioning schedule.
Use Foam dressing for drainage management.
Castor oil / Balsam / Peru / Trypsin spray is the preferred
treatment for wounds with Intact eschar.
Sharp or enzymatic debridement for the management of
slough.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
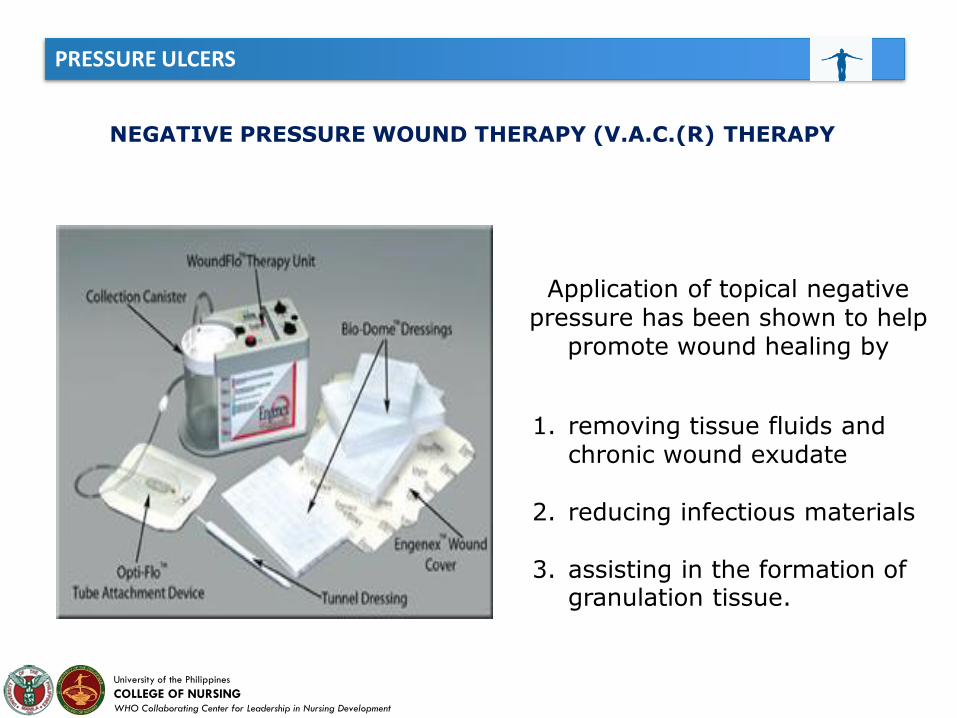
NEGATIVE PRESSURE WOUND THERAPY (V.A.C.(R) THERAPY
This negative pressure wound therapy consists of a specialized open cellfoam dressing, evacuation tubing, a fluid-collection canister, and a vacuumtherapy pump with adjustable settings and continuous feedbacktechnology. The foam dressing is cut to conform to the specific size andshape of the wound and is then placed into the wound cavity. Theevacuation tube is either inserted into or attached to the foam dressing sothat it exits parallel to the skin and the wound site. The foam dressing isthen covered with a thin adhesive film to create an airtight seal. Thisconverts the previously open wound to a controlled closed system. Afterthe wound is sealed, the proximal end of the evacuation tube is attached toan effluent collecting canister, and the canister is connected to theadjustable vacuum pump. Depending on the nature of the wound, thepump can deliver either continuous or intermittent subatmosphericpressures ranging from -50 to -200 mm Hg. This negative pressure istransmitted uniformly through the open cell foam dressing to all woundsurfaces.
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
NEGATIVE PRESSURE WOUND THERAPY (V.A.C.(R) THERAPY
1. removing tissue fluids and chronic wound exudate
2. reducing infectious materials
3. assisting in the formation of granulation tissue.
Application of topical negative pressure has been shown to help
promote wound healing by
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Patient and wound assessment
Assessing risk factors and establishing that a patient is at risk should be part of the initial assessment for any patient who is
entering the health care system. Incorporating this assessment into a comprehensive examination ensures that systemic factors compromising wound healing are promptly
identified. Following global evaluation of the patient, attention is then focused on the pressure ulcer itself, and a detailed
wound evaluation is accomplished. Once the patient and the wound have been completely assessed, the practitioner must
initiate a plan of care to address the factors placing the patient at risk, the systemic factors compromising host
healing, and the advanced wound care efforts to be initiated.
Nursing Implications
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Risk Assessment
Preventing pressure ulcers or inhibiting progression of an existing ulcer is greatly facilitated by the use of a practical,
validated risk assessment instrument that enables the practitioner to objectively evaluate a patient's level of risk.
Nursing Implications
The guideline on pressure ulcer prevention from the Agency for Health Care Policy and Research (AHCPR; now the Agency for Healthcare Research and Quality
PRESSURE ULCERS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Nursing Implications
PRESSURE ULCERS
Wounds are very painful, thus causing patients a great deal of suffering.
The anatomical location of the ulcer may result in a loss of dignity.
Quality of life is affected, as the patient must alter activities to help heal the wound and may face long-term hospitalization.
A nonhealing ulcer is at high risk for infection, which can be life threatening.
Ulcer treatments may require surgical procedures such as debridement, colostomies, and amputations, which the patient would otherwise not have to face.
An ulcer that heals forms scar tissue, which lacks the strength of the original tissue and is more easily ulcerated again and again.

Feeding ProblemsGeriatric Syndrome
Alfie R. Espinosa, RNInfection Control Officer
Perioperative Nurse
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
DEFINITIONS
•Feeding: The concept of feeding is defined as, "the process of getting the food from the plate to the mouth. It is a primitive sense without concern for social niceties"( Katz, Downs, Cash, & Grotz, 1970, p. 22).
•Eating: Feeding is differentiated from eating, which is defined as "the ability to transfer food from plate to stomach through the mouth"(Siebens et al., 1986, p. 193).
•Feeding behavior: an environmental and contextual approach to examining the interaction between the person being fed and the caregiver, as well their separate actions (Amella & DiMaria, 2001).
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
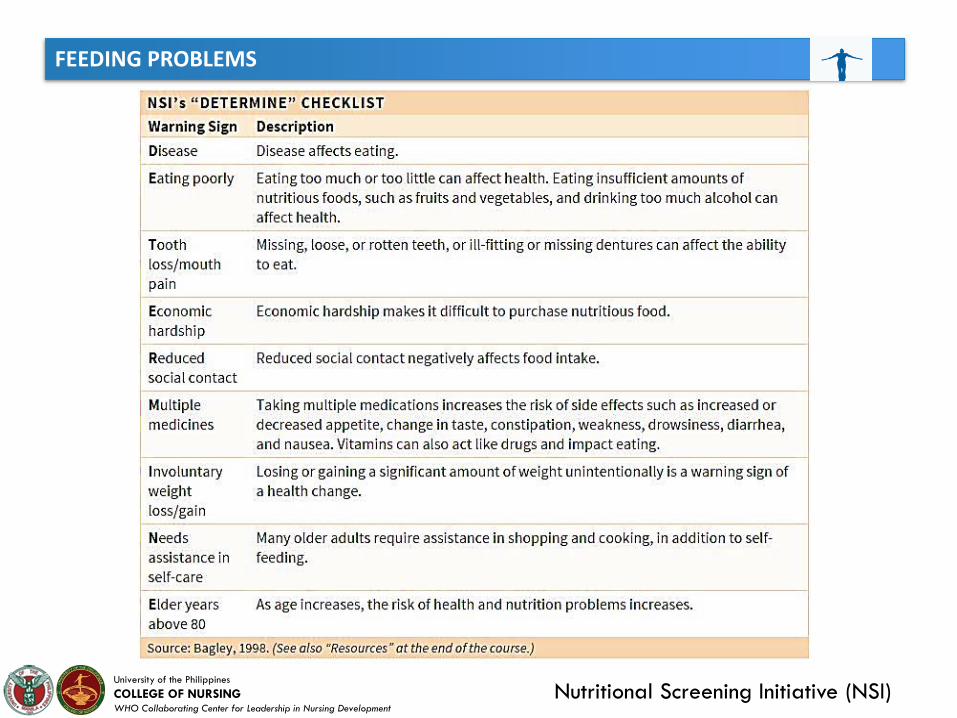
Nutritional Screening Initiative (NSI)
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
FACTORS LEADING TO DECREASED NUTRITION IN THE ELDERLY
Physical Obstacles to Eating
• difficulty in holding and using utensils or in conveying food from plate to mouth• decreased ability to chew and swallow• decreased appetite• decreased awareness of hunger and thirst
Arthritis
When arthritis occurs in the hands, an
inability to manipulate utensils—due to
swelling and decreased joint function
as well as pain and inflammation—can
affect the ability to pick up or cut food
or use a cup.
Stroke
Stroke can lead to paralysis; weakness
and changes in muscle tone, usually on
one side of the body; and difficulty
chewing, manipulating food in the
mouth, and swallowing.
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
FACTORS LEADING TO DECREASED NUTRITION IN THE ELDERLY
Physical Obstacles to Eating
DENTITION PROBLEMS
Missing or painful teeth and ill-fitting
or uncomfortable dentures may make
chewing difficult or impossible.
SMELL AND TASTE PROBLEMS
Diminishes as a natural consequence of
aging, which can decrease interest in
and appreciation of food
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
FACTORS LEADING TO DECREASED NUTRITION IN THE ELDERLY
Apraxia is the inability to perform
physical actions despite having
intact physical ability.
APRAXIA
Amnesia can lead people to forget to
eat altogether; to forget that they have
just eaten, leading them to eat again;
or to think they have eaten when they
haven’t, causing them to skip the nextmeal.
AMNESIA
Cognitive/Perceptual Obstacles to Eating
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
FACTORS LEADING TO DECREASED NUTRITION IN THE ELDERLY
Executive functioning is necessary for
self-regulation and awareness. A
deficit in this area can lead people to
exhibit unsafe behavior or behavior
that is socially inappropriate, such as
taking food from other people’s
plates or not regulating the amount
of food they are eating.
EXECUTIVE FUNCTIONING
Agnosia is the inability to interpret sensory
information despite having intact senses.
Those with agnosia may not react to smells
and taste with an increased appetite,
decreasing the likelihood that they
experience hunger. In addition, they might
eat dangerous, non-food items. They may
not recognize the feeling of thirst and may
become dehydrated.
AGNOSIA
Cognitive/Perceptual Obstacles to Eating
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
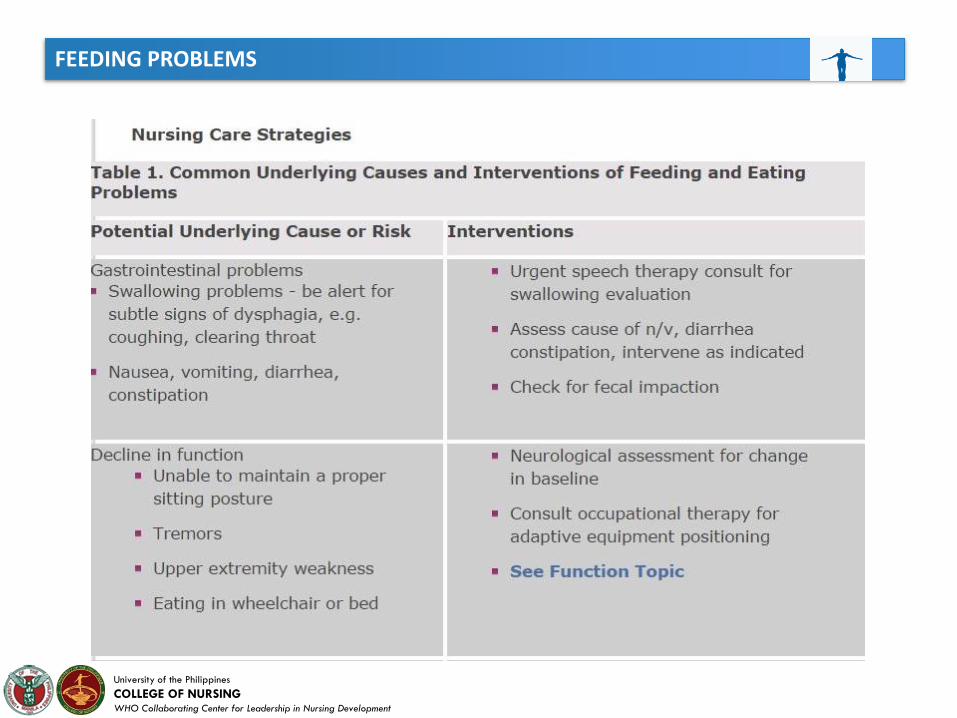
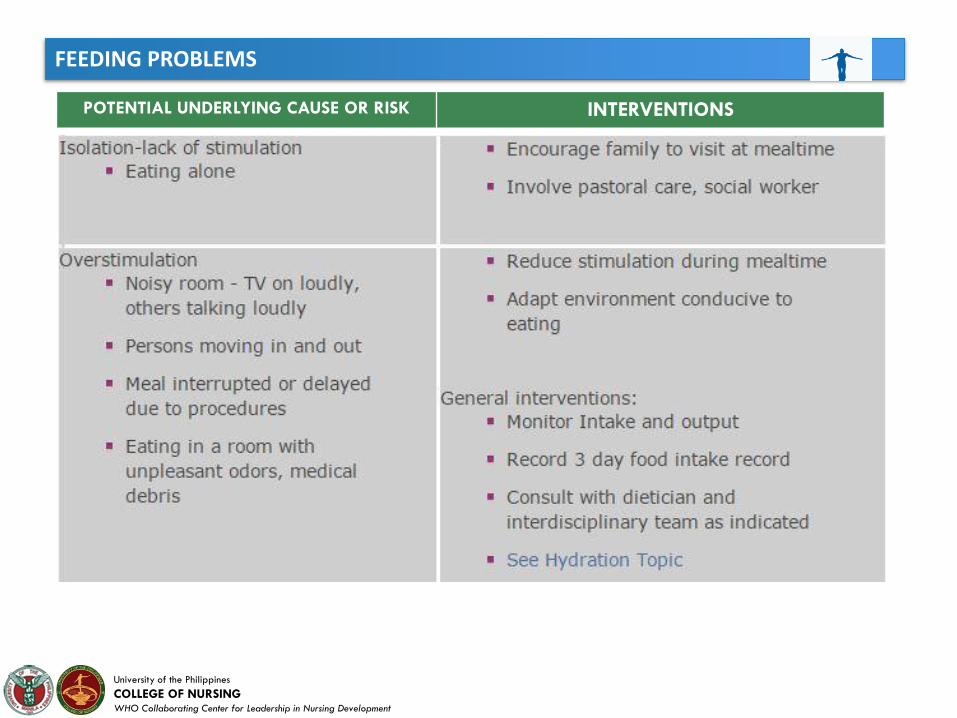
POTENTIAL UNDERLYING CAUSE OR RISK INTERVENTIONS
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
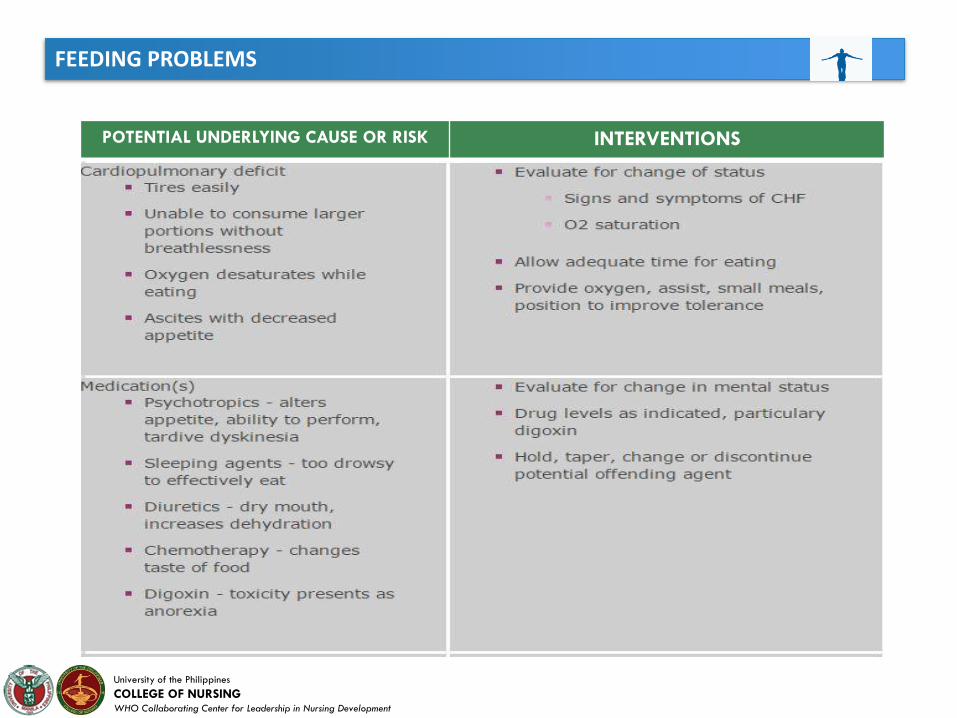
POTENTIAL UNDERLYING CAUSE OR RISK INTERVENTIONS
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
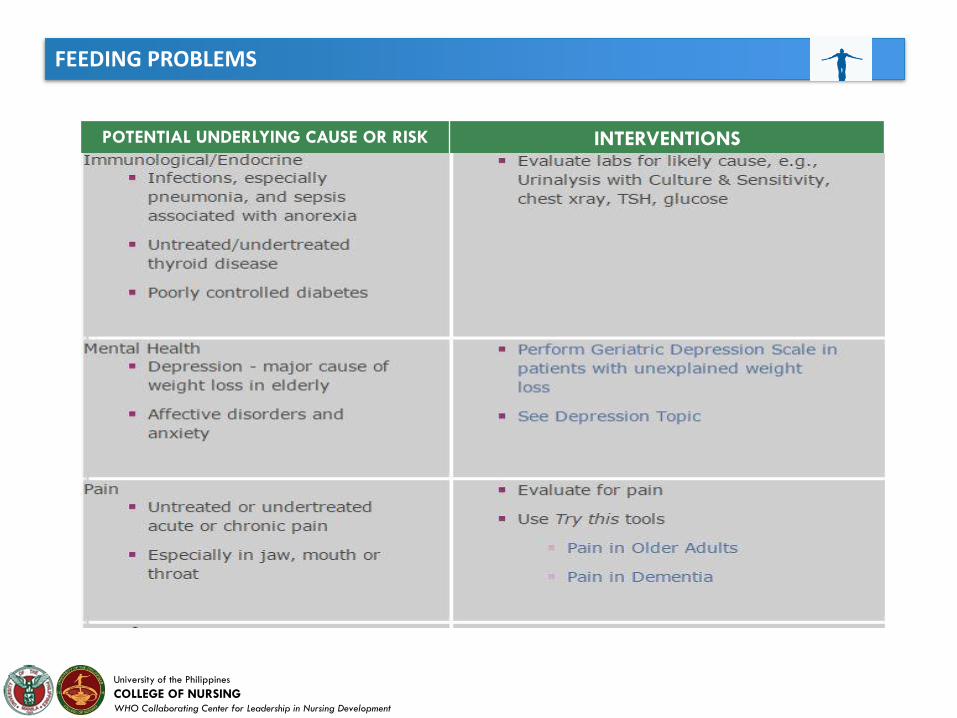
POTENTIAL UNDERLYING CAUSE OR RISK INTERVENTIONS
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
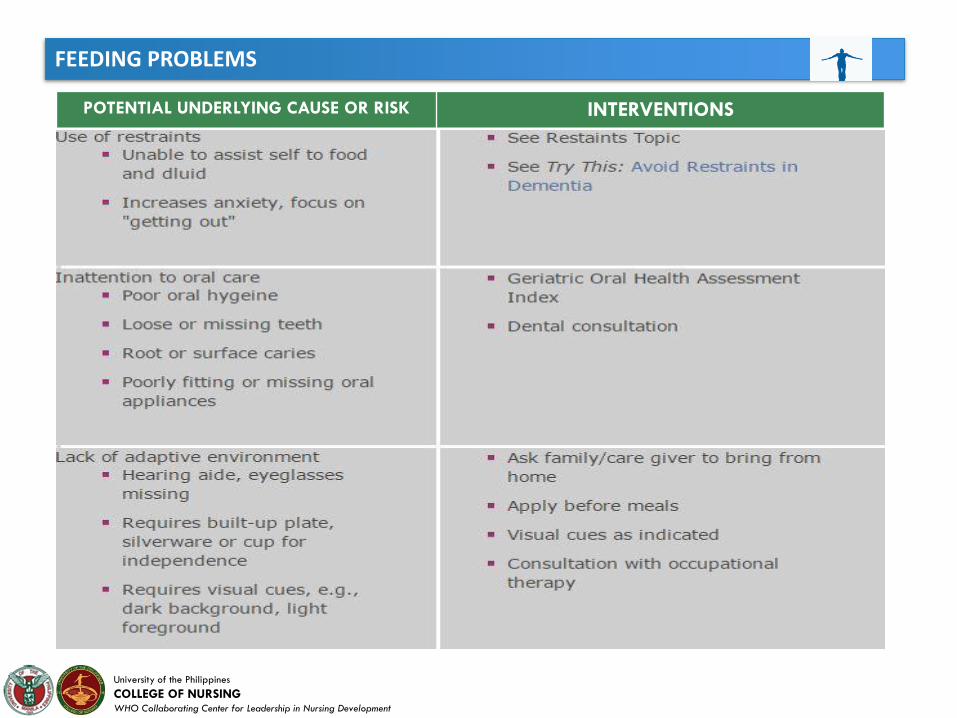
POTENTIAL UNDERLYING CAUSE OR RISK INTERVENTIONS
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
ADAPTIVE EQUIPMENT
Some of the equipment includes:
• Non-slip materials; the use of foam handles or large, molded handles
that slip over regular utensils; or a universal cuff to increase the
client’s ability to grip and/or for joint protection
• Rubber-coated spoons for people who have a tendency to bite down
on utensils
• Plates with a built-up edge for scooping against and plate guards to
prevent food from being pushed off the edge
• Rocker knives or roller knives, similar to pizza cutters, which require
less strength and coordination to cut with than standard knives
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
ADAPTIVE EQUIPMENT
Some of the equipment includes:
• Divided plates to keep food separate on plates and prevent it from moving
around too much
• Two-handled mugs
• Cups with a cut-out near the top or an integral straw so that the client can
drink without tilting the head back (to prevent aspiration), for those with
tremors who have a difficult time sipping, or for those who have only a
sucking reflex
• Suction cups or non-slip mats to keep cups, bowls, and plates in place
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Nursing Implications to Caring
A. Environment
1. Dining or patient room: encourage older adult to eat in dining room to increaseintake, personalize dining room, no treatments or other activities occurring duringmeals, no distractions.
2. Tableware: use of standard dinnerware (e.g., china, glasses, cup and saucer,flatware, tablecloth, napkin) versus disposable tableware and bibs
3. Furniture: older adult seated in stable arm chair; table-appropriate height versuseating in wheelchair or in bed.
4. Noise level: environmental noise from music, caregivers, and television is minimal;personal conversation between patient and caregiver is encouraged.
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Nursing Implications to Caring
A. Environment
5. Music: pleasant, preferred by patient.
6. Light: adequate and nonglare-producing versus dark, shadowy, or glaring.
7. Contrasting background/foreground: use contrasting background and foregroundcolors with minimal design to aid persons with decreased vision.
8. Odor: food prepared in area adjacent to or in dining area to stimulate appetite.
9. Adaptive equipment: available, appropriate, and clean; caregivers and/or older adultknowledgeable in use; occupational therapist assists in evaluation.
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Nursing Implications to Caring
B. Caregiver/Staffing
1. Provide an adequate number of well-trained staff.
2. Deliver an individualized approach to meals including choice of food,tempo of assistance.
3. Position of caregiver relative to elder: eye contact; seating so caregiverfaces elder patient in same plane.
4. Cueing: caregiver cues elder whenever possible with words or gestures.
5. Self-feeding: encouragement to self-feed with multiple methods versusassisted feeding to minimize time.
6. Mealtime rounds: interdisciplinary team to examine multifaceted processof meal service, environment, and individual preferences.
REFERENCES
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Amella EJ, DiMaria RA (2001). Feeding behavior. In GL Maddox, RC Atchley, JG Evans,
RB Hudson, RA Kane, EJ Masoro, MD Mezey, LW Poon, IC Siegler (eds.).The
Encyclopedia of Aging (3rd ed.) (pp. 389 - 391). New York: Springer
American College of Obstetricians and Gynecologists. Urinary incontinence in
women. Obstet Gynecol. Jun 2005;105(6):1533-45
Bernstein M & Luggen AS. (2010). Nutrition for the older adult. Sudbury, MA: Jones
and Bartlett.
Berrut, G., Favreau, A. M., Dizo, E., Tharreau, B., Poupin, C., & Gueringuili, M.
(2002). Estimation of calorie and protein intake in aged patients: Validation of a
method based on meal portions consumed. Journals of Gerontology: Medical
Science, 57(1), M52–M56. Evidence Level III: Quasi-experimental Study.
Bottomley J. (2010). Geriatric rehabilitation: a textbook for the physical therapy
assistant. Thorofare, NJ: SLACK.
DeVere R & Calvert M. (2011). Navigating smell and taste disorders. St. Paul, MN:
AAN Enterprises.
REFERENCES
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Groher, M. E. (1997). Dysphagia: Diagnosis and Management (3rd ed.). Boston:
Butterworth-Heinemann.
JF Schnelle, PA Cruise, A. Rahman. Developing rehabilitative behavioral interventions
for long-term care: technology transfer, acceptance, and maintenance issues. J Am
Geriatr Soc, 46 (1998), pp. 771–778
Katz S, Downs TD, Cash HR, Grotz RC. (1970). Progress in the development of the
Index of ADL. The Gerontologist, 10, 22.
Katz, S., Downs, T. D., Cash, H. R., & Grotz, R. C. (1970). Progress in the development
of the Index of ADL. The Gerontologist, 10(1), 20–30. Evidence Level IV: Quasi-
experimental Study.
Myers, B.A. (2004). Wound Management: Principles and Practice. Prentice Hall:
Upper Saddle River, New Jersey, 37-45, 369-391
Nakasato Y. (2011). Geriatric rheumatology. New York: Springer.
National Pressure Ulcer Advisory Panel (NPUAP)
REFERENCES
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Nazir T, Khan Z, Barber HR. Urinary incontinence. Clin Obstet Gynecol. Dec
1996;39(4):906-11
Rogers RG. Clinical practice. Urinary stress incontinence in women. N Engl J Med. Mar
6 2008;358(10):1029-36
Siebens H, Trupe E, Siebens A, Cook F, Anshen S, Hanauer R, Oster G. (1986).
Correlates and consequences of eating dependency in institutionalized
elderly.Journal of the American Geriatric Society, 34,193.
Watson, R. (1996). The Mokken Scaling Procedure (MSP) applied to the measurement
of feeding difficulty in elderly people with dementia. International Journal of
Nursing Studies, 33, 385–393. Evidence Level III: Quasi-experimental Study.
Wilson, M.M. (2007). Assessment of appetite and weight loss syndromes in nursing
home residents. Missouri Medicine, 104(1), 46-51. Evidence Level VI.
www.npuap.org.
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Katz, S., Downs, T. D., Cash, H. R., & Grotz, R. C. (1970). Progress in the development of the Index of ADL. The Gerontologist, 10(1), 20–30. Evidence Level IV: Quasi-experimental Study.
Wilson, M.M. (2007). Assessment of appetite and weight loss syndromes in nursing home residents. Missouri Medicine, 104(1), 46-51. Evidence Level VI.
Groher, M. E. (1997). Dysphagia: Diagnosis and Management (3rd ed.). Boston: Butterworth-Heinemann.
Watson, R. (1996). The Mokken Scaling Procedure (MSP) applied to the measurement of feeding difficulty in elderly people with dementia. International Journal of Nursing Studies, 33, 385–393. Evidence Level III: Quasi-experimental Study.
Berrut, G., Favreau, A. M., Dizo, E., Tharreau, B., Poupin, C., & Gueringuili, M. (2002). Estimation of calorie and protein intake in aged patients: Validation of a method based on meal portions consumed. Journals of Gerontology: Medical Science, 57(1), M52–M56. Evidence Level III: Quasi-experimental Study.
References
FEEDING PROBLEMS
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
Amella EJ, DiMaria RA (2001). Feeding behavior. In GL Maddox, RC Atchley, JG Evans, RB Hudson, RA Kane, EJ Masoro, MD Mezey, LW Poon, IC Siegler (eds.).The Encyclopedia of Aging (3rd ed.) (pp. 389 - 391). New York: Springer
Katz S, Downs TD, Cash HR, Grotz RC. (1970). Progress in the development of the Index of ADL. The Gerontologist, 10, 22.
Siebens H, Trupe E, Siebens A, Cook F, Anshen S, Hanauer R, Oster G. (1986). Correlates and consequences of eating dependency in institutionalized elderly.Journal of the American Geriatric Society, 34,193.
References
University of the Philippines
COLLEGE OF NURSINGWHO Collaborating Center for Leadership in Nursing Development
THANK YOU!