Embed Size (px)
Citation preview
PRESSURE ULCERS
Kansas Reynolds Program in Aging
Shelley B. Bhattacharya, D.O., M.P.H.Assistant Professor, Director of Geriatric Education
Department of Family Medicine
OBJECTIVES
Know and understand:
The morbidity and mortality associated with pressure ulcers for older adults
The common risk factors for pressure ulcer development
Evidence based techniques for preventing pressure ulcers
The pressure ulcer staging system and treatment
strategies for each stage
ACOVE INDICATOR Concerning the pressure ulcer care of an older adult : If a vulnerable older adult is admitted to an intensive
care unit or a medical or surgical unit of a hospital and cannot reposition himself or herself or has limited ability to do so, THEN risk assessment for pressure ulcers should be performed on admission
If a vulnerable older adult is identified as at risk for pressure ulcer development or a pressure ulcer risk assessment score indicates that the person is at risk, THEN preventive intervention must be instituted within 12 hours, addressing repositioning needs and pressure reduction (or management of tissue loads)
ACOVE INDICATOR If a vulnerable older adult presents with a
pressure ulcer, THEN the pressure ulcer should be assessed for 1) location, 2) depth and stage, 3) size and 4) presence of necrotic tissue
If a vulnerable older adult is identified as at risk for pressure ulcer development and has malnutrition (involuntary weight loss >10% over 1 year or low albumin or prealbumin levels), THEN nutritional intervention or dietary consultation should be instituted
TOPICS COVERED
Epidemiology
Complications
Risk Factors and Risk Assessment
Evidence based review of prevention techniques
Ulcer Assessment and 2007 Staging definitions
Monitoring and Treatment
PRESSURE ULCER: DEFINITION
Definition (2007 National Pressure Ulcer Advisory Panel): an injury caused by unrelieved pressure on a specific region of skin and muscle in bed or chair bound patients
The time for pressure ulcer development is variable due to severity of illness and a number of comorbid conditions
PRESSURE ULCERS: A MAJOR ISSUE IN GERIATRIC MEDICINE
Affects 1 million adults annually
Higher risk in older persons because: Local blood supply to skin decreases Epithelial layers flatten and thin Subcutaneous fat decreases Collagen fibers lose elasticity Tolerance to hypoxia decreases
1 of 3 sentinel events for long-term care
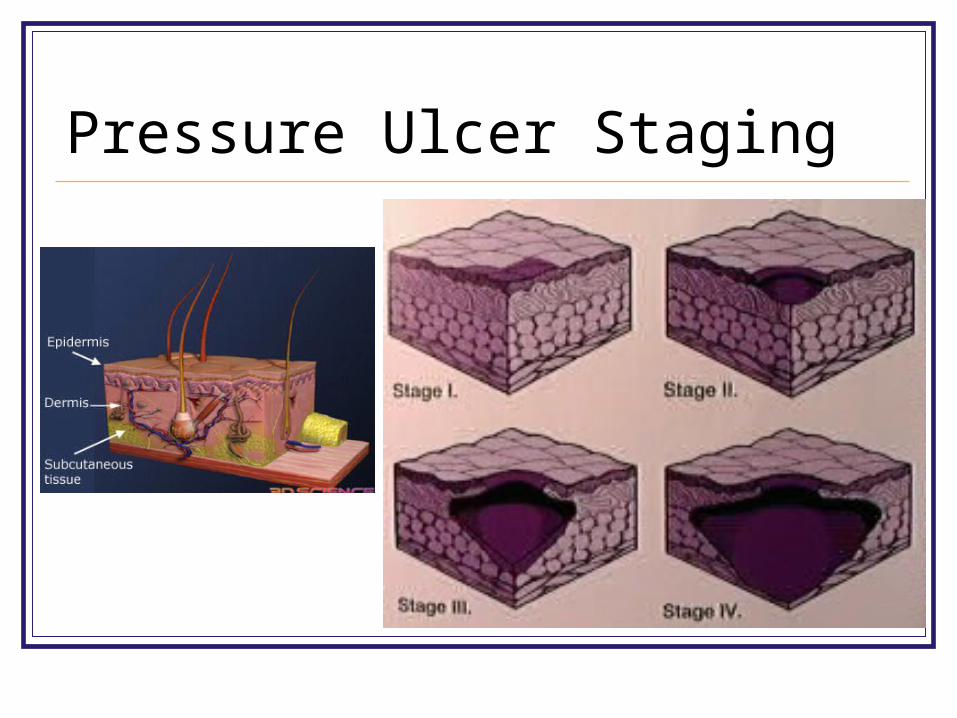
Pressure Ulcer Staging
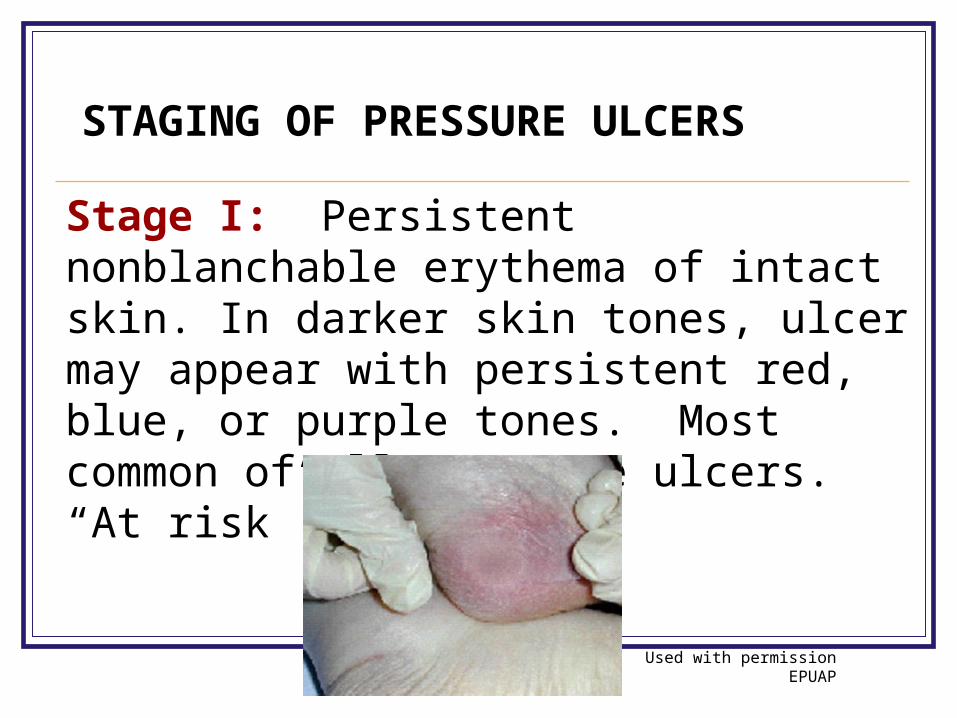
Stage I: Persistent nonblanchable erythema of intact skin. In darker skin tones, ulcer may appear with persistent red, blue, or purple tones. Most common of all pressure ulcers. “At risk” person.
STAGING OF PRESSURE ULCERS
Used with permission EPUAP
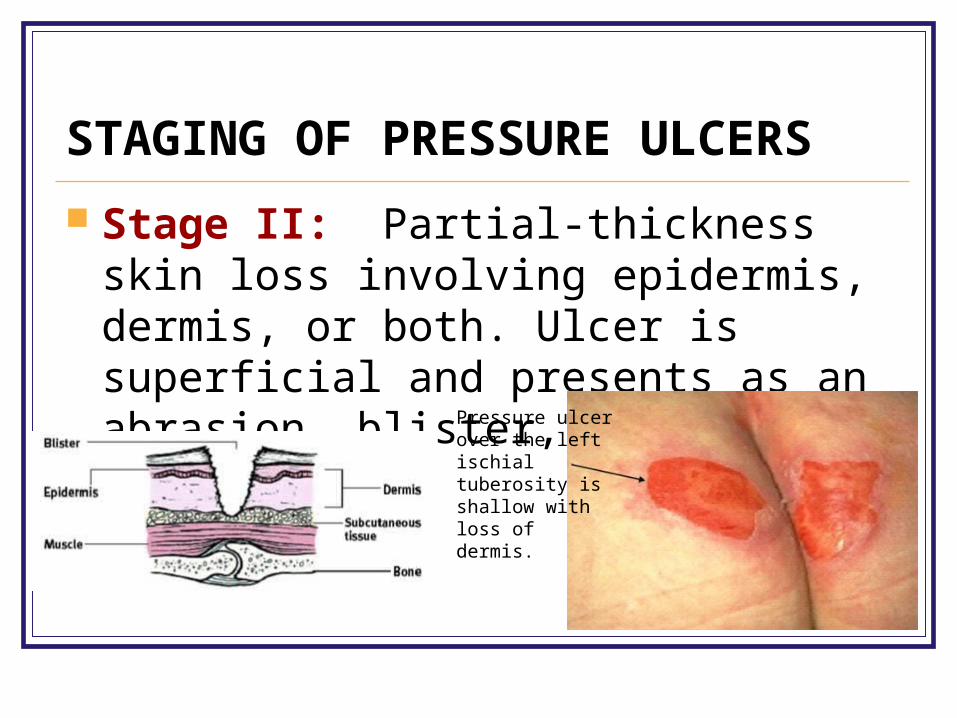
STAGING OF PRESSURE ULCERS
Stage II: Partial-thickness skin loss involving epidermis, dermis, or both. Ulcer is superficial and presents as an abrasion, blister, or shallow crater.
Pressure ulcer over the left ischial tuberosity is shallow with loss of dermis.
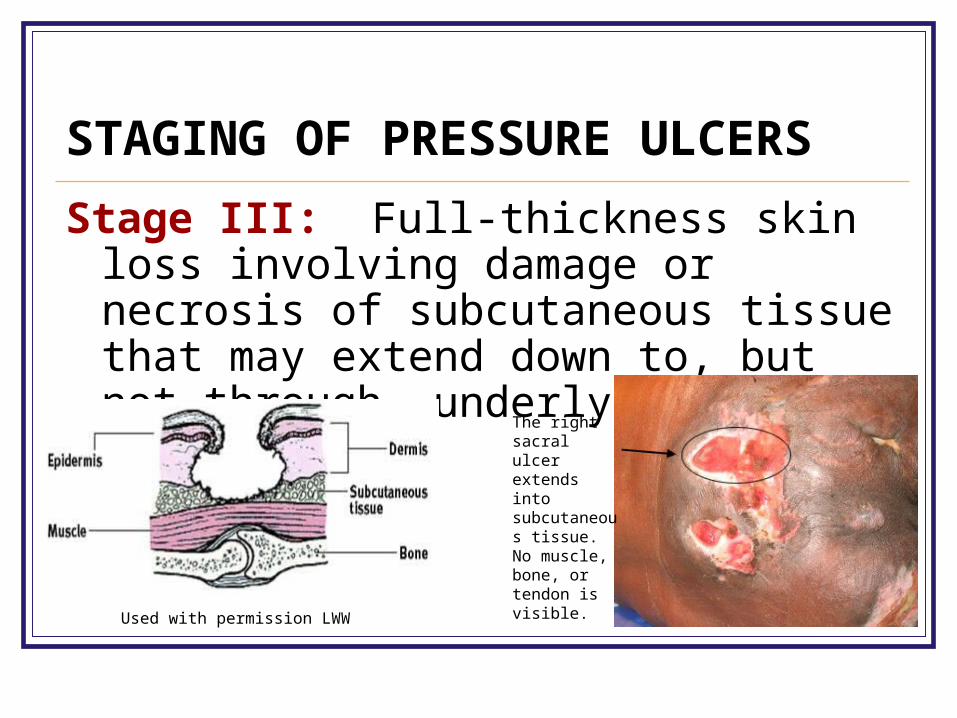
STAGING OF PRESSURE ULCERS
Stage III: Full-thickness skin loss involving damage or necrosis of subcutaneous tissue that may extend down to, but not through, underlying fascia.
Used with permission LWW
The right sacral ulcer extends into subcutaneous tissue. No muscle, bone, or tendon is visible.
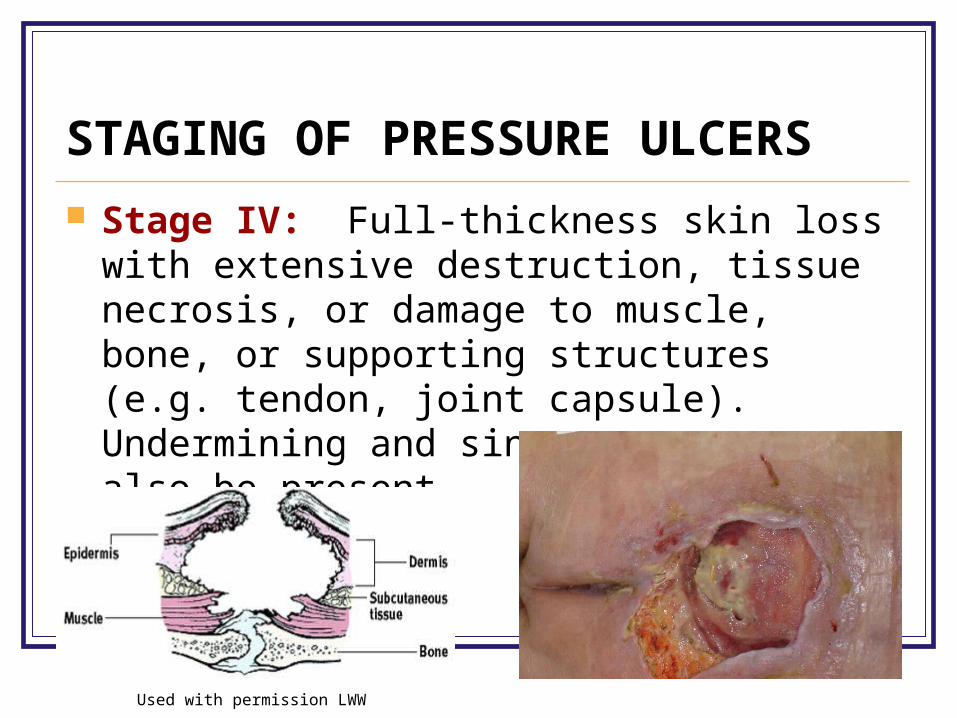
STAGING OF PRESSURE ULCERS
Stage IV: Full-thickness skin loss with extensive destruction, tissue necrosis, or damage to muscle, bone, or supporting structures (e.g. tendon, joint capsule). Undermining and sinus tracts may also be present.
Used with permission LWW
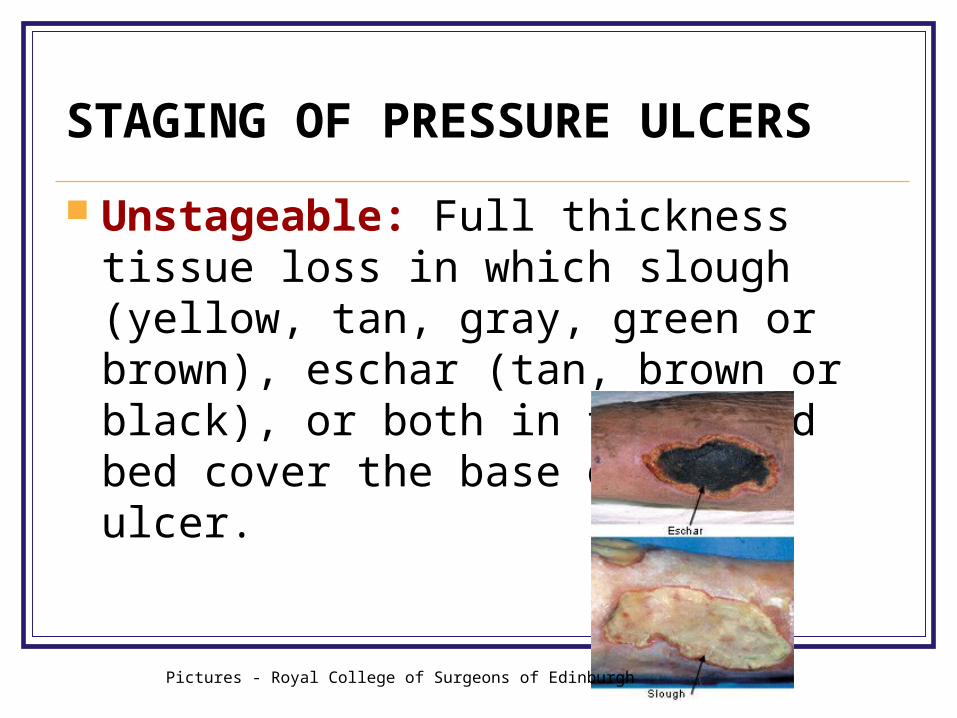
STAGING OF PRESSURE ULCERS
Unstageable: Full thickness tissue loss in which slough (yellow, tan, gray, green or brown), eschar (tan, brown or black), or both in the wound bed cover the base of the ulcer.
Pictures - Royal College of Surgeons of Edinburgh
0
5
10
15
20
25
30
35
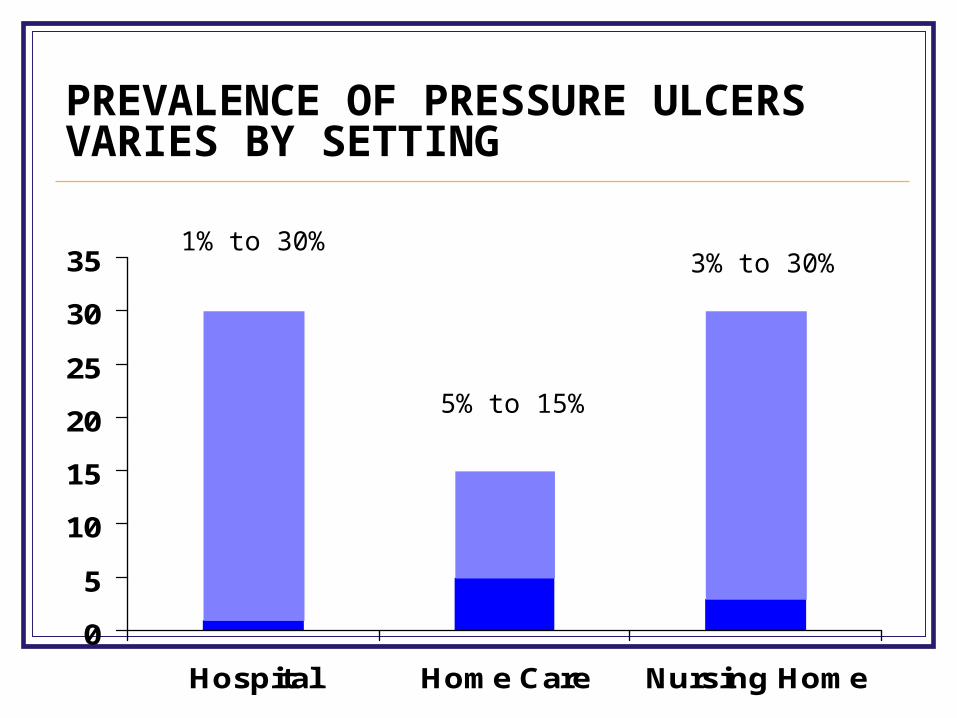
Hospital Home Care Nursing Home
PREVALENCE OF PRESSURE ULCERS VARIES BY SETTING
1% to 30%3% to 30%
5% to 15%
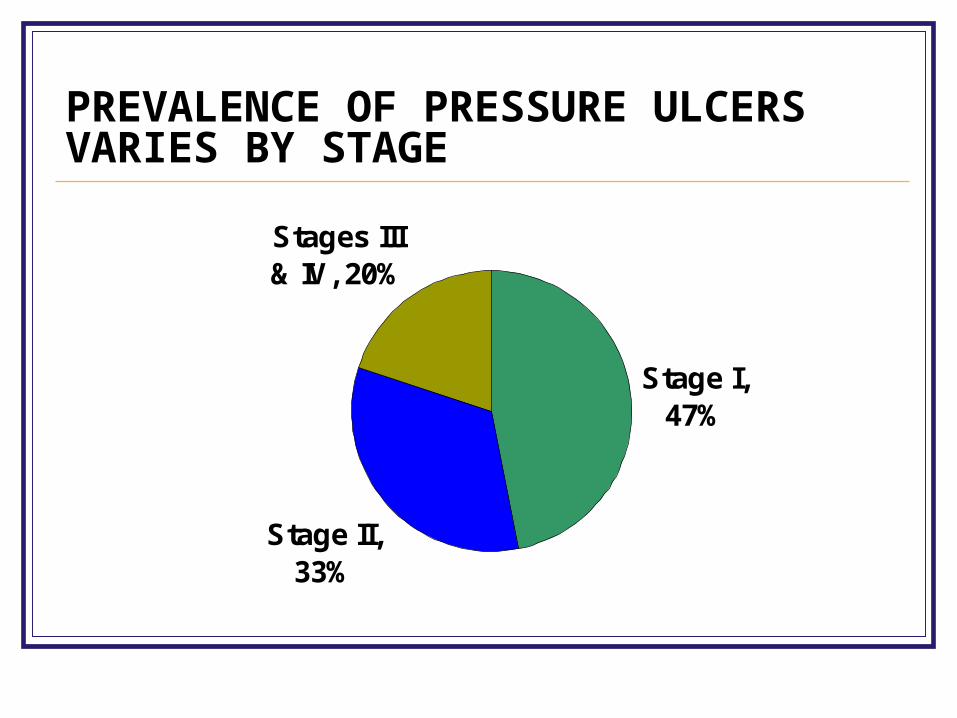
PREVALENCE OF PRESSURE ULCERS VARIES BY STAGE
Stages III & IV, 20%
Stage I, 47%
Stage II, 33%
RISK FACTORS
Older adults have a much higher likelihood of developing pressure ulcers due to their risk factors
Intrinsic risk factors are physiologic factors or disease states that increase the risk for pressure ulcer development
Extrinsic risk factors are external factors that damage skin
INTRINSIC FACTORS PREDICTIVE OF PRESSURE ULCER DEVELOPMENT
Age 70+ Impaired mobility Current smoking Low BMI Confusion Urinary and fecal
incontinence Malnutrition Restraints
Comorbid conditions: malignancy, diabetes, stroke, pneumonia, CHF, fever, sepsis, hypotension, renal failure, dry skin, history of pressure ulcers, anemia, lymphopenia, hypoalbuminemia
EXTRINSIC FACTORS PREDICTIVE OF PRESSURE ULCER DEVELOPMENT
Alcohol/drug abuse, Friction/shear/pressure Inadequate current wound care Immunosuppressive and chemotherapeutic agents Nutritional deficiency Uncontrolled excess local pressure Adverse reactions to skin care products Smoking Fecal and urinary incontinence
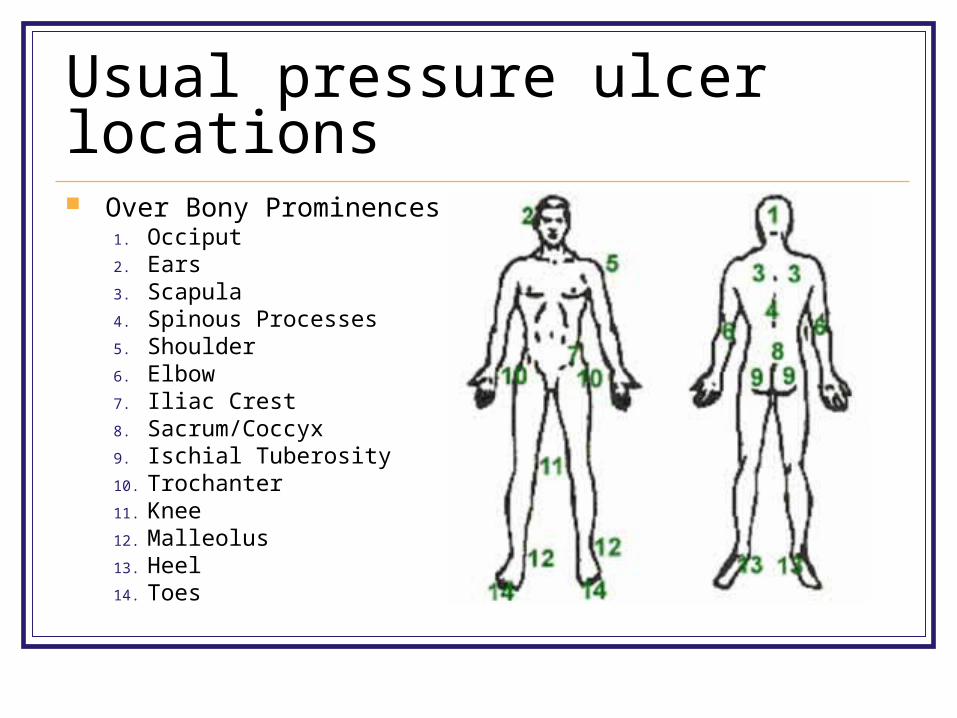
Usual pressure ulcer locations Over Bony Prominences
1. Occiput 2. Ears 3. Scapula 4. Spinous Processes 5. Shoulder 6. Elbow 7. Iliac Crest 8. Sacrum/Coccyx 9. Ischial Tuberosity 10. Trochanter 11. Knee 12. Malleolus 13. Heel 14. Toes
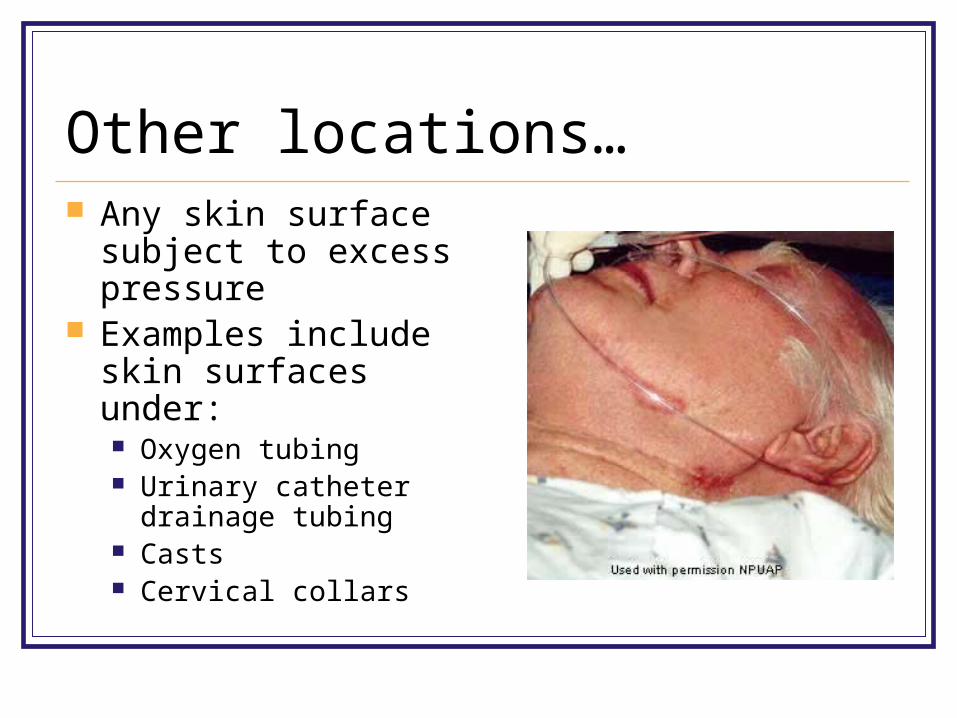
Other locations… Any skin surface
subject to excess pressure
Examples include skin surfaces under: Oxygen tubing Urinary catheter
drainage tubing Casts Cervical collars
POSSIBLE COMPLICATIONS
Sepsis (aerobic or anaerobic bacteremia)
Localized infection, cellulitis, osteomyelitis
Pain
Depression
Mortality rate = 60% in older persons who develop a pressure ulcer within 1 year of hospital discharge
RISK ASSESSMENT INSTRUMENTS
Widely used tools for identifying older patients at risk for developing ulcers: SCREENING TOOLS
Norton scale:sensitivity =73%–92%, specificity = 61%–94%
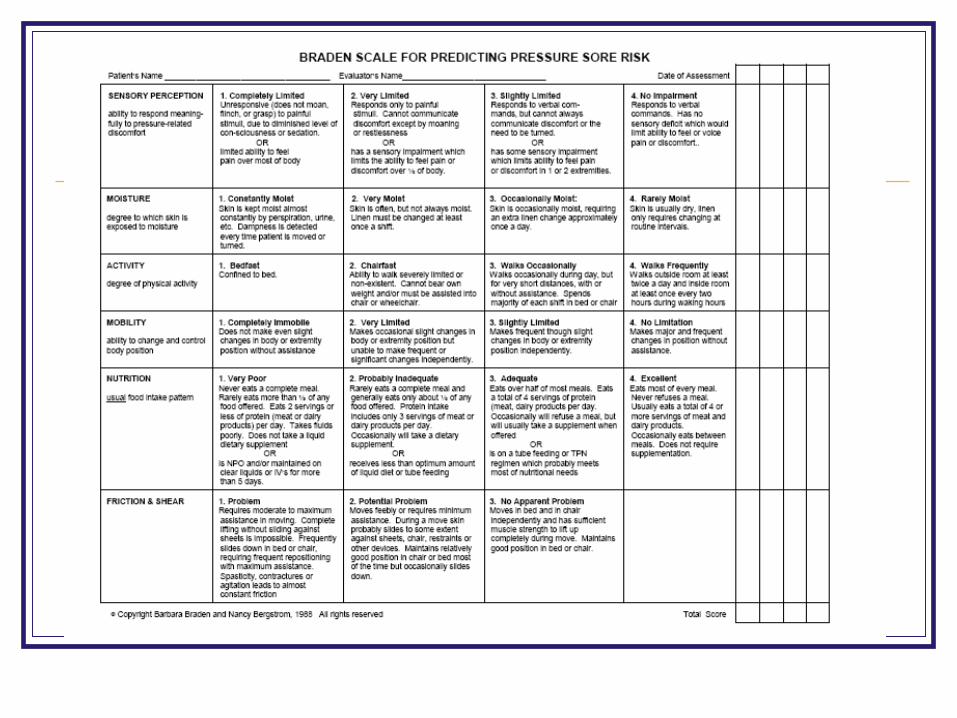
Braden scale: sensitivity = 83%–100%, specificity = 64%–77%
Both recommended by Agency for Healthcare Research and Quality
BRADEN SCALE
Provides method for assessing a patient’s pressure ulcer risk by evaluating:
Sensory perception: ability to respond to pressure-related discomfort
Moisture: degree to which skin is exposed to moisture
Activity: degree of physical activity Mobility: ability to change and control body
position Nutrition: usual food intake
NORTON SCALE
Provides method for assessing a patient’s pressure ulcer risk by evaluating:
Physical condition Mental condition Level of physical activity Mobility Continence or incontinence
Scale Documentation Frequency October 2007 JAGS article recommends
using the scales: If in hospital setting: on admission, if at risk then
q 48 hours thereafter; If in skilled nursing facility: on admission, q wk for
1st 4 weeks, then q 3mos thereafter; If in home health program: on admission, if found
to be at risk, then q wk for 4 weeks and every other week thereafter.
PREVENTION
An evidence-based approach to preventing pressure ulcers focuses on:
Skin care
Mechanical loading
Support surfaces
PREVENTION: SKIN CARE
Daily systematic skin inspection and cleansing
factors that promote dryness
Avoid massaging over bony prominences
moisture (incontinence, perspiration, drainage)
Minimize friction and shear
PREVENTION:MECHANICAL LOADING
Reposition at least every 2 hours (may use pillows, foam wedges)
Keep head of bed at lowest elevation possible
Use lifting devices to decrease friction and shear
Remind patients in chairs to shift weight every 15 min
“Doughnut” seat cushions are contraindicated,may cause pressure ulcers
Pay special attention to heels (heel ulcers account for 20% of all pressure ulcers)
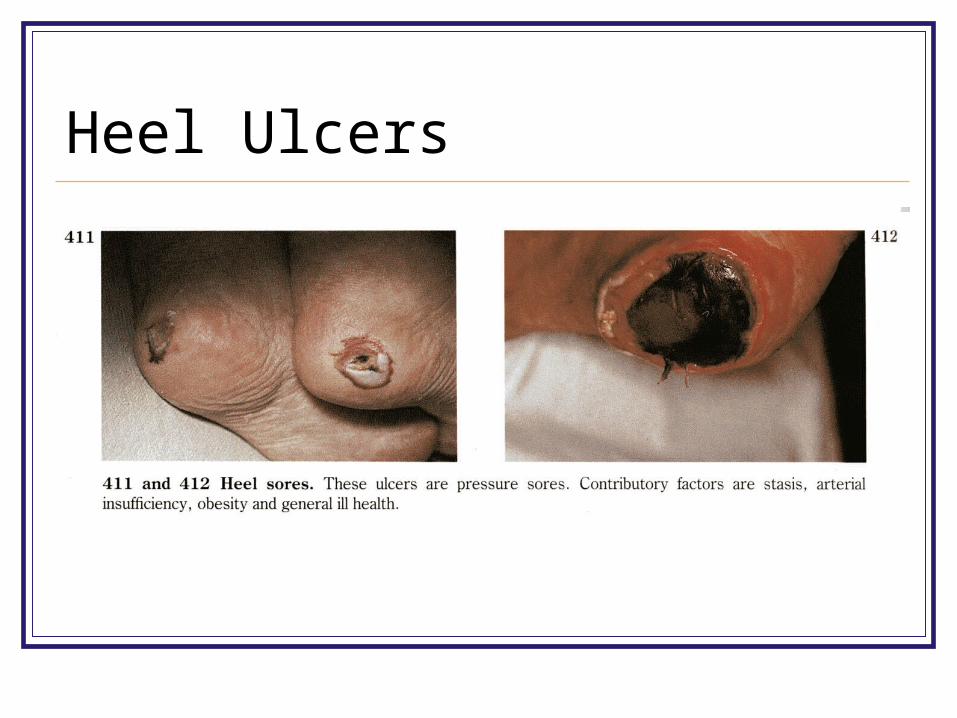
Heel Ulcers
PREVENTING HEEL ULCERS
Assess heels of high-risk patients every day
Use moisturizer on heels (no massage) twice a day
Apply dressings to heels: Transparent film for patients prone to friction
problems Single or extra-thick hydrocolloid dressing for
those with pre-stage 1 reactive hyperemia

PREVENTING HEEL ULCERS
Have patients wear: Socks to prevent friction (remove at bedtime) Properly fitting sneakers or shoes when in wheelchair
Place pillow under legs to support heels off bed
Place heel cushions to prevent pressure
Turn patients every 2 hours, repositioning heels
PRESSURE-REDUCINGSUPPORT SURFACES
**Use for all older persons at risk for ulcers**
Static Foam, static air, gel, water, combination (less expensive)
Dynamic Alternating air, low-air-loss, or air-fluidized Use if the status surface is compressed to <1 inch or high-risk
patient has reactive hyperemia on a bony prominence despite use of static support
Potential adverse effects: dehydration, sensory deprivation, loss of muscle strength, difficulty with mobilization
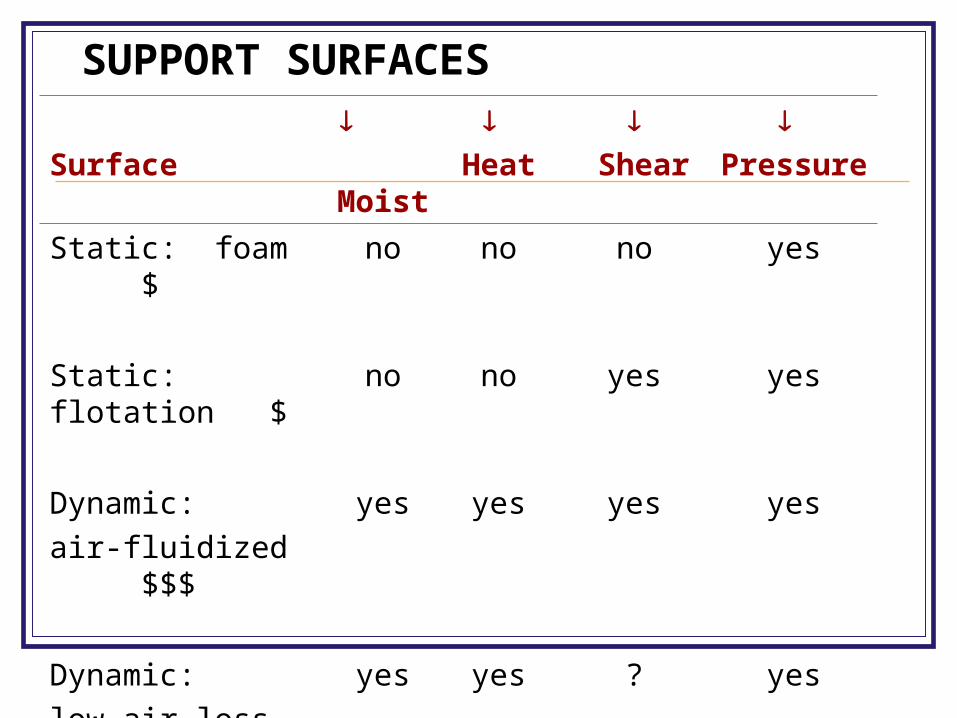
SUPPORT SURFACES
Surface
Moist
Heat
Shear
Pressure
Static: foam $ no no no yes
Static: flotation $ no no yes yes
Dynamic:
air-fluidized $$$
yes yes yes yes
Dynamic:
low-air-loss $$$
yes yes ? yes
Dynamic: alternating air $$
no no yes yes
MANAGEMENT: GENERAL ASSESSMENT
Identify and effectively manage issues that have placed patient at risk for pressure ulcers:
Medical diseases Health problems (eg, urinary incontinence) Nutritional status Pain level Psychosocial health
MANAGEMENT: ULCER ASSESSMENT
Evaluate and document the following:
Location Stage Area Depth Pain
Drainage Necrosis Granulation Cellulitis
MANAGEMENT:MONITORING HEALING
Document all observations over time
Describe each ulcer to track progress of healing
Do not use “reverse staging” Ulcers are filled with granulation tissue (endothelial cells,
fibroblasts, collagen, extracellular matrix) Ulcers do not replace lost muscle, subcutaneous fat, or dermis
before re-epithelializing E.g. Stage IV cannot become stage III
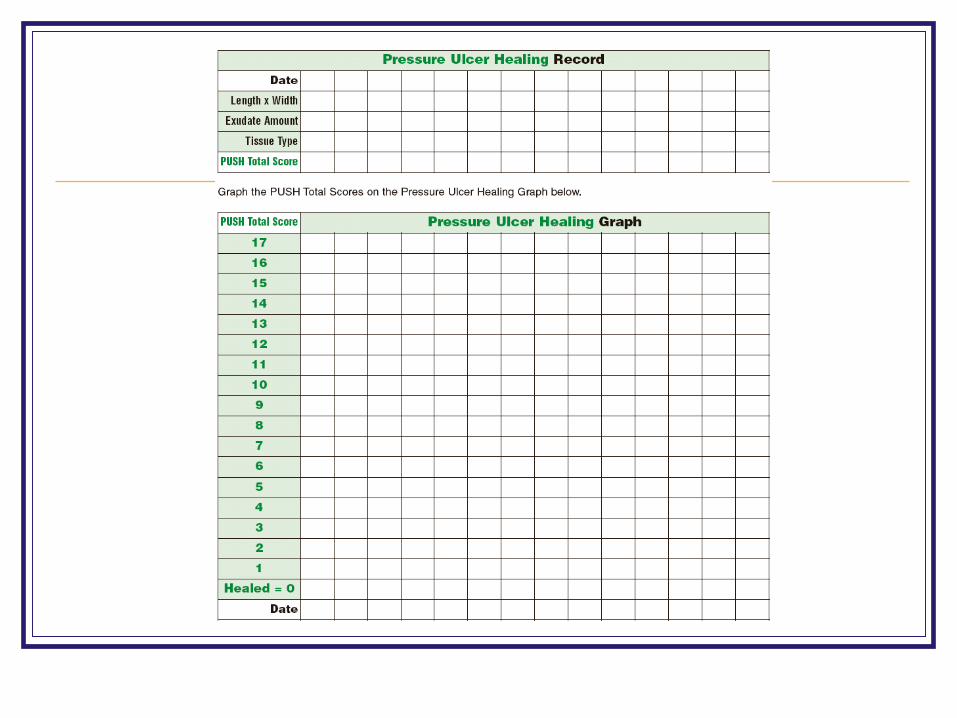
Use validated tools (eg, PUSH, see next slide)
A validated method to document healing over time
Observe and measure the ulcer’s: Surface area: measure with centimeter ruler Exudate: estimate portion of ulcer bed covered by drainage Appearance: estimate portion of ulcer for each tissue type
(epithelial, granulation, slough, necrotic)
Assign weighted score to obtain total score; total scores over time indicate healing or deterioration
PRESSURE ULCER SCALE FOR HEALING (PUSH)
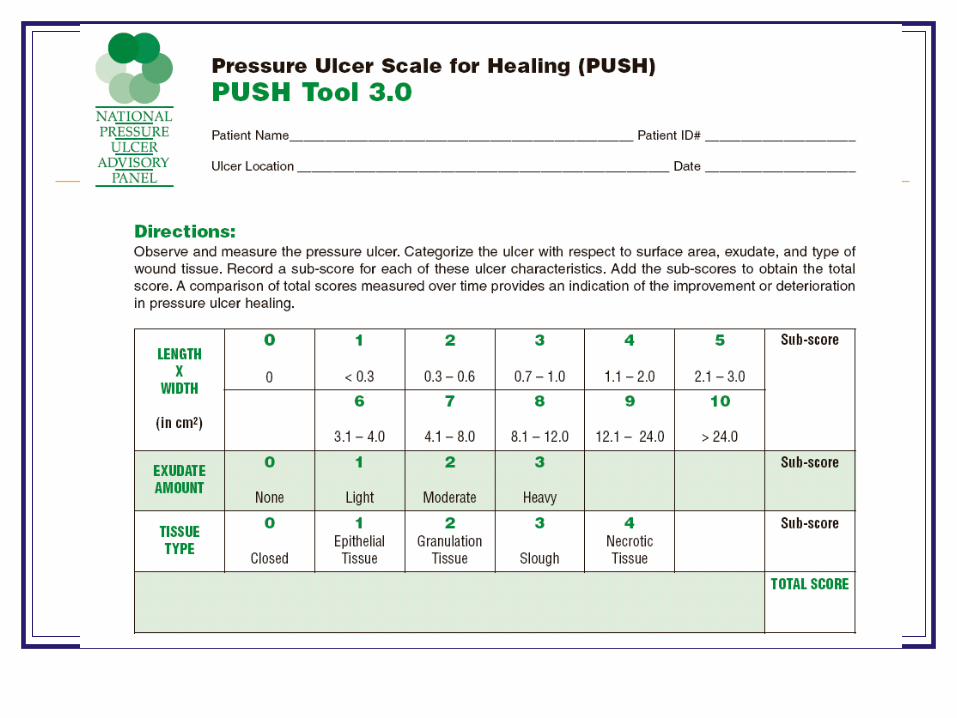
Evidence for Wound Assessments
No direct evidence that wound assessments improve clinical outcomes, but has been found that identifying wound characteristics can predict time to healing
Adequate assessment guides treatment, provides data for comparison and can help predict time to healing
MANAGEMENT:CONTROL OF INFECTIONS
Wound cleansing and dressing are the key frequency when purulent or foul-smelling drainage is first
observed Avoid topical antiseptics because of their tissue toxicity
With failure to heal or persistent exudate after 2 weeks of optimal cleansing, consider trial of topical antibiotics
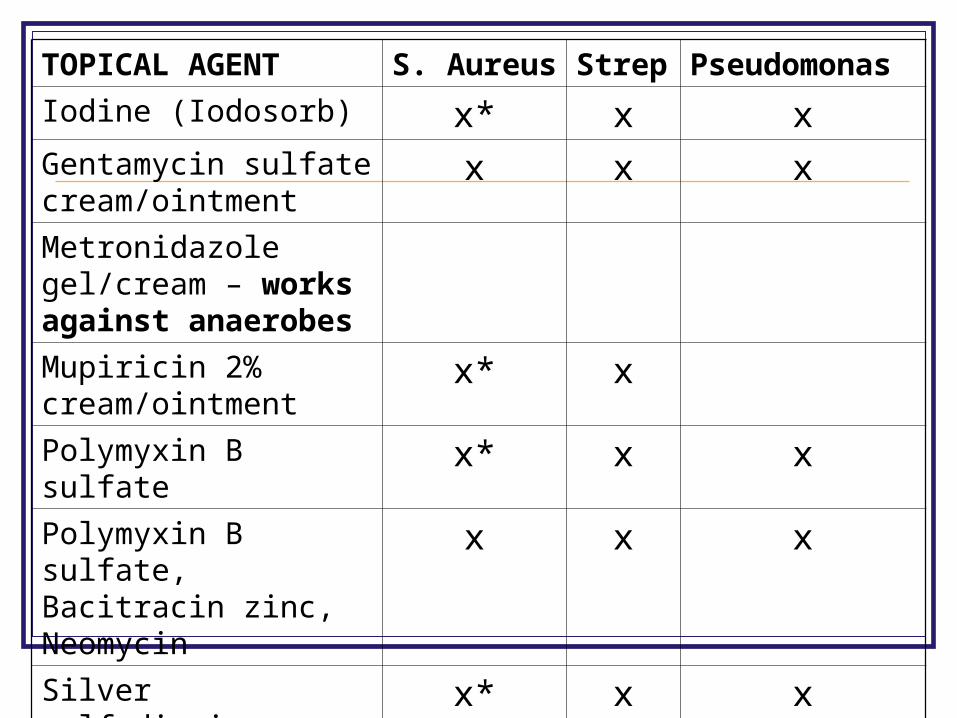
TOPICAL AGENT S. Aureus Strep Pseudomonas
Iodine (Iodosorb) x* x xGentamycin sulfate cream/ointment
x x x
Metronidazole gel/cream – works against anaerobes
Mupiricin 2% cream/ointment
x* x
Polymyxin B sulfate x* x xPolymyxin B sulfate, Bacitracin zinc, Neomycin
x x x
Silver sulfadiazine x* x xIonized Silver x* x x
MANAGEMENT:CONTROL OF INFECTIONS If still no healing, consider presence of:
Cellulitis-- Biopsy for culture of underlying tissue, bone May need systemic antibiotics
or Osteomyelitis— Staphylococcus aureus is by far the most commonly involved X-Ray—Soft tissue swelling, bone destruction (10-21 d after
infection) CT—Medullary and cortical destruction MRI—Better for soft tissue assessment, good for early bony edema
Remember, the white-blood-cell count is not a reliable indicator and can be normal even when infection is present.
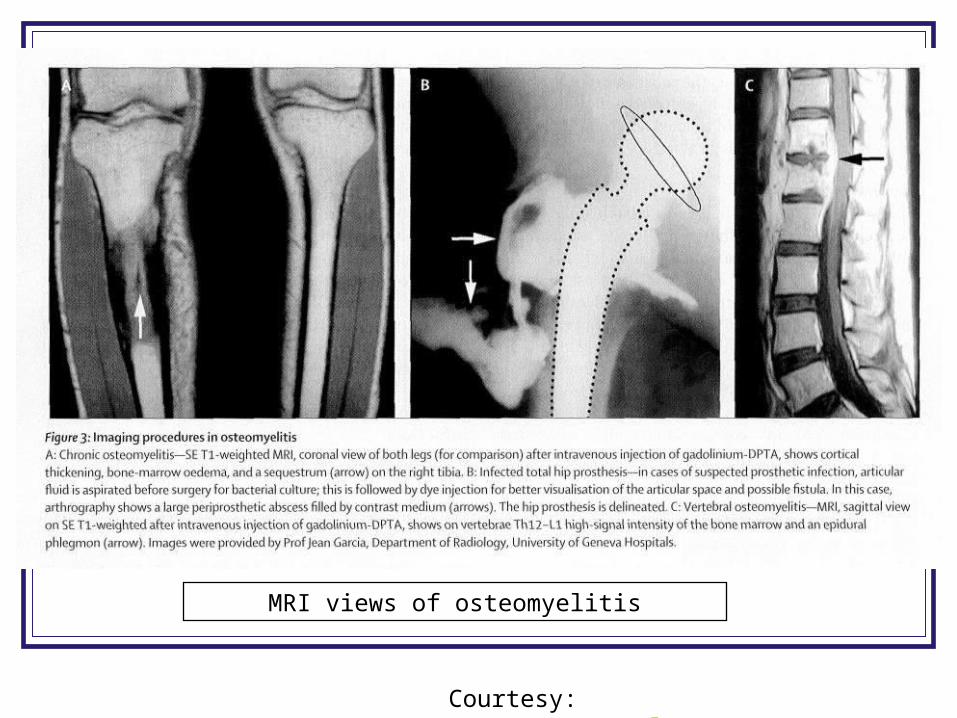
MRI views of osteomyelitis
Courtesy: Lancet 2004 Jul 24;364(9431):369
Bacterial Culture Collection Bacterial culture: IF have nonhealing
wounds, increased discharge or develop a new odor
Done selectively only IF suspect deep tissue infection
Take from cleaned wound margin Swab healthy-appearing granulation tissue
by rotating the swab in a zigzag pattern
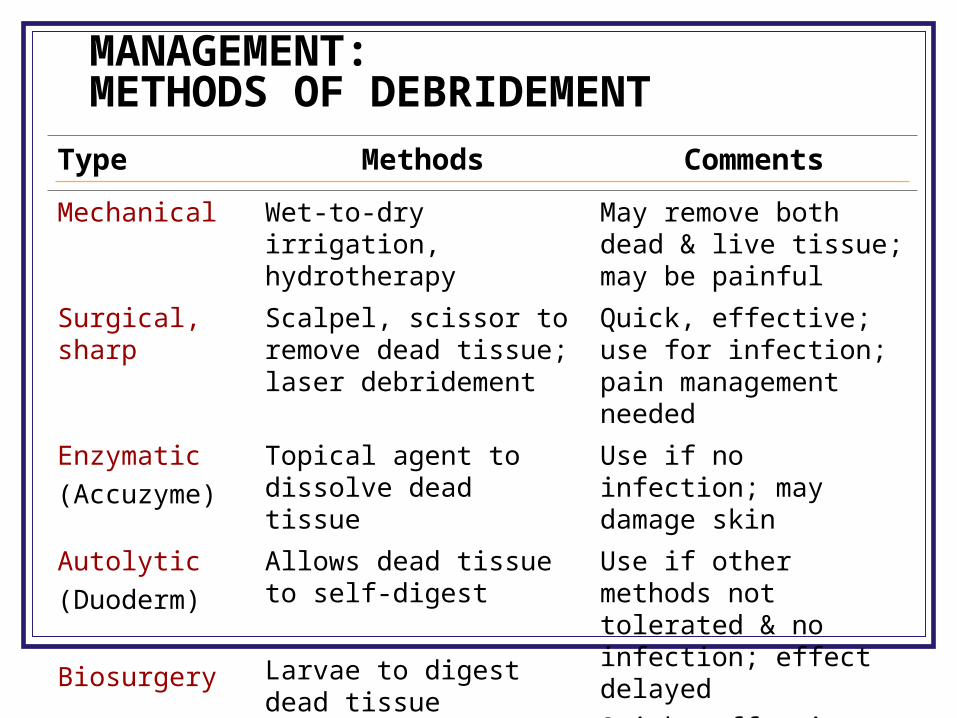
MANAGEMENT:METHODS OF DEBRIDEMENT
Type Methods Comments
Mechanical Wet-to-dry irrigation, hydrotherapy
May remove both dead & live tissue; may be painful
Surgical, sharp Scalpel, scissor to remove dead tissue; laser debridement
Quick, effective; use for infection; pain management needed
Enzymatic
(Accuzyme)
Topical agent to dissolve dead tissue
Use if no infection; may damage skin
Autolytic
(Duoderm)
Biosurgery
Allows dead tissue to self-digest
Larvae to digest dead tissue
Use if other methods not tolerated & no infection; effect delayed
Quick, effective, good if surgical debridement not an option
MANAGEMENT:DRESSINGS
Transparent film: stage I, protects from friction
Contraindicated: skin tears, draining, suspected infection
Foam island: stages II, IIIContraindicated: excessive exudate; dry, crusted wound
Hydrocolloid: stages II, III
Contraindicated: poor skin integrity, infection, wound needs packing
Petroleum-based nonadherent: stages II, III, graft sites
MANAGEMENT:DRESSINGS
Calcium Alginate: stages II, III, IV, excessive drainage
Contraindicated: dry or superficial wound with maceration
Hydrogel, amorphous: stages II, III, IV; must combine with gauze dressing
Contraindicated: maceration, excess exudate
Hydrogel, sheet: stage II, skin tears
Contraindicated: maceration, moderate to heavy exudate
Gauze packing: stages III, IV, deep wounds
MANAGEMENT:NUTRITION
If an older adult at risk for pressure ulcers has malnutrition, a nutritional assessment must be done
Markers of poor dietary and protein intake, low albumin and weight are associated with pressure ulcer development and healing
Nutrition and Ulcers—the evidence! No causal relationship found between
malnutrition and pressure ulcer development Weak evidence for nutritional support that
achieves 30 to 35 calories/kg/day and 1.25 to 1.5 g of protein/kg/day to heal pressure ulcers
Weak evidence for supplemental vitamins and minerals for pressure ulcer prophylaxis
MANAGEMENT:SURGICAL REPAIR
May be used for stage III and IV ulcersDirect closure, skin grafting, skin flaps, musculocutaneous flaps, free flaps
Risks and benefits of surgery must be carefully weighed for each patient:
• Many stage III and IV ulcers heal over a long time with local wound care
• Rate of recurrence of surgically closed pressure ulcers is high
MANAGEMENT:ADJUNCTIVE THERAPIES
No data to support low-energy laser irradiation, therapeutic ultrasound
Promising research continues: Recombinant platelet-derived growth factors Electrical stimulation Vacuum-assisted closures Warm-up therapy ( basal ulcer temperature promotes healing) Hyperbaric oxygen
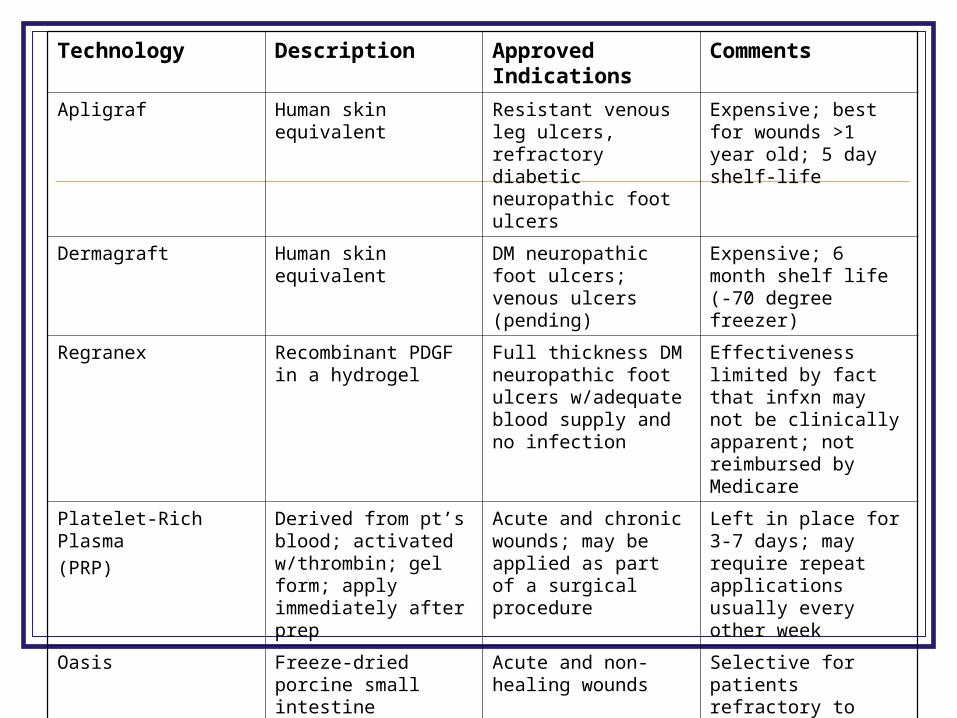
Technology Description Approved Indications
Comments
Apligraf Human skin equivalent Resistant venous leg ulcers, refractory diabetic neuropathic foot ulcers
Expensive; best for wounds >1 year old; 5 day shelf-life
Dermagraft Human skin equivalent DM neuropathic foot ulcers; venous ulcers (pending)
Expensive; 6 month shelf life (-70 degree freezer)
Regranex Recombinant PDGF in a hydrogel
Full thickness DM neuropathic foot ulcers w/adequate blood supply and no infection
Effectiveness limited by fact that infxn may not be clinically apparent; not reimbursed by Medicare
Platelet-Rich Plasma
(PRP)
Derived from pt’s blood; activated w/thrombin; gel form; apply immediately after prep
Acute and chronic wounds; may be applied as part of a surgical procedure
Left in place for 3-7 days; may require repeat applications usually every other week
Oasis Freeze-dried porcine small intestine submucosa
Acute and non-healing wounds
Selective for patients refractory to appropriate wound care; easy use; inexpensive; usually reimbursed
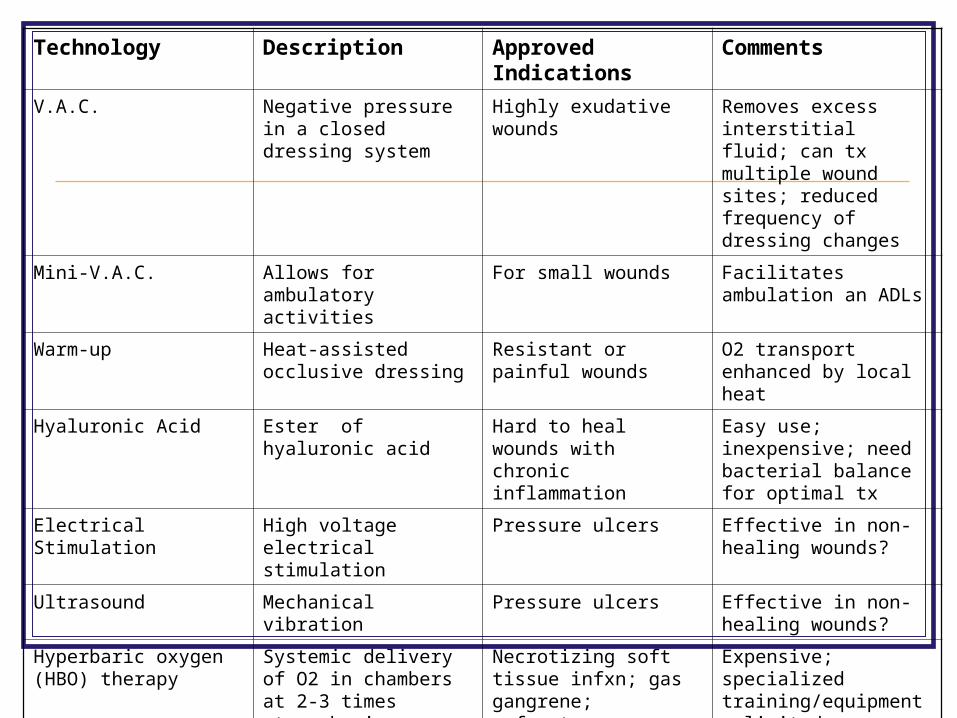
Technology Description Approved Indications
Comments
V.A.C. Negative pressure in a closed dressing system
Highly exudative wounds Removes excess interstitial fluid; can tx multiple wound sites; reduced frequency of dressing changes
Mini-V.A.C. Allows for ambulatory activities
For small wounds Facilitates ambulation an ADLs
Warm-up Heat-assisted occlusive dressing
Resistant or painful wounds
O2 transport enhanced by local heat
Hyaluronic Acid Ester of hyaluronic acid Hard to heal wounds with chronic inflammation
Easy use; inexpensive; need bacterial balance for optimal tx
Electrical Stimulation High voltage electrical stimulation
Pressure ulcers Effective in non-healing wounds?
Ultrasound Mechanical vibration Pressure ulcers Effective in non-healing wounds?
Hyperbaric oxygen (HBO) therapy
Systemic delivery of O2 in chambers at 2-3 times atmospheric pressure while breathing 100% O2
Necrotizing soft tissue infxn; gas gangrene; refractory osteomyelitis; thermal burns; radiation damage; compromised skin grafts and flaps
Expensive; specialized training/equipment; limited availability
SUMMARY
Older adults are at high risk for development of pressure ulcers
Pressure ulcers may result in serious morbidity and mortality
Techniques that reduce pressure, moisture, friction, and shear can prevent pressure ulcers
Pressure ulcers should be treated with proper cleansing, dressings, debridement, or surgery as indicated
References Geriatrics Review Syllabus, 6th edition, p259-268 Bates-Jensen, B et al. Quality Indicators for the care of pressure
ulcers in vulnerable elders; JAGS: 55:S409-S416, October 2007 AHCPR, Pressure Ulcers in Adults: Prediction and Prevention.
Rockville, MD: US Dept of Health and Human Services, Public Health Service, Agency for Healthcare Policy and Research. May 1992
Fowler E, Krasner D, et al. Healing Environments for chronic wound care: optimizing local wound management as a component of holistic interdisciplinary patient care. Treatment of Chronic Wounds: Number 11 in a series.
Krasner D, Margolis DJ, et al. Prevention and management of pressure ulcers. Treatment of Chronic Wounds: Number 6 in a series.
Patterson, BL. A Pictorial Guide to Pressure Ulcers. Consultant. Feb 2006: 205-8.
References http://www.nursingquality.org/NDNQIPressureUlcerTrain
ing/index2.htm www.medicaledu.com - Wound Care Network www.etrs.org – European Tissue Repair Society www.woundsource.com http://www.npuap.org/PDF/push3.pdf Sussman C, Bates-Jensen BM. Wound Care: A Collaborative
Practice Manual for Physical Therapists and Nurses. 1st edition. 1998.
Ham et al, Primary Care Geriatrics, 3rd ed., p.431-439 Lancet 2004 Jul 24;364(9431):369