Embed Size (px)
Citation preview

Geriatric Urology
MORGAN STOREY, MSN, APRN, FNP -C
UAMS GENERAL UROLOGY

Demographics
• Elderly (>65 years) compromise 13% total USA population
• Predicted to reach 20% by 2030
• Fastest growing segment >85 years

Introduction• 47% OF MEDICARE CLIENTS
SERVED BY UROLOGY 2006• OVER 4 MILLION MEDICARE
PATIENTS SERVED BY UROLOGY 2009

Definition • Urinary incontinence (UI):
◦ defined as the involuntary loss of urine. ◦ Stress incontinence
◦ Urge incontinence
◦ Mixed incontinence
◦ Unaware incontinence
◦ Nocturnal enuresis
◦ Continuous incontinence
• Voiding dysfunction (VD):◦ constitutes a broader definition of urinary pathology referring to any anomaly in storage and
elimination of urine.
• Nocturia:◦ >2 voids per night associated with worse sleep and QOL
• Overactive bladder (OAB): ◦ Symptoms of urgency, usually with frequency, and nocturia. ◦ Dry or wet.
UI and VD can and should be actively treated even in elderly and often frail older patients.




Epidemiology• Urinary incontinence may affect 15% to 30% of older adults living at home.
• In nursing homes the incidence of urinary incontinence has been reported to be as high as 50%.
• Lower urinary tract symptoms (LUTS) in males increases 10% per decade from 40-79 years of age.

Risk factors• For elderly men:• Prostatic enlargement
• Treatments related to prostate cancer
• For older women◦ Multiparity
◦ Pelvic organ prolapse
• Pelvic surgery (gynecologic or colorectal) and radiation can contribute to both sphincteric weakness as well as bladder instability.
• Neurologic conditions are strongly correlated with UI and VD: neurovascular accidents (i.e. stroke), spinal cord disease, multiple sclerosis and Parkinson's disease.

Causes of Urinary IncontinenceUrethral
◦ Intrinsic sphincter deficiency
◦ Urethral hypermobility
◦ Detrusor overactivity
◦ Low bladder compliance
◦ Urinary retention
Extraurethral◦ Urinary fistula
◦ Ectopic ureter

Clinical Conditions associated with Urinary Incontinence

Transient Urinary incontinence in ElderlyDIAPERS mnemonic

Medications causing UI

Evaluation• Allow time from secondary source: spouse and family, nursing
• Ask patient/family to repeat back important information: tests and plans
• Write down pertinent info for family and patient to review after visit
• Use ancillaries to check patient wounds, stoma care, medication monitoring, etc.

Considerations• Decreased hearing/vision
• Medical literacy level
• Cultural barriers
• Functional status : ◦ Activities of daily living (ADL): toilet, bathe, eat, dress
◦ Instrumental activities of daily living (IADL): phone, shop, cook, laundry
• Nutritional status
• Social status
• Legal documents

History• Precipitating factors
• Severity of incontinence
•Other voiding symptoms
•Obstetrical history
•History of genitourinary conditions
•History of pelvic surgery
•Neurological disease
•Fluid consumption
•Medications

Evaluation:Frality/cognition
• Sit-stand
• 3 meter walk
• 180◦ turn
• Mini-mental status evaluation (MMSE)

Male Evaluation• The medical history should place particular emphasis on medication use and onset of symptoms
• Rectal exam◦ DRE
◦ Stool impaction
• Lower extremities
• Focused neurological exam◦ Perineal sensation
◦ Anal sphincter tone
◦ Bulbocavernous reflex
• Discuss PSA screening if life expectancy greater than 10 years, for shared decision making.
• Uroflow/PVR


Female evaluation• Obstetric and gynecologic history
• Pelvic exam in the lithotomy position: ◦ Vaginal epithelium-atrophic changes, erythema, lesions
◦ Anterior vagina-urethral hypermobility, cystocele, urethral diverticulum
◦ Pelvic organ prolapse
◦ Exhibition of leakage. Often a standing exam can unmask pelvic organ prolapse and/or urinary incontinence that is not evident in the supine position.
• Urodynamics◦ Can be helpful in the presence of underlying neurogenic voiding
dysfunction, diabetics, when empiric therapy is unsuccessful, and in patients who have previously undergone surgery.

Office procedures

Treatment• For transient incontinence: Reverse the underlying pathology in as minimal a fashion as possible.
• Overactive bladder (OAB): 1. Behavioral
2. Physiotherapeutic
3. Pharmacologic
4. Minimally invasive
• Stress urge incontinence (SUI): Surgical intervention
• Circumvent the problem: catheter, diaper

Behavioral Modification• Fluid restriction
• Voiding diary
• Dietary modification (avoiding bladder irritants such as caffeinated beverages)
• Alterations in voiding habits, e.g. double and timed voiding schedules

Behavioral• If patients have dementia then they require additional
strategies including reminders from caregivers.

Physiotherapy
• Physiotherapy can include simple exercises but also involve biofeedback and electrical stimulation.
• Results appear to be enhanced when physiotherapy is carried out by experienced therapists.
• Pelvic floor muscle training improves stress, urge, and mixed incontinence.
• Pelvic floor muscle training can help relax the levators in dysfunctional voiding.


Pharmacological• Correct drug and dose: start low go slow, check polypharmacy
• Correct patient: commonly used source of medications to be potentially avoided in older adults is the “Beers list”
• Affordable cost: 40% of prescriptions are never picked up, cost is a major factor
• Which anticholinergic has the lowest risk of CNS effects?• Trospium (Sanctura) and Tolteroide (Detrol) cause minimal changes on EEG
• Oxybutynin (Ditropan) causes significant changes on EEG
•Memory impairment with oral Oxybutynin (Ditropan) is equivalent to 10 years of normal brain aging and the patients taking it are not aware of the deterioration

Antimuscarinics• Apart from Mirabegron (Myrbetriq) (which was launched after the 2012 Beers Criteria revision), there are currently no other oral pharmaceutical substitutes for the antimuscarinics.
• While behavioral management should be used primarily, the use of anatimuscarinics remains an important part of the management in appropriately selected patients.
• The Beers Criteria acknowledge that its use could be appropriate under certain circumstances with shared decision- making between the prescribing clinician and patient.

Pharmacological therapy for OAB

Alternative therapies for OAB

Surgical management • Generally reserved for patients who fail conservative management
• Consider: ◦ Healthy at age 65= expectancy 17 years, at 85= expectancy 7 years ; offer
normal treatment regimen
◦ two or fewer comorbidities= life expectancy less; offer regimen adapted to co-morbidities
◦ More than two comorbidities=expectancy much less; treatment to provide comfort/palliation
Adopted from: Lichtman SM. Guidelines for the treatment of elderly patients. Cancer Control. 2003; 10:445-53

Stress Urinary Incontinence• For men who have undergone radical prostatectomy
◦ artificial urinary sphincters: gold standard
◦ male sling procedures for mild cases
• For women ◦ Cystoscopic injection of urethral bulking agents
◦ Retropubic suspensions
◦ Slings midurethral/ pubovaginal
◦ Surgical correction of pelvic organ prolapse and concomitant sling may be necessary to achieve improved urinary outcomes regarding continence

Indwelling Catheter Use- F315
§483.25(d) (1) A resident who enters the facility without an indwelling catheter is not catheterized unless the resident’s clinical condition demonstrates that catheterization was necessary; and
§483.25(d) (2) A resident who is incontinent of bladder receives appropriate treatment and services to prevent urinary tract infections and to restore as much normal bladder function as possible.

Indications for an indwelling catheter beyond 14 d
1. Urinary retention that cannot be corrected medically or surgically, for which alternative therapy is not feasible, and
◦ Documented post void residual (PVR) volumes in a range over 200 milliliters (ml);
◦ Inability to manage the retention/incontinence with intermittent catheterization
◦ Persistent overflow incontinence, symptomatic infections, and/or renal dysfunction.
2. Contamination of Stage III or IV pressure ulcers with urine which has impeded healing, despite appropriate personal care for the incontinence
3. Terminal illness or severe impairment, which makes positioning or clothing changes uncomfortable, or which is associated with intractable pain.

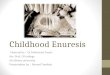
Algorithm for incontinence treatment in the Elderly

Summary• Incontinence should not be considered normal at any age.
• Even in the presence of cognitive decline or restricted mobility, UI should be evaluated and treated.
• Elderly patients require a multifactorial approach to their urologic care, and with thorough and appropriate diagnostic testing and assessment, targeted treatment plans can be developed.

ReferencesGuzzo, T. J., Drach, G. W., & Wein, A. J. (2012). Primer of Geriatric Urology. Berlin, Germany: Springer Science & Business Media.
McDougal, W. S., Wein, A. J., Kavoussi, L. R., Partin, A. W., & Peters, C. A. (2015). Campbell-Walsh Urology 11th Edition Review. St. Louis, MO: Elsevier Health Sciences.
Wieder, J. A. (2014). Pocket Guide to Urology, 5th Edition.