Embed Size (px)
Citation preview

Vasoactive Agents
in Emergency Care
Vasoactive Agents
in Emergency Care
Susan P. Torrey, M.D., FACEP
Baystate Medical Center
Tufts University School of Medicine
Susan P. Torrey, M.D., FACEP
Baystate Medical Center
Tufts University School of Medicine

Vasopressors for shockVasopressors for shock
Cochrane Database of Systematic Reviews
• “The current available evidence is not suited to inform clinical practice.”
• Mullner, et al. 2005

Vasopressors for shockVasopressors for shock
Cochrane Database of Systematic Reviews
• “there is not sufficient evidence to prove that any of the vasopressors…were superior to others”
• Havel, et al. 2011

Adrenergic receptor physiologyAdrenergic receptor physiology
• α1 adrenergic receptors
• β1 adrenergic receptors
• β2 adrenergic receptors

Adrenergic receptor physiologyAdrenergic receptor physiology
• α1 adrenergic receptors– vasoconstriction of many vascular beds– smooth muscle in arterioles
• skin, mucosa, skeletal muscle, kidneys• not cerebral and cardiac
– positive inotropic response in myocardium• with little effect on heart rate
norepinephrine, epinephrine, +/- dopamine

Pressure-dependent vascular bedsPressure-dependent vascular beds
• Heart and brain (without α-receptors)– ↑blood flow as MAP increases
• Gut and kidney (with α-receptors)– ↑blood flow as MAP ↑ to some minimal level – then vasoconstriction gut and renal ischemia
• Two primary principles of vasopressor use– a minimal MAP is imperative (MAP 65)– excessive vasopressors vital organ
compromise

Adrenergic receptor physiologyAdrenergic receptor physiology
• β1 adrenergic receptors– predominant adrenergic receptor in
myocardium– positive inotropic and chronotropic response
dobutamine, isoproterenol, epinephrine

Adrenergic receptor physiologyAdrenergic receptor physiology
• β2 adrenergic receptors– vasodilation in muscles (bronchial, uterine)
terbutaline (bronchodilator, tocolytic)

Effects of adrenergic agentsEffects of adrenergic agents
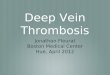
vasopressor β1 β2 α1expected effects
Dopamine ++ + ++ ↑CI,↑MAP,↑SVR
Dobutamine +++ + + ↑↑CI, -/↑ MAP
Isoproterenol +++ +++ 0 ↑↑HR
Norepinephrine ++ 0 +++ ↑↑MAP, ↑↑SVR
Epinephrine +++ ++ +++ ↑↑CI, ↑MAP
Phenylephrine 0 0 +++ ↑↑MAP, ↑↑SVR

DopamineDopamine
• Dose-dependent stimulation– Low-dose (< 5 μg/kg/min)
• dopaminergic receptors– Moderate dose (5-10 μg/kg/min)
• β1 stimulation ↑cardiac output
– High dose (> 10 μg/kg/min)
• α1 stimulation ↑ SVR

DopamineDopamine
• Expect ↑ MAP of ~ 25%
• Adverse effects– tachycardia, tachyarrhythmias– vasoconstriction-induced myocardial
ischemia– ↓ splanchnic perfusion multiple organ
failure

DobutamineDobutamine
• Potent nonselctive β- and mild α-stimulation– ↑ cardiac contractile force– +/- ↑ heart rate– ↓ cardiac-filling pressure
• Indications– decompensated CHF– with norepinephrine if CI ≤ 3 L/min/m2
• Dosage: 2 – 20 μg/kg/min

EpinephrineEpinephrine
• Potent α- and β-agonist– vasoconstriction ↑ MAP– ↑contractility and heart rate ↑cardiac
output
• Indications for low cardiac output states– cardiovascular resuscitation– anaphylaxis

NorepinephrineNorepinephrine
• Potent α1 and β1 agonist with little β2 activity– α stimulation vasoconstriction
– β1 effects balanced by reflex activity little effect on heart rate and cardiac output
• Indications– an excellent vasopressor
• Dosage: 0.5 – 30 μg/min

PhenylephrinePhenylephrine
• Selectively stimulates α1 receptors– vasoconstriction ↑SVR– as BP increases, vagal reflexes ↓heart rate
• Pure α-adrenergic agent – no ↑inotropy– distributive shock often cardiac depression– restoring MAP without ↑inotropy ↓C.O.

PhenylephrinePhenylephrine
• Indications– anesthesia-induced hypotension– spinal shock– useful with tachycardia
• arrhythmias with other vasopressors

IsoproterenolIsoproterenol
• Potent nonselective β activity– inotropic and chronotropic effects ↑CO
• Indications– temporary treatment of bradycardia– overdrive “pacing” for torsade de pointes

VasopressinVasopressin
• Antidiuretic hormone– V2 receptors on renal tubules water
resorption
• An important stress hormone– V1 receptors on vessels vasoconstriction
– V3 receptors in pituitary ACTH production
– ↑ BP only with relative hypovolemia• SIADH does not cause hypertension

VasopressinVasopressin
• Indications– catecholamine resistance in sepsis– cardiac arrest unresponsive to epinephrine– may be useful for “irreversible” shock
• Dosage– Shock – 0.01 to 0.05 U/min by infusion– ACLS – 40 U as IV bolus

Push-dose PressorsPush-dose Pressors
• Phenylephrine– In 3ml syringe, draw up 1ml from vial 10mg/ml
– Inject this into 100ml bag normal saline– Thus 100ml phenylephrine of 100μg/ml
– Draw solution into syringe; each ml = 100μg
– Dose: 0.5 – 2 ml every 2-5 min (50 – 200 μg)
• Epinephrine– Draw 9ml of NS into 10ml syringe– Add 1 ml of 1:10,000 epinephrine (100μg/ml)– Thus 10 ml of epi at 10 μg/ml
– Dose: 0.5 – 2 ml every 2-5 min (5 – 20 μg)


Case #1Case #1
50-year-old man with urticaria after bee-sting.VS: 78/40, 130, 26, 90% O2
Rx: epinephrine 0.3 mg SQ and diphenhydramine 50 mg IM continued hypotension with confusion

AnaphylaxisAnaphylaxis
• Epinephrine 0.3 – 0.5 mg (0.3 –0.5 ml of 1:000)
– SQ absorption slow – give IM– marked vasoconstriction – urticaria – β-blocker controversy
• epi less effective give more• unopposed α-effect give less

Unresponsiveto IM epinephrine
Unresponsiveto IM epinephrine
• More epinephrine– Push-dose epinephrine (100μg over 5-10 min)– IV infusion – 0.5 to 1.0 µg/min up to 10 µg/min
• Glucagon– 1 – 5 mg IV over 5 min– then 5 – 15 μg/min infusion
• Vasopressin ?

Vasopressin ?Vasopressin ?
• Schummer Anesth Analg 2008
– Six cases of anesthesia-induced anaphylaxis, unresponsive to epinephrine and fluids, had prompt hemodynamic stabilization after vasopressin (2 – 8 U).
– Helpful even in patients on β-blockers.

Case #2Case #2
70-year-old woman with altered mental status.PMH: CAD with CHF, HTN, dementiaVS: 80/48, 110, 22, 100.8°, 88% O2
Labs: WBC, BUN/Cr, CO2, pyuria remains hypotensive despite 2 liters NS IV

Current Rx of septic shockCurrent Rx of septic shock
• Aggressive fluid resuscitation – 4 - 6 liters of crystalloid (or colloid)– Vasopressors to support BP (MAP ≥ 65 mmHg)
• Dopamine or norepinephrine initially– Adjuncts to therapy
• early antibiotics• Corticosteroid ?• Activated protein C ??
Dellinger Surviving Sepsis Campaign Crit Care Med 2008

The EvidenceThe Evidence
• Annane Lancet 2007
– prospective, randomized, double-bind study– 330 patients with septic shock from France– epinephrine or norepinephrine plus dobutamine– titrated to MAP ≥ 70mmHg
– no difference in 28-day mortality or safety

The EvidenceThe Evidence
• Morelli Crit Care 2008
– prospective, randomized, controlled study– 32 patients with septic shock from Rome– MAP < 65mmHg despite adequate fluid– norepinephrine or phenylephrine for MAP 65-75– over initial 12 hours, no differences in:
• cardiopulmonary performance• global oxygen transport• regional hemodynamics

The EvidenceThe Evidence
• Myburgh Intensive Care Med 2008
– Prospective, double-blind, randomized – 280 patients from Australia– norepinehrine or epinephrine for MAP ≥ 70mmHg
– no difference to achieve MAP goal or mortality– Epinephrine had significant but transient metabolic
effects withdrawal of 13% epinephrine group

The EvidenceThe Evidence
• DeBacker Lancet 2010
– Randomized trial of 1679 patients with shock– either dopamine (to 20μg/kg/min) or
norepinephrine (up to 0.19μg/kg/min)– no difference in rate of death at 28 days– more arrhythmias in dopamine group (24% vs 12%)

Initial choice of vasopressorInitial choice of vasopressor
• With cardiac index ≥ 3.0 L/min/m2
– Norepinephrine is first choice– Phenylephrine, if brief and no cardiac dysfunction
• With cardiac index < 3.0 L/min/m2
– need more inotropic support…– Dopamine– Norepinephrine plus dobutamine
• Another possibility– Epinephrinemm
Kellum Curr Opin Crit Care 2002

If high-dose vasopressorsaren’t enough?
If high-dose vasopressorsaren’t enough?
• Addition of vasopressin may augment vasopressor treatment in septic shock
• Patel Anesth 2002
– 24 patients with severe septic shock on high-dose norepinephrine
– randomized and blinded to either more norepi or vasopressin (0.01 – 0.08 U/min)
– Baseline norepinephrine infusion signficantly reduced in vasopressin group

The EvidenceThe Evidence
• Russell N Engl J Med 2008
– Multicenter, randomized, double-blind trial– 778 patients with septic shock receiving norepi– received either norepinephrine (5-15μg/min) or
low-dose vasopressin (0.01-0.03 U/min)– no significant difference in 28-day mortality or
rates of serious adverse events
– In less severe septic shock (norepi < 15 μg/min), mortality was lower in vasopressin group (26% vs 36%)…

Case #3Case #3
70-year-old man collapses at home – v. fib arrest.After full pre-hospital ACLS asystole on arrival in ED

Vasopressin in ACLSVasopressin in ACLS
• 2010 ACLS guidelines– pulseless arrest (v. fib, v. tach or asystole)– Epinephrine 1 mg IV Q 3 – 5 min, or– Vasopressin 40 U as IV bolus x 1
• to replace first or second dose epi
• European recommendation– 1 mg epinephrine alternate 40 U
vasopressin and 1 mg epinephrine Q 3 min
Krismer Crit Care Med 2004 (Wenzel, et al. in Austria)

The EvidenceThe Evidence
• Wenzel N Engl J Med 2004
- double-blind, prospective, randomized, controlled- compared epinephrine and vasopressin
similar for v. fib. and PEA vasopressin better for asystole
- epinephrine more effective after vasopressin ?

Vasopressin in ACLSVasopressin in ACLS
Wenzel N Engl J Med 2004
VasoEpi
•% Survival to Hospital Admit– Ventricular fibrillation 46 43– PEA 33 30– Asystole 29
20
•% Survival to Discharge– Asystole 4.7
1.5

The EvidenceThe Evidence
• Aung Arch Intern Med 2005
- meta-analysis of 1519 patients with cardiac arrest from 5 randomized controlled trials
- No clear advantage of vasopressin over epi
- “ACLS should not recommend vasopressin in resusvitation protocols until more…data”

The EvidenceThe Evidence
• Gueugniaud New Engl J Med 2008
– multicenter randomized trial – 2894 out-of-hospital cardiac arrest patients– epinephrine/vasopressin vs epinephine– combination of drugs was not superior for:
• survival to hospital (20.7% vs. 21.3%)• survival to discharge (1.7% vs. 2.3%)

Case #4Case #4
48-year-old man with upper GI bleed.PMH: cirrhosisVS: 70/50, 120, 24, 98% O2
Despite aggressive Rx hypotension persists

Intractable hypotension in late-phase hemorrhagic shock
Intractable hypotension in late-phase hemorrhagic shock

Vasopressin for irreversible shock Vasopressin for
irreversible shock
69-year-old man in MVA with extensive injury
- received crystalloid, colloid, hypertonic saline
- hemorrhagic shock 2.5 mg epinephrine
- asystole arrest 40 U vasopressin + CPR
- v. fibrillation defib with 200 J
- stable BP x 20 minutes (CT and to OR)
- retroperitoneal hemorrhage uncontrolled
Haas (Wenzel) J Trauma 2004

Vasopressin for irreversible shockVasopressin for
irreversible shock

Vasopressin for irreversible shockVasopressin for irreversible shock
• Epinephrine – decreased effectiveness– hypercapnic acidosis– hypoxia
• Vasopressin better than epinephrine– better vasopressor during severe acidosis
• ? inhibition of nitric oxide vasodilation– blood from muscle, and gut heart and brain

ConclusionsConclusions
• Use norepinephrine, if you need it– Add dobutamine if need inotropic help
• Dopamine is rarely enough• When all else fails, try epinephrine• Watch vasopressin