Embed Size (px)
Citation preview

Initial Assessment and Management
Committee on Trauma Presents
Abdominal and Pelvic
Trauma

Objectives
● Identify key anatomical features of the abdomen.
● Recognize patients at risk for abdominal and pelvic injuries based on the mechanism of injury.
● Describe the evaluation of patients with suspected abdominal and pelvic injuries.
● FAST exam with Ultrasound
● Describe the acute management of abdominal and pelvic injuries.

External Anatomy of Abdomen

Abdominal Injury
When should you suspect abdominal injury?

Abdominal Injury
Blunt
●Speed
●Point of impact
●Intrusion
●Safety devices
●Position
●Ejection
When should you suspect abdominal injury? Penetrating
●Weapon
●Distance
●Number and location of wounds

Can you tell me
• What are the top 3 most commonly injured organs in the abdomen?

Abdominal Injury
●Spleen
●Liver
●Small bowel
Blunt Force MechanismCommonly Injured Organs

Abdominal Injury
●Stab● Low energy, lacerations
●Gunshot● Kinetic energy transfer● Cavitation, tumble● Fragments
Penetrating Mechanism
Any Organ at Risk

Abdominal Injury
How do I determine if there is an abdominal injury?

Abdominal Injury
How do I determine if there is an abdominal injury?
●Inspection
●Auscultation
●Percussion
●Palpation
Assessment: Physical Exam

A missed abdominal injury can cause a preventable death.
Abdominal Injury
Factors that Compromise the Exam
●Alcohol and other drugs
●Injury to brain, spinal cord
●Injury to ribs, spine, pelvis
Caution

Basilar skull / facial fractures
Can induce vomiting / aspiration
Adjuncts
●Relieves distention
●Decompresses stomach before DPL
Caution
Gastric Tube

Adjuncts
●Monitors urinary output
●Decompresses bladder before DPL
●Diagnostic
●If there is blood in meatus, do not place catheter
Caution
Urinary Catheter

Adjuncts
●No mandatory blood tests before urgent laparotomy
●Hemodynamically abnormal: type and crossmatch, coagulation studies
●Pregnancy testing
●Alcohol or other drug testing
●Hematuria (gross versus microscopic)
Blood and Urine Tests

Adjuncts
●Blunt: AP chest and pelvis
●Penetrating: AP chest and abdomen with markers (if hemodynamically normal)
X-ray Studies

Adjuncts
●Abdominal CT
●Urethrogram
●Cystogram
●IVP
●GI studies
Contrast Studies
Don’t delay definitive care!
Caution

Diagnostic Studies
Blunt Trauma

Diagnostic Studies
Penetrating Trauma – Hemodynamically NormalLower chest wounds
●Serial exams, thoracoscopy, laparoscopy, or CT scan
Anterior abdominal stab wounds
●Wound exploration, DPL, or serial exams
Back and flank stab wounds
●DPL, serial exams, or double- or triple-contrast CT scan

FAST exam

FAST
• Focused• Assessment using• Sonography for • Trauma

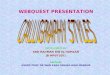
RUQ• 1) RUQ (perihepatic)
view:• Transducer
orientation: In-between pt’s ribs
• Transducer placement: right midaxillary line at level of 9th to 11th intercostal space
• Key Structures: right kidney, liver, diaphragm
• Pathology: fluid in Morison’s pouch, hemothorax

Right upper quadrant
• R Kidney
RUQ
Liver
R Kidney
Diaphragm

Morrison’s pouch + fluid

LUQ• LUQ (perisplenic) view:• Transducer orientation:
coronal (indicator towards pt’s head)
• Transducer placement: left posterior axillary line at level of 5th to 8th intercostal space
• Remember “knuckles to the bed” because of posterior location of left kidney
• Key Structures: left kidney, spleen, diaphragm
• Pathology: fluid in splenorenal space or between sleen and diaphragm, hemothorax

Left Upper QuadrantLUQ
L Kidney
Spleen
Diaphragm

LUQ +fluid

Pericardial• Subxiphoid view:• Transducer orientation:
indicator towards pt’s right• Transducer placement:
15 degree angle to the chest wall aiming transducer towards the patient’s left shoulder. Key is to lay probe almost parallel to patient
• Key Structures: liver, diaphragm, pericardial space
• Pathology: pericardial effusion

Subxiphoid view

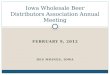
Pericardial Long• 5) Parasternal Long
view:• Transducer placement:
perpendicular to the chest wall at the 3rd or 4th intercostal space immediately left of the sternum with indicator pointing towards pt’s left shoulder
• Key Structures: right ventricle, left ventricle, left atrium, and pericardial space
• Pathology: pericardial effusion

Parasternal Long ViewParasternal Long
LA
RV
LV
Pericardial space

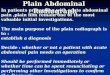
Pelvic views Longitudinal and Transverse

PELVIS• Suprapubic views
(Longitudinal and Transverse):
• Transducer orientation: – longitudinal (indicator
towards pt’s head)– transverse (indicator towards
pt’s right)• Transducer placement: just
above pubic symphysis along midline of abdomen
• Key Structures (males): bladder, retrovesicular space
• Key Structures (females): bladder, uterus, pouch of Douglas
• Pathology: fluid in retrovesicular space or pouch of Douglas
Suprapubic Female (Longitudinal)
Bladder
Pouch of Douglas
Bladder
Suprapubic Male (Transverse)
Retrovesicular space

Longitudinal view +

Transverse +

Explosions
●ABCDE
●Combination mechanism
● Blunt
● Penetrating fragments (multiple)
● BlastConsider proximity, enclosed
space, multiple fragments and secondary impacts (thrown or
fall from height).

Laparotomy
Who requires a laparotomy?

Laparotomy
Who requires a laparotomy?

Laparotomy
Indications for Laparotomy – Blunt Trauma●Hemodynamically
abnormal with suspected abdominal injury (DPL / FAST)
●Free air
●Diaphragmatic rupture
●Peritonitis
●Positive CT

Laparotomy
Indications for Laparotomy – Penetrating Trauma●Hemodynamically
abnormal
●Peritonitis
●Evisceration
●Positive DPL, FAST, or CT
Early operation is usually the best strategy for GSW

Pelvic Fractures
●Significant force
●Associated injuries
●Pelvic bleeding
● Venous / arterial

Pelvic Fractures
●Inspection
● Leg-length discrepancy, external rotation
● Open or closed
●Palpation of pelvic ring, stability
●Rectal / GU / vaginal exam
● Open or closed? Palpate prostate
Assessment of Pelvic Fractures

Pelvic Fractures
How do I manage patients with pelvic fractures?

Pelvic Fractures
●AB, as usual
●C: Control hemorrhage
● Wrap / Binder
● Rule out abdominal hemorrhage
● Angiography, fixation, open surgery
How do I manage patients with pelvic fractures?

Pelvic Fractures
Hemodynamically Abnormal Patients
Surgical consultPelvic wrap Intraperitoneal gross blood?
Yes No
Laparotomy Angiography
Control hemorrhage
Fixation device

● Delayed intervention for abdominal hemorrhage
● Occult intraabdominal / retroperitoneal injuries
● Back and flank wounds
● Repeated manipulation of a fractured pelvis
● Spinal cord injury / altered sensorium
Pitfalls
Pitfalls

Summary
●ABCDEs and early surgical consultation
●Evaluation and management vary with mechanism and physiologic response
●Repeated exams and diagnostic studies
●High index of suspicion
●Early recognition / prompt laparotomy

Case Scenario
● 35-year-old male passenger in high-speed motor vehicle collision
● BP: 105/80; Pulse: 110; RR: 18
● GCS score: 15
● Complaining of pain in chest, abdomen, and pelvis
What injuries do you suspect and how would you manage this patient?


Thanks to…
• Viam Dinh, MD• http://www.sonoguide.com/FAST.ht
ml