Embed Size (px)
Citation preview

ECMO in Cardiac Arrest
Johnny iliff
references LITFL Alfred Hospital ECMO Project
What is it ECMO is extra-corporeal membrane oxygenation extracorporeal life support (ECLS) may be a better
term The extracorporeal circuit allows for the
oxygenation and removal of carbon dioxide from blood
used as a supportive strategy in patients who have a high risk of death despite conventional therapy
Why are we considering it in the ED for Cardiac Arrest ldquoPatients with refractory ventricular fibrillation
receiving E-CPR tended to have higher survival rates and significantly improved neurological outcomes when compared with those receiving C-CPRrdquo Managing cardiac arrest with refractory ventricular fibrillation in the emergency department Conventional cardiopulmonary resuscitation versus extracorporeal cardiopulmonary resuscitation1113088 -Fu-Yuan Siao et al RESUSCITATION April 2015
Drive to start ECMO in SCGHED
Indications acute severe REVERSIBLE respiratory or cardiac
failure with a high risk of death that is refractory to conventional management
poor gas exchange compliance lt 05mLcmH2Okg PF ratio lt 100 shunt fraction gt 30
Absolute Contraindications progressive non-recoverable cardiac disease (not
transplant candidate) progressive and non-recoverable respiratory disease
(irrespective of transplant status) chronic severe pulmonary hypertension advanced malignancy GVHD gt120kg unwitnessed cardiac arrest
Relative Contraindications age gt 75 multi-trauma with multiple bleeding sites CPR gt 60 minutes multiple organ failure CNS injury
Types VV = veno-venous VA = veno-arterial peripheral or central Veno-pulmonary artery ECMO (provides short-
term right ventricular and respiratory support following LVAD insertion)
high (2 venous cannulae) vs low flow (1 venous cannula)
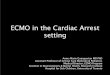
VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
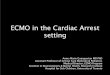
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
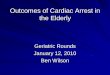
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

references LITFL Alfred Hospital ECMO Project
What is it ECMO is extra-corporeal membrane oxygenation extracorporeal life support (ECLS) may be a better
term The extracorporeal circuit allows for the
oxygenation and removal of carbon dioxide from blood
used as a supportive strategy in patients who have a high risk of death despite conventional therapy
Why are we considering it in the ED for Cardiac Arrest ldquoPatients with refractory ventricular fibrillation
receiving E-CPR tended to have higher survival rates and significantly improved neurological outcomes when compared with those receiving C-CPRrdquo Managing cardiac arrest with refractory ventricular fibrillation in the emergency department Conventional cardiopulmonary resuscitation versus extracorporeal cardiopulmonary resuscitation1113088 -Fu-Yuan Siao et al RESUSCITATION April 2015
Drive to start ECMO in SCGHED
Indications acute severe REVERSIBLE respiratory or cardiac
failure with a high risk of death that is refractory to conventional management
poor gas exchange compliance lt 05mLcmH2Okg PF ratio lt 100 shunt fraction gt 30
Absolute Contraindications progressive non-recoverable cardiac disease (not
transplant candidate) progressive and non-recoverable respiratory disease
(irrespective of transplant status) chronic severe pulmonary hypertension advanced malignancy GVHD gt120kg unwitnessed cardiac arrest
Relative Contraindications age gt 75 multi-trauma with multiple bleeding sites CPR gt 60 minutes multiple organ failure CNS injury
Types VV = veno-venous VA = veno-arterial peripheral or central Veno-pulmonary artery ECMO (provides short-
term right ventricular and respiratory support following LVAD insertion)
high (2 venous cannulae) vs low flow (1 venous cannula)
VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

What is it ECMO is extra-corporeal membrane oxygenation extracorporeal life support (ECLS) may be a better
term The extracorporeal circuit allows for the
oxygenation and removal of carbon dioxide from blood
used as a supportive strategy in patients who have a high risk of death despite conventional therapy
Why are we considering it in the ED for Cardiac Arrest ldquoPatients with refractory ventricular fibrillation
receiving E-CPR tended to have higher survival rates and significantly improved neurological outcomes when compared with those receiving C-CPRrdquo Managing cardiac arrest with refractory ventricular fibrillation in the emergency department Conventional cardiopulmonary resuscitation versus extracorporeal cardiopulmonary resuscitation1113088 -Fu-Yuan Siao et al RESUSCITATION April 2015
Drive to start ECMO in SCGHED
Indications acute severe REVERSIBLE respiratory or cardiac
failure with a high risk of death that is refractory to conventional management
poor gas exchange compliance lt 05mLcmH2Okg PF ratio lt 100 shunt fraction gt 30
Absolute Contraindications progressive non-recoverable cardiac disease (not
transplant candidate) progressive and non-recoverable respiratory disease
(irrespective of transplant status) chronic severe pulmonary hypertension advanced malignancy GVHD gt120kg unwitnessed cardiac arrest
Relative Contraindications age gt 75 multi-trauma with multiple bleeding sites CPR gt 60 minutes multiple organ failure CNS injury
Types VV = veno-venous VA = veno-arterial peripheral or central Veno-pulmonary artery ECMO (provides short-
term right ventricular and respiratory support following LVAD insertion)
high (2 venous cannulae) vs low flow (1 venous cannula)
VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

Why are we considering it in the ED for Cardiac Arrest ldquoPatients with refractory ventricular fibrillation
receiving E-CPR tended to have higher survival rates and significantly improved neurological outcomes when compared with those receiving C-CPRrdquo Managing cardiac arrest with refractory ventricular fibrillation in the emergency department Conventional cardiopulmonary resuscitation versus extracorporeal cardiopulmonary resuscitation1113088 -Fu-Yuan Siao et al RESUSCITATION April 2015
Drive to start ECMO in SCGHED
Indications acute severe REVERSIBLE respiratory or cardiac
failure with a high risk of death that is refractory to conventional management
poor gas exchange compliance lt 05mLcmH2Okg PF ratio lt 100 shunt fraction gt 30
Absolute Contraindications progressive non-recoverable cardiac disease (not
transplant candidate) progressive and non-recoverable respiratory disease
(irrespective of transplant status) chronic severe pulmonary hypertension advanced malignancy GVHD gt120kg unwitnessed cardiac arrest
Relative Contraindications age gt 75 multi-trauma with multiple bleeding sites CPR gt 60 minutes multiple organ failure CNS injury
Types VV = veno-venous VA = veno-arterial peripheral or central Veno-pulmonary artery ECMO (provides short-
term right ventricular and respiratory support following LVAD insertion)
high (2 venous cannulae) vs low flow (1 venous cannula)
VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

Indications acute severe REVERSIBLE respiratory or cardiac
failure with a high risk of death that is refractory to conventional management
poor gas exchange compliance lt 05mLcmH2Okg PF ratio lt 100 shunt fraction gt 30
Absolute Contraindications progressive non-recoverable cardiac disease (not
transplant candidate) progressive and non-recoverable respiratory disease
(irrespective of transplant status) chronic severe pulmonary hypertension advanced malignancy GVHD gt120kg unwitnessed cardiac arrest
Relative Contraindications age gt 75 multi-trauma with multiple bleeding sites CPR gt 60 minutes multiple organ failure CNS injury
Types VV = veno-venous VA = veno-arterial peripheral or central Veno-pulmonary artery ECMO (provides short-
term right ventricular and respiratory support following LVAD insertion)
high (2 venous cannulae) vs low flow (1 venous cannula)
VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

Absolute Contraindications progressive non-recoverable cardiac disease (not
transplant candidate) progressive and non-recoverable respiratory disease
(irrespective of transplant status) chronic severe pulmonary hypertension advanced malignancy GVHD gt120kg unwitnessed cardiac arrest
Relative Contraindications age gt 75 multi-trauma with multiple bleeding sites CPR gt 60 minutes multiple organ failure CNS injury
Types VV = veno-venous VA = veno-arterial peripheral or central Veno-pulmonary artery ECMO (provides short-
term right ventricular and respiratory support following LVAD insertion)
high (2 venous cannulae) vs low flow (1 venous cannula)
VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

Relative Contraindications age gt 75 multi-trauma with multiple bleeding sites CPR gt 60 minutes multiple organ failure CNS injury
Types VV = veno-venous VA = veno-arterial peripheral or central Veno-pulmonary artery ECMO (provides short-
term right ventricular and respiratory support following LVAD insertion)
high (2 venous cannulae) vs low flow (1 venous cannula)
VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

Types VV = veno-venous VA = veno-arterial peripheral or central Veno-pulmonary artery ECMO (provides short-
term right ventricular and respiratory support following LVAD insertion)
high (2 venous cannulae) vs low flow (1 venous cannula)
VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

VV ECMO most common mode venous drainage from large central veins -gt
oxygenator -gt venous system near RA support for severe respiratory failure (no cardiac
dysfunction) Proven to be improve survival 6months (63
vrs 47) with acute respiratory failure
VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

VV ECMO
Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

Pathology pneumonia ARDS -acute GVHD pulmonary contusion smoke inhalation status asthmaticus airway obstruction aspiration bridge to lung transplant drowning
VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

VA ECMO venous drainage from large central veins -gt
oxygenator -gt arterial system in aorta support for cardiac failure (+- respiratory failure)
Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

Pathology graft failure post heart or heart lung transplant non-ischaemic cardiogenic shock failure to wean post CPB bridge to LVAD drug OD Sepsis PE cardiac or major vessel trauma massive pulmonary haemorrhage pulmonary trauma acute anaphylaxis
The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

The ALFRED guidelines Patients in the EampTC with out-of-hospital cardiac arrest which is
refractory to standard advanced cardiac life support (ACLS) treatment AND
The patient meets ALL the following criteria in regards to the characteristics of the arrest
Likely due to Respiratory or Cardiac cause Witnessed arrest Chest compressions started within 10 mins Less than 60 mins duration in total 12-70 years old No major co-morbidities
The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

The patient is profoundly hypothermic (lt32degC) due to accidental exposure
The patient has taken a significant overdose of a vaso-active drug(s) (ie β-Blocker tricyclic acid digoxin etc)
Any other cause where there is likely to be reversibility of the cardiac arrest if an artificial circulation can be provided
In order to ensure that out-of-hospital cardiac arrest patients arrive within a short time-frame eligible patients will be transported by ambulance with an AutopulseTM as soon as possible after the initiation of ACLS
STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

STEPs1 Identify potential patient2 US guided Line- Venous and Arterial (Training Required)3 Prime Circuit (Training Required)4 Attach Circuit5 Intensive Care6 Optimize and treat potential casues
Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

Cannulation Itrsquos central access whatrsquos the big deal
The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

The Circuit
httpswwwyoutubecomwatchv=OM27HovykWY

httpswwwyoutubecomwatchv=OM27HovykWY