Embed Size (px)
Citation preview

ECMO for cardiac arrest patients: Update 2017
Lim Swee Han MBBS (NUS), FRCS Ed (A&E), FRCP (Edin), FAMS
Senior Consultant, Department of Emergency Medicine, Singapore General Hospital
Adjunct Associate Professor, Yong Loo Lin School of Medicine and Duke-NUS Graduate Medical School of National University of Singapore
Treasurer and Member BLS Taskforce, ILCOR
Chairman, Resusciation Council of Asia
Secretary, Asian Society for Emergency Medicine
President, Society of Emergency Medicine in Singapore

Acknowledgements
Dr Lim Jia Hao Consultant
Department of Emergency Medicine Singapore General Hospital
Dr Tan Boon Kiat Kenneth Consultant
Department of Emergency Medicine Singapore General Hospital

What is ECMO?
• The use of extracorporeal circulation and gas exchange to provide TEMPORARY life support in patients with REVERSIBLE pulmonary and/or cardiac failure.

History of ECMO
• Dimethylpolysiloxane (DMPS, silicone), was discovered in 1957, and by 1963, used in the construction of oxygenators
• It will pave the way for extracorporeal life support systems

First Successful ECLS Patient, 1971

1972 - 1975
First Cardiac ECMO Survivor, 1972
First Neonatal ECMO Survivor, 1975

ELSO
• Extracorporeal Life Support Organization
• Established 1989
• Outgrowth of a study group contributing to a registry of cases starting in 1984
• Surgeons, neonatologists, nurses, perfusionists, RTs, biomedical engineers
• Develops ECLS guidelines, textbooks, and maintains a registry

Types of ECMO
• Veno-arterial ECMO – Used for refractory cardiogenic shock and for E CPR
• Veno-venous ECMO – Usually used for respiratory failure refractory to other conventional
treatments. Conditions like severe pneumonia, Pneumonitis

V-V ECMO Indications
• Adult Respiratory Distress Syndrome (ARDS)
• Pneumonia
• Trauma
• Graft failure following lung transplantation
• Paediatric and neonatal respiratory support
– E.g., HMD, MAS, PPHN, CDH etc
– Extensive research done in this patient population

V-A ECMO
• Severe cardiac failure
– Decompensated cardiomyopathies
– Myocarditis
– Acute coronary syndromes with cardiogenic shock
– Profound cardiac depression due to drug overdose or sepsis
• Post-cardiotomy or post-heart transplant
• Cardiac arrest (<15 min, with excellent CPR)

Increased Survival
• Adult ARDS survival up to 70%
• Paeds ARDS survival up to 75%
• For cardiogenic shock:
– Myocarditis 70%
– Decompensated CMP 50%
– Cardiogenic shock with ACS 40%
• In-hospital cardiac arrest 34%
• Out-of-hospital cardiac arrest 13%

ECLS vs CPB
Feature CPB ECMO
Duration Hours Days to Months
Configuration VA bypass VA or VV
Membrane Microporous Nanoporous
Blood pump Roller Centrifugal
Circuit volume Large Small
Anticoagulation High Low
Reservoir Large Small or absent
Cannulation Central (RA to aorta) Peripheral
Patient Anaesthetized, paralysed Awake, or sedated
Management Perfusionist Nurse, Perfusionist, RT

ECMO Circuit
• About 15-30 min to prime a full circuit
• Lasts about 30 days

Components of Circuit (I)
• Access Cannula: – Distal tip has multiple holes and a main central lumen;
drains deoxygenated blood from venous system
• Return Cannula – Single end lumen; returns oxygenated blood back to
patient

Components of Circuit
• Centrifugal Pump Head – “Artificial heart” that pushes the
deoxygenatd blood into the oxygenator
– Pressure differential at inlet and outlet results in flow
• Oxygenator with integrated heat exhanger – “Artificial lung” where gas
exchange takes place – Temperature regulation

Components of Circuit (II)
• Monitor displaying venous O2 saturation and HCT • Pump console and drive motor to adjust flow • Flow probes and flow sensors • Circuit pressure monitors (pre-pump, post-pump) • Heater/cooler unit with temperature display • Frequent inspections for clots in circuit • Watch for circuit “chatter” • Minimize excessive connections e.g., stopcocks, tube
connectors etc • Minimize length • CLAMPS and TORCHLIGHT readily available

ECMO Complications (I)
• Haemorrhage • Embolism • Leg ischaemia • Infection • Anticoagulation and resultant bleeding
– Balancing act between sufficient anticoagulation, and thrombosis
• Cerebrovascular infarct / bleed • Pulmonary oedema • Sepsis • Increase in LV afterload

ECMO Complications (II)
• Non-pulsatile (if high flow VA ECMO)
• Altered physiology
• Harlequin syndrome – flow competition in the aorta (native cardiac output, vs retrograde aortic perfusion from arterial cannula), if pulmonary function impaired, then: – “Blue head”
– “Red legs”
– Always measure SpO2 and blood gases on R side


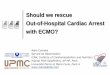
Extracorporeal membrane oxygenation support

In-hospital cardiac arrest
• Aged 18-75 who underwent CPR >10min • Cardiac origin – raised cardiac enzymes before
CPR, sudden collapse without obvious causes, or with pre-existing cardiovascular disease
Exclusion Criteria: • Severe irreversible brain damage • Terminal malignancy • Traumatic origin with uncontrolled bleeding • Non-cardiac arrest • Previously signed “Do not attempt resuscitation”
Chen, Lancet 2008, 554-61

In-hospital cardiac arrest
Chen, Lancet 2008, 554-61

In-hospital cardiac arrest
Chen, Lancet 2008, 554-61

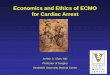
ECRP vs CCPR in adults OHCA: A prospective observational study
Inclusion criteria: 1. VF/VT initial ECG 2. Cardiac arrest on hospital arrival with or without pre-hospital ROSC 3. Within 45min from reception of the emergency call or onset of cardiac
arrest to the hospital arrival 4. No ROSC at least during the 15min after hospital arrival (ROSC defined as at least 1min of continuing confirmation of pulsation)
Exclusion criteria: 1. Under 20 years old, or 75 years and older 2. Poor level of activities of daily livings before onset of cardiac arrest 3. Non-cardiac origin (eg external factors such as trauma and drug
intoxication, primary cerebral disorders, acute aortic dissection diagnosed prior to the introduction of PCPS, and terminal phase of cancer)
4. Core body temperature less than 30°C
Sakamoto T Resuscitation 2014

Sakamoto T Resuscitation 2014


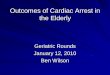
Dion et al. Resuscitation 2015
Patients with refractory OHCA were eligible for the study if • aged 18-65 years
• cardiac arrest due to suspected cardiac aetiology
• chest compressions commenced within 10 mins by bystanders or EMS
• initial cardiac arrest rhythm of ventricular fibrillation (VF)
• mechanical CPR machine (Autopulse) available
Patients with IHCA were eligible at the discretion of the attending critical care physician when it was considered likely that the cardiac arrest would be reversible if veno-arterial ECMO and definitive treatment could be provided immediately.
• Patients with IHCA were excluded if they were known to have • significant pre-existing neurological disability
• Non-cardiac co-morbidities that cause limitations in activities of daily living such as severe chronic airways disease, cirrhosis of the liver , renal failure on dialysis and terminal malignancy
• Patients with cardiac arrest and ROSC followed by cardiogenic shock who were later treated with veno-arterial ECMO are not included in this report

Dion et al. Resuscitation 2015


A Bunch of Caveats:
• Patient selection is crucial
• Centers with high volume of ECMO patients demonstrate the best outcomes
• Scrutinize the evidence – observational studies++, small numbers
• No randomized study data available for ECMO/ECLS use in cardiogenic shock

A Dash of Cold Water
• ECMO resuscitates the moribund… it cannot reanimate the dead.
• It remains a non-durable technology
• ECLS itself is a relatively simple procedure, however, the management paradigms are complex
• ECLS accomplishes nothing (non-therapeutic), but facilitates EVERYTHING – It can support patients awaiting good clinical decision
making… it is ineffective in supporting bad clinical decisions
– It truly is a bridge

End