Emergency ECMO
Emergency ECMO/E-CPRSam Phillips
CasePC29 yr old male out of hospital witnessed VF arrest.
HPCCall from St John Ambulance to say they had a 29 year old
male complaining of central chest pain.ECG performed on route.
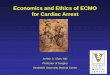
ECG from ambulance
Cath lab activated and decision to go straight up on
arrival.
Call back from SJA to say patient has now had a VF arrest
without ROSC and they are 5 mins away.Using the lucas for chest
compressionsPatient now to come through ED.
Further hx from ambulance staff and familyPatient was well this
am.Went out of the house for a couple of hours and may have used
methamphetamines.Arrived back and then developed central chest pain
and diaphoresis. (around 12.30pm).Sister called the SJA who arrived
within 10 mins.
Further collateral hxPatient has no known medical problems other
than intermittent meth use.No medicationsStrong FHx of cardiac
disease father died age 37 of an MI!mother had first MI age 50
1st ECG by SJA at 1253.VF arrest at 1310 on route.6 cycles of
CPR with 6 shocks in total given for refractory VF. Also given
amiodarone.On arrival in ED at 1335 now in PEA.
Would this patient be a potential candidate for ECMO?
Ongoing ManagementContinuation of PEA algorithm, intubated
patient.I felt good candidate for ECMO, cardiologist (Michael
Muhlman) present and agreed.Called intensivist Dave Moxon and
cardiothoracic surgeon down to ED to help to try to facilitate
this.After a further 10mins PEA, established ROSC but required
adrenaline infusion at 10mls/hr.Treatment as per STEMI
protocol.
Transferred straight up to the cath lab where he had another VF
arrest on arrival which reverted with one shock.Found blocked prox
LAD with one stent inserted.IABP inserted to support BP.Transferred
to ICU on 5mls/hr adrenaline.
Clinical courseDay 1 post arrest;increasing lactate and
abdominal distension. CT confirmed an ischaemic gut involving the
caecum and proximal small bowel.Had bowel resected.Required
haemo-filtration for acute kidney injury.Day 4Extubated, obeying
commands, sedation still wearing off.Day 7No neurological deficit
however still requiring haemo-filtration for acute kidney
injury.Day 10Off haemo-filtrationDay 14D/C home neurologically
intact.
ECMO OverviewWhat is it?Who patient selectionWhat equipmentWhy
what is the evidenceWhat can we expect at Charlies
ELSO ECMO DefinitionECMO (Extracorporeal Membrane Oxygenation)is
defined as the use of a cardiopulmonary bypass circuit for
temporary life support for patients with potentially reversible
respiratory and/or cardiac failure failing to respond to maximal
medical therapy.E-CPR (Extracorporeal Cardiopulmonary
Resuscitation) is the initiation of bypass during resuscitation of
the arresting patient.
ELSO extracorporeal life support organisation14
Two types of ECMOVV = Veno-venousVA = Veno-arterial
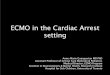
VV ECMOMost common mode used in the ICU.Provides respiratory but
no haemodynamic support.Venous drainage from large central veins
oxygenator and CO2 remover venous system near RA. Proven to improve
survival at 6 months (63% vs 47%) with acute severe respiratory
failure. (CESAR trial-Conventional Ventilatory Support vs
Extracorporeal membrane oxygenation for Severe Acute Respiratory
Failure)
CESAR trial randomly assigned 180 patients with Severe ARDS
(defined by hypercapnic resp acidosis PH 3 (quantifies severity of
lung disease based onPaO2/FiO2, PEEP, lung compliance and CXR ,to
be referred to the ECMO centre in the UK vs continued conventional
management. NB Exclusion criteria age 65, intubation >7 days, CI
to anticoagulation.16
VV ECMO
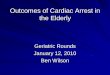
VA ECMO/E-CPRPerformed in the ED setting.Provides both
respiratory and haemodynamic support.Venous drainage from the right
atrial inlet via the CFV and infusion into the iliac artery via the
FA.Establishment of the circuit is therefore retrograde.
VA ECMO
Femoral backflow cannula19
Alfred Indications for ED ECMOPatients with out-of-hospital
cardiac arrest which is refractory to standard ACLS treatment
AND:The patient meets all of the following criteria:Likely primary
cardiac or respiratory cause.Witnessed arrest.Duration of arrest
(collapse to arrival in ED )