Embed Size (px)
Citation preview
Onn Akbar Ali
MBBS (Adelaide) FRACP
North Adelaide
Ashford Hospital
Consultant CardiologistThe Queen Elizabeth & Lyell Mc Ewin Hospitals
www.OnnAkbarAli.com
Update: Dr. Onn Akbar Ali has moved to Malaysia and now
practicing at
KPJ Kajang Specialist Hospital ( Aug 2013 onwards)
1. Increase confidence in managing chronic heart failure – appropriate use of combination therapy
2. Increase rate of beta blocker use and appropriate dose escalation- decrease reliance on “specialist”
3. Manage symptoms during dose escalation
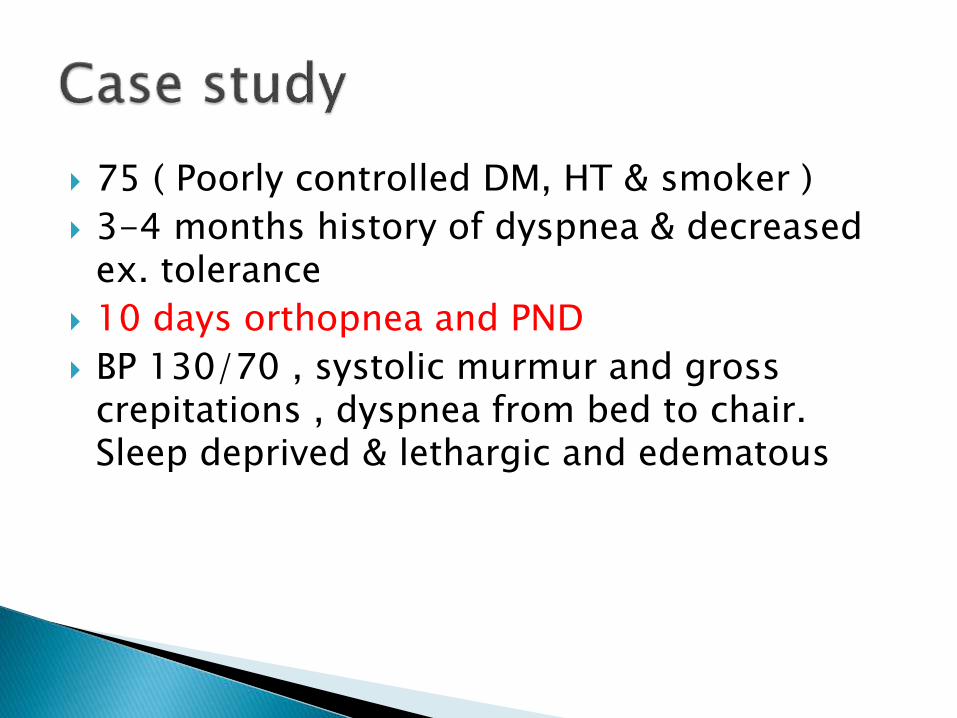
75 ( Poorly controlled DM, HT & smoker )
3-4 months history of dyspnea & decreased ex. tolerance
10 days orthopnea and PND
BP 130/70 , systolic murmur and gross crepitations , dyspnea from bed to chair. Sleep deprived & lethargic and edematous
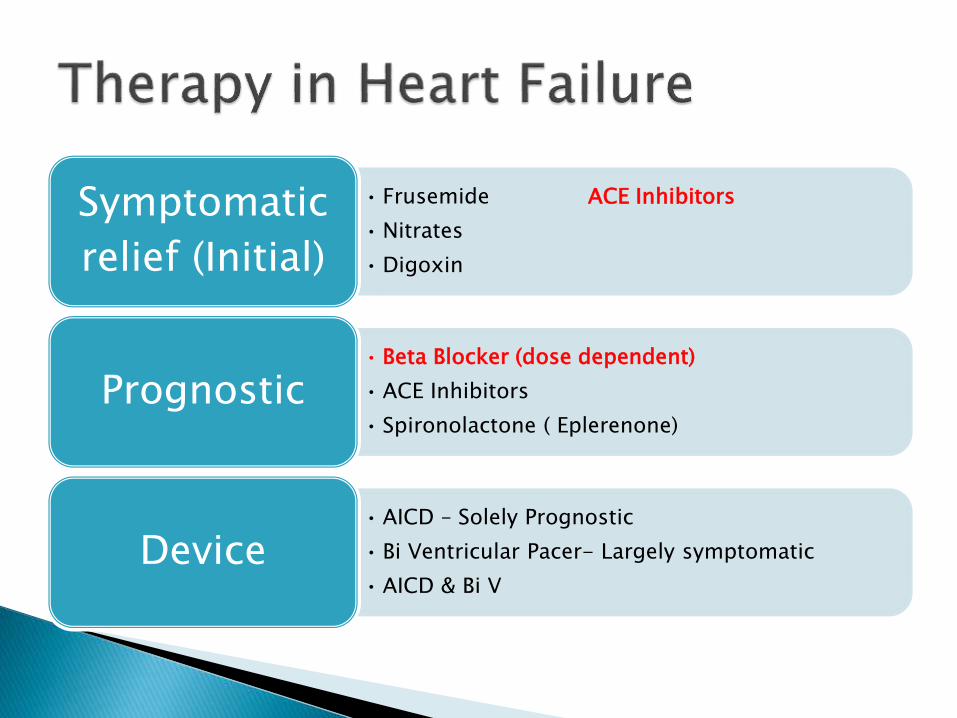
• Frusemide ACE Inhibitors
• Nitrates
• Digoxin
Symptomatic
relief (Initial)
• Beta Blocker (dose dependent)
• ACE Inhibitors
• Spironolactone ( Eplerenone)
Prognostic
• AICD – Solely Prognostic
• Bi Ventricular Pacer- Largely symptomatic
• AICD & Bi V
Device
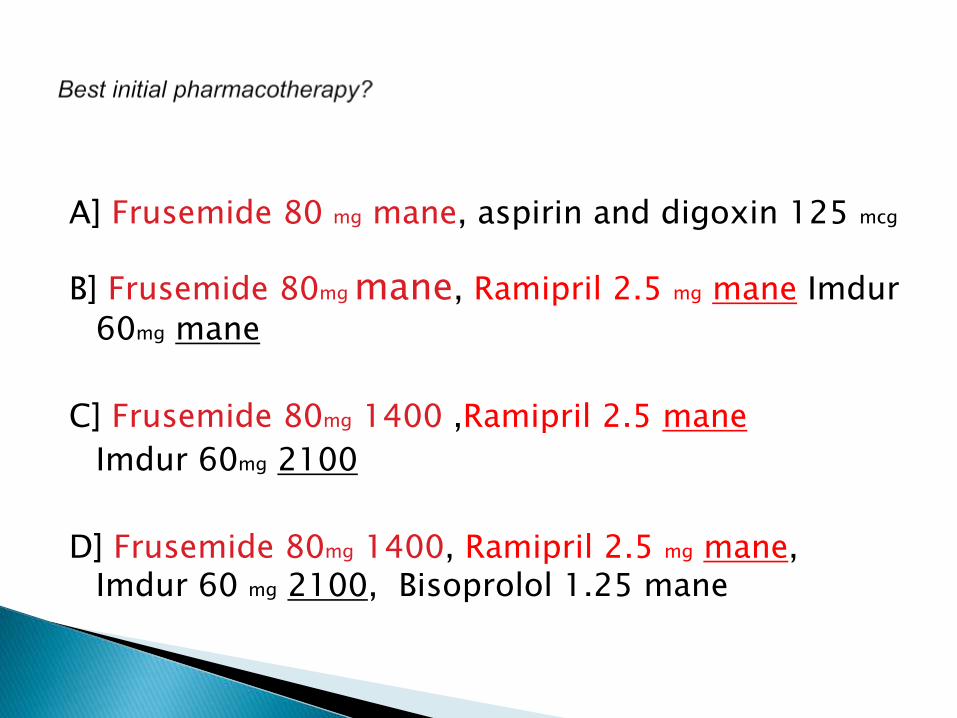
A] Frusemide 80 mg mane, aspirin and digoxin 125 mcg
B] Frusemide 80mg mane, Ramipril 2.5 mg mane Imdur
60mg mane
C] Frusemide 80mg 1400 ,Ramipril 2.5 mane
Imdur 60mg 2100
D] Frusemide 80mg 1400, Ramipril 2.5 mg mane, Imdur 60 mg 2100, Bisoprolol 1.25 mane
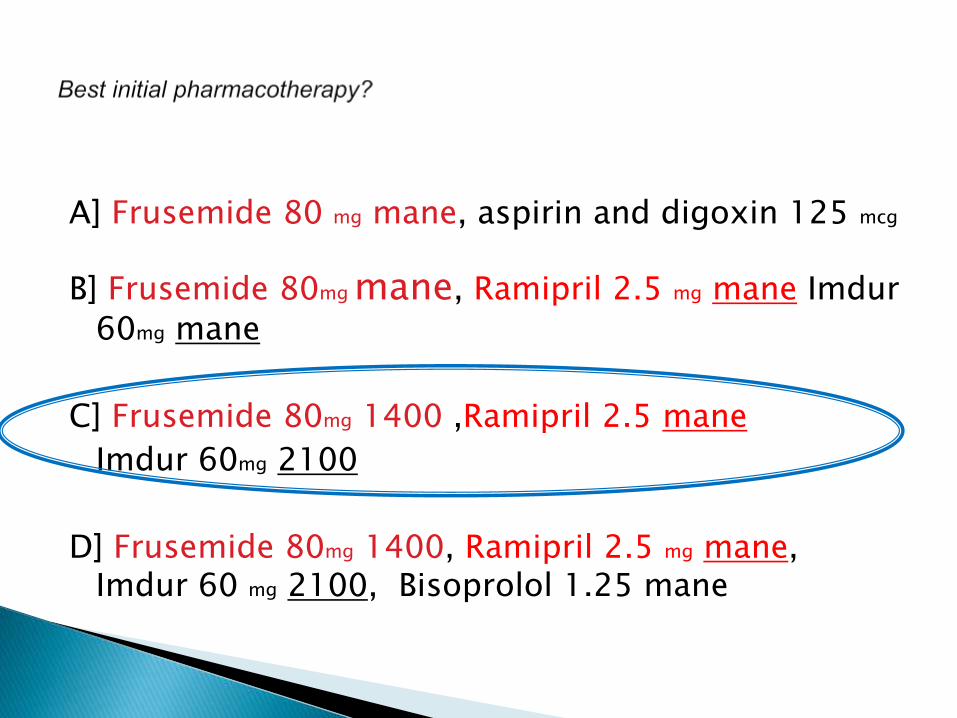
A] Frusemide 80 mg mane, aspirin and digoxin 125 mcg
B] Frusemide 80mg mane, Ramipril 2.5 mg mane Imdur
60mg mane
C] Frusemide 80mg 1400 ,Ramipril 2.5 mane
Imdur 60mg 2100
D] Frusemide 80mg 1400, Ramipril 2.5 mg mane, Imdur 60 mg 2100, Bisoprolol 1.25 mane

DrugStarting dose (mg)
Target dose/day
Doses /day
Mean total daily dose achieved in clinical trials
Angiotensin-Converting enzyme inhibitors (ACEI)
Ramipril 1.25 10 daily 1 or 2 8.7 mg
Perindopril 2.5 od 10 daily
Enalapril 2.5 20-40 mg 2 16.6 mg
Angiotensin Receptor 2 blockers
Candersartan 4 32 1 24mg
Beta Blockers
Carvedilol 3.125 bd 50-100 mg 2 37 mg
Bisoprolol 1.25 od 10 1 6.2 mg
Metoprolol CR/XL
12.5 or 25 200 1 159 mg
Aldosterone Blockers
Spironolactone 12.5 mg 50 mg 1 26 mg
Eplerenone 25 50 1 43 g
Provides symptomatic benefit
Vasodilator ( reduce after load)Vasodilatation however induce salt & fluid retention
ACEI facilitate salt and water excretion.
Reduce thirst
Reduce sympathetic drive and catecholamine level
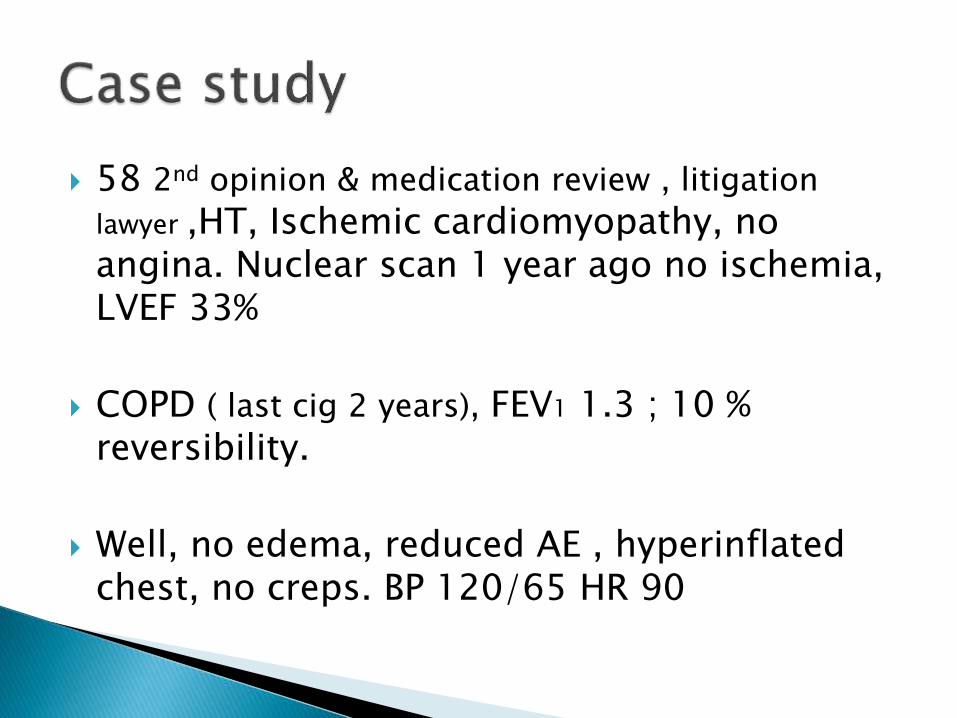
58 2nd opinion & medication review , litigation
lawyer ,HT, Ischemic cardiomyopathy, no angina. Nuclear scan 1 year ago no ischemia, LVEF 33%
COPD ( last cig 2 years), FEV1 1.3 ; 10 % reversibility.
Well, no edema, reduced AE , hyperinflated chest, no creps. BP 120/65 HR 90
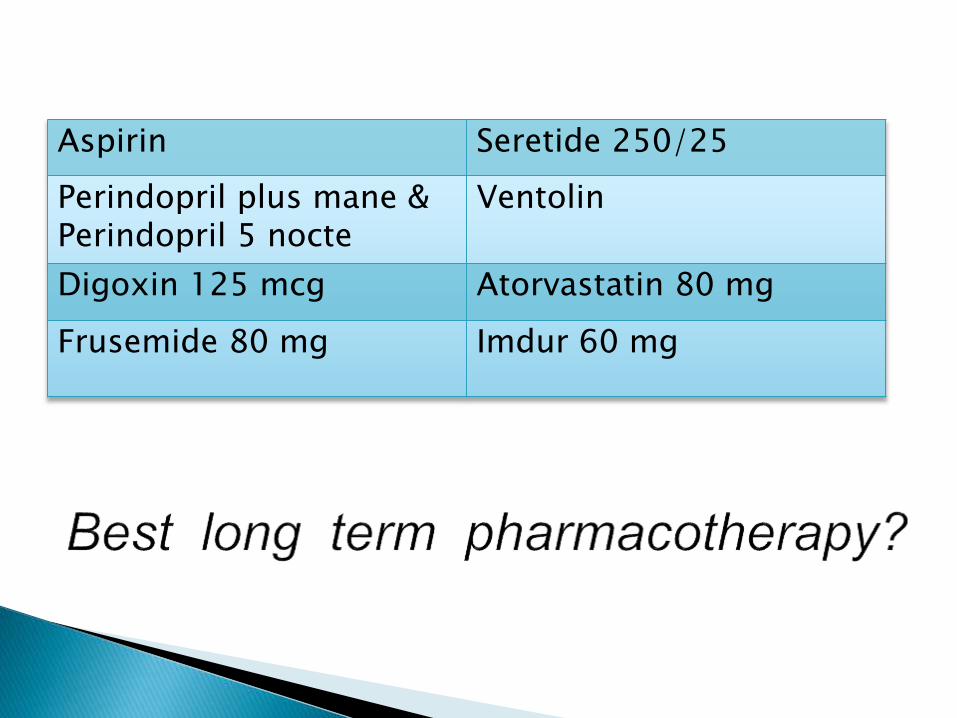
Aspirin Seretide 250/25
Perindopril plus mane &Perindopril 5 nocte
Ventolin
Digoxin 125 mcg Atorvastatin 80 mg
Frusemide 80 mg Imdur 60 mg

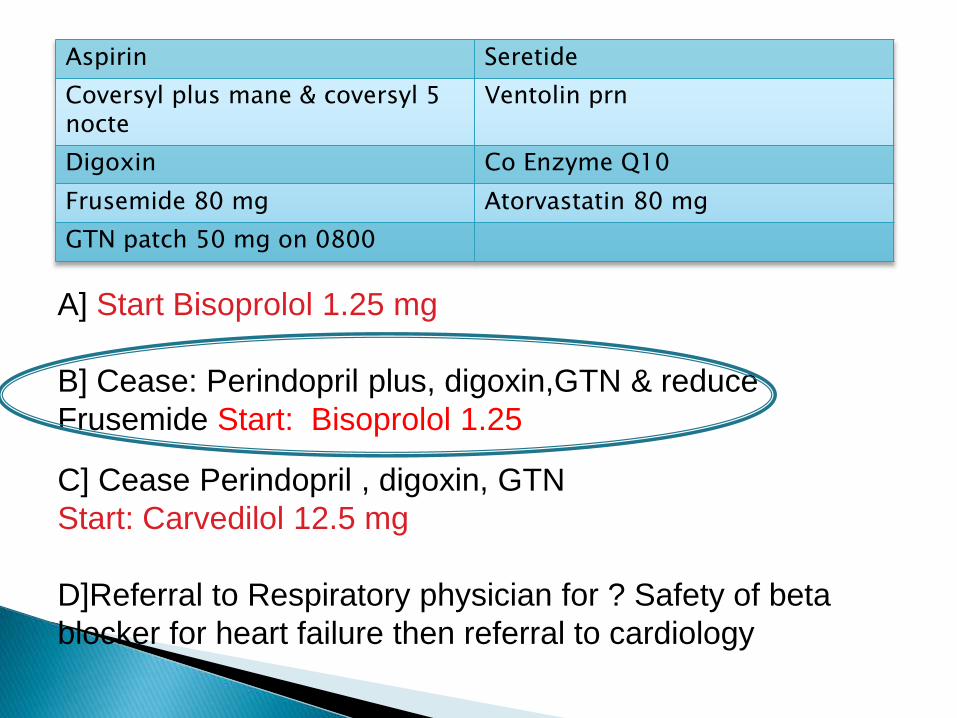
Aspirin Seretide
Coversyl plus mane & coversyl 5 nocte
Ventolin prn
Digoxin Co Enzyme Q10
Frusemide 80 mg Atorvastatin 80 mg
GTN patch 50 mg on 0800
A] Start Bisoprolol 1.25 mg
B] Cease: Perindopril plus, digoxin,GTN & reduce
Frusemide Start: Bisoprolol 1.25
C] Cease Perindopril , digoxin, GTN
Start: Carvedilol 12.5 mg
D]Referral to Respiratory physician for ? Safety of beta
blocker for heart failure then referral to cardiology
Aspirin Seretide
Coversyl plus mane & coversyl 5 nocte
Ventolin prn
Digoxin Co Enzyme Q10
Frusemide 80 mg Atorvastatin 80 mg
GTN patch 50 mg on 0800
A] Start Bisoprolol 1.25 mg
B] Cease: Perindopril plus, digoxin,GTN & reduce
Frusemide Start: Bisoprolol 1.25
C] Cease Perindopril , digoxin, GTN
Start: Carvedilol 12.5 mg
D]Referral to Respiratory physician for ? Safety of beta
blocker for heart failure then referral to cardiology
Highest prognostic benefit but under utilised
Better tolerated than generally perceived
Few contraindication; severe bradycardia and high degree heart block
( pace maker), severe bronchospasm
Even severe chronic airway disease ( FEV1 < 1.0) could tolerate beta blockers (
preferably selective e.g.. Bisoprolol) with prognostic benefit even with small dose

Start low and go slow
Prepare the patient pharmacologically and mentally
◦ ( reduce other vasoactive if appropriate and motivate patient)
Start ≤10% of the maximum dose and increase every 7-14 days
Aim maximum tolerated dose within 12 weeks or less
Excessive reliance on specialist“Need specialist supervision”
Maximum dose of ACEI before β blocker
Poor patient preparation & motivation.
Medication error.
Permanent Treatment Withdrawal or dose reduction before other measures
Adverse effects, disease progression or just myth?
Bradycardia & conduction abnormalities
Worsening Heart failure
Dizziness ,Hypotension : Lethargy & malaise
Worsens airways disease ( COPD)

COMET ( Carvedilol vsmetoprolol trial) In Carvedilol versus
placebo trial , Carvedilol significantly reduced HR
12.6±12.8 bpm vs.
1.4±12.2, P<0.001)
The Effect of Carvedilol on Morbidity and Mortality in
Patients with Chronic Heart Failure; 1996

1. Consider Holter monitor
2. Reduce or stop digoxin & amiodarone ,ensure
Verapamil or diltiazem are discontinued
3. Consider PPM (particularly biventricular device if QRS
greater than 120 and advanced conduction disease
4. β Blocker at night
Adverse effects, disease progression or just myth?
√Bradycardia & conduction abnormalities
Worsening Heart failure
Dizziness and Hypotension
Worsens airways disease ( COPD)
Lethargy & malaise
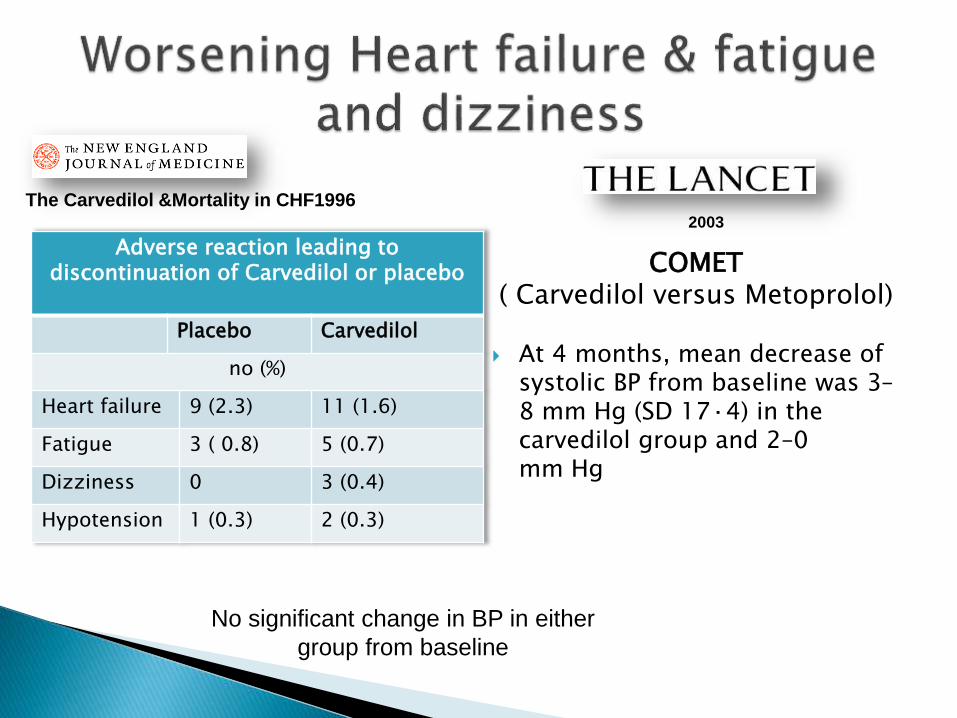
COMET( Carvedilol versus Metoprolol)
At 4 months, mean decrease of systolic BP from baseline was 3–8 mm Hg (SD 17·4) in the carvedilol group and 2–0 mm Hg
The Carvedilol &Mortality in CHF1996
Adverse reaction leading to discontinuation of Carvedilol or placebo
Placebo Carvedilol
no (%)
Heart failure 9 (2.3) 11 (1.6)
Fatigue 3 ( 0.8) 5 (0.7)
Dizziness 0 3 (0.4)
Hypotension 1 (0.3) 2 (0.3)
No significant change in BP in either
group from baseline
2003

1. Give β blocker 2 hours before/after other vasoactive agents
2. Beta blocker at bedtime & ACEI/ARB in the a.m
3. Reduce diuretics or nitrates & even ACE Iprazosin (prostate)
4. Reduce beta-blocker dose only as last resortMotivate and wait as symptoms are often self-limiting

39 %
COPD
NO
COPD
Chronic Heart FailureAHJ 2006
Majority of COPD dies from CV
disease & lung cancer related cause.
Despite clear benefit , beta blocker
under prescribed

Cardio selective β blockers, as a single
dose or chronic:
1. Produced no change in FEV1 or,
2. Respiratory symptoms
3. Do not affect the FEV1 treatment
response to beta2-agonists.
Even in subgroup participants with
severe COPD or for those with a
reversible obstructive component.
Salpeter et al; 2009
Withdrawal or reduction of beta blocker dose
Avoid dual renin angiotensin system (RAS) blockade, improve albuminuria but increased creatinine & dialysis without mortality benefit (Ontarget).
Long term , loosely supervised diuretics combination (loop, thiazide, spironolactone ).

JACC 2008
Days since Discharge
Mort
ality
rate
(%
)

Permanent withdrawal of treatment increased mortality
In CIBIS II trial 81% of withdrawal in active and placebo arms were not due to medical reason (patient and physician “personal decision” )

0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Reduced versus
stopped
Reduced or stopped
versus maintained
(unadjusted)
Reduced or stopped
versus maintained
(adjusted)
COMET: Mortality after hospitalization by whether beta-
blocker dose was stopped, reduced, or maintained
Rela
tive r
isk P=0.43
P=0.03P<0.001
Effects of beta blocker dose
reduction
Metra M. American Heart Association Scientific Sessions 2004. Nov 7-10, 2004; New Orleans, LA.

Motivate your patient !! This medication will,
make you breath better, make your heart stronger, keep you out off hospital ,
LIVE LONGER

Motivate your patient !!
It may make you feel a bit tired and very occasionally dizzy but most of the time will improve if you continue and persist
22.4% of patients in the placebo arms develop symptoms of fatigue, and 33.5% developed
worsening dyspnea
Appropriate use of combinations therapy
Lower threshold for commencing beta blocker in heart failure
Managing side effects
Majority of COPD dies from CV disease & lung cancer related
cause.
Despite clear benefit , beta blocker under prescribed
20 RCTs have shown that use of cardio selective Beta
blockers do not lead to worsening symptoms or decrease in
FEV1 even with Severe COPD or reversibility
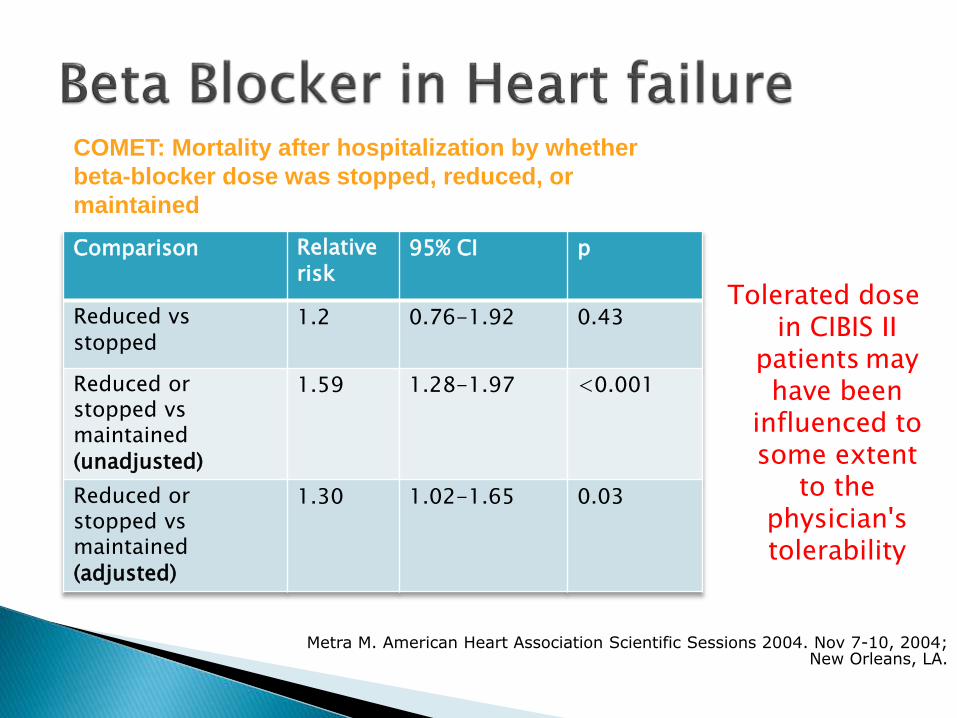
Tolerated dose in CIBIS II
patients may have been
influenced to some extent
to the physician's tolerability
Comparison Relative
risk 95% CI p
Reduced vs
stopped 1.2 0.76-1.92 0.43
Reduced or stopped vsmaintained
(unadjusted)
1.59 1.28-1.97 <0.001
Reduced or stopped vsmaintained
(adjusted)
1.30 1.02-1.65 0.03
Metra M. American Heart Association Scientific Sessions 2004. Nov 7-10, 2004; New Orleans, LA.
COMET: Mortality after hospitalization by whether
beta-blocker dose was stopped, reduced, or
maintained

Onn Akbar Ali
MBBS (Adelaide) FRACP
North Adelaide
Ashford Hospital
Consultant CardiologistThe Queen Elizabeth & Lyell Mc Ewin Hospitals
www.OnnAkbarAli.com
Update: Dr. Onn Akbar Ali has moved to Malaysia and now practicing at
KPJ Kajang Specialist Hospital ( Aug 2013 onwards)