Embed Size (px)
Citation preview

Changes Of Visual Function With Age
Arjun Sapkota B. Optometry Maharajgunj Medical Campus Institute Of Medicine

Presentation OutlineIntroduction
Visual Function Visual Acuity Colour Vision Contrast Sensitivity Dark Adaptation Visual Fields Binocular Vision
Management

Aging
The gradual, irreversible biological changes that occur over the course of time, that do not result from diseases or other accidents and eventually lead to the increased risk of death in near future

As a person ages, anatomy and physiology undergo many changes, that become more apparent with increasing age
Ageing is a progressive physiological process, characterized by degeneration of tissues and organ systems with consequent loss of functional reserves of these systems

Similarly ageing results anatomical and physiological changes in eye (as discussed in previous presentation)
These changes result in alteration of visual functions

The term refers to organ(eye) function
Are the parameters of the organ(eye) function such as VA, CV, CS VF…etc
Can generally be measured psychophysically with fair accuracy & for each eye separately
Also describe how the eyes and the basic visual system function
Visual Function

Visual FunctionsDescribe how the eye &
visual system function Eg. VA, CV, CS ,VF… etc
For each eye separately
How the person functions in vision related activities of daily living
Eg.Reading, Driving, Mobility, Daily living skills… etc
For the person as a whole
Functional Vision
Driving ability Test
Driving in actual traffic
Driving
Acuity Test
Color test
Field Test

Many elderly people experience visual problems that interfere with their daily lives
Decreased visual function is a combination of mainly aging changes in neuronal elements of visual system, changes in ocular media, and pupillary miosis

•Ocular disease and vision loss are more prevalent in the elderly population, the four leading causes of visual impairment being:
age-related macular degenerationcataractglaucomadiabetic retinopathy

There are several reasons why certain aspects of visual function deteriorate with increasing age
Optical vs Neural factors

Optical Changes
Good vision requires good optics
Vision is ultimately dependent upon the ability of the optics of the eye:
= to produce a good quality retinal image
Age related changes in the optics of the eye can have a major effect on the visual function of the elderly patient

One major change is an increase in the amount of light that is absorbed by the ocular structures along the visual axis
Blue light of wavelength (475nm)
Reduction in the transmission of light and loss of transparency is greatest in the crystalline lens but also occurs to a lesser extent in the cornea and vitreous
1. Absorption

The main consequence of increased absorption is a decrease in the amount of light that reaches the retina:
i.e. retinal illumination
The increase in absorption is much greater for shorter wavelength light

Transmission of Visible Light by Ocular Media

Another major change in the optics of the eye in later life is increased intraocular light scatter
Although increased scatter may not lead to a reduction in the amount of retinal illumination BUT
2. Scatter

it does cause image degradation due to loss of image contrast via the introduction of veiling luminance

Neural Changes
Retinal pigment epithelium (RPE), is vital for integrity of the rods and cones, shows with age:
Increased pleomorphism
Decrease in number of cells in the posterior pole
Decreased melanin content
Increased lipofuscin content
Decreased volume of cytoplasm

loss of rods and cones
Decreased in cone density
Decreased cone photo pigment density
Structural changes in the outer segments of photoreceptors
Decreased in the number of ganglionic cells & optic nerve fibres

Visual acuity
Measurement of the threshold of discrimination of the two spatially separated targets
Many studies show that acuity decreases with increasing age
A large proportion of this acuity loss is due to neural deterioration and cell death in the visual pathway

FactorsRefractive Changes
Age Related Diseases
Decreased retinal luminance
Increased light scattering
Aging neural elements

Refractive Changes
In the normal eye free from cataract and diabetes
Refractive change is hypermetropia at a rate of little more than 0.25D per decade after 40
Due to increase in axial thickness of lens and flattening of the anterior surface

1.Spherical Ametropia
Hirsch found that the median refractive state
increased from +0.18D at ages 45-49 to +1.02 over
the age of 75
The dispersion in refractive state increased markedly
with age

MyopiaPrevalence of myopia of -1.13D at ages 45 to 64
Increased to 15% (-1.29D) over the age of 75
Decreased in depth & volume of anterior chamber
Nuclear sclerosis
Factors

HyperopiaPrevalence of hyperopia of +1.13D at ages 45 to 49
Increased to 48% (+1.67D) at ages 70 to 74
Increased refractive index of vitreous
Cortical cataract
Factors

Astigmatism
Against the rule astigmatism increases in older patients while with the rule astigmatism decreases
Hirsch found that between the age of 40 & 80 the average change in astigmatism was 1.00D in the ARA
Or an average of 0.25D every 10 years

Changes in astigmatism with age could result from changes in
Corneal astigmatism Internal astigmatism Or both

On the basis of data concerning astigmatism at various stages of life;
Against the rule astigmatism
With the rule astigmatism
Against the rule astigmatism

As the upper tarsal plate begins to lose its rigidity in middle life or beyond, the horizontal meridian is allowed to steepen so that
The cornea again assumes an approx. spherical shape, resulting in a small amount of against-the-rule astigmatism
Causes

Presbyopia
Lens becomes more difficult to deform in increasing age due to lenticular sclerosis and poor elasticity of lens capsule
Near point lengthening with age, amplitude of accommodation decreases with age resulting difficulty
in near vision (decrease in near acuity)

Generally onset is thought to occur when amplitude of accommodation has decreased 5D or less
Amplitude of accommodation decreases, becomes 0 by sixth decade of life

Pathophysiology of presbyopia
Changes in the elastic properties of lens capsule
Sclerosis or hardening of the lens substance
Weakening of the ciliary muscle

Age Related Diseases
1. Cataract
2. Age related macular degeneration
3. Diabetic Retinopathy

Affects equally persons of either sex usually above the age of 50 years
Usually bilateral but almost always one eye is affected earlier than the other
Two forms: a.The cortical cataract(soft) b.The nuclear cataract(hard)
Common to find nuclear and cortical senile cataracts existing in same eye
1. Cataract

Patient with nuclear sclerosis , distant vision deteriorates:
But the near vision remains unaffected(second sight)
- Due to progressive index myopia

Change in the density of lens nucleus Compression of older fibers by new fiber formation
Increased refractive index of nucleus
Lens acts as a more conversing optical system
Increased power of the lens(i.e myopic)

2. Age related macular degeneration
Acquired retinal degeneration caused by degenerative changes in RPE with subsequent degeneration of cones and rods
Causes progressive , irreversible loss of central vision from fibrous scarring of macular area
Hypermetropia is most common Ref.. error found in ARMD

Dry/non-exudative/atrophic ARMDResponsible for 90% of cases
Causes mild to moderate, gradual loss of vision
Visual acuity ranges from 6/6 –3/60
Patients complain of disorted vision and difficulty in reading due to central shadowing

Wet/exudative/neo-vascular ARMD
Responsible for only 10% cases of ARMD
Causes rapidly progressive marked loss of vision
VA is worse than 3/60

3. Diabetic RetinopathyIs a highly specific vascular complication of both
type1 and type 2 diabetes with ageing
Change in refraction with the fluctuation in serum
glucose level
Develops early presbyopia
VA ranges from 6/6 to total blindness and decreased
vision results due to lens changes and retinal
changes(diabetic retinopathy)

Decreased retinal luminance
Young lens absorbs UV light , which damages it
This damage accumulates ,leading it to absorbs increasing amount of blue light(475nm)
The increased lenticular absorption reduces retinal illumination
1.Nuclear sclerosis
As the lens aged

2.Senile MiosisPupil becomes smaller & less responsive with age
20 years old man has a diameter of about- 5.3 mm
60 years – 3.2 mm
Senile miosis is due to: ▪ Atrophy of the dilator muscle fibers ▪ Increased rigidity of the iris blood vessels ▪ Or both

Reduction in pupil area, a 60 yr old man receives one third of the retinal luminance of 20 yr old
Cause decreased retinal blur circles and decreased retinal luminance

But has advantage of small pupil
It acts as a pinhole, thus increasing the patient’s depth of field
Patients with senile miosis have often less reliance on their spectacles, particularly under high illumination due to reduced pupillary area

Colour Vision
There is a reduction in sensitivity of the short wavelength sensitive (S) cones in later life
Whether this loss extends to the middle (M) and long (L) wavelength sensitive cones is still the matter of debate

The loss of S-cone sensitivity may be due in part to optical factors
since we know that absorption for short wavelength sensitive light increases in the elderly crystalline lens
But even when this increased absorption is accounted for S-cone sensitivity is still reduced in the older eye, suggesting that neural age changes must also play some part

Some researchers argue that the S-cone system is more susceptible to damage by the ageing process than either the L or M-cone systems

As a consequence of this reduced S-cone sensitivity elderly patients tend to exhibit more tritan like performance in colour vision tasks
This was demonstrated by Knoblauch et al. (1987) who used the Farnsworth-Munsell 100 hue test to assess the variations of colour vision with age as well as luminance

They showed increases in the error score with age with scores reaching a maximum along the near vertical axis indicating tritanopia
Tritanopia Color Spectrum

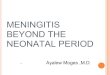
Contrast sensitivityStudies have shown that with advancing age, contrast
sensitivity declines for gratings of intermediate and high spatial frequency
There is little or no loss at low spatial frequencies
Age-related loss of contrast sensitivity can be explained through changes in:– Optical properties of the eye– Pupillary miosis– Lens opacification– Increased intraocular light scatter– Contribution of neural factors

Older individuals are only 1/3 as sensitive to low spatial frequencies(below 4 cycles/degree)as younger people
Sensitivity loss occur even in absence of diseases/degenerations even at intermediate and high frequencies

Spatial Contrast sensitivity
Generally losses at intermediate and high spatial frequencies only
The magnitude of this loss increases with increasing spatial frequency
There is greater sensitivity loss when the surrounding light levels decrease

1
10
100
1000
0.1 1 10 100
Con
tras
t Sen
sitiv
ity
Spatial Frequency (cycles/deg)
71 yrs
21 yrs

Temporal contrast sensitivity
It measures the sensitivity of the visual system to stimuli which change as a function of time ( flickering /moving )
Studies have shown that there is a loss in temporal resolution for luminance modulated uniform fields
With drifting sinusoidal grating stimuli there is a loss of contrast sensitivity with ageing even at low temporal frequencies, for both colour and luminance stimuli


Critical flicker frequencyThe rate at which consecutive visual stimuli are
presented and still be perceived as separate is called critical flicker frequency
Decline in CFF with ageing from a value of 40Hz(cycles/sec) during the fifth decade to about 30Hz in the eighth decade
The persistent miosis in the elderly contribute to this decline

Visual Field Changes with Age
Visual sensitivity across the whole visual field is adverse affected by the processes of ageing
Studies have indicated isopter constriction in older adults as well as a generalised loss in sensitivity throughout the whole of the visual field
A loss in size of visual field ranges from 3% to 3.5% in middle age to two and four times as much at 60 and above 65 years respectively

Another approach to examining the visual field is to assess the ‘functional’ or ‘useful’ field of view
This involves the localisation and identification of
complex stimuli in the periphery

Age related macular degenerationCentral & Para central Scotoma with normal
peripheral finding
Diabetic Retinopathy
In proliferative disease retinal ischemia laser scars & RD can cause corresponding field loss

Glaucoma
Early glaucomatous field defects include paracentral scotoma
Arcuate, scotoma, nasal steps & temporal wedges
Progressive VF loss occurs as the disease worsen

Sensitivity and visual thresholdVisual threshold is the minimum amount of light
necessary to see an object
Increases with age
Factors responsible are: a. Decrease in pupillary aperture results in less light input
b. Decline in the number of photoreceptor cells(rods)

c. Other ageing changes in the retina results in reduced availability and regeneration capacity of the photoreceptor pigment(rhodopsin): - leading to reduce light utilization in aged eye
This is tested by measuring change in visual threshold as a function of time spent in darkness(dark adaptation)

Dark Adaptation
Is the time dependent increase in visual sensitivity that occurs in darkness following exposure to bright illumination levels
Due to miosis and lens growth (Weale, 1962)

Numerous studies have shown that the elderly have elevated thresholds( i.e. decreased sensitivity) throughout the entire time course of dark adaptation
It reveals fundamental information about the function of rods and cones

Both the rod & cone portions of the function are affected(rods are affected before cones )
The mechanisms that underlie these changes in adaptation in the elderly may be both neural and optical components

Scotopic sensitivity
Scotopic sensitivity shows o.5 log unit decrease with age
The loss is enhanced in the perimacular region

Glare function Scattering of external light within the eye that cast a hazy
veil over the retina: - Reduces image quality Elderly patients are more sensitive to glare than younger
An increase in reaction and redetection time in the presence of a glare source

Disability GlareCaused by scatter of ocular media
Reduces contrasts Eg. person at the beach(sun, sand & light reflected off the water
Discomfort Glare When the illumination in visual field is much greater
than the level of illumination for which retina is adapted
Eg. person driving at night

Specular Glare
When patches of bright light are reflected from smooth, shiny surface into eye
eg. Light reflected off snow & ice interferes with visibility
Tested by Photostress tests

Binocular vision and ocular motor system
27 per cent of adults in their sixties have binocular vision or eye movement disorder. This number rises to 38 per cent for those over age 80.
Under scotopic conditions, aging people have
difficulty with fixation
– exotropia with age

tonic vergence with distance heterophoria
positive fusional vergence but same negative۔
fusional vergence
accommodation with AC/A ratio۔
Stereopsis: studies have suggested a decline in
stereoacuity thresholds
The range of voluntary eye movements becomes limited
– supraduction es with age

Dynamic VA and motion perception
Sensitivity to temporal modulation decreases with age for
all temporal frequencies
The ability to detect motion as measured by the minimum
displacement threshold diminishes with age

Decline in Dynamic VA with target velocity increases with increasing age
During saccadic eye movements older subjects show an increased latency of onset
To a lesser extent saccade duration and velocity may decrease with age

Older people also exhibit significantly slower smooth pursuit eye movements for targets moving at
speeds greater than 10º/s.
There is also a decrease in the ability to resolve the detail of moving stimuli (Dynamic VA)

Management
Best optical correction and home vision therapy
Progressives glasses
Bifocals and trifocals glasses
Single-vision reading glasses
Multifocal contact lenses
Tinted and coated lenses

To reduce reflected glare to the eye from viewed surfaces
Also enhances the contrasts
AR coating
Yellow tint(amber) Blue light blocker Block out the blue color Also enhances the green color

Photochromatic
Absorb UV radiation in their darkened state
- absorbs 100% UV-B(320 nm – 290 nm) - and 98% of UV-A(380 nm – 320 nm)
provide the correct amount of protection for the varying light condition
absorb UV radiation that can otherwise damage eyes

Will prevent UV light from reaching the eyes
Reducing the risk of certain eye disorders such as the formation of cataracts and macular degeneration
UV Tint

Advise the ways and means of improving their
visual functions:
– Using more light
– Substitute incandescent for fluorescent light
– Reducing driving speeds
– Avoiding looking directly into the headlights of
oncoming vehicles at night
– Closing one eye in the presence of momentary glare

References Internet
Visual perception, 2nd edition
- Stephen J Schwartz Primary Care Optometry, Theodore Grosvenor
Geriatric ophthalmology - Andrew G. Lee/Beaver A. Hilary
Previous Presentations

Thank you




![The Impact of Supplemental Antioxidants on Visual Function ... · wavelength [blue] light-filtering) properties make these com- ... with coantioxidants on visual function in patients](https://img.pdfslide.us/doc/110x75/5afd67737f8b9a994d8d6f5a/the-impact-of-supplemental-antioxidants-on-visual-function-blue-light-ltering.jpg)