Embed Size (px)
Citation preview
Examination of Visual and Vestibular Function in the Home Health Setting
Speaker(s): Diane Wrisley, PT, PhD, NCS; Sharan Zirges, PT, MSHA Session Type: Educational Sessions Session Level: Multiple Level This information is the property of the author(s) and should not be copied or otherwise used without the express written permission of the author(s).
www.homehealthsection.org
Home Health Section of the American Physical Therapy Association
Page 1 of 14 total pages
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 1
Examination of Visual and Vestibular Function in the Home
Health SettingDiane M. Wrisley PT, PhD, NCS
Sharan D. Zirges, PT, MSHA
Objectives
• By the end of this session, the participant will be able to:• Discuss the physiology and pathophysiology of vestibular and visual
function• Perform vestibular and visual assessment tools appropriate for the home• Differentiate visual signs and symptoms requiring referral for additional
assessment• Differentiate vestibular signs and symptoms requiring referral for
additional assessment
University at BuffaloPT 604
Vestibular RehabilitationDr. D. M. Wrisley
Anatomy and Physiology Review
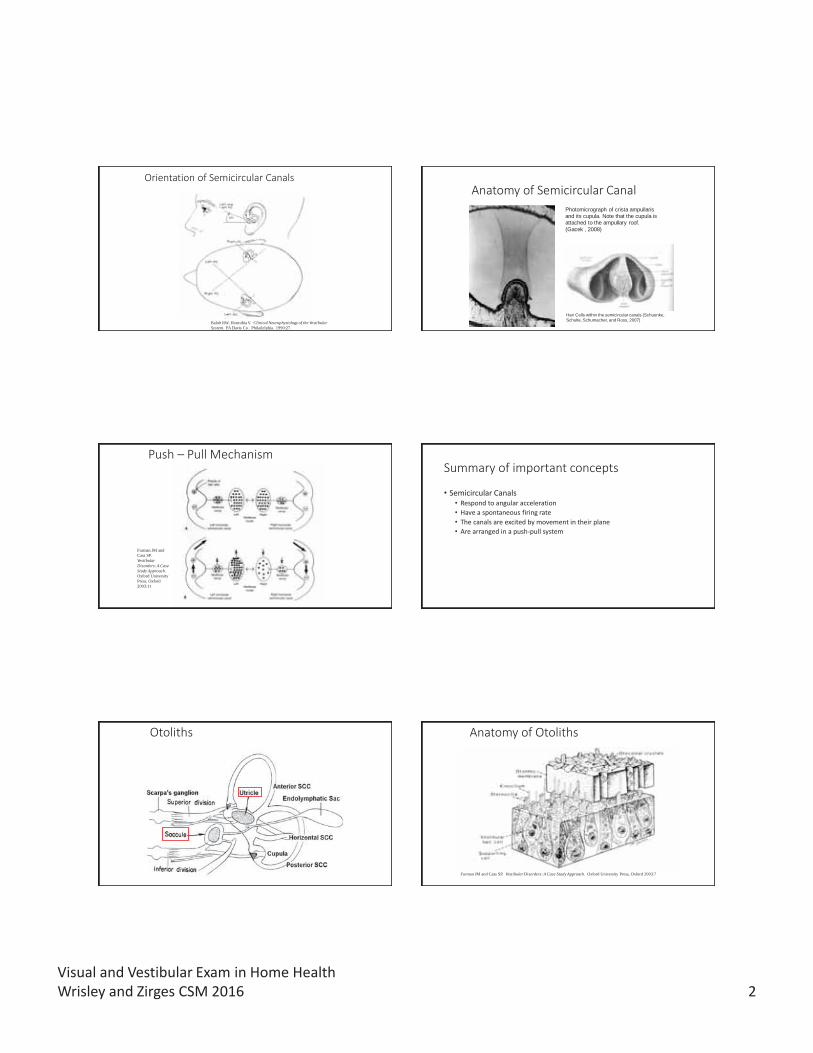
Peripheral Vestibular System
Hain TC, Hillman MA. Anatomy and physiology of the normal vestibular system. In Herdman SJ. (ed.) Vestibular Rehabilitation. FA Davis Co. Philadelphia. 1994:4
Membranous Labyrinth
Kelly JP. The sense of balance. In Kandel ER, Scwartz JH, Jessell TM. (eds) Principles of Neural Science: Third Edition. Appleton and Lange. Norwalk, CN. 1991:502
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 2
Orientation of Semicircular Canals
Baloh RW, Honrubia V. Clinical Neurophysiology of the Vestibular System. FA Davis Co. Philadelphia. 1990:27.
Anatomy of Semicircular CanalPhotomicrograph of crista ampullarisand its cupula. Note that the cupula isattached to the ampullary roof.(Gacek , 2008)
Hair Cells within the semicircular canals (Schuenke, Schulte, Schumacher, and Ross, 2007)
Push – Pull Mechanism
Furman JM and Cass SP.Vestibular Disorders: A Case Study Approach. Oxford University Press, Oxford 2003:11
Summary of important concepts
• Semicircular Canals • Respond to angular acceleration• Have a spontaneous firing rate• The canals are excited by movement in their plane• Are arranged in a push-pull system
Otoliths Anatomy of Otoliths
Furman JM and Cass SP. Vestibular Disorders: A Case Study Approach. Oxford University Press, Oxford 2003:7
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 3
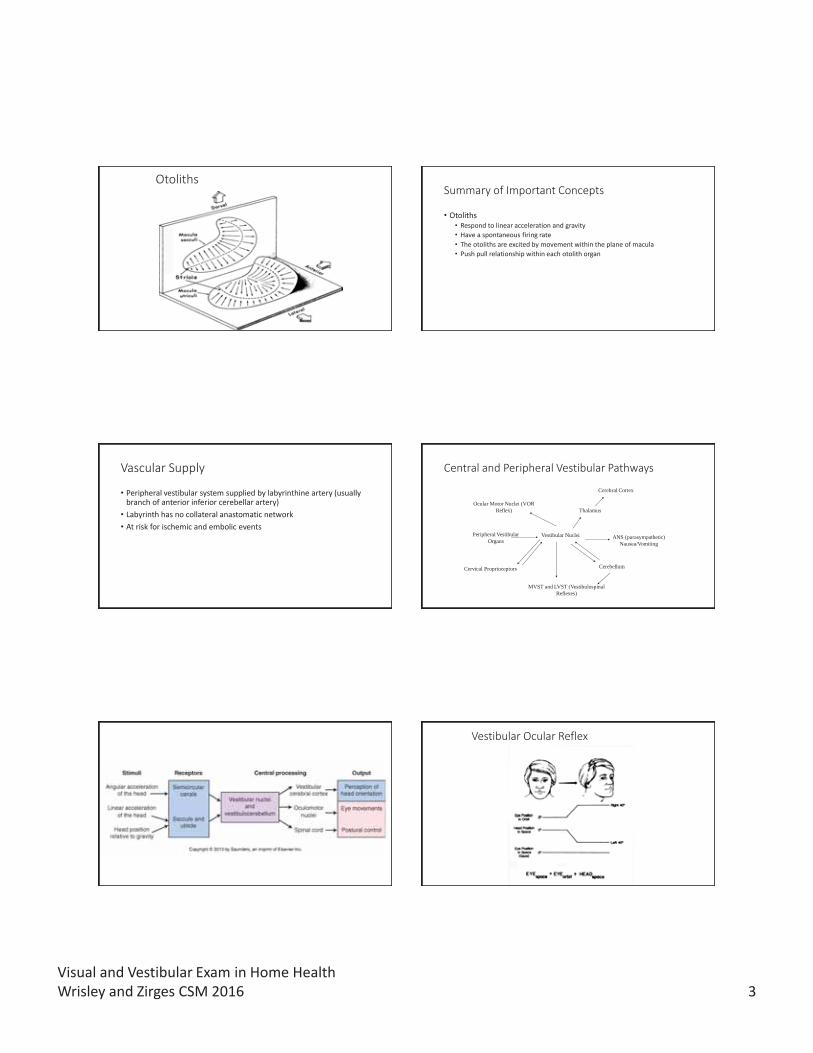
OtolithsSummary of Important Concepts
• Otoliths• Respond to linear acceleration and gravity• Have a spontaneous firing rate• The otoliths are excited by movement within the plane of macula• Push pull relationship within each otolith organ
Vascular Supply
• Peripheral vestibular system supplied by labyrinthine artery (usually branch of anterior inferior cerebellar artery)
• Labyrinth has no collateral anastomatic network • At risk for ischemic and embolic events
Central and Peripheral Vestibular Pathways
Peripheral Vestibular Organs
Vestibular Nuclei
Ocular Motor Nuclei (VOR Reflex) Thalamus
ANS (parasympathetic) Nausea/Vomiting
Cerebral Cortex
Cerebellum
MVST and LVST (Vestibulospinal Reflexes)
Cervical Proprioceptors
Vestibular Ocular Reflex
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 4
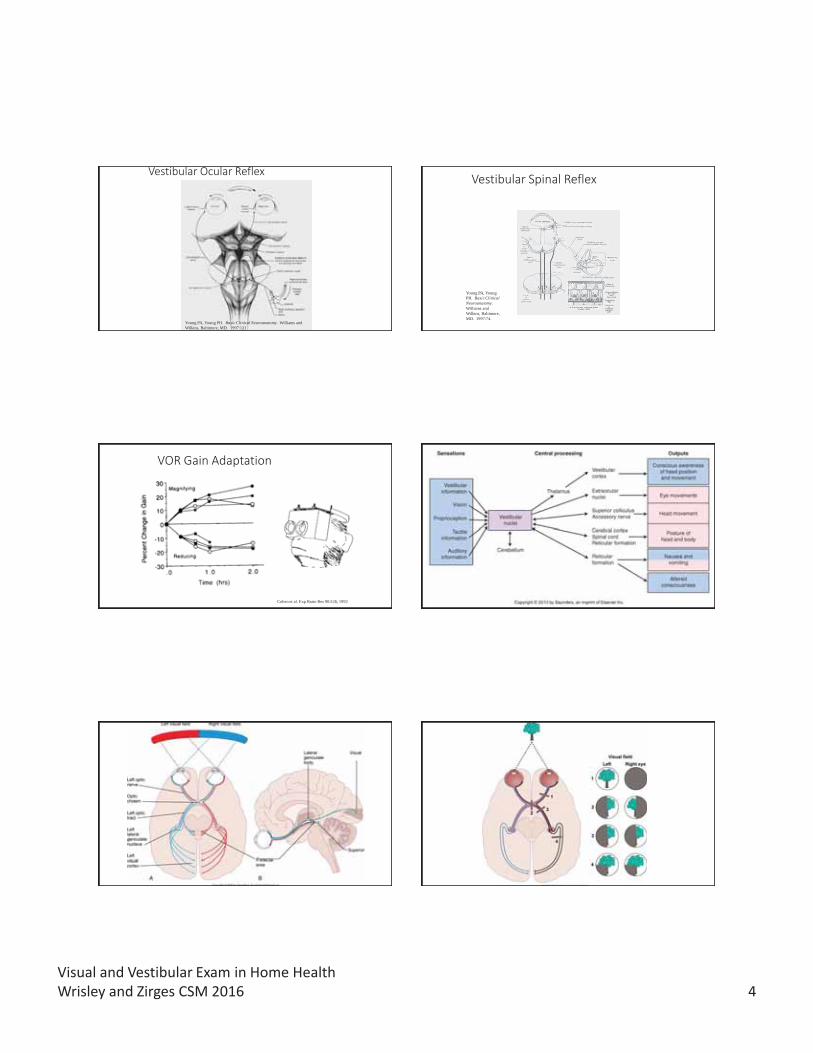
Vestibular Ocular Reflex
Vestibular RehabilitationDr. D. M. Wrisley
Young PA, Young PH. Basic Clinical Neuroanatomy. Williams and Wilkins, Baltimore, MD. 1997:121.
Vestibular Spinal Reflex
Young PA, Young PH. Basic Clinical Neuroanatomy. Williams and Wilkins, Baltimore, MD. 1997:74.
VOR Gain Adaptation
Cohen et al. Exp Brain Res 90:526, 1992
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 5
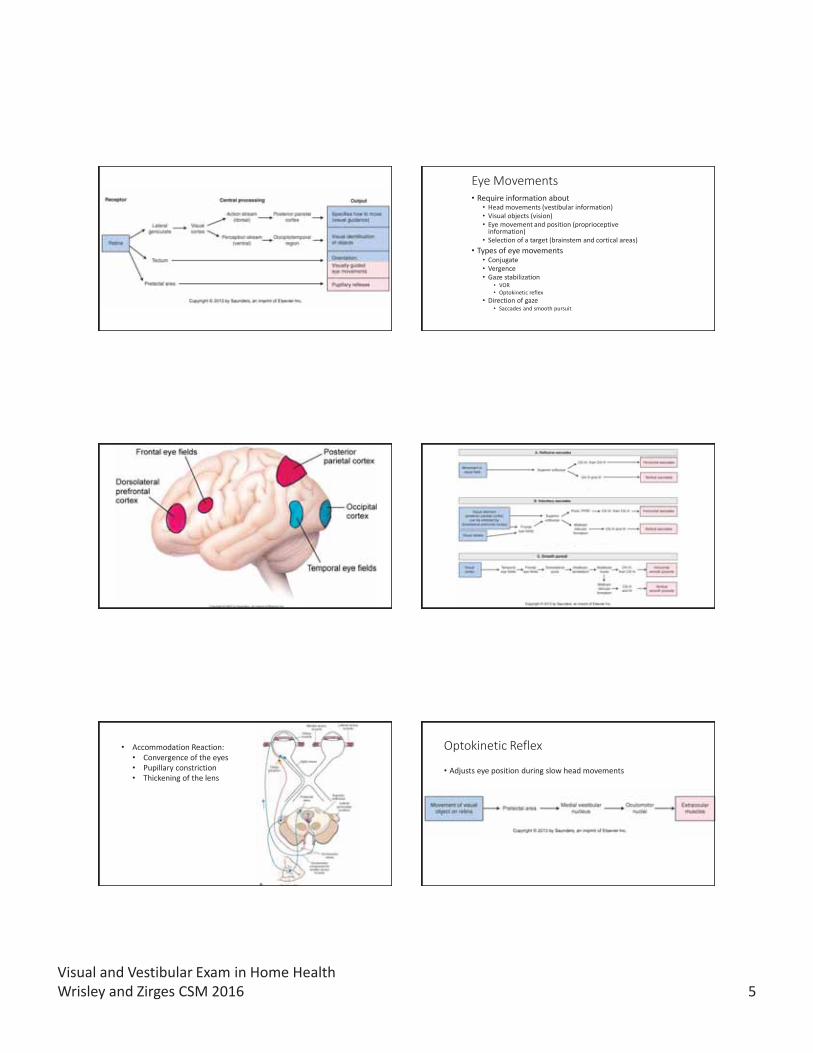
Eye Movements• Require information about
• Head movements (vestibular information)• Visual objects (vision)• Eye movement and position (proprioceptive
information)• Selection of a target (brainstem and cortical areas)
• Types of eye movements• Conjugate• Vergence• Gaze stabilization
• VOR• Optokinetic reflex
• Direction of gaze• Saccades and smooth pursuit
• Accommodation Reaction:• Convergence of the eyes• Pupillary constriction • Thickening of the lens
Optokinetic Reflex
• Adjusts eye position during slow head movements
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 6
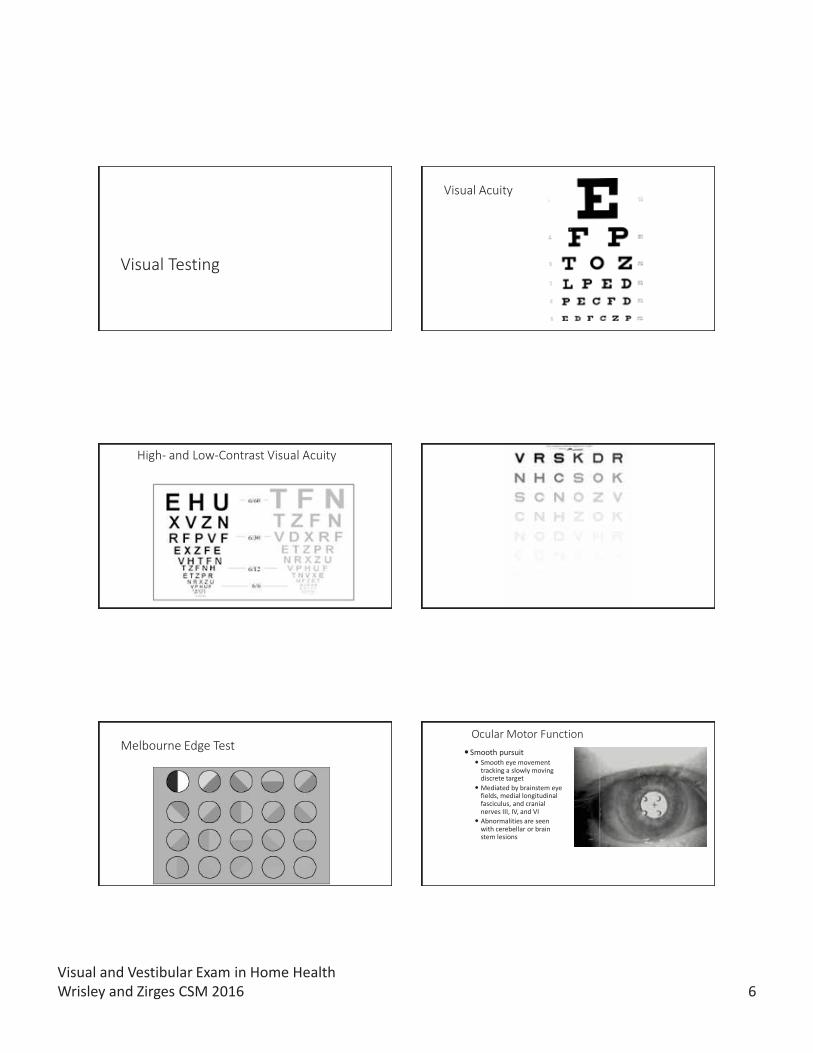
Visual Testing
Visual Acuity
High- and Low-Contrast Visual Acuity Visual Contrast Sensitivity
Melbourne Edge Test Ocular Motor Function Smooth pursuit
Smooth eye movement tracking a slowly moving discrete targetMediated by brainstem eye fields, medial longitudinal fasciculus, and cranial nerves III, IV, and VIAbnormalities are seen with cerebellar or brain stem lesions
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 7
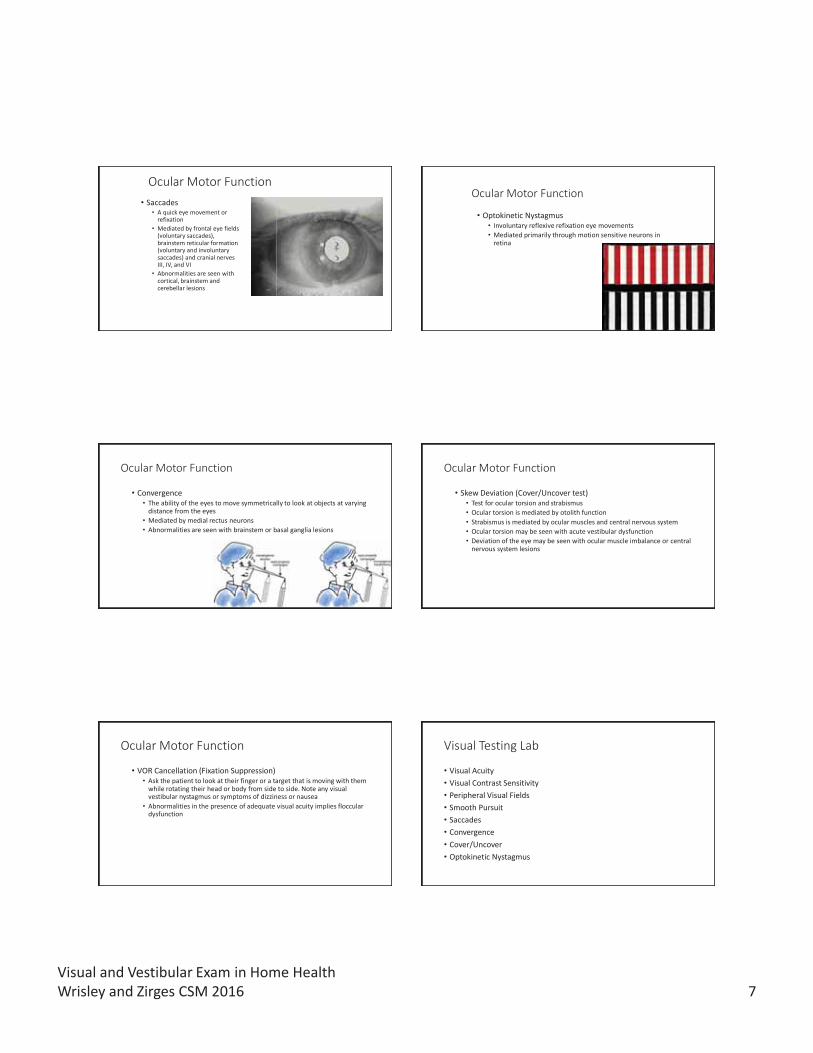
Ocular Motor Function• Saccades
• A quick eye movement or refixation
• Mediated by frontal eye fields (voluntary saccades), brainstem reticular formation (voluntary and involuntary saccades) and cranial nerves III, IV, and VI
• Abnormalities are seen with cortical, brainstem and cerebellar lesions
Ocular Motor Function
• Optokinetic Nystagmus• Involuntary reflexive refixation eye movements • Mediated primarily through motion sensitive neurons in
retina
Ocular Motor Function
• Convergence• The ability of the eyes to move symmetrically to look at objects at varying
distance from the eyes• Mediated by medial rectus neurons• Abnormalities are seen with brainstem or basal ganglia lesions
Ocular Motor Function
• Skew Deviation (Cover/Uncover test)• Test for ocular torsion and strabismus• Ocular torsion is mediated by otolith function• Strabismus is mediated by ocular muscles and central nervous system• Ocular torsion may be seen with acute vestibular dysfunction• Deviation of the eye may be seen with ocular muscle imbalance or central
nervous system lesions
Ocular Motor Function
• VOR Cancellation (Fixation Suppression)• Ask the patient to look at their finger or a target that is moving with them
while rotating their head or body from side to side. Note any visual vestibular nystagmus or symptoms of dizziness or nausea
• Abnormalities in the presence of adequate visual acuity implies flocculardysfunction
Visual Testing Lab
• Visual Acuity• Visual Contrast Sensitivity• Peripheral Visual Fields• Smooth Pursuit• Saccades• Convergence• Cover/Uncover• Optokinetic Nystagmus
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 8
Vestibular Testing
Clinical Measures of Vestibular Function
• Spontaneous Nystagmus• Look for repetitive fast and slow movements of the eyes in room light with
and without fixation and/or with fixation suppressing goggles• Direction fixed, horizontal-rotary nystagmus is indicative of an acute
asymmetry in the firing of the labyrinth, VIII cranial nerve or vestibular nucleus• The nystagmus will intensify with gaze in the direction of the fast phase
• Direction changing horizontal, vertical, torsional or pendular nystagmus is indicative of brain stem, cerebellar or cortical lesions
Clinical Measures of Vestibular Function
• Active and Passive VOR• Mediated by labyrinth, VIII cranial nerve, and vestibular nucleus• Active VOR
• While the patient looks at a target have them move their head horizontally and then vertically at about 2 cycles/second. Look for refixation saccades, note reports of dizziness or nausea
• Passive VOR• Hold the patient’s head tipped down approximately 30 degrees, move the patient’s head
horizontally and vertically at about 2 cycles/second while asking them to focus on your face. Look for refixation saccades, note reports of dizziness or nausea
• Abnormalities are indicative of vestibular dysfunction
Clinical Measures of Vestibular Function
• Dynamic Visual Acuity Longridge and Mallinson 1984
• Performed with a Snellen Eye Chart. The patient reads the lowest line comfortably with the head still and then with the head moving at 2 Hz horizontally and vertically. The number of lines of acuity lost are recorded.
• Patients with bilateral vestibular dysfunction will have a loss of >5-6 lines; patients with acute unilateral vestibular loss will have a loss of >2-3 lines
Clinical Measures of Vestibular Function
Head Thrust (Head Impulse Test) Schubert et al 2004; Halmagyi and Curthoys 1988
95% specificity, 35% sensitivity for detecting vestibular lesion
82% specificity, 71% sensitivity UVL, 84% sensitivity BVL Schubert et al 2004
The patient is asked to fixate on a target while the examiner moves the patients head rapidly to each side
The examiner looks for any movement of the pupil during the head thrust and a refixation saccade
http://library.med.utah.edu/neurologicexam/movies/cranialnerve_n_13_x2.mov
Clinical Measures of Vestibular Function
• Head Shake (Postheadshake nystagmus) Burgio et al 1991, Fetter 2000, Tseng and Chao 1997
• The head is tilted forward 30 degrees and the head is shaken at 2 Hz for 20 seconds. Observe for any postheadshake nystagmus either in room light or with fixation suppressing goggles. Can be repeated in vertical direction
• Indicative of acute imbalance in vestibular inputs in the plane of rotation
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 9
Clinical Vestibular Evaluation
• Positional Testing• Motion Sensitivity Quotient Norre and deWeerdt 1981, Smith-Wheelock et al 1991, Shepard et al 1993
• Provides an objecive score of the patient’s dizziness
• The subject moves into positions that involve head and body movement
• The patient reports a dizziness intensity score and the duration of the symptoms is recorded.
• The symptom intensity and the duration values are added to get a score. The MSQ is calculated by multiplying the number of provoking positions by the score and dividing by 2048. 0 = no symptoms; 100 = severe dizziness in all positions
• The positions can also be used for treatment
Unrecognized BPPV in the Elderly
• 100 consecutive patients referred to geriatric clinic • Age range was 51-95 (mean 74)
• Dizziness was reported by 61% of the older adults although they were not seeking intervention for dizziness
• Balance disorders were noted in 77% of the patients• 9% of these subjects had unrecognized BPPV
Oghalai JS et al, May, 2000
BPPV in the Elderly• Retrospective study of 404 patients diagnosed with
BPPV• Patients over 70 took longer to consult for problem• Presentation of unsteadiness, or imbalance without vertigo
more common in the elderly• Effectiveness of CRM less• Higher recurrence rate
Bateucas-Caetrio et al 2013
• Study of 571 75 year olds• BPPV found in 11%• Dizziness reported by 36%• People with BPPV demonstrated impaired balance and
walking testsKollen et al 2012
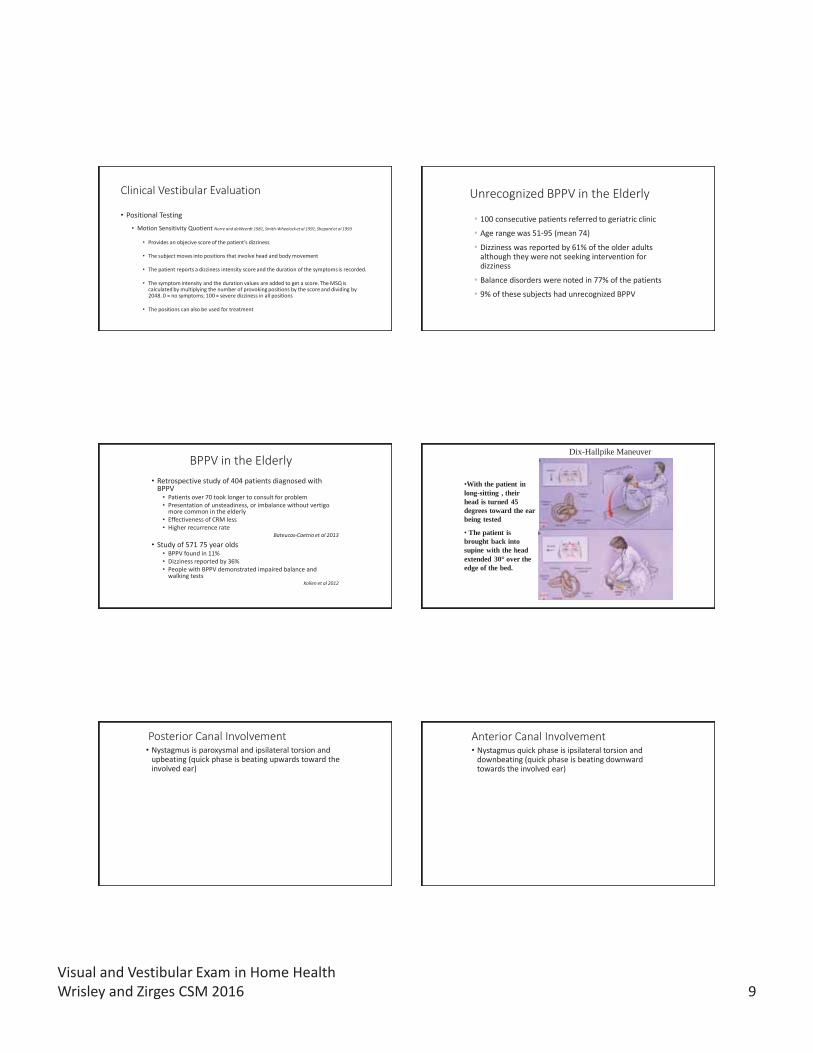
Furman and Cass. New England Journal of Medicine. 1999;340:1590-1596
•With the patient in long-sitting , their head is turned 45 degrees toward the ear being tested
• The patient is brought back into supine with the head extended 30° over the edge of the bed.
Dix-Hallpike Maneuver
Posterior Canal Involvement• Nystagmus is paroxysmal and ipsilateral torsion and
upbeating (quick phase is beating upwards toward the involved ear)
Anterior Canal Involvement• Nystagmus quick phase is ipsilateral torsion and
downbeating (quick phase is beating downward towards the involved ear)
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 10
What systems need to be checked before testing for BPPV?
• Clear cervical spine
• Ocular motor function
• Vestibular Ocular Reflex
• Vertebral artery test (?)
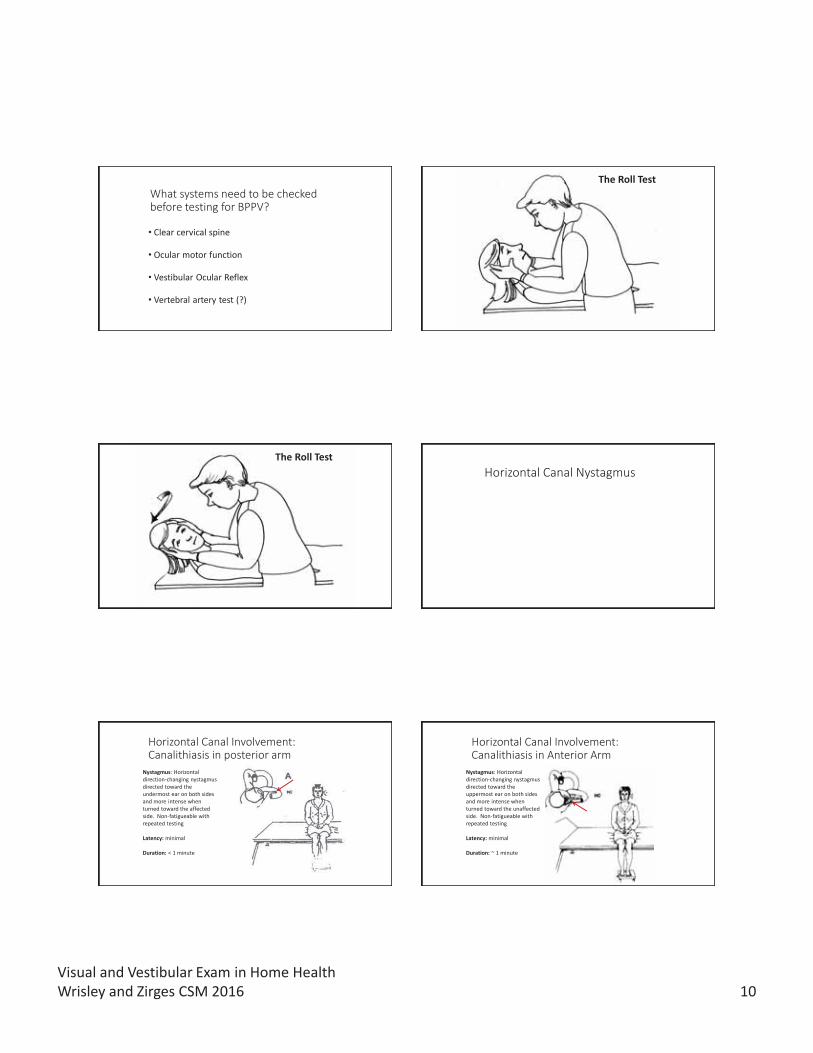
The Roll Test
Begin with the patient supine and the head in midline. Tilt the head up 30° in midline
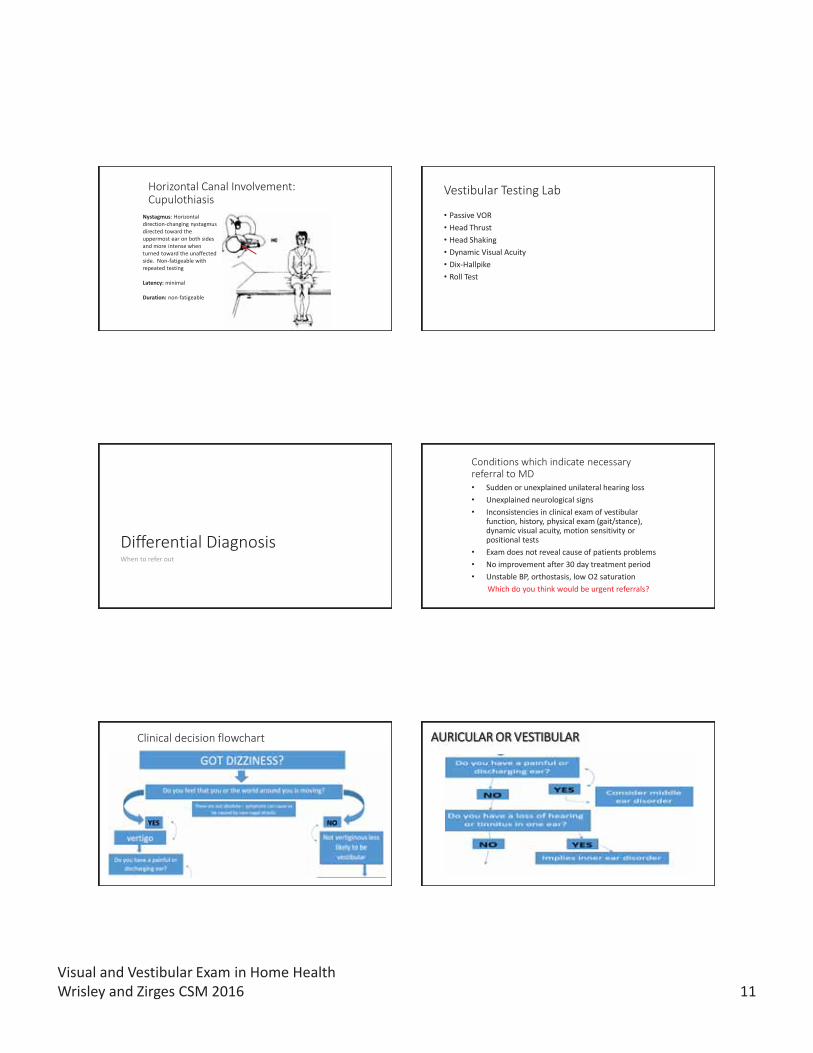
The Roll Test
Roll head quickly to one side, observe for nystagmus, ask patient to report symptoms
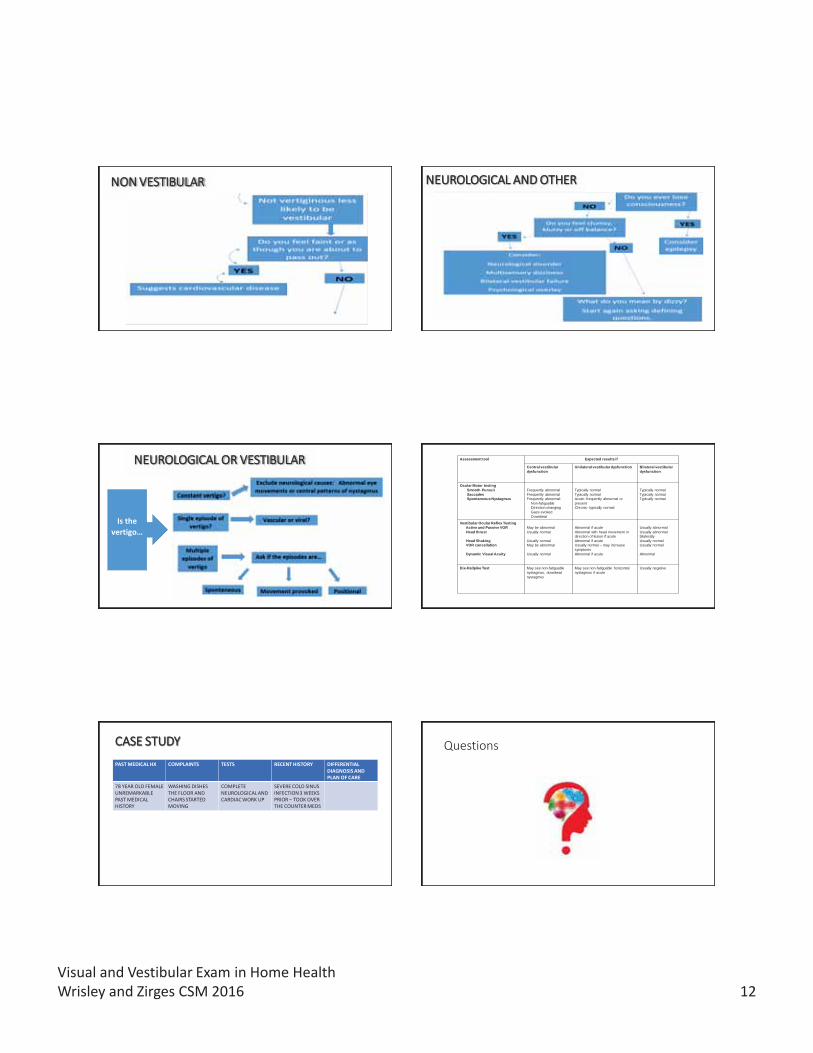
Horizontal Canal Nystagmus
Horizontal Canal Involvement: Canalithiasis in posterior arm
Nystagmus: Horizontal direction-changing nystagmus directed toward the undermost ear on both sides and more intense when turned toward the affected side. Non-fatigueable with repeated testing
Latency: minimal
Duration: < 1 minute
Horizontal Canal Involvement: Canalithiasis in Anterior Arm
Nystagmus: Horizontal direction-changing nystagmus directed toward the uppermost ear on both sides and more intense when turned toward the unaffected side. Non-fatigueable with repeated testing
Latency: minimal
Duration: ~ 1 minute
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 11
Horizontal Canal Involvement: Cupulothiasis
Nystagmus: Horizontal direction-changing nystagmus directed toward the uppermost ear on both sides and more intense when turned toward the unaffected side. Non-fatigeable with repeated testing
Latency: minimal
Duration: non-fatigeable
Vestibular Testing Lab
• Passive VOR• Head Thrust• Head Shaking• Dynamic Visual Acuity• Dix-Hallpike• Roll Test
Differential DiagnosisWhen to refer out
Conditions which indicate necessary referral to MD• Sudden or unexplained unilateral hearing loss• Unexplained neurological signs• Inconsistencies in clinical exam of vestibular
function, history, physical exam (gait/stance), dynamic visual acuity, motion sensitivity or positional tests
• Exam does not reveal cause of patients problems• No improvement after 30 day treatment period• Unstable BP, orthostasis, low O2 saturation
Which do you think would be urgent referrals?
Clinical decision flowchart AAURICULAR OR VESTIBULAR
Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 12
NNON VESTIBULAR NEUROLOGICAL AND OTHER
NEUROLOGICAL OR VESTIBULAR
Is the vertigo…
Assessment tool Expected results if
Central vestibular dysfunction
Unilateral vestibular dysfunction Bilateral vestibular dysfunction
Ocular Motor testingSmooth Pursuit SaccadesSpontaneous Nystagmus
Frequently abnormalFrequently abnormalFrequently abnormal:
Non-fatiguableDirection changingGaze evokedDownbeat
Typically normalTypically normalAcute: frequently abnormal or present Chronic: typically normal
Typically normalTypically normalTypically normal
Vestibular Ocular Reflex Testing Active and Passive VORHead thrust
Head Shaking VOR cancellation
Dynamic Visual Acuity
May be abnormalUsually normal
Usually normalMay be abnormal
Usually normal
Abnormal if acuteAbnormal with head movement in direction of lesion if acuteAbnormal if acuteUsually normal – may increase symptomsAbnormal if acute
Usually abnormalUsually abnormal bilaterallyUsually normalUsually normal
Abnormal
Dix-Hallpike Test May see non-fatiguable nystagmus, downbeat nystagmus
May see non-fatiguable horizontal nystagmus if acute
Usually negative
CASE STUDYPAST MEDICAL HX COMPLAINTS TESTS RECENT HISTORY DIFFERENTIAL
DIAGNOSIS AND PLAN OF CARE
78 YEAR OLD FEMALEUNREMARKABLE PAST MEDICAL HISTORY
WASHING DISHES THE FLOOR AND CHAIRS STARTED MOVING
COMPLETENEUROLOGICAL AND CARDIAC WORK UP
SEVERE COLD SINUS INFECTION 3 WEEKS PRIOR – TOOK OVER THE COUNTER MEDS
Questions

Visual and Vestibular Exam in Home HealthWrisley and Zirges CSM 2016 13
References
• Lord et al. Sensorimotor function, balance abilities and pain influence Timed Up and Go performance in older community-living people. Aging Clin Exp Res. 2011;23(3):196-201.
• Lord. Visual risk factors for falls in older adults. Age Ageing. 2006;35 Suppl 2:ii42-ii45.
• Lord SR et al. Vision and falls in older people: risk factors and intervention strategies. Clin Geriatr Med. 2010;26(4):569-81.
• Mucha et al. A brief vestibular ocular motor screening assessment to evaluate concussions.
• Honaker and Shepard. Use of dynamic visual acuity test as a screener for community-dwelling older adults who fall. J Vestib Res. 2011;21(5):267-276.
• Rubin and Cheshire. Evaluation of dizziness in neurology office. Semin Neurol. 2011;31(1):29-41.
• Huh and Kim. Bedside evaluation of dizzy patients. J Clin Neurol. 2013;9(4):203-213.• Omar, R. (2015). Faints, fits and funny turns for the physician. Clinical Medicine. Vol
15, No 6: 557–61.