Embed Size (px)
Citation preview

Avascular Necrosis Femoral Head

Synonyms • avascular necrosis of the femoral head,
osteonecrosis, osteonecrosis of the femoral head, ischemic necrosis, ischemic necrosis of the femoral head, ischemic bone necrosis, bone necrosis of the femoral head, bone infarct of the femoral head, idiopathic bone necrosis of the femoral head, nontraumatic avascular necrosis of the femoral head, traumatic avascular necrosis of the femoral head, subchondral avascular necrosis, coronary artery disease of the femoral head, AVN


Etiology Pathologic changes
are intravascular and extravascular factors.


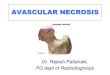
The normal circulation of the femoral head. The posterior-superior retinacular arteries provide the major blood supply to the epiphysis. They traverse the femoral neck and are contained within the joint
capsule. They give rise to the lateral epiphyseal vessels at the junction of the femoral head and neck. From there, they penetrate
the femur and supply the femoral epiphysis.



Blood Supply to Bone:

Intravascular factors Extraosseous vascular factors - The femoral head is an end-organ system with poor collateral development. Trauma to the hip may lead to contusion or mechanical interruption to the lateral retinacular vessels, the main blood supply of the femoral head and neck Vasculitis, as seen in Raynaud disease, or vasospasm, as seen in decompression sickness, can interfere with extraosseous circulation.


The blood supply to the femoral head is compromised by subcapital femoral fractures or slipped capital femoral epiphysis.
As the epiphysis or femoral neck separates from the femoral head, the femoral metaphysis displaces superolaterally and the femur
rotates externally. This causes the distal posterior-superior retinacular arteries and proximal lateral epiphyseal vessels to kink
or rotate, compromising the blood flow to the epiphysis.

Intraosseous vascular factors - Arterial
Circulating microemboli that block the microcirculation of the femoral head.
sickle cell disease (SCD), fat embolization, or air embolization from
dysbaric phenomena. ed by fat emboli, in hyperlipidemia associated with
alcoholism, steroid therapy, SCD, and nitrogen bubbles in decompression
sickness.

Intraosseous vascular factors - Venous
Conditions such as Caisson disease and SCD have a strong tendency to involve
the venous side of the circulation, reducing venous outflow and causing
stasis. Enlargement of intramedullary fat cells may be the most significant factor
leading to obstruction of venous drainage.

Extravascular factors


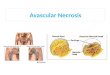
Bone Anatomy• Diaphysis• Metaphysis• Epiphysis – Prox/Dist• Epiphyseal line• Periosteum• Compact cortical bone• Spongy bone• Articular Cartilage• Medullary cavity• Marrow• Nutrient artery

Compact Bone:

Intraosseous factors The bone system within the subchondral region is enclosed within a rigid shell of cortical bone. This is particularly sensitive to increases in pressure resulting in a compartment syndrome. Fat cells, Gaucher cells and inflammatory cells, encroach on intraosseous capillaries, reducing intramedullary circulation and resulting in compartment syndrome. Blood flow normally is poorer in fatty marrow. Transmitted pressure in the weight bearing region of the femur compresses capillary circulation, which is already compromised by increased intraosseous pressure.Repeated microfractures in the weightbearing segment of the femur may cause multiple vascular lesions resulting in ischemia within fragile and poorly repaired bone. In cellular cytotoxic factors, such as alcoholism and steroid-related AVN, there could be a direct toxic metabolic effect on osteogenic cells. Trabecular deformation, which normally occurs during weight bearing, also compresses the marrow space to some degree In idiopathic osteonecrosis, a possible quantitative or qualitative deficiency in the bone architecture. Effects of raised pressure are on the sinusoids and the small marrow capillaries, then on the venous outflow. Reflex spasm can even block nutrient vessels before they enter the cortex.

Capsular factors Disease processes within the hip joint that produce effusions, such as trauma, infection, and arthritis, may affect the blood supply to the epiphysis adversely. The mechanism involves tamponade of the lateral epiphyseal vessels , which are located within the synovial membrane, through increased intracapsular pressure.

Pathophysiology:
The cause is multifactorial The final common pathway may
represent intravascular coagulation with fibrin-platelet thrombosis
beginning in the vulnerable subchondral microcirculation
(capillary and sinusoidal beds) resulting in vasoconstriction and
impaired fibrinolysis and infarction.

Sequelae of AVN Minimal disease: Small vascular area not adjacent to an articular surface -- asymptomatic and it could heal spontaneously – undetected severe disease: AVN develops, repair starts at the interface between viable and necrotic bone. Dead bone is reabsorbed Reactive and reparative bone is laid down on dead trabeculae resulting in a sclerotic margin of thickened trabeculae . The incomplete resorption of dead bone results in a mixed sclerotic and cystic appearance . Mechanical failure: subchondral region, microfractures do not heal because they occur within an area of dead bone. Progression of the microfractures results in a diffuse subchondral fracture, the crescent sign Following subchondral fracture and progressive weightbearing, collapse of the articular cartilage occurs . Continued fracture, necrosis, and further weightbearing can
progress to degenerative joint disease (DJD) and joint dissolution.

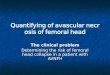
Anteroposterior view of the pelvis shows flattening of the outer portion of the right femoral head from
avascular necrosis (arrow), with adjacent joint space narrowing, juxta-articular sclerosis, and osteophytes
representing degenerative joint disease.

flattening of the right femoral head (black arrows).

Conditions associated with AVN
• Trauma • Alcoholism • Steroid use • Decompression sickness (Caisson disease) • Metastatic disease • Pancreatic disease • Hemoglobinopathies • Gaucher disease • Irradiation • Hemophilia • Dialysis• Hypercoagulable states

Trauma Trauma is the most common cause of AVN. AVN
can occur within 8 hours after traumatic disruption of the blood supply. The superior retinacular
vessels and the nutrient artery can be damaged as they enter the femur. The artery of the ligamentum
teres (ALT) also may be damaged. Intracapsular hematoma increases intracapsular pressure, which
can cause tamponade of the vessels within the joint capsule.
Intertrochanteric and extracapsular fractures of the femur rarely develop AVN. Following hip
dislocation, circulation is interrupted because of tears of the ligamentum teres, tearing the ALT. Tearing of the joint capsule compromises the
vessels within the capsular reflections.

Alcoholism Alcohol may have a toxic effect on
osteogenic cells. The direct toxic effect of alcohol results in fat deposition in the
liver. Livers with fat deposits are a constant source of low-grade
asymptomatic fat emboli. Intraosseous fat emboli become hydrolyzed to free fatty acids, which cause endothelial damage.
Alcohol intake exceeding 40 mL per week increases the risk of AVN more than 11
times compared to the risk in nondrinkers. A clear dose-response relationship exists.

Steroid use 1.Occlusion of small vessels occurs related to fat emboli from the liver. 2. Increased intraosseous pressure results from a steroid-related increase in the size of the intramedullary fat cells without an equivalent compensatory loss of trabecular and cortical bone. 3. Fat emboli become hydrolyzed to free fatty acids, which are toxic to vascular endothelium, causing
intravascular coagulation. 4. Angiogenesis is inhibited by a reduction of proteolytic activity by the synthesis of polyclonal antithyroid hormone receptor alpha-1 antibody 5. A direct toxic effect occurs on osteogenic cells. 6. Steroid use causes conversion of hematopoietic marrow to fatty marrow, a prerequisite for the development of AVN.

Decompression sickness (Caisson disease) Workers in underwater enclosures requiring compressed air to prevent water seepage are at risk. AVN occurs as a result of exposure to pressure greater than 17 lb per square inch. These infarcts tend to be large. Undersea divers are at risk. Key risk factors are the depth of the dive, the number of dives, uncontrolled decompression, and low oxygen concentrations. The presence of intravascular bubbles of nitrogen obstructs capillaries. Extravascular nitrogen within the fatty marrow, encased within the bone, compresses intramedullary vessels. Arteriolar spasm also may occur. Fat cells have a 5-fold ability to absorb dissolved nitrogen. Such absorption increases their volume within the nonexpandable confines of the bony trabeculae and cortex, increasing intraosseous marrow pressure and causing venous stasis.

Metastatic disease Metastatic cells can pack the
marrow, resulting in increased intramedullary pressure obstructing the intramedullary vessels. Patients
are at higher risk if they are receiving steroid therapy and/or are undergoing local radiation therapy
to the hip.

Pancreatic disease The release of lipolytic enzymes into the bloodstream results in breakdown of the fat within the marrow cells into free fatty
acids, which are toxic to endothelium, causing intravascular coagulation. Upon
entering the portal venous radicals in patients with pancreatitis, pancreatic
enzymes can cause release of intracellular fat from fat-laden hepatic
cells.

Hemoglobinopathies (SCD, thalassemia, hemoglobin C disease, hemoglobin D disease, hemoglobin E disease) Hemoglobinopathies are the principal cause of AVN . Infarcts in hemoglobinopathies tend to be large. AVN only occurs when a sickle gene is present to cause the sickling phenomena. Sickling of abnormal red blood cells occurs in intramedullary capillaries and venules, causing hyperviscosity and vascular occlusion. Bone marrow hyperplasia resulting from chronic anemia may pack the marrow, placing it at increased risk for developing AVN from elevated intramedullary pressure.

Gaucher disease Gaucher disease is a metabolic disorder consisting of a deficiency of the enzyme b-glucosidase, which normally catalyzes
the removal of glucose from glucocerebroside. Glucocerebroside
accumulates in the reticuloendothelial cells within the bone marrow, resulting in
packing of marrow, compression of interosseous sinusoids, and elevation of
interosseous pressure. Infarcts tend to be large.

Dialysis Elevated levels of parathormone may cause increased subchondral bone turnover with replacement by disorganized bone matrix unable to support normal weightbearing, resulting in microfractures and increased intramedullary pressure. Irradiation Fibrosis and endothelial proliferation resulting from radiation-induced arteritis cause underlying vascular compromise. Patients with metastatic lymphoma or carcinoma to the femoral head who are treated with steroids and chemotherapy are at increased risk of developing AVN. AVN occurs with doses exceeding 30 Gy. Hemophilia Repeated microhemorrhages within the confines of the marrow result in increased intramedullary pressure. Capsular distension from hemorrhage may compress the retinacular vessels within the synovial capsule.

Hypercoagulable states - Inherited disordersHypercoagulable states - Acquired disorders Legg-Calvé-Perthes (LCP) disease Slipped capital femoral epiphysis Congenital dislocation of the hip Fatty liver Femoral head fracture Femoral head dislocation Sickle cell disease Pregnancy

Pathology

Gross pathology Cancellous bone in the femoral head shows irregular areas of yellow necrosis extending up to several millimeters of articular cartilage. With progression, a patchy zone of softening develops in the necrotic cancellous bone, adjacent to viable bone, representing resorption of the necrotic segment. With further weightbearing and bone resorption, structural support is lost in the subarticular region with resultant microfractures and subsequent creation of an articular sequestrum. A line of trabecular fractures extends across the dead bone, which creates and separates an articular sequestrum. Following trabecular fracture, the load-bearing segment of the femoral head collapses. Breaks in the smooth contour of the femoral head become visible, most often at the superior margin of the fovea and beneath the acetabular lip. After collapse of the femoral head, progressive destruction of the articular cartilage and underlying bone occurs, loose bodies appear, and marginal osteophytes develop, heralding the development of DJD

Histopathology Cell necrosis of the Hematopoietic elements ,the bone cells, eg, osteocytes, osteoclasts, and osteoblasts and marrow fat cells is seen.
Bone infarcts can be divided into 4 zones, ie, a central zone of cell death surrounded by successive zones of ischemia, hyperemia, and normal tissue. Repair Bone resorption occurs first, followed by new bone formation. Repair begins along the outer perimeter at the junction between the dead area and the viable area containing an intact circulation

Sex: disease affects males 4 times more frequently than it affects females. Age: AVN usually occurs in patients in the third-to-fifth decades unless predisposing conditions exist that place different age groups at risk, ie, LCP and slipped capital femoral epiphysis.

Clinical Details: Patients may be asymptomatic or may develop pain gradually , experience a decreased range of motion (ROM), and walk with a limp. Pain can be excruciating and of sudden onset. Pain Pain can be focal, over the groin or hip, or it can radiate to the buttocks, anteromedial thigh, or knee. Pain can be induced mechanically by standing and walking and can be eased by rest. Pain can be very intense, especially in the large infarcts When the disease is chronic, pain can be vague. Following treatment of a traumatic hip fracture, AVN may manifest as worsening pain. Click A click may be heard when the patient rises from a sitting position. A click may be elicited by external rotation of an abducted hip.Range of motion ROM may be diminished, especially after collapse of the femoral head. ROM may be limited, especially in flexion, abduction, and internal rotation. Gait: Patients may walk with a limp.

X ray findings

Stage 0 (preclinical and preradiologic)
AVN can be suggested only if it has already been
diagnosed in the contralateral hip.

Stage 1 (preradiologic) Stage 1 represents the early resorptive stage. Late in this stage, plain radiographs may show minimal osteoporosis and/or blurring and poor definition of the bony trabeculae. Osteoporosis appears when one third of the mineral content of bone has been lost.

Stage 2 Demineralization is evident. It may be generalized or patchy or appear in the form of small cysts within the femoral head. Demineralization is the first manifestation of the stage and it represents resorption of dead bone. Patchy sclerosis appears , usually in the superolateral aspect of the femoral head . Patchy sclerosis appears as increased density on radiographs and may be diffuse, focal, or in a linear arc, which is concave superiorly. Patchy sclerosis usually coexists with demineralization, appearing as alternating regions of increased density and increased lucency.

Stage 3 (early collapse of the femoral head) A linear subcortical lucency, representing a fracture line, is present immediately beneath the articular cortex. It may extend into the articular cartilage at the superolateral aspect of the femoral head. This is termed the crescent sign and is best demonstrated on a frogleg view . The subarticular cortex may remain attached to the cartilage and is separated from the underlying femur by soft tissue, termed the eggshell sign. The femoral head initially preserves its round appearance, but later, it demonstrates collapse. This may be indicated by joint-space widening.

Stage 4 Further flattening of the femoral head occurs with loss of its smooth convex contour . Fragments of bone and cartilage may separate from the underlying femur, roam freely within the hip joint, and become loose bodies. Severe collapse and destruction of the femoral head leads to progressive DJD with joint space narrowing, marginal osteophyte formation, and subchondral cyst formation.


Stage 0 is both preclinical and preradiologic. Most patients with stage 0 disease are identified when imaging is performed to evaluate AVN in the contralateral hip or to exclude other diseases. Stage 1 demonstrates normal radiograph findings or shows minimal demineralization or blurred trabeculae. Pain in the anterior groin or thigh is common. Limited ROM in the hip may be present. Stage 2 shows diffuse or localized areas of sclerosis, lucencies, or both within the femoral head. Clinical signs persist or worsen. Stage 3 is characterized by the crescent sign (subchondral fracture). Stage 4 demonstrates marked collapse and fracture involving the articular surface. Segmental flattening of the femoral head demonstrates an out-of-round appearance.
Stage 5 is characterized by the development of DJD.

Early CT signs of AVN Osteoporosis is the first sign visible. Later, the central bony asterisk is distorted, appearing as clumping and fusion of the peripheral asterisk rays. Clumping appears as spots or as hyperdense "roads" of various width .

MRI anatomy Fatty marrow is present in the femoral capital epiphysis and the greater trochanter .This has high signal on T1-weighted images (T1WIs) and T2-weighted images . Hematopoietic marrow, when present, is found in the femoral neck, intertrochanteric region, and acetabulum. It has low signal on T1WIs and high signal on T2WIs The medullary cavity contains prominent vertically orientated linear striations of low signal on all imaging sequences extending from the inferolateral aspect to the superomedial aspect of the femoral head. These represent the weightbearing trabeculae and are analogous to the asterisk sign seen on CT scans . The medullary cavity is surrounded by a sharply marginated low-intensity line representing the cortex of the bone. Cortex and trabeculae have weak MRI signals because of a low concentration and decreased mobility of hydrogen ions A thin high-signal line, representing the articular cartilage, surrounds the outer margin of the femoral head. A curvilinear low-signal line, representing the physis, crosses the marrow of the femoral neck laterally to medially

MRI findings T1-weighted images: A peripheral band of low signal is present in the superior portion of the femoral head outlining a central area of bone marrow. This is considered to represent the reactive interface between the necrotic and reparative zones and extends to the subchondral bone plate . T2-weighted images: The inner border of the peripheral band demonstrates high signal. This may represent chemical shift artifact because the position of the signal changes when the phase and frequency directions are changed. This is termed the double-line sign and is pathognomonic for AVN . The outer low-signal ring represents the interface of repair tissue with the necrotic zone.

Nuclear Medicine Findings: Single-photon emission computed tomography A cold spot (photon-deficient region) within the femoral head is highly specific for AVN and is the earliest scintigraphic evidence of AVN. This usually is seen 7-10 days after the ischemic event. Over a period of weeks to months, increased uptake representing revascularization and repair surrounds and eventually replaces the region of photopenia. The central region of photopenia with surrounding zone of increased uptake is termed the doughnut sign. Perfusion and static planar radionuclide imaging Initially, uptake is decreased in the perfusion and static phases, which represents the early ischemic event. Later, uptake is decreased within the femoral head in the perfusion phase and increased around the cold region in the static phase. The latter represents the reactive zone around the infarcted segment. The increased uptake from the reparative zone eventually replaces the photopenic region.











THE END