Embed Size (px)
Citation preview

Mædica A Journal of Clinical Medicine, Volume 4 No.1 200926
M K pag 26
EEEEEDITORIALSDITORIALSDITORIALSDITORIALSDITORIALS
Mædica - a Journal of Clinical Medicine
Avascular necrosisof the femoral headHoria Bogdan ORBAN, MD, PhD; Valentin CRISTESCU, MD;Mihaela DRAGUSANU, MD
Orthopaedics and Traumatology Department,“Elias” Emergency University Hospital, Bucharest, Romania“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
Address for correspondence:Horia Bogdan Orban, MD, PhD, 17 Marasti Blvd., District 1, Bucharest, Zip Code 011461, Romaniaemail address: [email protected]
ABSTRACTAvascular necrosis (AVN) is a disease that may affect several different bones as a result of temporary or
permanent loss of the blood supply to these bones. The femoral head is most commonly affected by thisdisease. Usually, the patients are in their third, fourth or fifth decade of life at the time of diagnose.
Initially, patients are asymptomatic, but, in time, AVN leads to joint destruction, requiring surgicaltreatment and, in latter stages, total hip replacement. It is essential that AVN of the femoral head isdiagnosed early because delaying this disease by joint preserving measures has a much better prognosisand because the results of joint replacement are poorer in young individuals.
There are various conditions than can be incriminated as triggers for this disease. However, almost halfof the patients diagnosed present none of these conditions. This type of avascular necrosis is termed primary,or idiopathic. All the other forms of this disease are secondary.
Treatment has been facilitated by using widely accepted international classification systems and byeffective earlier diagnosis using MRI and other imaging techniques.
Although treatment has turned more and more towards surgery, no universally satisfactory therapy hasbeen developed, even for early disease.
Key words: avascular necrosis, femoral head, hip pain, ficat-Arlet classification, coredecompression, total hip replacement
INTRODUCTION
Avascular necrosis (AVN), also known asosteonecrosis, aseptic necrosis or ischemic bonenecrosis is a disease that may affect several dif-ferent bones as a result of temporary or per-manent loss of the blood supply to these bones.The ischemia causes the death and eventualcollapse of the bone tissue, with its overlyingjoint surface (1).Koenig was the first to describethis condition, which he termed osteochondri-
tis dissecans, in 1888. In 1925, Haenish de-scribed the first case that involved the femoralhead. In 1940, the cause of the necrosis wasdeemed to be arterial occlusion. Pietrograndidescribed the first case of femoral head AVNafter steroid use in 1957 (2). Ever since, scien-tists have found out more and more about thecomplex physiopathology of this disease whichto this days remains largely unknown.
The femoral head is most commonly affectedby this disease. Usually, the patients are in their

Mædica A Journal of Clinical Medicine, Volume 4 No.1 2009 27
AAAAAVASCULAR N N N N NECROSIS OF THE FFFFFEMORAL H H H H HEAD
M K pag 27
third, fourth or fifth decade of life at the timeof diagnose. Men are more prone to this dis-ease than women, the sex ratio being about 4.
Initially, patients are asymptomatic, but, intime, AVN leads to joint destruction, requiringsurgical treatment and, in latter stages, total hipreplacement (THR) (2). Although treatment hasbeen facilitated by using a widely accepted inter-national classification system, effective earlier di-agnosis using MRI, and more aggressive surgicalmanagement, no universally satisfactory therapyhas been developed, even for early disease.
It is essential that AVN of the femoral head isdiagnosed early because delaying this disease byjoint preserving measures have a much betterprognosis and because the results of joint replace-ment are poorer in young individuals (2).
ETIOLOGY
There are various conditions than can be incriminated as triggers for this disease. How-
ever, almost half of the patients diagnosedpresent none of these conditions. This type ofavascular necrosis is termed primary, or idio-pathic. All the other forms of this disease aresecondary (2-8). One of the most common rea-sons for secondary avascular necrosis is pro-longed systemic steroid use in high doses(equivalent to 4000 mg of Prednisone) for ex-tended periods of up to 3 months, or longer.There were cases cited in literature of AVN ofthe femoral head after relatively brief periods(7 days) of oral steroids. The mechanism ofaction is not yet fully understood, but it isthought to be linked to the hypercoagulablestate, with subsequent impaired fibrinolysis andvenous thrombosis in the femoral head. Othercommon causes include trauma, blood disor-ders or decompression disease.
Taking these facts into account, AVN can beclassified as follows:
Primary (idiopathic)Secondary to:– Trauma – Fracture of the femoral neck
Slipped capital femoral epiphysisProximal femoral epiphysiolysisDislocation of the femoral headEpiphyseal compressionVascular traumaBurnsRadiation exposure
– HemoglobinopathiesSickle cell disease
Hemoglobin S or hemoglobin ChemoglobinopathyPolycythemia
– Caisson disease – Dysbaric osteo-necrosis
– Local infiltrative diseaseGaucher diseaseInfectionNeoplasms
– HypercortisolismCorticosteroid medicationsCushing disease
– Alcohol consumption– Pancreatitis– Chronic renal failure– Cigarette smoking– Collagen vascular diseases– Congenital and developmental
Congenital dislocation of the hipEhlers-Danlos syndromeHeredity dysostosisLegg-Calvé-Perthes disease
– Fabry disease– Giant cell arteritis– Gout and hyperuricemia– Hemodialysis– Hypercholesterolemia– Hypercoagulable states– Hyperlipidemia– Hyperparathyroidism– Intravascular coagulation– Organ transplantation– Pregnancy– Systemic lupus erythematosus– Thrombophlebitis– Hemophilia
PHYSIOPATHOLOGY
Extraosseous arterial factors are the mostimportant. The femoral head is at increased
risk because the blood supply is an end-organsystem with poor collateral development. Bloodsupply can be interrupted by trauma, vasculitis(Raynaud disease), or vasospasm (decompres-sion sickness) (2,3).
Intraosseous arterial factors may block themicrocirculation of the femoral head throughcirculating microemboli. These can occur insickle cell disease (SCD), fat embolization or airembolization from dysbaric phenomena (2,9).
Intraosseous venous factors affect thefemoral head by reducing venous blood flowand causing stasis. These factors may accom-pany conditions such as Caisson disease, SCDor enlargement of intramedullary fat cells (2,8).

Mædica A Journal of Clinical Medicine, Volume 4 No.1 200928
AAAAAVASCULAR N N N N NECROSIS OF THE FFFFFEMORAL H H H H HEAD
M K pag 28
Intraosseous extravascular factors affectthe hip by the increasing the pressure, resultingin a femoral head compartment syndrome (2).For example:
– Fat cells hypertrophy after steroid admin-istration or abnormal cells, such asGaucher and inflammatory cells, canencroach on intraosseous capillaries,reducing intramedullary circulation andcontributing to compartment syndrome.
– Repeated microfractures in the weight-bearing segment of the femur may causemultiple vascular lesions resulting in is-chemia within fragile and poorly repairedbone.
– Cytotoxic factors, such as alcoholism andsteroid use, have a direct toxic metaboliceffect on osteogenic cells (2).
– Decreased concentrations of 1,25 di-hydroxyvitamin D3 can cause a quanti-tative or qualitative deficiency in the bonearchitecture, causing the bone to deformunder pressure.
Extraosseus extravascular (capsular) fac-tors involve the tamponade of the lateral epi-physeal vessels located within the synovial mem-brane, through increased intracapsular pressure.This occurs after as trauma, infection, and ar-thritis, causing effusion that may affect the bloodsupply to the epiphysis (2,3).
CLINICAL DETAILS
History
Avascular necrosis may be asymptomatic andis occasionally discovered following radiog-
raphy.Pain in the affected joint, described as throb-
bing, deep and, often, intermittent (2), is typi-cally the presenting symptom. Patients with AVNof the femoral head often report groin or hippain that can radiate to the buttocks, ante-romedial thigh, or knee that is exacerbated byweight bearing and sometimes by coughing. Thepain may initially be mild but progressivelyworsens over time and with use. Eventually, thepain is present at rest and may be present oreven worsen at night (7), in which case, it maybe associated with morning stiffness.
Physical
Usually the initial findings are unrevealing.In the latter stages of the disease, jointfunction deteriorates and the followingsigns may be found:
– The patient may walk with a limp andmay experience loss of range of motion,both active and passive, most frequentlyin flexion, abduction, and internal rota-tion, especially after collapse of the femo-ral head.
– The patient may have tenderness aroundthe affected area.
– A neurological deficit may be found (7).– The Trendelenburg sign may be positive.– A click may be heard when the patient
rises from a chair or after external rota-tion of the abducted hip (2).Advanced disease leads to joint deformityand muscle wasting (7).
Imaging
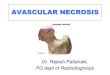
Plain film radiographic findings are ab-sent in stages 0 and 1 of AVN. A normalradiograph does not equal a normal hip.A delay of 1-5 years can occur betweenthe first symptoms and the appearanceof radiographic modifications (2). Inmore advanced disease, radiographsshow sclerosis and changes in bone den-sity. As the disease progresses, subchon-dral radiolucent lines (crescent sign), flat-tening or the collapse of the femoral headmay appear (7).CT scan is used to determine the extentof involvement, such as subchondrallucencies and sclerosis present in the re-parative stage (2) (before the collapse ofthe femoral head), but it is not as sensi-tive as MRI in stages 0 and 1. CT is excel-lent for detecting femoral head collapse,early degenerative joint disease and thepresence of loose bodies especially whenusing multiplanar reconstruction (2).MRI is the most sensitive means of diag-nosing AVN, representing the gold-stan-dard of noninvasive diagnostic evaluation(FIGURE 1). It has several advantages:
– It allows accurate staging by clearly de-picting the size of the lesion.
– It detects asymptomatic lesions (7) thatare undetectable on plain radiographs,thus facilitating early treatment and bet-ter response.
– It provides multiplanar imaging and ex-cellent soft tissue resolution (10,11).
– It can demonstrate response of the femo-ral head to treatment (2).Single-photon emission computed to-mography (SPECT) is used as an alterna-

Mædica A Journal of Clinical Medicine, Volume 4 No.1 2009 29
AAAAAVASCULAR N N N N NECROSIS OF THE FFFFFEMORAL H H H H HEAD
M K pag 29
tive for MRI when the latter cannot beperformed or when MRI results are in-determinate. SPECT is difficult to use be-cause it requires remaining still for longperiods of time. Also, bladder artifacts area frequent problem (2,10).
Scintigraphic imaging reveals a central areaof decreased uptake, surrounded by an areaof increased uptake (the doughnut sign or cold-in-hot sign) (2). It indicates the reactive zonesurrounding the necrotic area. The main dis-advantages are that it lacks specificity (2) andthat the same image may be encountered inother conditions such as osteoarthritis, fracture,and inflammatory arthritis. Results are difficultto interpret if disease is bilateral.
Bone biopsy is not routinely used becauseof the availability of sensitive noninvasive testssuch as MRI (7). It is a valuable diagnostic toolafter analyzing the bony fragment extracted aftercore decompression.
– Malignancy– Hemangioma– Radiation therapy– Sympathetic dystrophy– Bone marrow edema syndrome (2,7)
CLASSIFICATION
Ficat and Arlet have developed a staging sys-tem using radiographic findings, consisting
of four stages. Hungerford and Lennox modi-fied this staging system when MRI became avail-able, adding stage 0 to the classification (2,3).
– Stage 0 (preclinical and preradiologic) –negative findings on a plain radiograph,in an asymptomatic patient with a posi-tive diagnose in the contralateral hip. TheMRI shows a double-line sign, consistentwith a necrotic process.
– Stage I (preradiologic) – normal findingson radiographs and positive findings onMRI or bone scintigraphy. Stage 1 repre-sents the early resorptive stage. The firstradiographic findings appear late in thisresorptive stage (minimal osteoporosisand/or blurring and poor definition of thebony trabeculae).
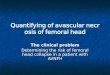
– Stage II (reparative stage) occurs beforethe flattening of the femoral head. It canlast for several months or years. The ra-diographic changes are evident and theyare represented by demineralization(early manifestation of the reparativestage, representing resorption of deadbone) and sclerosis (appearing after dem-ineralization, representing apposition ofnew bone on dead trabeculae). Dem-ineralization may be generalized orpatchy or appear in the form of smallcysts within the femoral head. Patchysclerosis appears as increased density onradiographs, usually in the superolateralaspect of the femoral head and may bediffuse, focal, or in a linear arc, which isconcave superiorly. These changes areconsistent with stage IIA (FIGURE 2). StageIIB (FIGURE 3) is a transition phase char-acterized by the presence of the crescentsign, seen as a linear subcortical lucency,situated immediately beneath the subcor-tical bone, representing a fracture line. Itis best seen on a frog leg view. The femo-ral head remains round, initially, but latercollapses, creating a joint-space widening.
– Stage III (early collapse of the femoralhead) is heralded by the presence of
Differential diagnose
– Trauma– Degenerative disease– Osteoporosis– Arthritis– Inflammatory synovitis– Epiphyseal dysplasia– Epiphyseal stress fracture– Transient osteoporosis of the hip– Osteomyelitis
FIGURE 1. MRI scan of bilateral type II lesion

Mædica A Journal of Clinical Medicine, Volume 4 No.1 200930
AAAAAVASCULAR N N N N NECROSIS OF THE FFFFFEMORAL H H H H HEAD
M K pag 30
sequestration and depression, with theappearance of decrochage, without ac-etabular involvement. The femoral headis no longer round and smoothly con-toured. It appears flattened or collapsed.(FIGURE 3)
– Stage IV (progressive degenerative disease)is represented by the severe collapse anddestruction of the femoral head alongwith joint space narrowing, osteophyteand subchondral cyst formation, as defi-nite signs of degenerative joint disease.
Steinberg et al. expanded this staging sys-tem, by dividing stage III lesions into femoralheads with or without collapse or hips with orwithout acetabular involvement. In addition,they quantified the amount of involvement ofthe femoral head into mild (<15%), moderate(15-30%) and severe (>30%), based on radio-graphs (TABLE 1).
Ohzono et al. incorporated the concept oflocation of the lesion, with prognostic value. Intype 1 lesions, there is a line separating thenormal femoral head from the affected, scle-rotic part. Depending on the amount of weight-bearing area involved, they are classified as A
FIGURE 2. Crescent sign
TABLE 1. Steinberg classificationFIGURE 3. Ficat-Arlet Stage IV of femoral head avascularnecrosis

Mædica A Journal of Clinical Medicine, Volume 4 No.1 2009 31
AAAAAVASCULAR N N N N NECROSIS OF THE FFFFFEMORAL H H H H HEAD
M K pag 31
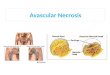
(<30%), B (30-60%) or C (>60%). Type 2 is acollapsed head without a separating line andtype 3 is represented by the presence of cysts(FIGURE 4). Type 3 A lesions are central, 3 Blesions involve the supero-lateral aspect of thefemoral head. Types 1 A, 1 B, 2 and 3 A havea better prognosis than types 1 C and 3 B. Morerecently, a new classification has been com-pleted by ARCO, which joins the Ficat Arlet stag-ing system, the Hungerford-Lennox modifica-tion, the quantification of involvement(Steinberg) and the concept of prognosis basedon location (Ohzono) (FIGURE 5).
Stage 0 – Bone biopsy results consistent withosteonecrosis; other test results normalStage I – Positive findings on bone scan,MRI, or both
– A – <15% involvement of the femoralhead (MRI)
– B – 15-30% involvement– C – >30% involvement
Stage II – Mottled appearance of femo-ral head, osteosclerosis, cyst formation,and osteopenia on radiographs; no signsof collapse of femoral head on radio-graphic or CT study; positive findings onbone scan and MRI; no changes in ac-etabulum
– A – <15% involvement of the femoralhead (MRI)
– B – 15-30% involvement– C – >30% involvement
Stage III – Presence of crescent sign le-sions classified on basis of appearance onAP and lateral radiographs
– A – <15% crescent sign or <2-mm de-pression of femoral head
– B – 15-30% crescent sign or 2- to 4-mmdepression
– C – >30% crescent sign or >4-mm de-pression
Stage IV – Articular surface flattened; jointspace shows narrowing; changes in ac-etabulum with evidence of osteosclero-sis, cyst formation, and marginal osteo-phytes.
TREATMENT
The goal of the treatment is to keep jointsfrom breaking down, because severe pain
and limitation in movement will occur within 2years, in the absence of treatment. There areseveral options that one can choose from andin order to determine the most appropriatetreatment, one has to take into considerationthe age of the patient, the stage of the disease,the location and amount of bone affected andthe underlying cause of avascular necrosis (un-less corticosteroid or alcohol use is stopped,treatment may not work) (1).
There are conservative and surgical meth-ods for treating this disease. Conservative treat-ments have been used experimentally alone orin combination, but they rarely provide lastingimprovement. Most patients will eventuallyneed surgery either to delay, or even to repairthe joint permanently (1).
Conservative Treatment
– Statin therapy, bisphosphonates (6,12,13)or nonsteroidal anti-inflammatory drugsmay be helpful.
– In some early cases, reduced weight bear-ing, limiting activities or using crutches canslow the damage caused by avascularnecrosis and permit natural healing (1).However, these patients run a risk of 85%of femoral head collapse (2). Protectedweight-bearing may be effective when theinvolved segment is smaller than 15% and
FIGURE 4. Ohzono Prognostic Classification

Mædica A Journal of Clinical Medicine, Volume 4 No.1 200932
AAAAAVASCULAR N N N N NECROSIS OF THE FFFFFEMORAL H H H H HEAD
M K pag 32
FIG
UR
E 5
. AR
CO
Inte
rnat
iona
l Cla
ssif
icat
ion
of O
steo
necr
osis

Mædica A Journal of Clinical Medicine, Volume 4 No.1 2009 33
AAAAAVASCULAR N N N N NECROSIS OF THE FFFFFEMORAL H H H H HEAD
M K pag 33
located far from the weight-bearing re-gion (5).
– Range-of-motion exercises are helpful formaintaining joint function (1).
– Electrical stimulation is thought to inducebone growth (1).
Surgical Treatment
– Core decompression is achieved by re-moving the inner layer of bone (1) andprovides immediate pain relief by reduc-ing pressure in the bone, decreasing vas-cular engorgement and inflammation andrelieving the compartment syndrome (2).It enhances the process of creeping sub-stitution and also encourages the forma-tion of new blood vessels, thereby in-creasing blood flow to the bone (1). It isindicated in people with early stages ofavascular necrosis, before the collapse ofthe head and when less than 30% of thefemoral head is involved (2). Core de-compression is also effective for pain re-lief (11) and helps delay the need for ar-throplasty, acting as a joint preserver.
– Bone grafting uses healthy bone from onepart of the patient and transplants it tothe diseased area. After the failure of non-vascularized grafts, present-day grafts(called vascular grafts) include an arteryand veins, increasing the blood supply tothe affected area (1). Bone grafting canbe combined with core decompression,acting together towards stopping the cycleof ischemia. It is indicated in early stagesof the disease and, when it is successful,it can ensure lifelong survival of the femo-ral head, in the absence of foreign body–associated complications. If unsuccessful,the procedure allows the patient to re-tain the option of total hip arthroplastyin the future (3).
– Osteotomy is a procedure by which thebone is reshaped to reduce stress on theaffected area. It requires a longer recov-ery period and limited activities for 3 to12 months after surgery. This procedureis most effective for patients with ad-vanced avascular necrosis and those witha large area of affected bone (1). Inter-trochanteric and transtrochanteric rota-tional osteotomies aim at bringing an in-tact area of bone and cartilage to theweight-bearing area of the femoral headand, at the same time, at improving
blood supply (biotrophic effect) (5,14).The consensus is that femoral osteoto-mies should be performed in more ad-vanced stages of the disease (II or III Ficat-Arlet), but that they should be limited topatients with Kerboul necrotic angle (sumof angles bordering the sequestrum onantero-posterior and lateral X-ray views)inferior to 200°. Historically, 25-30 yearsago, varisation, with or without media-lisation osteotomies were thought to besufficient, but later, flexion (Kempf) or ro-tational (Sugioka) osteotomies began togain ground. One possible problem withosteotomies is that they may make con-version to total hip arthroplasty more dif-ficult technically and less successful on along-term period.
– Arthroplasty. Most patients address anorthopaedic surgeon in advanced stagesof the disease, after femoral head col-lapse. Total joint replacement is the treat-ment of choice in the final stages of avas-cular necrosis or when the joint is irre-versibly destroyed (1). The procedure canbe done in numerous fashions, accord-ing to the surgeon’s preference. The sur-geon may use various approaches(antero-lateral, Hardinge, postero-lateral,minimal invasive, etc.) and may employan even broader array of implants. Clas-sic total hip endoprostheses (cementedor, preferably, cementless) account forthe majority of implants used but sur-geons and patients alike turn more andmore towards resurfacing arthroplasty(14), a procedure that holds several ad-vantages. Unlike classic implants thatemploy a friction couple of metal onpolyethylene, or ceramics or, more re-cently, Oxinium heads on polyethylenecups, resurfacing arthroplasty employs ametal on metal friction couple that is thenearest to the normal hip joint. By thistechnique, the acetabulum is replacedwith a cementless metal cup, very similarto its classic predecessor, but instead ofremoving the entire head and femoralneck (as is the case with classic implants),the femoral head is prepared by remov-ing its cartilage and a thin layer of bone,thus preserving most of the bone stock.A large diameter femoral implant is ce-mented (usually larger than 44 mm),

Mædica A Journal of Clinical Medicine, Volume 4 No.1 200934
AAAAAVASCULAR N N N N NECROSIS OF THE FFFFFEMORAL H H H H HEAD
M K pag 34
which ensures a superior stability againstdislocation. Also, the design of these im-plants ensures an even better range-of-motion, that can sometimes be crucialfor young, active patients. Also, resurfac-ing arthroplasty preserves more of thepatient’s bone stock, a feature that be-comes increasingly more important, tak-ing into account the patients’ young age,meaning that he/she will probably requirea second and sometimes even a third in-tervention (15) sometime later. Total hiparthroplasty, be it classic or resurfacing,yields excellent results, with immediateand long-lasting pain relief (4) and allowsearly mobilization and a quicker returnto an active lifestyle. However, severalauthors have observed that there is anearlier failure of total hip replacement inosteonecrosis than in age-matched pa-tients with other diagnosis. This is prob-ably because of abnormal remodeling ofbones and subsidence of prosthesis be-cause of the poor bone quality of theproximal femur. Other factors may in-
REFERENCES
1. Schoenstadt A – Avascular Necrosis,available at http://bones.emedtv.com/avascular-necrosis/avascular-necrosis.html, lastupdated/reviewed: November 05,2008
2. Aiello MR – Avascular Necrosis ofthe Femoral Head, available at http://emedicine.medscape.com/article/386808, updated: Aug 1, 2008
3. Aldridge JM 3rd, Urbaniak JR – Avascular necrosis of the femoralhead: etiology, pathophysiology,classification, and current treatmentguidelines. Am J Orthop Jul 2004;33(7):327-332
4. Assouline-Dayan Y, Chang C,Greenspan A, et al – Pathogenesisand natural history ofosteonecrosis. Semin ArthritisRheum Oct 2002; 32(2):94-124
5. Dudkiewicz I, Covo A, Salai M, etal –Total hip arthroplasty afteravascular necrosis of the femoralhead: does etiology affect theresults?. Arch Orthop TraumaSurg Mar 2004; 124(2):82-85
6. Lai KA, Shen WJ, Yang CY, et al –The use of alendronate to preventearly collapse of the femoral head inpatients with nontraumaticosteonecrosis. A randomized clinicalstudy. J Bone Joint SurgAm Oct 2005; 87(10):2155-2159
7. Jeanne K, Tofferi JK, Gilliland W –Avascular Necrosis, available at http://emedicine.medscape.com/article/333364, updated: Oct 24, 2008
8. Marti-Carvajal A, Dunlop R,Agreda-Perez L – Treatment foravascular necrosis of bone in peoplewith sickle cell disease. CochraneDatabase Syst Rev Oct 18 2004
9. Kerachian MA, Harvey EJ,Cournoyer D, et al – Avascularnecrosis of the femoral head: vascularhypotheses. Endothelium Jul-Aug 2006; 13(4):237-244
10. Sarikaya I, Sarikaya A, Holder LE –The role of single photon emissioncomputed tomography in boneimaging. Semin Nucl Med Jan 2001;31(1):3-16
11. Petsatodis GE, Antonarakos PD,Christodoulou AG, et al – Total HipArthroplasty for Osteonecrosis of theFemoral Head After Allogenic BoneMarrow Transplantation. JArthroplasty Jun 12 2008
12. Woo SB, Hellstein JW, Kalmar JR –Narrative (corrected) review:bisphosphonates and osteonecrosis ofthe jaws. Ann Intern Med May16 2006; 144(10):753-761
13. Agarwala S, Jain D, Joshi VR, et al –Efficacy of alendronate, abisphosphonate, in the treatment ofAVN of the hip. A prospective open-label study. Rheumatology(Oxford). Mar 2005; 44(3):352-359
14. Steffen RT, Foguet PR, Krickler SJ,et al – Femoral Neck Fractures AfterHip Resurfacing. J Arthroplasty Jun12 2008
15. Kelly JD IV, Wald D – Femoral HeadAvascular Necrosis, available athttp://emedicine.medscape.com/article/86568, updated: Nov 6, 2007
clude ongoing systemic disease, defectsin mineral metabolism, use of steroids,high level of activity in young patients andincreased body weight.
Over the years, as our knowledge of this dis-ease has improved, several surgical and con-servative methods of treatment have been per-fected. Their goal is to preserve the femoral headand prevent its collapse for as long as possiblekeeping in mind at the same time that the maxi-mal and definitive treatment is total hip replace-ment. Efforts should be made to delay themoment when arthroplasty is needed, withoutcompromising the chance of a straight-forwardhip replacement.
Although there have been extensive studiesregarding avascular necrosis of the femoral head,we still know little about its pathogenesis, andtherefore about the best method to treat thisdisease. Future medical treatment should beaimed at the cause of this disease, thus slowingdown or even stopping the evolution of avas-cular necrosis and thus delaying as much aspossible the need for surgery.